
Abstract
Insulin injections have never been an entirely satisfactory therapy, and as a result a continuing ‘biobetter’ technological cascade has driven changes in purity and manufacture, in structure and excipients, and in administration devices. The resulting deck of insulin preparations has to be matched by health-care teams and users with individual need. This latter is itself a complex ranging from ambulatory care in type 1 and type 2 diabetes, the topic generally addressed by guidelines and funding advice, to in-patient care and the newly diagnosed, plus secondary diabetes with very different effects on insulin need, through to co-morbidities and medications interfering with glucose metabolism. In this article the match of different clinical scenarios to the available insulins is discussed in the context of available evidence, quality guidelines, and diabetes best practice. Additionally the role of biosimilars of the insulin analogues is addressed, their limited but useful price advantage, and the management consequences of substitution for the originator product.
Background
Insulin therapy now has a history of over 100 years’ duration, over which it has often been at the forefront of basic medical and applied research, as exemplified by its relation to no less than six Nobel prize winners.1,2 And yet it remains highly problematic, with a therapeutic ratio in type 1 diabetes mellitus (T1DM; dose for hypoglycaemia:dose for normoglycaemia) being well below 1.0 and perhaps <0.5. Further there are few medications for which the dose range within the target population is so large, ranging from 10 to 250 U/day between individuals, thus requiring dose titration burdensome to both the user with diabetes and their medical advisors. Indeed, within individuals, when under conditions of metabolic stress (e.g. as a sick in-patient) dose requirement can vary similarly, and change critically in a matter of hours.
Each major technological advance in marketed insulin preparations has added cost, and often been adopted with delay by the market. These advances may be described as ‘biobetters’, for the underlying molecule remains essentially the same mandated by the conformation(s) required to activate the insulin receptor, and the need to avoid immunological insulin resistance (neutralising antibodies), in a hormone which is essential to life (Table 1). The term ‘biobetters’ can be applied to other biological medicines too, but is not so restricted to a natural molecular conformation; an example being humanised TNF-α blockers engineered to elicit reduced inflammatory responses. For insulin, biobetters appeared early in its therapeutic history over its first 50 years. 1 Firstly came higher purity through the use of recrystallisation, then extended-acting insulins of which NPH insulin is still in widespread use today, then highly purified insulin which essentially abolished injection site lipoatrophy, immunological insulin resistance and immunological neonatal hypoglycaemia (Figure 1). After 60 years, in the early 1980s, insulin was the first medication to benefit from new DNA-based manufacturing techniques, and thus ‘human’ insulin could replace slaughterhouse pancreatic insulin. But this technology also set the scene for designer insulins, both meal-time and basal analogues of human insulin, 3 and it is the continuing developments in this area and their practical application we discuss here.
Definitions and intent of biobetter and biosimilar medicines.
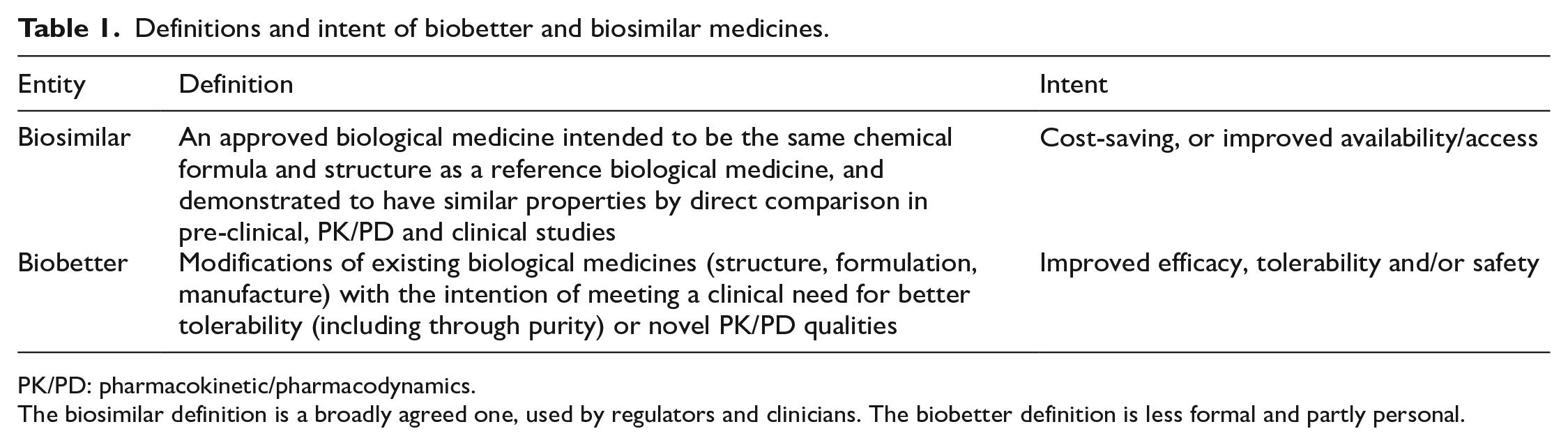
PK/PD: pharmacokinetic/pharmacodynamics.
