
Abstract
Background:
Dengue is a major international health concern prevalent in tropical and sub-tropical countries. There are a paucity of studies on the relationship of hepatic complications with inflammatory parameters in dengue infection.
Methods:
Single-centre observational study was conducted at the tertiary care centre in North India. Patients (>12 years) diagnosed with dengue infection between August and November 2021 were enrolled in the study. The frequency of hepatic derangements and their associations with inflammatory severity was analysed.
Results:
Based on the clinical symptoms, 170 patients were classified into three categories, namely, dengue fever, warning dengue and severe dengue. Higher incidence of liver dysfunction was observed in severe dengue patients with median values of aspartate aminotransferase (AST) (3051 U/L, p < 0.001), alanine aminotransferase (ALT) (1792 U/L, p = 0.009), alkaline phosphatase (172 U/L, p = 0.001), T.Bil (34.2 µmol/L, p < 0.001), albumin (30 g/L, <0.001), and gamma-glutamyl transferase (152 U/L, p < 0.001) along with inflammatory marker C-reactive protein (CRP) (43 mg/dL, p < 0.001) highly deranged, in comparison to patients with/without warning signs. Median levels of CRP were found to be positively and significantly correlated with the median levels of AST and ALT (p < 0.05, r = 0.99) in all three categories of dengue patients. Liver injury was noted in 107 (63%) of the cohort, and mixed type of liver injury involving both hepatocellular and cholestatic patterns was observed as the most common type of injury (n = 50, 29.4%). Liver injury correlated with the severity of dengue illness as about 85% of severe dengue patients had significant liver injury (p = 0.014).
Conclusion:
In dengue patients, the association of the liver injury with inflammatory severity suggests that the mechanism of liver injury may be related to inflammatory response apart from the hepatotropic nature of the virus.
Introduction
The World Health Organisation (WHO) estimated that around 40% of the world’s population resides in dengue-endemic regions, and Asia accounts for over 70% of such cases. The estimated incidence of infections/year worldwide is around 100–400 million. 1 Dengue is endemic in India, and increased infection rate is observed following the monsoon season. Rapid urbanisation and poor hygiene are attributable to the high incidence of infection in developing nations like India.
‘Dengue’ is derived from a Swahili phrase Ka-dingapepo, meaning ‘cramp-like sensation’. It is mostly transmitted by mosquito bites with few case reports of maternal transfusion, via blood transfusion, and organ transplantation. 2 The clinical spectrum of dengue can range from undifferentiated viral illness to dengue haemorrhagic fever or dengue shock syndrome. 3 The involvement of organs such as liver, brain, central nervous system, and kidneys usually occurs in the critical phase of the infection. Currently, no specific antiviral drug effective against dengue infection is available.
A varied spectrum of liver dysfunction has been reported in dengue infection, ranging from asymptomatic enzyme derangements to fulminant liver failure resulting in high mortality. However, the commonly observed abnormality is raised transaminase levels. This is attributed to various mechanisms, which include: decreased perfusion leading to ischaemic injury, direct viral toxicity causing apoptosis of hepatocytes and immune-mediated injury. 4 In this article, we have analysed the clinical features of dengue along with the pattern of liver injury and the relation of inflammatory parameter with the clinical severity of the disease.
Methods
Study population
This single-centre retrospective observational study was conducted between August and November 2021 at our tertiary care centre in North India.
Case definition
A total of 170 individuals, aged above 12 years, diagnosed with dengue fever were recruited in the study. The diagnosis was based on clinical presentation of acute febrile illness along with typical clinical manifestations (headache, nausea, vomiting, retro-orbital pain, myalgia, arthralgia, rash, haemorrhagic manifestations, positive tourniquet test and leucopenia) and relevant epidemiological exposure with detection of viral components in serum or indirectly by serology. Dengue serology was tested either using commercially available immunochromatographic test – rapid antigen antibody detection kit, with detection of NS1 antigen and immunoglobulin M (IgM) or immunoglobulin G (IgG) antibodies or with the help of IgM antibody capture Enzyme-linked immunosorbent assay (MAC-ELISA), which is based on capturing human IgM antibodies on a microtiter plate using anti-human-IgM antibody followed by the addition of dengue virus antigens or by detecting dengue NS1 antigen by micro ELISA. The antigens used for this assay were derived from the envelope proteins of four dengue virus serotypes (DENV-1-4).
