
Abstract
The curriculum comprises all learners’ learning experiences that enable them to achieve specific learning outcomes. The Subspeciality Stroke Medicine Curriculum is designed to train doctors in Stroke Medicine as specialists capable of providing holistic healthcare in preventing, treating and rehabilitating stroke through achieving the desired competencies. This article discusses the influence of factors like the development of learning theory, the democratisation of social process, public demand for accountability and transparency, political imperatives, economic factors and professional standards set by professional bodies on curriculum design. The curriculum focuses on an outcome-based educational approach, workplace-based assessment with formative feedback to promote learning, summative evidence for knowledge, skills and attitudes and greater integration to make learning closer to actual practice. This outcome-based, integrated approach is approved by regulating bodies as positively impacting doctors’ training and, consequently, the health of individual patients and society.
Introduction
Stroke is the fourth leading cause of death and creates long-term disabilities that pose a significant challenge for the National Health Service (NHS), 1 with a socio-economic burden of approximately £9 billion per year for care and rehabilitation. It predominantly affects older adults with multiple health issues, requiring physicians to have extensive experience and skills to manage these conditions. 2
The definition of the curriculum has evolved from a syllabus. 3 It encompasses all learning experiences that help learners achieve specific outcomes. 4 The Subspecialty Training Program for Stroke Medicine is designed for doctors (already accepted in specialist training in medicine) to gain additional skills to practice stroke medicine as a specialist. It has been developed by the Joint Royal Colleges of Physicians Training Board (JRCPTB) on behalf of the Federation of Royal Colleges of Physicians. 2 This model consists of dual training in speciality and general internal medicine (IM). The new Stroke Curriculum 2 complements the speciality curricula covering the whole stroke pathway using three capabilities in practice (CiPs) (Table 1) to produce specialists contributing to stroke care. At the end of the program, they will gain recognition recorded on the specialist register in addition to their main speciality.
Three CiPs for Stroke Medicine. 2
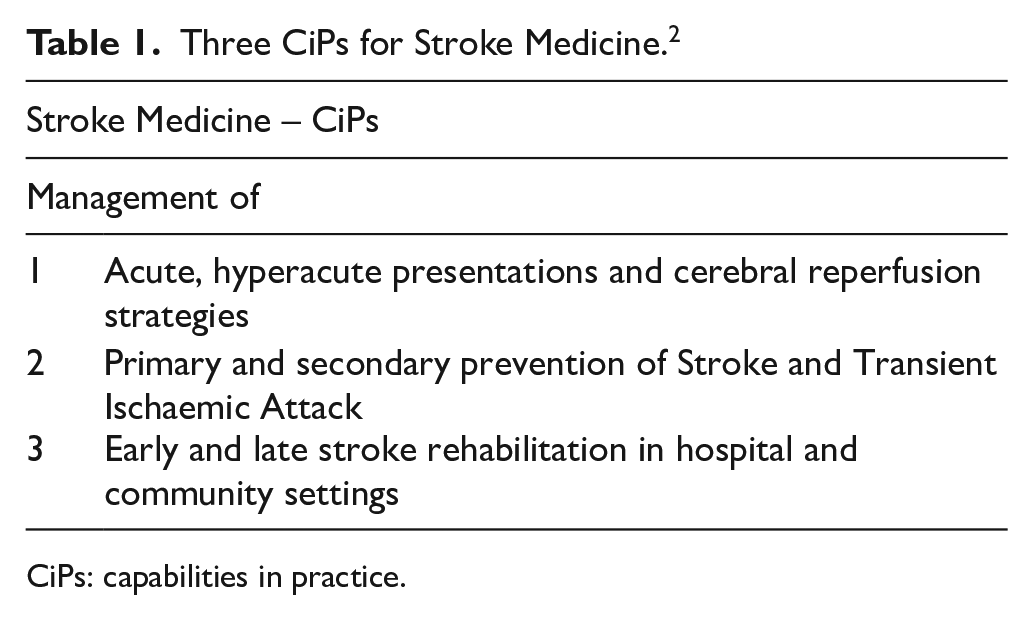
CiPs: capabilities in practice.
