
Abstract
‘Collegiality’ comes from the Latin term ‘Collegium’, which essentially refers to a community of individuals bounded by their collective pursuit of a common goal. The concept has historical roots in both organised religion and academia, with its use subsequently extended to various industrial and corporate settings including healthcare. Nowadays, ‘collegiality’ has become a common buzzword adopted by the medical fraternity – often deemed as having a polite and respectful demeanour, maintaining cordial work relationships and being a team player who demonstrates willingness to help others and avoid speaking ill of fellow colleagues. While it is true that workplace incivility, aggression, bullying and verbal abuse are not uncommonly reported in highly stressful healthcare settings, which are concerning phenomena that should be addressed and prevented, the concept of ‘medical collegiality’ is, in reality, a rich and multi-faceted concept that is not limited to behavioural attributes, but extends to larger cultural principles and organisational constructs. In this article, we herein define ‘medical collegiality’ as ‘a collective manifestation of respect, empathy and solidarity within the medical fraternity, driven by a common pursuit of clinical excellence in patient care, demonstrated through interpersonal/work relationships and organisational culture’, by referencing historical origins of ‘collegiality’ in organised religion and academia. We further review the concept of ‘medical collegiality’ through three core lenses of cultural, behavioural and structural collegiality. Finally, we discuss the importance of medical collegiality for physician mental health and well-being, and quality of clinical care.
Introduction
‘Collegiality’ is a term that originates from the Latin word Collegium, which essentially refers to a community of individuals bonded by their collective pursuit of a common goal. 1 Its earliest usage was largely rooted in organised religion, where the Collegium Pontificum referred to a gathering of highly ranked priests in the ancient Roman Catholic church 2 and the Collegia Pietalis described gatherings of protestant Christians for prayer and Bible study. 3 In academia, the idea of ‘collegiality’ can be traced back to the traditional Oxbridge collegiate model in the United Kingdom, which comprised small, self-governing academic communities working together in a shared physical space towards a common purpose. 4
Nowadays, collegiality has likewise become a popular buzzword within the medical fraternity, which too comprises a community of clinicians, researchers and educators with common academic interests, clinical purpose and obligations and operates on self-governance. 5 Ironically, the concept of medical collegiality has hitherto remained poorly defined in literature, with a lack of consensus understanding of its core constructs, which prevents the development of concrete, actionable strategies at the individual and systemic level that can promote collegiality. At present, ‘collegiality’ has often been relegated to being merely a vague descriptor of positive physician behavioural traits that promote cordial working relationships and good teamwork,5,6 when it is, in reality, a deeper and multi-dimensional concept that comprises interpersonal behavioural attributes, cultural principles and organisational/structural constructs (Figure 1). 7
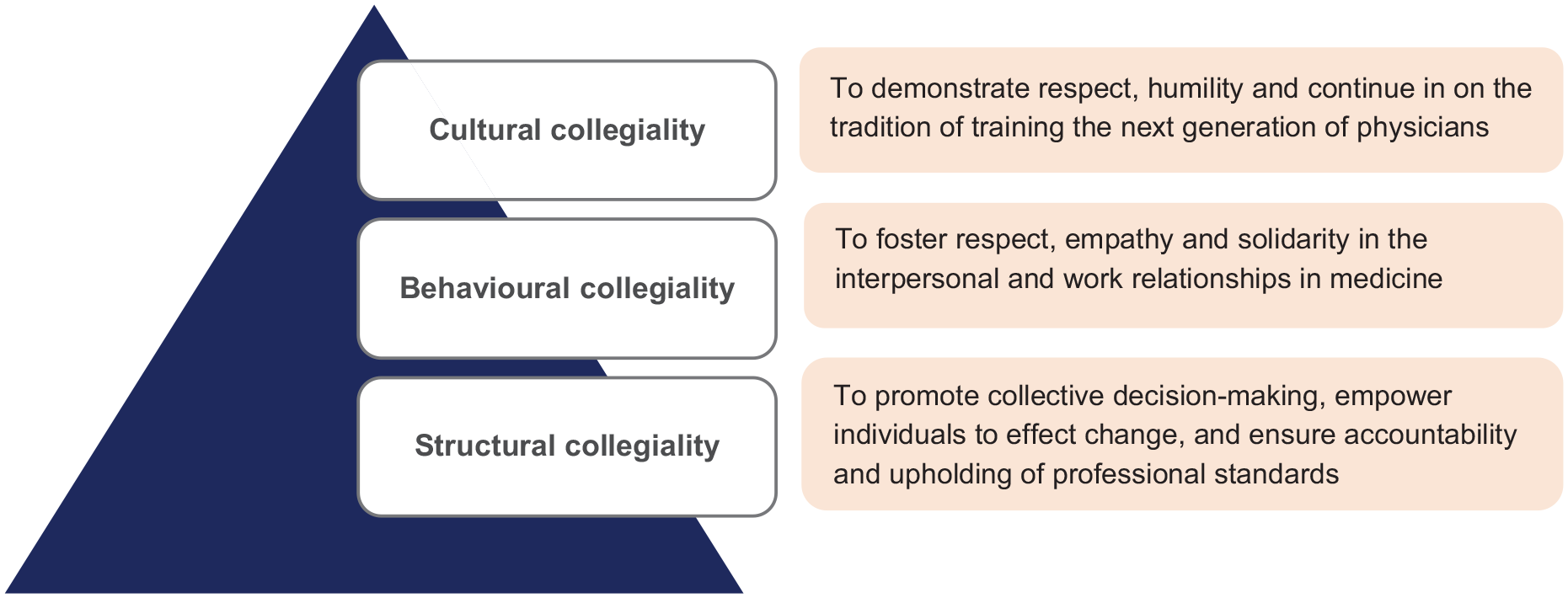
Three core components of collegiality including cultural, behavioural and structural collegiality.