Individuals with previous history of liver disease (e.g. alcoholic liver cirrhosis, chronic viral hepatitis or malignancy), pregnant women and children <12 years of age were excluded. Duplicate results, defined as any dengue-positive test in the same individual within 7 days, were also excluded from the study.
Serology positivity was a mandatory criterion for inclusion into the study cohort.
Laboratory investigations
Liver function tests (LFTs) and inflammatory marker (C-reactive protein [CRP]) were assessed in Random Access Autoanalyser, Roche Cobas 8000, Roche Diagnostics International Ltd (Roche Diagnostics), Switzerland and the following parameters were measured: aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), gamma-glutamyl transferase (GGT), total bilirubin, total protein and albumin. Abnormality in liver tests was defined as: ALT >40 U/L, AST >40 U/L, ALP >128 U/L, GGT >61 U/L, T.Bil >20.52 µmol/L, total protein <65 g/L and albumin <34 g/L.
Leucopenia and leucocytosis were defined by counts <4 × 109/L and >11 × 109/L.
Liver injury was classified into three categories: Elevations of LFTs were considered to amount to liver injury in the context of documented dengue if AST/ALT >3 × ULN (upper limit normal) and ALP or GGT >2 × ULN. Liver tests’ abnormalities not amounting to injury were defined by AST >40 U/L, ALT >40 U/L, ALP >128 U/L, GGT >61 U/L, and total bilirubin >20.52 µmol/L at any time point during hospitalisation. The type of injury was further classified into hepatocellular (AST/ALT >3 × ULN), cholestatic (ALP/GGT >2 × ULN), or mixed type (both AST/ALT >3 × ULN and ALP/GGT >2 × ULN). 5 Increase in inflammatory markers was defined by CRP >5 mg/dL.
Data on demographics (age at diagnosis, gender), symptomatology, signs and results of the initial laboratory tests, including liver function and inflammatory markers of 170 patients, were retrieved from the electronic medical records of the hospital after ethical approval by the Institutional Ethical Review Committee of our institution (No: NK/8014/Study/541 dated 10/12/21). In cases where multiple results were found for a single patient, the earliest result was recorded.
Statistical analyses
