
Abstract

Cutaneous tuberculosis constitutes about 1.5% of all forms of extra pulmonary tuberculosis and manifests as different types like lupus vulgaris, tuberculosis verrucosa cutis (TVC), scrofuloderma, tuberculous gumma, tuberculous chancre, miliary tuberculosis, papulonecrotic tuberculid and lichen scrofulosorum. 1 Coexistence of different types of cutaneous tuberculosis is occasionally reported.2,3
A 45 year old male presented with a painless swelling over left neck and left axilla for past 2 months which later eroded to form a discharging sinuses. He also had a wart-like growth over the dorsal aspect of the right hand. He also complained of weight loss which as per history was found to be significant.
On examination, there was well defined verrucous plaque in the centre of dorsal aspect of right hand which was 4 × 2 cm in size (Figure 1(a)). He also had two indurated sinuses over left neck (Figure 1(b)) and axilla (Figure 1(c)), 3 × 2cm and 4 × 3 cm respectively with irregular margins, undermined edges, and fixed to underlying structures with discharge of a thick white coloured fluid. Two discrete, mobile, non-tender lymph nodes of 2 × 2 cm and 1 × 3 cm were noted in the left inguinal region. Chest and abdomen were normal on examination.
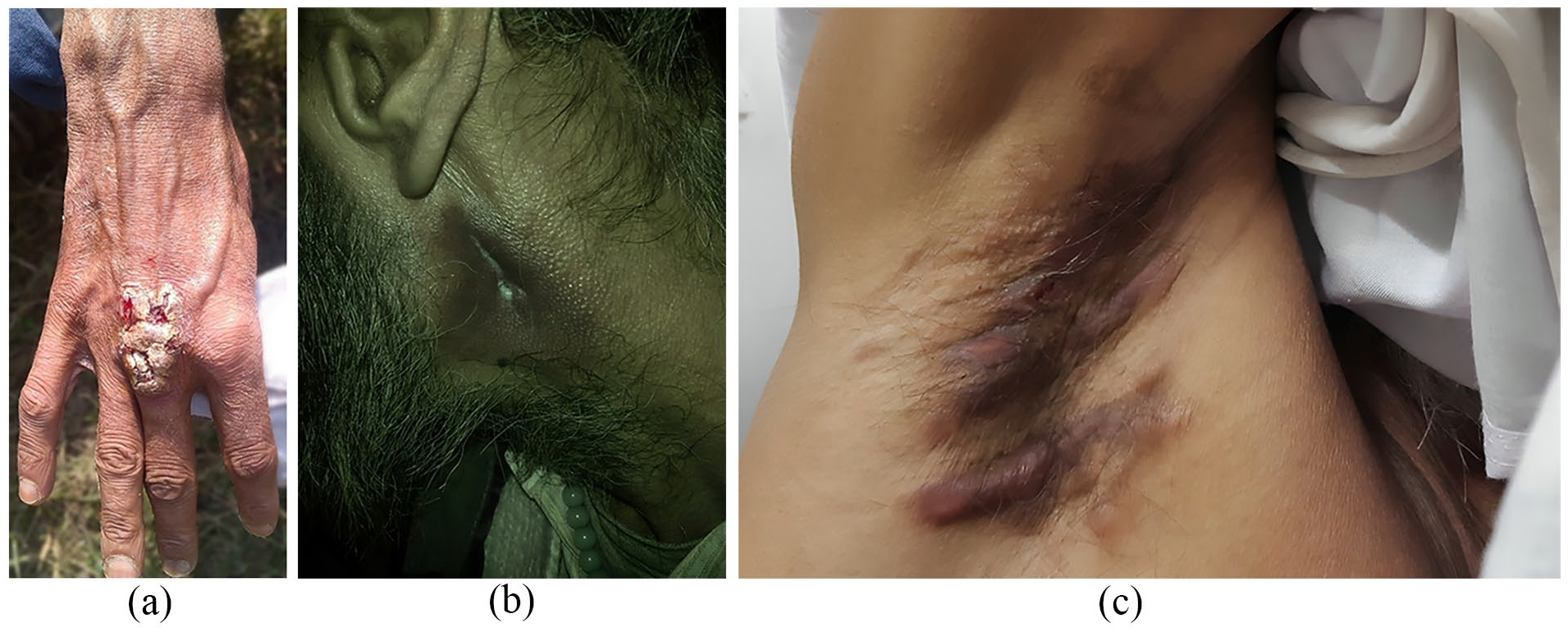
(a) Tuberculosis verrucosa cutis (TVC) – well defined verrucous plaque in the centre of dorsal aspect of right hand. (b) Scrofuloderma over the left neck. (c) Scrofuloderma in the right axilla.