In this article, we herein discuss the relevance/importance of collegiality in the medical profession and sought to establish a holistic, working definition through adopting the Bess’ model of collegiality. In addition, we elaborate on the individual components (cultural, behavioural and structural aspects) of medical collegiality and provide practical strategies for implementation, which can hopefully create a more optimal clinical environment for enhanced physician well-being and patient care.
Relevance of ‘Collegiality’ in medical practice and driving factors behind uncollegial behaviours
Firstly, uncollegial behaviours amongst medical and other healthcare professionals, such as incivility, aggression, verbal abuse/insults and bullying, are regrettably not uncommonly reported.6,8,9 This phenomenon may be contributed by heavy clinical workload, unrealistic work expectations and an overall unforgiving, harsh and pressurising clinical environment, which can lead to significant frustration, anxiety and discontentment amongst physicians that manifest as inappropriate or maladaptive behaviours.
Secondly, medicine is often seen as a highly competitive profession, in terms of clinical training opportunities and career progression, 10 research endeavours and grant applications 11 and health provider/organisational economics, 12 which perpetuates a tendency for medical trainees/practitioners to view each other as competing rivals instead of fellow colleagues in pursuit of the same professional goals. 5 In reality, this may manifest as unbecoming, unprofessional and unethical behaviours, such as refusal to share clinical knowledge, skills and learning opportunities (e.g. good clinical cases, procedures, tutorials/lectures, courses/workshops), demonstrating lack of integrity in research endeavours (e.g. ‘stealing’ research proposals or authorship positions, plagiarism) or even engaging in backstabbing behaviour and spreading of false/bad rumours about fellow colleagues.
Finally, there has often been a lack of physician empowerment, professional autonomy and shared decision-making at the systemic level that defines a collegiate model of medical practice, which may be attributed to intrinsic problems with healthcare structure and professional hierarchy. 13 In recent decades, with increasingly bureaucratic healthcare systems, government regulations, stringent requirements on electronic medical documentations, and increasingly complex technology, there has been an inadvertent loss of physician autonomy in patient care, where physicians are perceived as ‘micromanaged cogs in a machine’. 14
Bess’ model of collegiality
In 1992, Bess developed a practical three dimensional model of collegiality in higher education: cultural, behavioural and structural aspects. 7 In brief, cultural collegiality refers to shared values within a professional community, behavioural collegiality involves civil and respectful relationships between members of the community, and structural collegiality operates on the principle of shared governance at the systemic/organisational level that values democratic decision-making.7,15
Core components of ‘medical collegiality’
We herein adopt the Bess’ model 7 to describe the core components of medical collegiality, which essentially involves the presence of a shared, underlying professional purpose within the medical fraternity (cultural collegiality), that drives individual actions and interpersonal relationships (behavioural collegiality) and influences organisational governance (structural collegiality).