All values were expressed as the mean ± standard deviation or median with a range depending on their distribution about the mean. Discrete variables were described as frequency (n) and percentage (%). Assessment of normality of distribution was undertaken using the D’Agostino test. Continuous variables were compared with the Student’s t-test, analysis of variance, or non-parametric tests like Mann–Whitney U or Wilcoxon’s test. Chi-square or Fisher exact test was used to determine the differences between the categorical variables. A p < 0.05 was considered statistically significant. Analyses were performed using SPSS version 23.0 for Windows (SPSS Inc., Chicago, IL, USA). Pearson correlation analyses were performed using GraphPad Prism software version 5 (GraphPad Software, USA).
Results
Clinical presentation and correlation with inflammation
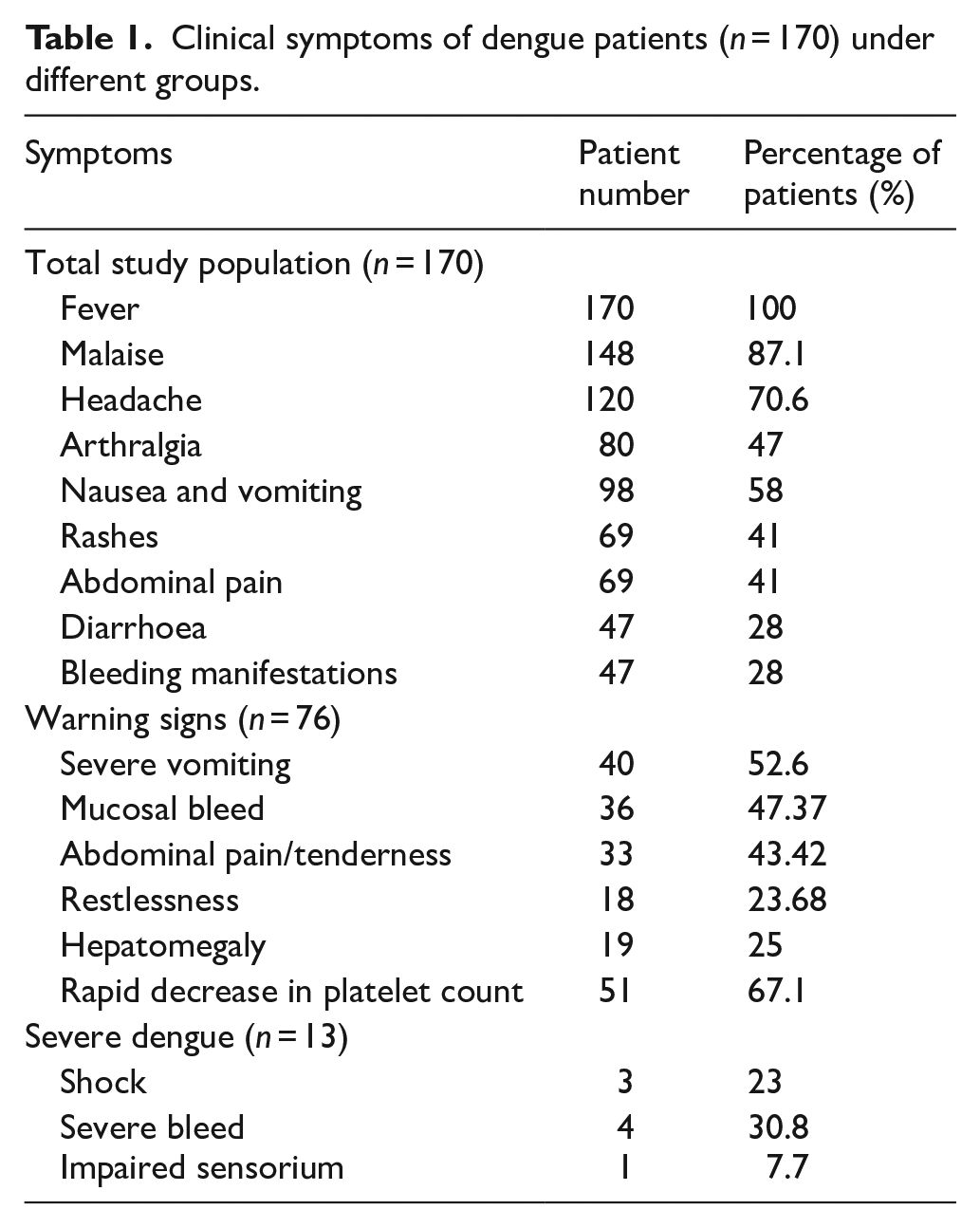
A total of 170 serologically diagnosed dengue patients with acute febrile illness were recruited in our study and their liver function was assessed. This included 100 male and 70 female patients with the median age being 30 (21–45.8) and 33.5 (25–47.3) years, respectively. The maximum frequency of dengue cases was observed in the most mobile and active group of the population, that is, 21–35 years (Figure 1). The most common symptoms at presentation were fever (170, 100%) followed by malaise (148, 87.1%). Others included headache (120, 70.6%), arthralgia (80, 47%), nausea and vomiting (98, 58%), rashes (69, 41%), abdominal pain (69, 41%), diarrhoea (47, 28%) and bleeding manifestations (47, 28%) (Table 1). Almost 70% (n = 121) of patients had platelet counts <100 × 109/L at some point of time during their hospital stay. About 52 patients (30.6%) had leucopenia, while 26 (15.1%) had leucocytosis at presentation. The cohort was divided into three categories based on WHO Guidelines 3 : dengue fever, warning dengue and severe dengue, wherein 81 (47.64%) patients presented with only fever, 76 (44.70%) patients were found to have warning signs which included severe vomiting (n = 40, 52.63%), mucosal bleed (n = 36, 47.37%), abdominal pain/tenderness (n = 33, 43.42%), restlessness (n = 18, 23.68%), hepatomegaly (n = 19, 25%) and rapid decrease of platelet count (n = 51, 67.11%) and 13 individuals (7.65%) had severe dengue evidenced by shock (n = 3, 23%), severe bleed (n = 4, 30.78%), severe organ involvement with AST/ALT>1000U/L (n = 12, 92.31%), impaired sensorium (n = 1, 7.69%) and organ failure (n = 2, 15.38%). Around 34.11% (n = 58) of the individuals had thrombocytopenia with platelet count <20 × 109/L. Shock was noted only in three individuals and was associated with 67% mortality.
