
Abstract
The negative impact of drug use is never far from the headlines in Scotland and is a constant reality in communities, primary care and hospital practice. The realisation that the medical establishment should attempt to quantify and define a larger education and research role allowed the Royal College of Physicians of Edinburgh (RCPE) to host a symposium ‘Alcohol and Substance Use: busting myths and finding solutions’ on 18th April 2024. This symposium was intended to bring together experts to explore the opportunities to energise systems to understand the challenges and coordinate appropriate responses.
Having supported several educational and strategy initiatives in recent years, including publishing the 2021 report ‘Drug Deaths in Scotland: an increasingly medical problem’ 1 combining with clinicians and researchers from the alcohol sector seemed like the most useful way to learn from the conspicuous success of Scottish Health Action on Alcohol (SHAAP). SHAAP is a partnership of the Medical Royal Colleges and Faculty of Public Health in Scotland, based in the RCPE, at a time when the internationally recognised flagship policy of minimum pricing of a unit of alcohol was being considered for revision in the Scottish Parliament.
The adoption in Scotland of an alcohol strategy based on WHO guidance reversed much of the increase in alcohol harm that Scotland had experienced in the decade from 1995. In 2009, per capita consumption in Scotland was 21% higher than in England and Wales with much of the difference due to low-cost vodka. By 2021, that gap had narrowed to 4% and the alcohol-specific mortality gap within the United Kingdom narrowed considerably over this period as Scottish deaths fell. 2 The effects of lockdown during the COVID-19 pandemic led to an increase in alcohol deaths internationally. Deaths in Canada and the United States rose almost 40% from 2019 to 2021. The 20% increase in Scottish deaths over that period is substantial but the preventative policies in place appear to have mitigated the effect.
In the illegal drug supply chain, the target and opportunity to disrupt demand or supply are less clear. Serial crises result in interventions becoming more responsive rather than preventative.
At the conference, speakers across a wide range of clinical and academic institutions agreed to speak and participate. There was a participant with lived experience in both sessions and panel discussions. The audience was made up of a range of health and research individuals from Scottish NHS and university departments. Online was a larger group of interested people from the United Kingdom, Europe, the Middle East, Asia and the Caribbean.
In an attempt to address the appalling statistics of drug-related deaths in Scotland and an admission of years of missed opportunities, the Government has spent considerable resources on the treatment and recovery sector and has a purposeful ‘mission’ to address the unacceptable numbers of drug deaths. 3 Embracing the concept of harm minimisation, the first time this phrase has been included in a national strategy document, 4 new initiatives such as the heroin-assisted treatment programme and the expected safer injecting environment clinic in Glasgow are signs of departure from a stagnant policy situation in the United Kingdom.