Cultural collegiality
Cultural collegiality in medicine refers to a deeply shared sense of common professional purpose within the medical fraternity. As outlined in the Hippocratic Oath recited by every physician, the ultimate goal of medical professionals is to provide the best possible treatment/care for the patients (or, in conventional terms, to ‘do good’ and ‘do no harm’). 16 On closer analyses of the traditional and modern versions of the Hippocratic Oath, it becomes evident that when the medical fraternity is bound by the common pursuit of excellence in patient care, it will influence their behaviour in interpersonal relationships, where medical trainees must be respectful towards their teachers, physicians should demonstrate humility in seeking help from fellow colleagues with greater expertise than them, and all practitioners should honour the tradition of training the next generation of physicians to continue their service to patients. 16
Behavioural collegiality
Behavioural collegiality describes the key attributes of interpersonal and work relationships within the medical fraternity. In a highly stressful, fast-paced and fairly unforgiving clinical environment with low margin for error, physicians often have a tendency to become highly critical, harsh and judgemental in their behaviours and may even engage in disparaging remarks or toxic shaming practices towards fellow colleagues.5,6 Such behaviour not only contributes to an unpleasant work environment that affects the mental well-being of medical professionals but also leads to ineffective healthcare communications and teamwork that have negative implications in patient care. Therefore, in our view, core behavioural attributes that demonstrate medical collegiality at the interpersonal level include respect for others, demonstrating empathy and standing in solidarity with fellow colleagues.
Firstly, ‘respect’ for others involves recognising that another person has intrinsic value and acting upon this belief. 17 In the medical community, respect for a fellow colleague is characterised by recognition of every individual’s professional capabilities and value to the healthcare team, which is demonstrated through intellectual humility in listening to others’ opinions and accepting constructive feedback. 5 In the article ‘A Call for Collegiality in Residency’, the authors argued that when we recognise that healthcare professionals in the hospital are all busy with meeting the heavy work demands for the same purpose of delivering optimal care to patients, we would then value and appreciate the unique contributions of our fellow colleagues in the provision of patient care. 18
Secondly, ‘empathy’ comes from the German word einfuhlung, (or ‘feeling into’), which necessitates self-removal from the personal context, imagining oneself in the other’s perspective, and approximating resultant cognitive and affective states. 19 When we apply empathy in our interpersonal relationships within the medical fraternity, we seek to be more understanding, less judgemental and hyper-critical, and avoid belittling the struggles faced by fellow colleagues or juniors just simply because we have ‘been through it’. To help promote empathy, open fora or smaller support groups can be created to promote open sharing of personal experiences between fellow colleagues in order to encourage and help one another in their medical journey. In 2018, Brewster and Waxman introduced the ‘K-ISBAR’ (Kindness (empathy and understanding), Introduction, Situation, Background, Assessment and Recommendation) tool for clinical handovers, to actively remind physicians to acknowledge the assistance of the receiving practitioner and to avoid engaging in harsh criticisms and judgemental behaviours towards fellow colleagues. 6
Finally, ‘solidarity’ means providing the necessary support and help to our fellow colleagues, and standing with them in situations of unfairness and injustice, even if our actions may come at a personal cost. In a 2021 philosophical paper on ‘Collegial Relationships’, the authors opined that collegial solidarity goes beyond cooperating with others to achieve a common goal, but also signals the willingness to help a fellow colleague even at personal cost due to similarities in the nature of work. 20 In practice, solidarity in medical practice may include generosity in sharing of knowledge, skills and clinical expertise with colleagues,5,21 sharing of medical information for purposes of patient care, 21 taking on additional duties and responsibilities to help one another when needed 21 and even advocating for fellow colleagues. 21 For example, in 2019, more than 4,000 doctors in Singapore signed a petition over a local medical council disciplinary tribunal ruling that imposed a maximum S$100,000 fine for failure to obtain informed consent for a routine hydrocortisone and lignocaine injection, raising concerns that the penalty was excessively punitive and could lead to defensive medicine practices with adverse downstream implications in patient care. 22 Eventually, this led to the creation of a health ministry review committee to look into professional consent taking requirements and medical council disciplinary processes. 22 The medical council was also requested by the health ministry to have the case reviewed in the judicial courts, which eventually overturned the conviction, setting a useful legal precedence for future cases regarding reasonable expectations of medical consent-taking. 22
Structural collegiality
Structural collegiality in medicine functions at a higher, systemic level, where the corporate governance of healthcare organisations should promote collective decision-making, individual empowerment to effect change, and adequate professional autonomy in medical practice, all while ensuring accountability and upholding of professional standards through effective self-governance.