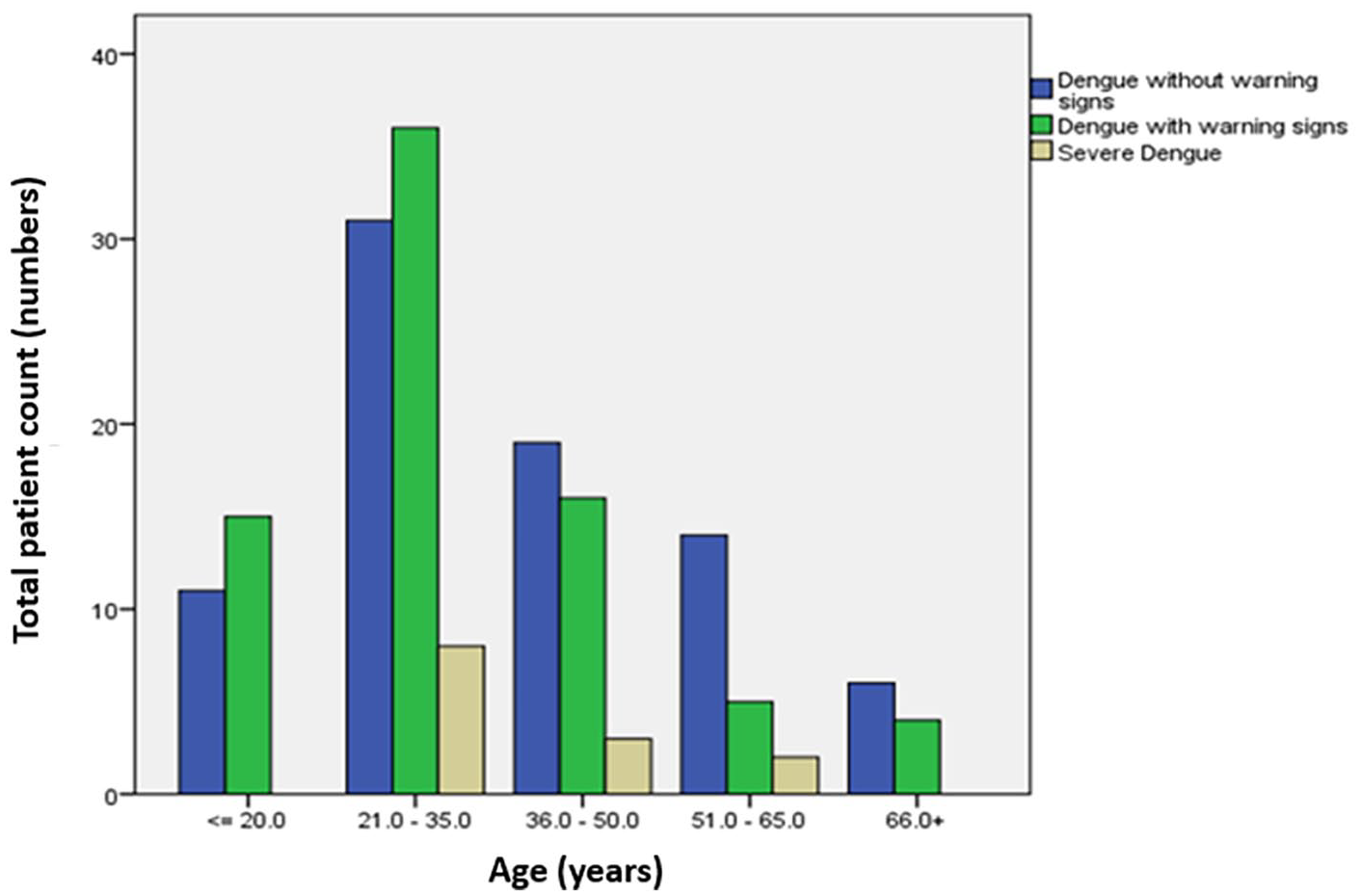
Clustered bar diagram depicting the frequency of dengue cases of varying severity among the varied age groups.
Clinical symptoms of dengue patients (n = 170) under different groups.