There is however good evidence to suggest that the number of drug-related deaths in Scotland is an underestimate. The real burden of mortality should include those deaths directly related to drug use but not included in the narrow definition used by the Office of National Statistics and the National Records of Scotland. These include delayed deaths from infections such as hepatitis and HIV and other causes like trauma, suicide and drug-related cancers which, if included, would increase the figures considerably.5 –8
Results from Public Health Scotland figures show the loss of life attributed to the consequences of drug use and the wide range of causation. It is striking how similar the figures are for men and women (Figures 1 and 2).
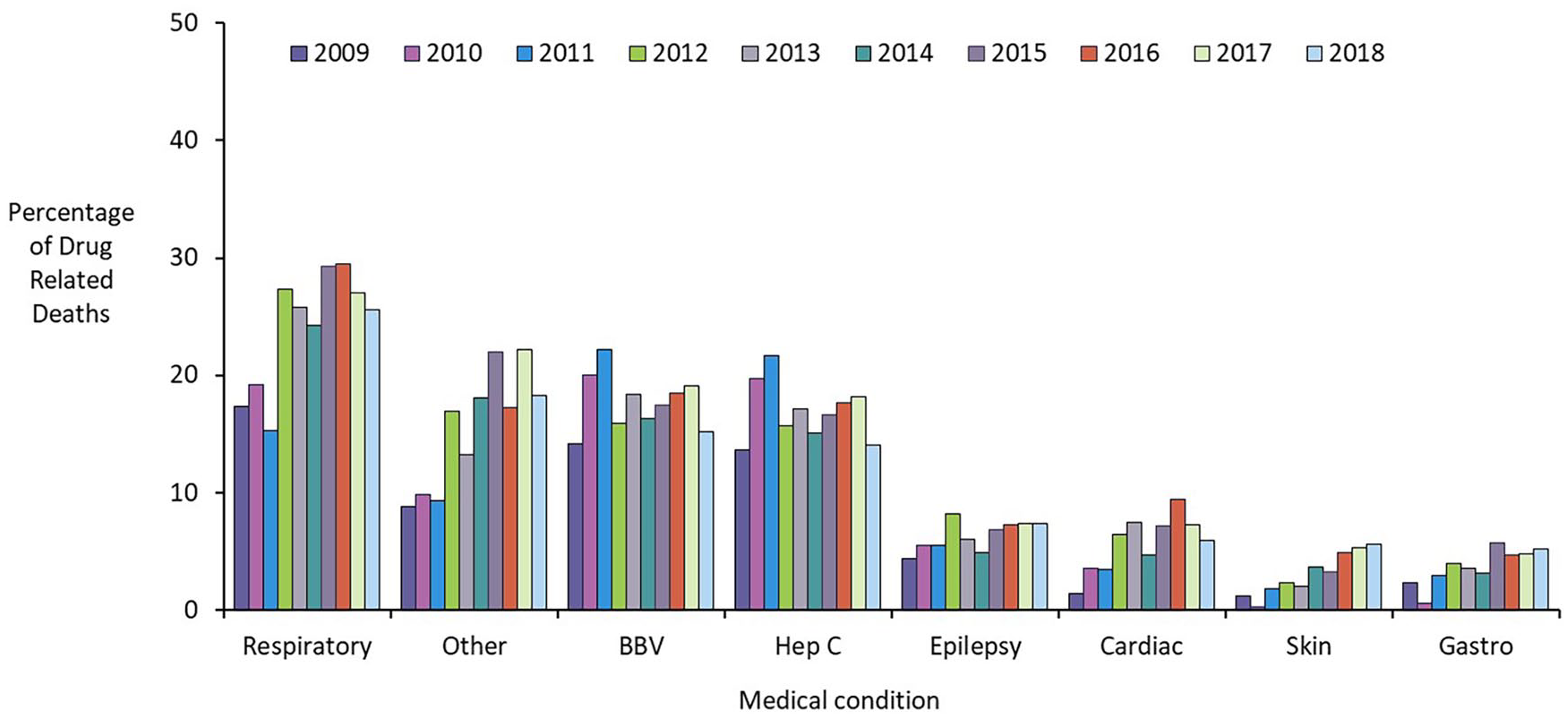
Medical conditions recorded in the 6 months prior to death (NDRDD: 2009–2018). For medical conditions, the category ‘Other’ encompasses the following diagnoses: eating disorder, learning disability, migraine, pancreatitis (not alcohol-related), and cases recorded as ‘Other medical condition’ (e.g. fracture, cancers).
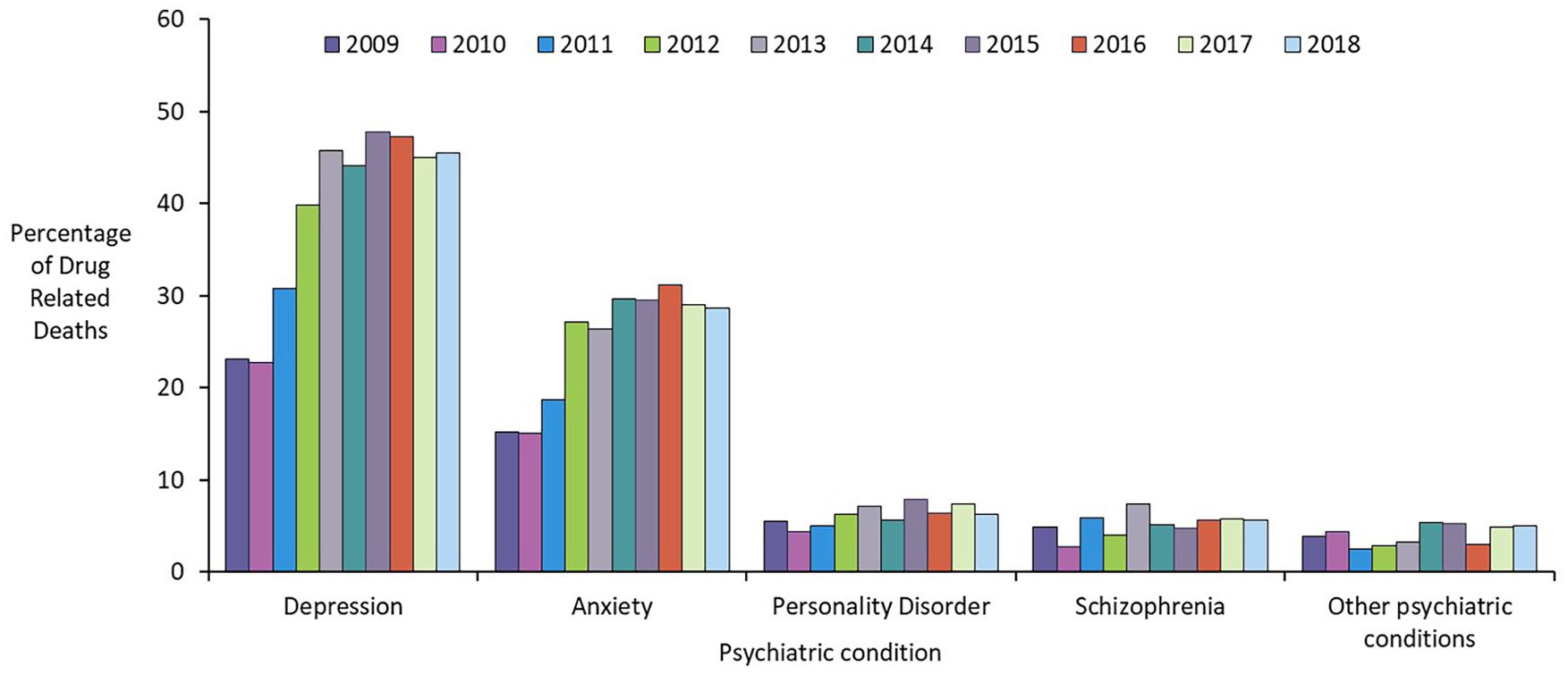
Psychiatric conditions recorded in the 6 months prior to death (NDRDD: 2009–2018). For medical conditions, the category ‘Other’ encompasses the following diagnoses: eating disorder, learning disability, migraine, pancreatitis (not alcohol-related), and cases recorded as ‘Other medical condition’ (e.g. fracture, cancers).
A wider view of the harms caused by drugs and possible solutions is required. We are in an era when those responsible in Government and the healthcare professions are keen to look for solutions rather than continue to define the problem. An example of an evidence-based approach is the recent contribution from Glasgow and Edinburgh universities highlighting specific changes in their message to the Government on how to address the inequalities in health care delivered by Primary Care.9,10
Drug problems have always been a moving target, and unlike alcohol, the supply chain is invisible (at least to those not involved in the murky business of trying to disrupt the international drug trade). The intersecting problems of multi-morbidity and the generalities of inequality of access to health care further complicate specific interventions, and the ever-expanding debate around drug control and regulation enshrined in the 1971 Misuse of Drugs Act 11 divert the minimal resources from progress in specific areas of reducing harm. Other than challenging the Government to redress the well-documented underfunding of mental health, the difficulty has been in identifying specific effective interventions.