Firstly, medical teams should generally adopt a transformational leadership style which emphasises interpersonal relationships, mutual respect and shared vision and is associated with enhanced work productivity, staff morale and overall job satisfaction. 23 Under such a model, individuals of the healthcare team feel that their contributions are acknowledged, opinions are valued, and they are actively empowered to partake in shared clinical decision-making for patient care. Nonetheless, in certain situations such as time-sensitive emergency settings, an autocratic leadership style might be more ideal for more efficient decision-making. 23
Secondly, at the organisational/senior management level, there must be an openness to feedback, and willingness to engage with opinions and ideas from its members, that leads to actual implementation. It is known that systemic factors such as hospital administrative support (e.g. if feedback is well received and actually implemented in practice), attitude of team leaders to their subordinates and extent of professional hierarchy significantly affect individual healthcare professionals’ willingness to speak up in clinical care. 24 To mitigate hierarchical power relationships (intra-professional (senior-junior) or interprofessional (doctors-nurses-allied health)) that often impede open communication of ideas and feedback, 13 practical strategies such as communication interventions to reframe how healthcare workers interact with one another or assignment of active roles to every member of the healthcare team can be adopted in clinical practice. 13
Lastly, structural collegiality requires the continued commitment to uphold professional standards of practice in a self-governance model, which demands individual accountability in conduct and competency. For example, to continue the collegiate model of professional self-governance, ‘qualified privilege’ compels physicians to be objective (willingness to state negative, but truthful evaluations) in providing reports of competency and behaviour of a fellow colleague during professional appraisals, malpractice or disciplinary hearings. 21
Towards a working definition of medical collegiality
Given the exposition of the multi-dimensional constructs of medical collegiality based on Bess’ model of collegiality, we herein propose a working definition of medical collegiality: ‘a collective manifestation of respect, empathy and solidarity within the medical fraternity, driven by a common pursuit of clinical excellence in patient care, demonstrated through interpersonal/work relationships and organisational culture’.
Implications of collegiality on physician well-being and patient care
Ultimately, the cultivation of medical collegiality has significant implications in both physician well-being and quality of clinical care.
Firstly, it is known that workplace conflicts and loss of professional autonomy have negative implications on physician mental health and well-being. 25 In particular, workplace conflicts with fellow colleagues, facing emotional abuse, lack of professional autonomy and recognition, and perception that the organisational management is out of touch with the ground and not receptive to employee feedback are all associated with physician burnout. 26 On the flipside, in a 2022 study of Thai medical students, the authors found that an improved perception of collegiality, achieved through instilling a greater sense of belonging to the clinical team, promoting psychological safety of the learning environment, good teamwork and peer support, was helpful to alleviate risk of burnout. 27
Secondly, healthcare collegiality leads to better clinical outcomes, work efficiency, patient safety and quality improvement by improving teamwork, care coordination, knowledge and skills sharing and collaborative decision-making.22,28 On the contrary, excessive professional hierarchy leads to fear in speaking up even in dangerous clinical situations, such as in operations, which can lead to patient harm. 29 In addition, excessive rivalry, poor relationships and distrust between physicians will inadvertently lead to inefficiency in work efforts, wastage of limited healthcare resources. 5 Finally, uncollegial behaviours such as speaking ill about fellow colleagues’ clinical skills and management in front of patients can undermine their trust in the clinicians and healthcare system. 5
Conclusion
In summary, medical collegiality is an important, multi-faceted conceptual model comprising three core components of cultural (shared pursuit of excellence in patient care), behavioural (co-dependent, respectful and civil work relationships) and structural (collectivist organisational culture) collegiality. Promoting collegiality in medical practice has important implications in physician mental health and well-being, as well as the quality of clinical care delivered to patients.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Not applicable.