The biosimilar definition is a broadly agreed one, used by regulators and clinicians. The biobetter definition is less formal and partly personal.
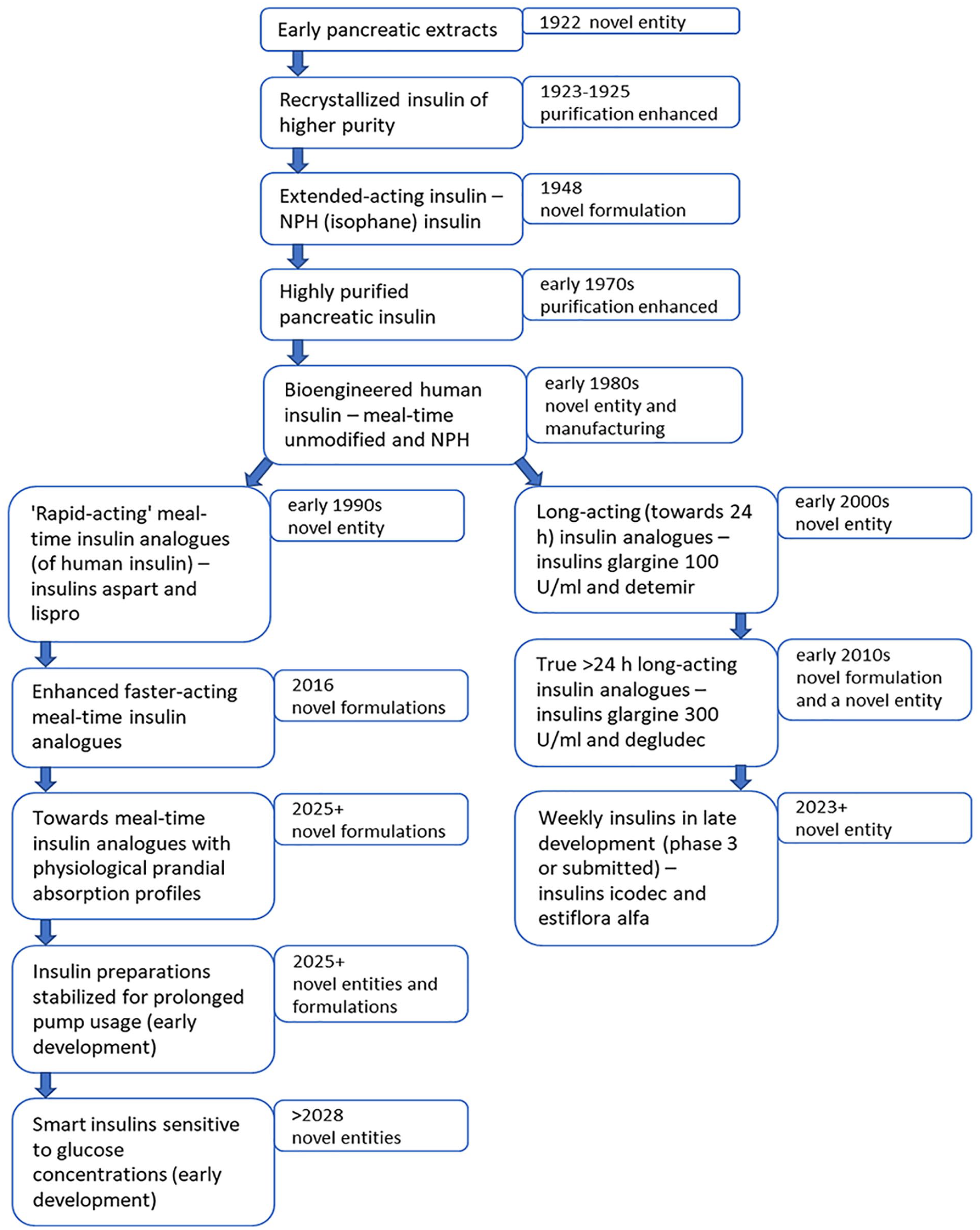
Biobetter insulin: outline of the major steps in the enhancement of the clinical properties of insulin medications, 1922–2023 and beyond.