The Stroke Medicine Curriculum defines the program objectives, training content, supervision, assessment and appraisal requirements. 2 The curriculum emphasises the outcome-based educational (OBE) approach to produce health professionals who can practice medicine at a defined level of proficiency. 5 Therefore, it aims to train Stroke Medicine specialists capable of providing holistic healthcare to prevent, treat and rehabilitate stroke by achieving the desired competencies.
Moreover, the content and design of a curriculum can be influenced by factors such as the development of learning theory, the democratisation of social process, public demand for accountability and transparency, political imperatives and economic factors. 6 Professional standards statements by professional bodies (such as GMC UK’s Good Medical Practice) influence curriculum guidance.6,7 Therefore, Swanwick 6 argues that the choice of curriculum model and design is socially, professionally, academically and politically constructed.
An integrated approach, including generic, leadership and health inequalities competencies, to stroke training has been adapted to ensure the curriculum meets the requirements for the GMC’s Excellence by Design standards for postgraduate medical curricula. 8 Complying with professional standards is central to its design to ensure transparency and accountability, showing strong socio-political influences. These influences include the focus on OBE, integration, diversity, problem-based learning, professionalism, feedback, reflection, work-based experiential learning, community-based training, student-centred learning, assessment and evaluation. Therefore, it is clear that efforts to make it consistent with the requirements of all stakeholders and meet professional standards set up by the GMC guide the design and have educational and socio-political motives.
Curriculum models and theoretical influences
As discussed earlier, the Stroke Medicine Curriculum is an outcome/competency-based curriculum. This model, initially proposed by Tyler, 9 is based on intended goals guiding the criteria for selecting materials, outlining content and developing instructional procedures and assessment methods, whereas Mager 10 proposed instructional objectives to shift the focus of objectives to student achievement. In opposition to Tyler and Mager, 9 Eisner 11 gave the idea of problem-solving and expressive objectives. Also, the Process Model proposed by Stenhouse 12 favoured the learner-centred, outcomes-based approach by focusing on acquiring, using and evaluating the knowledge. Regarding the stroke training program, the syllabus adopts a problem-based approach to clinical scenarios encountered in clinical practice, supported by learner-centred strategies in the form of a small group, self-directed learning and assessment, feedback, reflection, support and supervision appropriate for each stage of training. Therefore, various aspects of the competency model inform its design with elements of student-centred strategies.
However, Hyland 13 criticised the competency-based approach and described it as a fusion of behavioural objectives and accountability. Swanwick, 6 in agreement with Hyland, 13 argued that increasing concern about accountability and transparency, limited resources, increased pressures on health services and managerial and political imperatives are the main drivers for competency-based curricula rather than their justification in research evidence. Although the competency-based design inclines towards an assessment-focused approach reflecting socially and politically driven motives of transparency and accountability, there are multiple opportunities in the Stroke Curriculum for teaching and learning.
The taxonomy of educational goals developed by Bloom classified the objectives into knowledge, skills and attitudes. 14 Biggs et al.’s 15 constructive alignment curriculum framework aligns the learning outcomes with the teaching and learning process and assessment. Appropriate learning activities help the learner achieve the required proficiency and thus can promote deep learning. 16 Therefore, it can be argued that including learning in the theoretical foundation of OBE broadens it. Similarly, the Stroke Curriculum adopts the modern concepts of student-centred, active and self-directed learning to make it consistent with developing personal and professional attributes.
Furthermore, the adult learning theory, originally known as andragogy, identified certain characteristics of adult learning. 17 Its three distinct features explained in literature are the adult’s interest in meaningful learning, the relevance of knowledge to its practical application and the transfer of learning. 17 Kolb 18 believed that experiential learning helps transfer learning from academic to practical. In clinical practice, this concept of meaningful learning relevance and transfer of knowledge and skills to its application in the real world (the authentic curriculum) requires higher levels of integration. The learning outcomes and educational strategies defined in the stroke curriculum promoting the transdisciplinary practice in the inpatient and community setups align with higher levels of Harden’s 3 integration ladder. It also determines its theoretical basis in adult learning theory. Therefore, the influence of adult learning theories, student-centred, active and self-directed learning is evident in the Stroke Curriculum design.