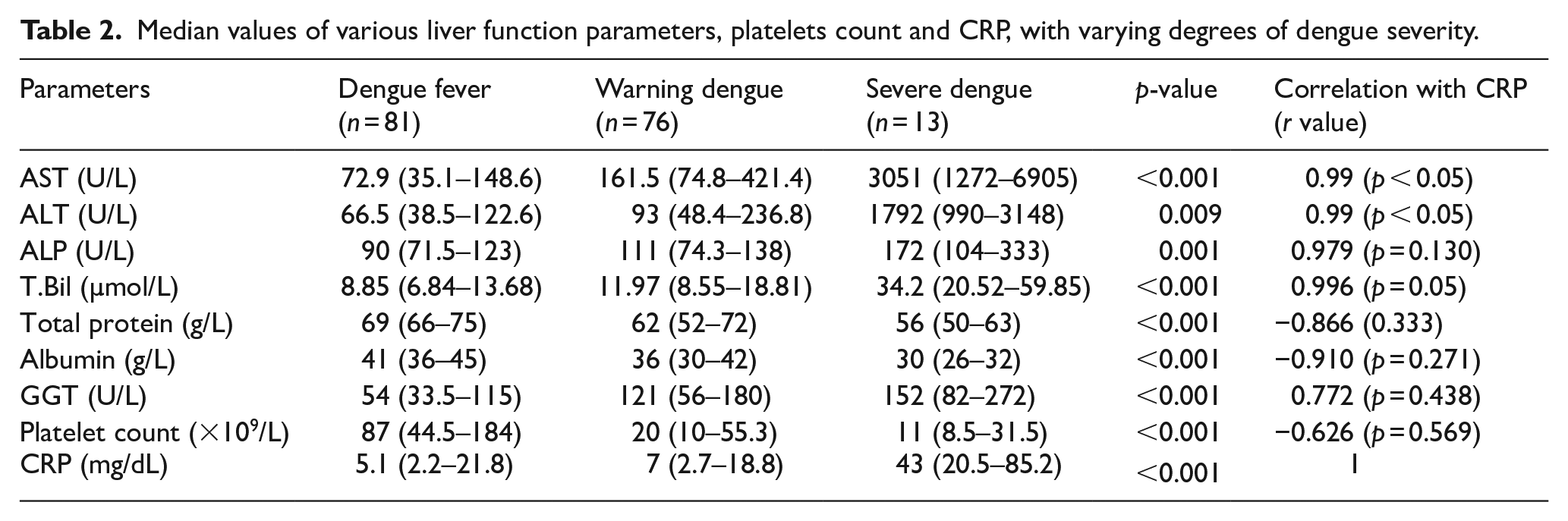
CRP was found to be elevated (>5 mg/dL) in a total of 101 individuals (58.7%). The median value of CRP among those with dengue fever v/s those with warning signs and severe dengue was 5.1 (2.2–21.8) mg/dL, 7 (2.7–18.8) mg/dL and 43 (20.5–85.2) mg/dL respectively (Table 2). Elevated CRP (>5 mg/dL), thus had a significant association with the severity of dengue illness with p = 0.001. Among the various liver function parameters studied, the median levels of AST and ALT were found to be positively and significantly correlated (r = 0.99, p < 0.05) with the levels of CRP in all three categories (Table 2).
Median values of various liver function parameters, platelets count and CRP, with varying degrees of dengue severity.
Biochemical analysis of liver function parameters
While assessing the liver function abnormalities in the patients, only 19 individuals had completely normal liver function parameters accounting for 11.2% of the study population while the rest manifested derangement in LFT parameters. One hundred and seven individuals were found to have liver injury (63%), which was further classified into the hepatocellular, cholestatic or mixed type. It was noted that while 41 individuals (24%) had hepatocellular type of injury with AST/ALT ⩾3 × ULN, 16 (9.4%) individuals had cholestatic pattern with ALP or GGT ⩾2 × ULN. Interestingly, the majority had the mixed type injury involving 50 individuals (29.4%) where both ALP/GGT and AST/ALT were deranged. Out of the remaining 63 individuals with no evidence of liver injury, 44 were found to have abnormal liver function though not severe enough to fit into the definition of liver injury (i.e. AST/ALT>ULN to <3 × ULN and ALP/GGT >ULN to <2 × ULN). The mean value of AST and ALT in those with significant liver injury was 188.3 (133–480.5) and 135 (87–304.3) U/L, respectively. Thus, the mean value of AST was higher than ALT. ALP was significantly elevated only in 14 individuals (8%), and GGT was found to be significantly elevated in 63 individuals (37%), signifying its higher sensitivity. Hepatomegaly was found in a total of 24 individuals accounting for 14% of the study population. Hyperbilirubinemia was observed in 31 (18.2%) of the patients.