Other issues are less clearly researched and championed. The RCPE should make an important contribution to the education and support of policy and research by establishing a focus on drugs like SHAAP does so effectively on alcohol-related harms. The conference identified the need for leadership and the enthusiasm and urgency for a partnership with other interested organisations. Universities and other Royal Colleges have their initiatives but there is clearly a cooperating and coordinating role that might be filled or initiated by the RCPE. The establishment of a working group that could take forward some of the ideas was one of the suggestions at the conference.
There were some general themes arising from the presentations and the discussions that followed. In the meeting room and online, there was a diverse group of interested clinicians and practitioners from a number of countries. This reflected the rather obvious reality that substance use problems affect many areas of medicine and social care across continents. The need for interventions at social, clinical and educational levels was apparent.
In its role of providing education and supporting research, the RCPE has a major role to play both in improving understanding and championing a revision of policy in the substance use sector. Three of the most tangible findings of the meeting were as follows: the need for improvement in undergraduate and postgraduate training and education, the vital role we could all play in lobbying policy in the profession(s) and political arena, and the feeling that drugs and alcohol are ‘everyone’s responsibility’ not just that of specialists.
As well as the ubiquity of dependency problems were the findings that there are overlapping problems between drugs, alcohol, multi-morbidity, poor education and social inequalities. Competing with the efforts of health and social care are the drivers of dependency. In the alcohol sector, this is the relentless marketing of alcohol across all platforms. 12 This leads to a normalisation of alcohol use in society as well as a false and engrained belief that alcohol use is less harmful than the evidence suggests. In the illegal drug supply chain, the target and opportunity to disrupt demand or supply are less clear.
The role of the RCPE might be to concentrate on specific actions. Advocacy on all fronts for resources to support medical interventions in Primary and Secondary care is apparent. Generating collaborations and supporting research initiatives across Scottish NHS and academic institutions would bring interested groups together to generate more substantial research grants and programmes. Hosting debates and events would allow the international reach of the RCPE to inform progress. 13
A practical first step may be bringing together a group of experts to develop a consensus statement on priorities and actions for the education of the medical community. The RCPE can also take a leading role in research by convening stakeholders such as policy decision-makers, clinicians, people with lived experience and academics to establish research priorities to ensure meaningful and translatable research.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.