With the expiry of patents of the original designer insulins, attempts to imitate these at lower market cost have happily followed. The development process here differs from that of generic versions of small molecule drugs, and these ‘biosimilars’ have spawned a new regulatory framework over the past 8 years. 4 Insulin, growth hormone, erythropoietin and anti-TNFs have benefitted, as well as also most recently monoclonal antibodies to treat wet macular degeneration. But insulin is unusual, not just in its dosing characteristics (as above), but also because its pharmacokinetic (PK, plasma concentration) time-profile is critical, largely because of immediacy of action with a circulating half-life of just 5 min. 5 Accordingly, the PK and pharmacodynamic (PD) profiles of any proposed biosimilar have to be established to be very close to the original reference preparation, 4 while the technique involved to assess this (the ‘glucose clamp’) is only available in a handful of clinical laboratories worldwide.
Biosimilar insulins suffer from another issue. As noted above, tolerability of insulin is very poor, due to hypoglycaemia being usual if effective glucose control is to be maintained. This side effect is very variable, but, when defined as <3.0 mmol/l, the median is about once a month in people with T1DM, 6 and lower but very dependent on insulin regimen in type 2 diabetes (T2DM). 7 It is however also highly erratic and unpredictable, both between and within individuals, largely due to the vagaries of subcutaneous insulin absorption. As a result, users often develop a love-hate dependence on their named insulins, and can be destabilised psychologically by any switch in insulin types. 8 Accordingly, switching between insulins, even to a biosimilar, has to be managed carefully, and interchangeability (medication substitution by a pharmacist) can be highly problematic.
Data sources
The insulin therapy literature consists of many tens of thousands of papers, and covers the many different insulin preparations discussed in this paper, and others. For new insulins developed in the last 30 years, a limited randomised control trial (RCT) database is available, this nucleus of papers being well documented in many reviews and commentaries. These have been the source of formal guidelines from the likes of the National Institute for Health and Care Excellence (NICE, England and Wales),9,10 formal recommendations from the Scottish Medicines Consortium (SMC), 11 and many consensus reports from professional and patient associations including, for example, the European Association for the Study of Diabetes and the American Diabetes Association jointly. 12 The current author has a long familiarity with the published papers and guidelines, having been a participant in many.
However there is a large issue here, namely that the RCTs generally only address a well-defined, but limited area of practice, such as people with T1DM already on therapy or people with T2DM starting insulin. This leaves a very large part of diabetes practice with insulin without a formal RCT evidence-base (Table 2), as will be clear below. This gap is filled here by extrapolating the RCT evidence beyond the populations of study, while using other evidence (PK/PD, observational) in a logical fashion to inform the other clinical scenarios. Mechanistic evidence is generally only used for illustrative purposes, while pharmacoepidemiological (‘real-world’) evidence for insulin is generally flawed.
Scenarios in the clinical use of insulin.