The median age of patients with significant liver injury was 34 (23–47) years, while the median age of those without liver injury was 27 (22–45) years. This, however, was not clinically significant (p = 0.105). Among male and female populations, the distribution of liver injury was uniform, with 61% and 65.7% of individuals being found to have liver injury respectively (p = 0.82) and the percentage of hepatocellular, cholestatic and mixed injury also remained equal among the two groups (Figure 2). The clinical features observed in patients with significant hepatic involvement were abdominal pain (36%), nausea/vomiting (56%), anorexia (42%) and diarrhoea (27%). Hypoalbuminemia was noted in 57 patients accounting for 33.5% of our cohort and hypoproteinemia was noted in 74 (43.5%) patients.
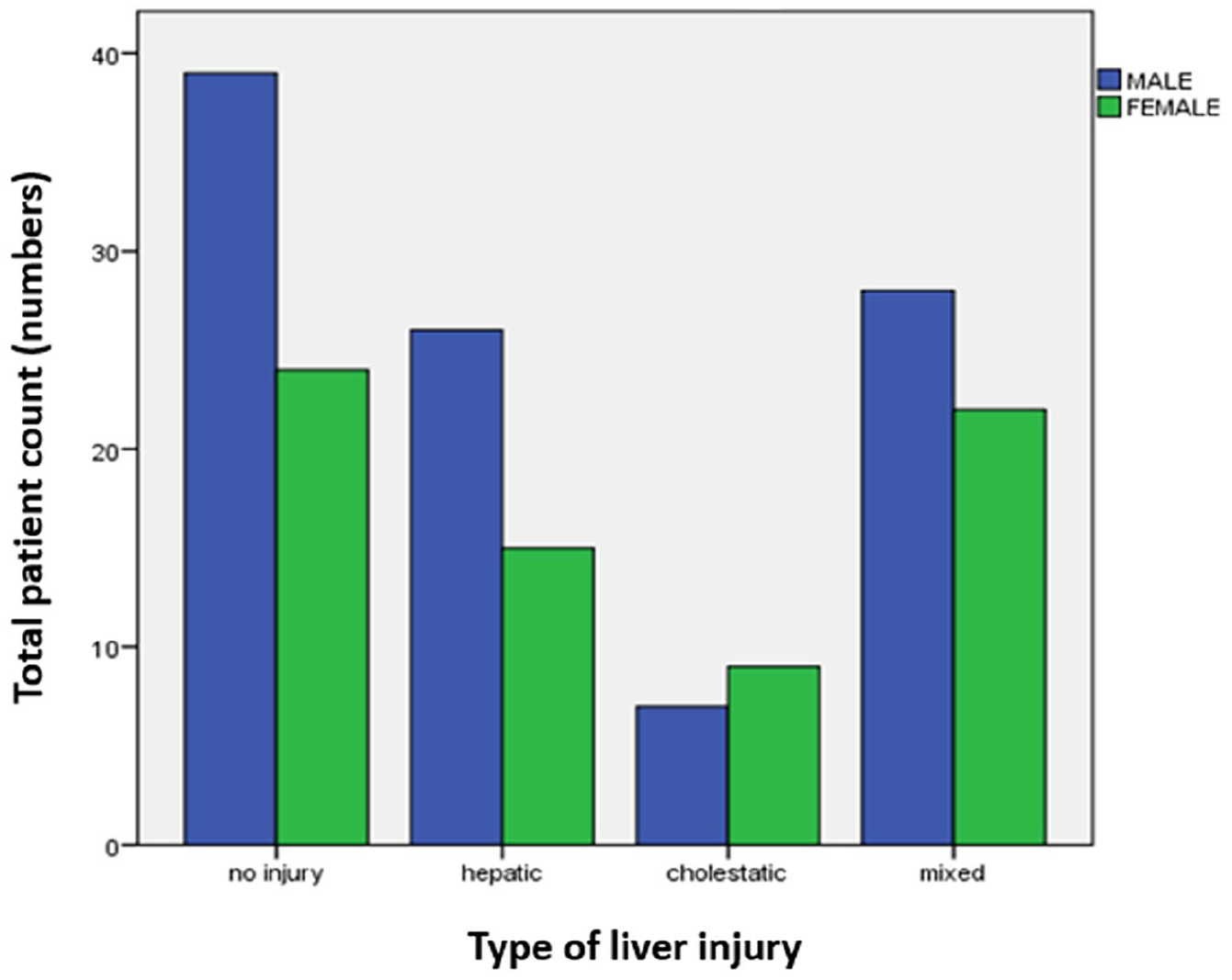
Gender-wise frequency of different types of liver injury depicting mixed-type liver injury being the most common.