Also, an integrated curriculum has been defined in literature as the integration of once-separate courses or clinical experiences into a single unit. 19 The modern domains of health and society, professionalism and leadership require greater integration of basic and clinical sciences. 20 Recommendations for integrated curricula have been published by GMC UK and regulating bodies globally. 20 It is clear that the greater integration in the Stroke Curriculum complies with the GMC recommendations and social demands of healthcare provision in the current healthcare climate. The integration of attitudes of medical practice (professionalism, ethics, etc.) into the knowledge and skills throughout the curriculum is important. 21 Therefore, the greater emphasis on integrating knowledge, skills and attitudes in the Stroke Curriculum can positively influence all aspects of a physician’s training for practice in the real world.
Effects of hidden curriculum
Situated learning theory (learning occurs through social interaction) relates to social cognitive theory (learning occurs through interaction between the learner and the environment). 22 Trainees learn during clinical and community attachments from communication and interaction with the community, advanced learners and mentors termed as professional socialisation. 6 According to Hafferty and Franks, 23 three levels of curriculum are formal, informal and hidden. The formal curriculum is the stated curriculum, and the informal curriculum includes explicit and unexpected goals resulting from teacher and learner interaction, clinical environment, other colleagues and personal interests. Part of the informal curriculum is the hidden curriculum, which teaches values and moral judgements and is linked to institutional policies, language, assessment strategies and allocation of resources of an institution. 6 Therefore, in postgraduate stroke training, the effects of the hidden curriculum can significantly influence communication skills, professionalism, community and clinical practice.
Moreover, it is important to consider that there could be a mismatch between the intended or planned curriculum, delivered (taught) curriculum and experienced (learned) curriculum. For example, in work-based experiential learning, factors like time constraints and workload can affect the quality of training. 24 Both positive and negative aspects of the hidden curriculum have been described in the literature and usually occur through actions, discussions and relationships among the community members and are related to the concept of role-modelling. 6 Both Dewhurst 25 and Swanwick 6 agree that senior colleagues can act as role models regarding the approach to problems of the disciple, knowledge building, regard for colleagues, etc. Also, time for guided reflection is essential to ensure the positive aspects of socialisation through role-modelling and mentoring in the curriculum. 26 Reflection enhances learning through experience, critical thinking and judgement in complex situations and encourages student-centred learning, thus promoting professionalism. 27 In the Stroke Curriculum, to comply with the responsibilities of supervisors defined by the GMC, there is a focus on a selection of both educational and clinical supervisors appropriately trained for the role of providing supervision, ensuring regular appraisals, overseeing clinical work, providing constructive feedback to the trainees and a recommendation for allocating appropriate time in the job plan for it. Although the mismatch between planned, delivered and learned curricula can significantly affect work-based training, methods have been devised to overcome this problem by focusing on positive role-modelling, mentoring and allocating time for guided reflection.
Professionalism
As doctors constitute a profession that embraces trust and accountability to society, social accountability in medical education means a willingness and ability to adjust to the needs of patients and healthcare systems nationally and globally. 28 In literature, although there is disagreement on a standard definition for professionalism, both Cruess et al. 27 and Hilton and Southgate 29 described it in terms of the professional values expected of a doctor. The Royal College of Physicians UK defines professionalism as a set of values, behaviours and relationships required to maintain public trust in doctors. 30 These values include integrity, compassion, altruism, continuous improvement, excellence and teamwork. 31 Therefore, pedagogical approaches and assessments can be argued to be guided by the intended objective of acquiring a professional identity.
Concerning professional training, in the Stroke Curriculum, various opportunities are provided for trainees to meet the set professional standards. These include workplace-based training in hospitals and community, effective communication skills, teamwork in a multi-professional safe and supervised environment, self-directed and peer learning, feedback and assessment (formative and summative), interprofessional and transdisciplinary integration and leadership, competency/outcome-based approach, role modelling and reflection, diversity and research opportunities to ensure independent and safe practice. The intended outcome of professional training is to become an expert, independent and safe professional. Thus, it can be seen that the design intends to fulfil the social demands of professionalism by meeting the set standards and developing the professional identity and values to maintain public trust.