Routine investigations were normal except Hb-8 gm/dl, TLC 3000 and Erythrocyte sedimentation rate (ESR) of 60. Patient turned out to be a HIV positive patient with a CD4 Count 17 cells/mm3. Mantoux test was positive with an induration of 15 mm. Sputum for Acid-fast bacilli (AFB) was negative. Fine needle aspiration cytology of left inguinal lymph nodes showed granulomatous pathology with presence of epitheloid cells and Langhans giant cells which was suggestive of tuberculosis. Chest X-ray and abdomino-pelvic ultrasonography were normal. Biopsy from the verrucous lesion on dorsal aspect of hand revealed epidermis with moderate spongiotic psoriasiform changes. Nodular tuberculoid granulomatous inflammation was seen throughout the dermis. Granuloma consisted of lymphocytes, plasma cells, histiocytes, epitheloid cells and occasional Langhan’s and foreign body giant cells (Figure 2).
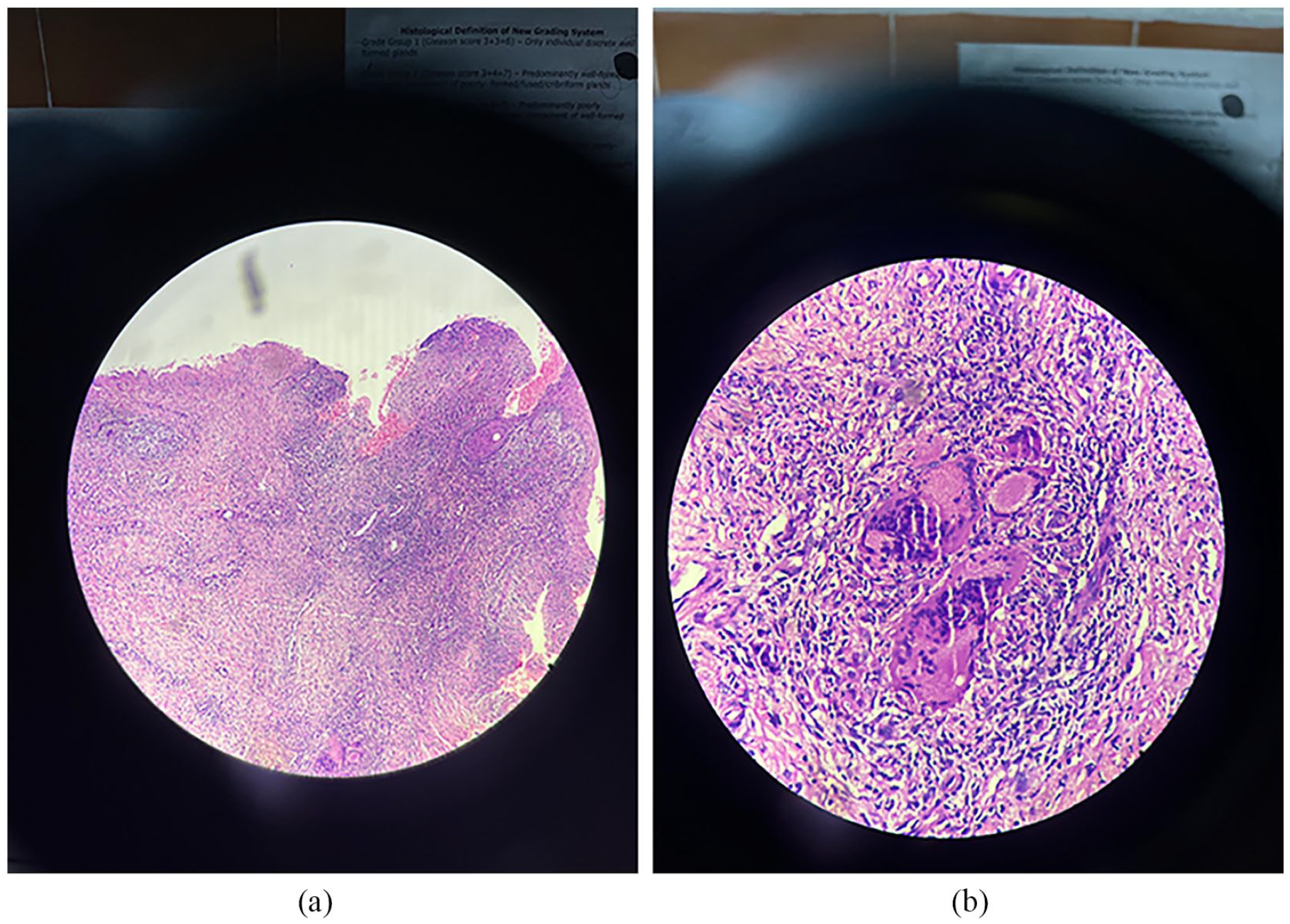
Haematoxylin and Eosin staining from the verrucous lesion on the hand revealed epidermis with moderate spongiotic psoriasiform changes (2a, 10×). Nodular tuberculoid granulomatous inflammation was seen throughout the dermis. Granuloma consisted of lymphocytes, plasma cells, histiocytes, epitheloid cells and occasional Langhan’s and foreign body giant cells (2b, 40×).
HIV infection is the greatest known risk factor for progression from latent tuberculosis infection to tuberculosis disease. 4 The risk of active tuberculosis in people co-infected with HIV and Mycobacterium tuberculos is is 3–8% per year, with a lifetime risk of 50% or more. 5
The uniqueness of our case lies in the finding that besides the presence of cutaneous tuberculosis, there can be multifocal presentation in HIV patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.