The median platelet count significantly varied across the different spectrum of liver injury. In patients without liver injury, the observed median platelet count was 156 × 109 (86 × 109–204 × 109)/L, in patients with mild enzyme abnormalities, the value was 86 × 109 (34.2 × 109–184 × 109)/L and in patients with significant liver injury, the median count was 29 × 109 (11 × 109–71 × 109)/L with p ⩽ 0.05.
Severe dengue had an overall higher incidence of liver dysfunction (Table 2). The median values of AST (3051 U/L, p < 0.001), ALT (1792 U/L, p = 0.009), ALP (172 U/L, p = 0.001), T.Bil (34.2 µmol/L, p < 0.001), albumin (30 g/L, <0.001) and GGT (152 U/L, p < 0.001) were significantly deranged in severe dengue group in comparison to patients with/without warning signs. Plasma leakage secondary to increased vascular permeability seen as a feature of severe dengue clinically characterised by third space fluid collection and shock was also found to be more prevalent in those with significant liver injury (p ⩽ 0.05), that is, 46 individuals out of 70 with third space fluid collection had significant liver injury. Hepatomegaly also correlated positively with liver dysfunction among dengue patients (p = 0.006).
Discussion
The present study on Indian adults and adolescents captures the liver function derangements in dengue patients. The study was carried out in 170 dengue-positive patients of both genders. Based on the clinical presentation, the prevalence of dengue fever without warning signs (n = 81, 47.6%) was greater than those with warning signs (n = 76, 44.7%) or severe dengue (n = 13, 7.6%). Liver injury was noted in 63% of the cohort (n = 107) and mixed type of liver injury involving both hepatocellular and cholestatic patterns was found to be more prevalent (n = 50, 29.4%). Liver injury correlated with the severity of dengue illness with almost 85% of those with severe dengue (n = 11) having significant liver injury (p = 0.014). Inflammatory marker CRP was found to correlate with the severity of dengue illness with the median value in those with severe dengue being 43 (20.5–85.2) mg/dL as compared to 5.1 (2.2–21.8) in dengue without warning signs (p ⩽ 0.001).
Several studies have shown that liver dysfunction in dengue illness can be attributed to direct viral toxicity, hypoxic injury secondary to hypoperfusion, and immune-mediated damage. 4 While asymptomatic derangement of LFTs is noted to be a frequent finding, rare cases of acute liver cell failure have also been reported.6 –8 Biopsy studies have revealed microvesicular steatosis, liver cell necrosis, councilman bodies, and portal tract inflammation to be present in such cases. 9 In our study, the median AST and ALT values were greater in those with severe dengue (3,051 and 1,792 U/L, respectively) than for classical dengue fever with no warning signs (72.9 and 66.5 U/L, respectively). This is in accordance with the study by Kuo et al. 10 and suggests the correlation between increased transaminase levels with disease severity. Also, in both classical dengue fever and severe dengue, AST was found to be higher than ALT. This reversal of AST:ALT ratio was not seen in other viral infections including infection with HAV, HBV, HCV, etc., but was observed in cases of alcoholic hepatitis.11,12 Hence, with the concurrent presence of thrombocytopenia, fever, and icterus, it acts as a differentiating clue from other viral hepatitis mimics. 13 However, since AST is produced from other sources apart from the liver such as the heart, striated muscle, and erythrocytes, the increased value noted in dengue fever may not be a true reflection of hepatic involvement. Previous studies have shown that elevations in AST/ALT although significant in severe disease did not affect the outcome including mortality. 14 In our study, the median platelet count was observed to be significantly low in those with liver injury (p < 0.001), and similar observation has been previously reported by Swami et al. 15 As dengue infection is associated with thrombocytopenia and bleeding diathesis, there is a possibility that liver injury may accelerate the disease progression as liver is the major source of prothrombin and vitamin K, which are required in the clotting cascade mechanism.