Purpose, aims and objectives
Stroke predominantly affects elderly patients with multiple comorbidities such as diabetes, cardiorespiratory conditions, cancer, dementia and other long-term problems. Therefore, physicians must have extensive medical experience and skills to manage these conditions. 2
The program’s main aim is to ensure that trainees from various clinical backgrounds develop the full range of capabilities in Stroke Medicine and can manage complex stroke patients upon completing their training. The strategy adopted for acquiring these competencies is guided by GMC UK’s framework for Good Medical Practice. 7 The curriculum includes learning objectives for specialist trainees in three main areas: acute stroke management (including thrombolysis and thrombectomy), stroke rehabilitation and stroke prevention (Table 1).
According to Harden and Laidlaw, 3 a statement of the intended learning outcomes and competencies needs to be communicated and accepted by all stakeholders. All stakeholders have input in the development process, including trainees, trainers, teachers, consultants, nurses, therapists, other multidisciplinary team members, carers and patients. Therefore, the participation of all stakeholders has been ensured, and the competencies of a stroke physician required to practice independently and safely in a multidisciplinary stroke service in a hospital or the community are communicated.
Content/Organisation of the program
Harden and Laidlaw 3 argue that for authenticity in a curriculum, the core curriculum should contain key concepts essential for the learner to master, the content should align with the desired learning outcomes, opportunities for electives should be provided and the danger of information overload should be addressed.
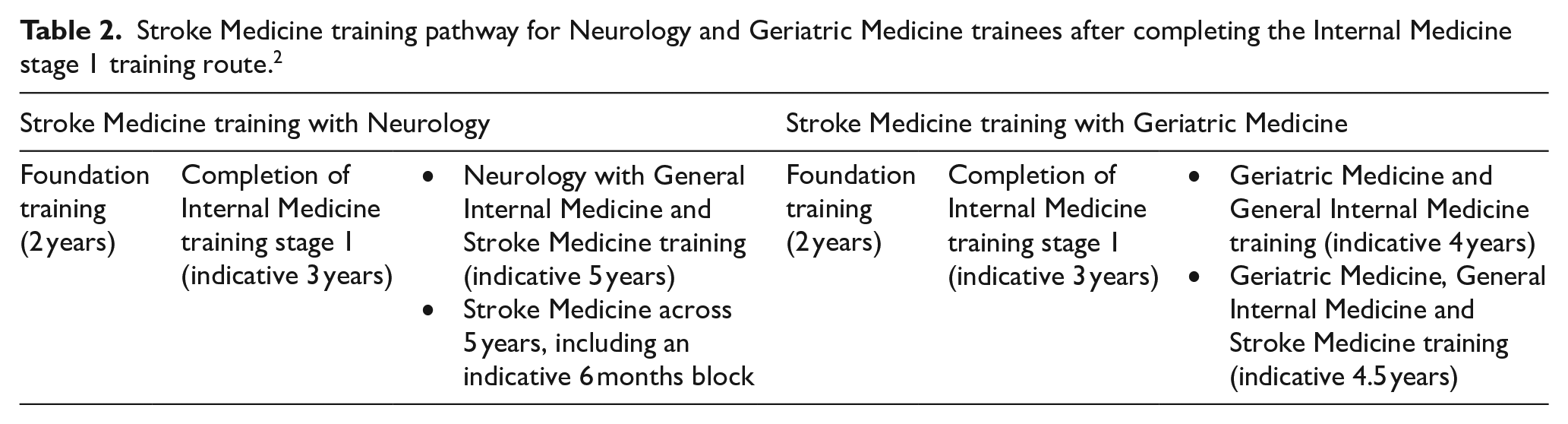
In the new curriculum, 2 doctors who have acquired basic proficiencies by completing stage 1 of IM training can undergo dedicated stroke training within the parent speciality or a standalone year of Stroke Medicine subspecialty training outside of the parent speciality. All Neurology trainees must complete stroke training as part of a 5-year Neurology and IM training program, with the flexibility of either within the program or as a dedicated subspeciality stroke training period (Table 2). Neither will extend the training. 2
Stroke Medicine training pathway for Neurology and Geriatric Medicine trainees after completing the Internal Medicine stage 1 training route. 2
The syllabus contains a variety of scenarios aimed at helping a trainee master multiple aspects of Stroke Medicine practice. There is also flexibility in pursuing special interests within Stroke Medicine, and the issue of unnecessary duplication during training has been addressed through integration between the placements. This shows that the content aligns with the program’s intended outcome.