Liver dysfunction has been studied previously in dengue patients, but the pattern of liver involvement and liver injury has not been described. In our study, we have defined and classified liver injury into hepatocellular, cholestatic, and mixed type of injury, 5 with the latter type being most common. GGT was found to have better sensitivity than ALP for assessing cholestatic liver injury and similar findings were observed in COVID-19-associated hepatic complications. 16 Hyperbilirubinemia was found in 18.2% (n = 31), which is likely secondary to biliary stasis and was significantly elevated in severe dengue patients compared to those with dengue fever without warning signs (p ⩽ 0.001). Bauer et al. observed bilirubin to be a more accurate predictor of liver injury than ALT in acute liver diseases. 17 Patients with liver injury had significant elevation of bilirubin compared to those with no injury, thus emphasising the pathology of cholestasis in dengue-associated liver injury.
Hypoproteinemia and hypoalbuminemia were noted in n = 74 (43.5%) and n = 57 (33.5%) of our cohort, respectively. Hypoalbuminemia correlated with the severity of dengue illness with significantly low levels in those with severe dengue with a median value of 30 g/L in comparison to 36 g/L in warning dengue and 41 g/L in dengue fever. This result is in concordance with previous studies.4,15 Hypoalbuminemia in severe dengue is attributed to increased vascular permeability and proteinuria, as a component of hepatic dysfunction or as a negative acute-phase reactant in acute illnesses. Thus, albumin levels could be a prognostic marker for dengue severity. Hypoalbuminemia and hypoproteinemia were also correlated with liver dysfunction with significantly decreased levels noted in those with liver injury compared to those with no injury (p ⩽ 0.001). This could suggest the possible down-regulation of albumin synthesis from the liver due to inflammation apart from the increased vascular permeability and proteinuria.
The role of inflammatory markers has been minimally explored in dengue infection. Liver produces CRP, which is an acute phase reactant in response to any infection or inflammation, and elevated CRP levels are found to be associated with both bacterial and viral infections. 18 We observed, in our study, a positive correlation between the increase in CRP with both liver function parameters and dengue severity with the median values of CRP in dengue fever without warning signs being 5.1 mg/dL and those with severe dengue being 43 mg/dL, substantiating that CRP could be a potential biomarker for severe dengue. 19
Our study had few limitations such as the lack of serial testing (which may have missed the highest peaks of derangements) and the lack of liver biopsy to confirm and correlate with histological changes, and it is a single-centre study. On the other hand, there are several strengths, including representation of all severities of dengue fever, and correlation with inflammatory parameters providing insights into the genesis of dengue hepatopathy.
To conclude, hepatic derangements are common in dengue and may be related to the inflammatory responses in dengue fever.
What is already known on the topic?
Liver dysfunction has been reported in dengue infection ranging from asymptomatic enzyme derangements to fulminant liver failure with the commonest abnormality noted being raised transaminases levels.
Liver dysfunction in dengue illness has been attributed to direct viral toxicity, hypoxic injury secondary to hypoperfusion and immune-mediated damage.
What this study adds?
In our study, the variation in LFTs along with inflammatory parameter was compared among the varied severity of dengue illness based on the clinical presentations. In conjunction, the extent of liver dysfunction was assessed by the types of liver injury in relation to the levels of the liver function parameters.
Liver injury was noted in 63% of the cohort, and mixed type of liver injury (hepatocellular and cholestatic pattern) was most common type. There was significant correlation between liver injury and clinical severity of dengue illness.
Significant positive correlation was observed between inflammatory marker and severity of dengue illness.
How this study might affect research, practice and policy?
Liver injury may be one of the common complications of dengue infection.
Elevated transaminase, GGT, hyperbilirubinemia, hypoproteinemia, hypoalbuminemia along with raised CRP levels could be used as potential biochemical markers in dengue patients to detect and monitor hepatic dysfunction
Footnotes
Author’s contribution
Ritin Mohindra and Divyashree K did the data analysis, statistical analysis, graphs preparation and drafted the manuscript. Vikas Suri and Ashish Behera provided the clinical samples for the study. Madhur Kalyan, Ishani Bora, and Roop Kishore Soni participated in data acquisition and analysis. Vishal Sharma and Neha Saini contributed to supervision, accuracy and editing of the manuscript. Deepy Zohmangaihi conceived, designed and analysed the study and created the final version of the manuscript. All authors reviewed and approved the final version of manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Institutional Ethics Review Board Reference No: NK/8014/Study/541 dated 10/12/21.