The Stroke Curriculum can be described as a spiral curriculum. According to Harden and Laidlaw 3 in a spiral curriculum, understanding is deep through each successive experience, which builds on the previous one. Four important features of a spiral curriculum include students revisiting topics, successive levels of difficulty, new learning and skills related to prior learning and increased learners’ competence until the achievement of outcomes. 3 It is clear that trainees from various medical specialities gradually build on their knowledge and skills in Stroke Medicine. They revise topics, gradually gaining independence and responsibility in practice until they achieve full competence as stroke physicians, which is the intended learning outcome.
Teaching and learning
According to Harden and Laidlaw 3 the Student-centred learning, Problem-based learning, Integrated, Community-based, Electives, Systematic (SPICES) model is a useful tool for analysing educational strategies.
Student-centred learning
Learning should be self-directed and adjusted according to the trainee’s needs. 3 In the Stroke Curriculum, peer learning is promoted through local postgraduate teaching opportunities through small group sessions, self-help groups and learning sets formation for examination preparation. Independent, self-directed learning involves allocating time for personal development based on individual needs and choices, such as reading (web-based, journals, books), research projects and maintaining a personal portfolio (including self-assessment, reflective learning and personal development plan). This shows that the educational strategy is mainly student-centred.
Problem-based learning
The curriculum can be structured around common clinical problems as a teaching and learning strategy. 3 The syllabus consists of real practice-based cases to prepare trainees for managing stroke-related issues effectively and independently.
Integrated
Harden and Laidlaw 3 described an interprofessional approach in which various professions share their experiences to develop teamwork skills. This is achieved through work-based experiential learning opportunities and multi-disciplinary team meetings to work effectively in a multi-disciplinary stroke service. Integration has become the standard approach and is a requirement for accrediting bodies globally, including in the United Kingdom. 3 Harden’s integration ladder outlines 11 steps of integration from isolation to transdisciplinary teaching and learning. 24 The stroke training program aims to integrate new competencies for stroke specialisation with those gained in the main speciality through multidisciplinary, inter- and transdisciplinary collaboration, representing higher levels of integration on Harden’s ladder.
Community-based
Harden and Laidlaw 3 noted a shift towards a community-based learning experience. The Stroke Curriculum emphasises work-based experiential learning in a community setup to provide holistic care in hospitals and communities.
Electives
The elective component in a curriculum allows students to study topics of their choice, promoting deep learning. 3 The curriculum allows trainees to pursue specialist interests in stroke medicine. It promotes individual choices and self-directed learning to motivate learners and develop positive attitudes towards learning.
Systematic (Planned)
Teaching, learning and assessment should systematically align with clearly defined learning outcomes. 3 The trainees achieve the intended learning outcomes through various teaching and learning methods in this curriculum. This includes formal teaching and work-based experiential learning such as ward rounds, lectures and grand rounds. The clear objectives and related teaching methods in the Stroke Curriculum effectively engage adult learners in learning. Therefore, the training program reflects a student-centred approach and aligns with the intended program outcome and recommendations from accrediting and regulating bodies.
Assessment
For an assessment to be program-focused it should span over time and from multiple sources. 3 The Stroke Curriculum emphasises gathering evidence of workplace-based assessment, providing regular formative feedback and making a summative decision based on overall outcomes from multiple assessments. This approach focuses on assessing trainees throughout the training period rather than with a single assessment at one point in time.
Moreover, professionalism is a crucial skill in medical education, requiring a variety of assessment tools for evaluation. 32 The Annual Review of Competence Progressions (ARCP) in the stroke program formally monitors and records trainees’ progression. Trainees are expected to collect evidence to be reviewed by ARCP panels in their e-portfolios and complete the minimum number of assessments specified in the curriculum. These include Multi-Source Feedback (MSF), mini-Clinical Evaluation Exercise (mini-CEX), Case-Based Discussion, Patient Survey, Clinical & Educational Supervisor Reports, Audit or Research Project Supervisor Reports, Assessed Teaching Presentation and Formal Course Report or Certificate. Feedback opportunities have been incorporated as an integral part of the assessment process to aid learning.
In the curriculum, various assessment approaches are used to address the challenges in evaluating the complex competencies of a stroke specialist. For instance, MSF assesses general skills such as communication, leadership, teamwork and reliability within the domains of Good Medical Practice. MSF is considered effective and reliable for formative assessment, providing trainees with comprehensive performance data and feedback. 33 Mini-CEX is utilised to observe trainees during patient encounters to assess skills like history taking, examination and clinical reasoning. Immediate feedback is provided to facilitate learning, and Mini-CEX is considered a valid and reliable tool, 34 supported by a study comparing clinical assessment tools for trainees. 35 Patient Surveys are employed to assess interpersonal skills, communication and professionalism based on patient perceptions of the doctor’s behaviour and the consultation’s effectiveness. Thus, robust, dependable assessment approaches with feedback to support learning are used to evaluate clinical competencies and professionalism.
Additionally, the Stroke Curriculum states that supervisors are responsible for providing feedback on day-to-day performance, conducting workplace-based assessments and allowing time for appropriate training. The assessment and evaluation methods in the curriculum are carefully planned to be transparent and acceptable to all stakeholders.
Review and evaluation
Evaluation can be described as an essential quality assurance process analogous to a clinical audit. It helps the curriculum evolve according to the requirements of trainees, society and institutions. 36 Trainee feedback, ARCP outcomes, performance in membership exams and outcomes in progression to speciality training are some of the methods used in curriculum evaluation. 24 For evaluation to be transparent, feedback should be collected from students and staff at regular intervals and provided to all the stakeholders, closing the loop. 36 The Stroke Curriculum is subject to an annual review that is informed by evaluation and monitoring. Specialist Advisory Committee (SAC) receives feedback through multiple sources (such as the annual GMC trainee questionnaire, reports from the educational supervisors, program directors, postgraduate deans, trainee contact, service providers, patients and voluntary organisations). This ensures the involvement of all stakeholders and is required for the curriculum to be up to date and fit for purpose. Therefore, ensuring regular feedback and involvement of all stakeholders can be seen as a strength of the curriculum for its quality assurance.
Conclusion
In conclusion, the subspeciality Stroke Medicine Curriculum has outcome-based, integrated and spiral design features. Regulating bodies, such as GMC UK and worldwide, approve an outcome-based and integrated approach. 3 Cook et al. 37 and Frank et al. 38 argued that OBE will positively impact doctors’ training and, consequently, the health of individual patients and society. Therefore, it can be seen that an OBE and integrated approach has been adopted in the Stroke Curriculum to serve the healthcare needs of society through better training of stroke physicians and satisfy the requirements of the GMC.
Moreover, in the United Kingdom, government policy supports patient involvement in developing, delivering and managing healthcare, which is accepted as an underlying principle in healthcare reform in a patient-led National Health Service. 6 This is to ensure that the health services suit the healthcare requirements of the population and communities they serve. 39 This led to public involvement in education and training policies. 6 The GMC Standards for Medical Education require training institutions to ensure public and patient involvement through opportunities for feedback on the quality of teaching and trainee performance. 11 The public’s healthcare needs and government policy for transparency and accountability can influence curriculum design. The Stroke Curriculum focuses on Outcome-Based Education, reliable assessment methods, workplace-based assessment with formative feedback, summative evidence for knowledge and skills and greater integration with actual practice. The educational strategies in the Stroke Curriculum aim to fulfil healthcare needs, meet accrediting and regulate body requirements.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.