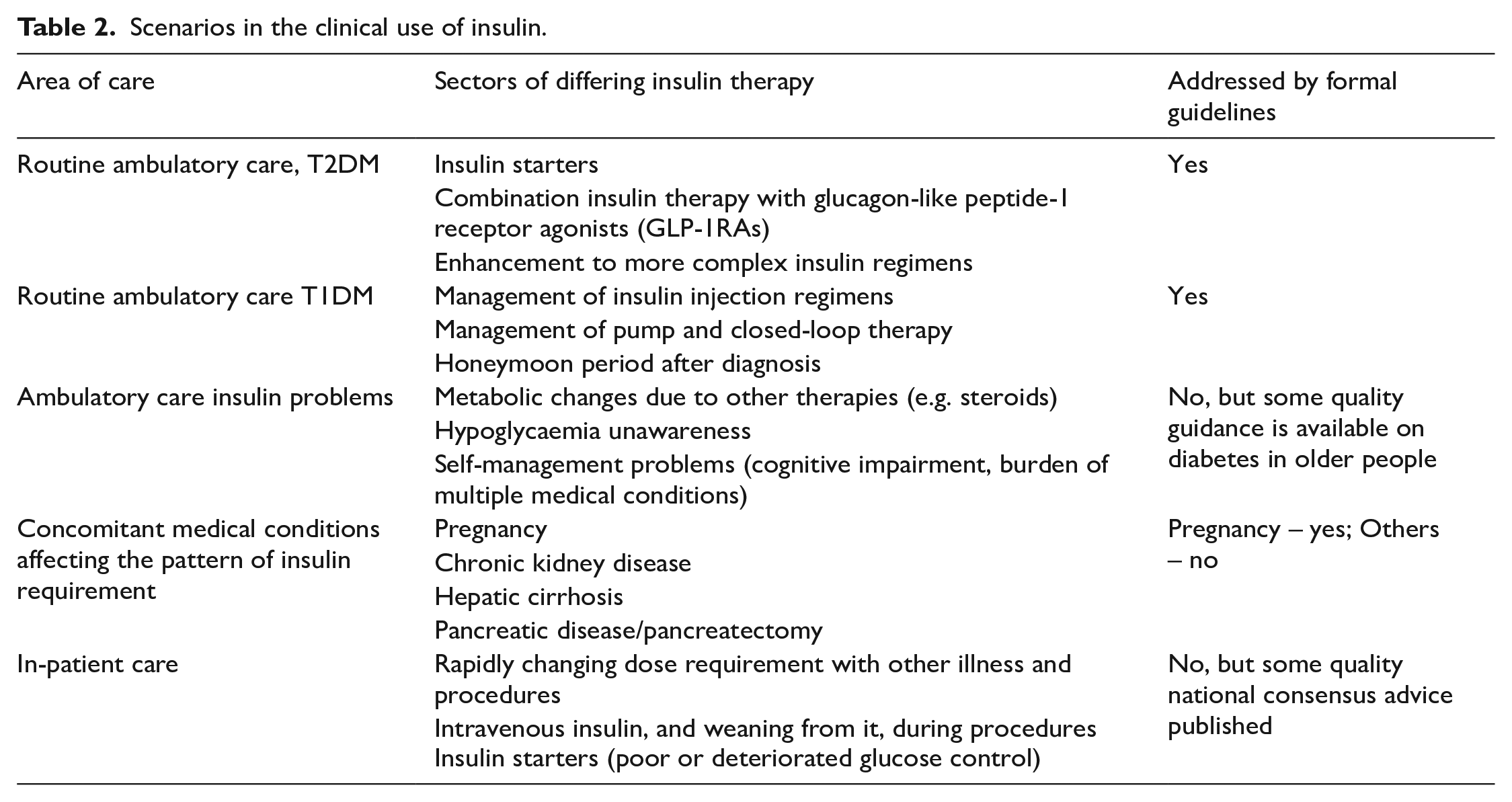
Care has been taken to be aligned with the guidelines, including recommendations from NICE and the SMC though these are both quite limited in scope being centred around ambulatory care (Table 2).9 –11 Some careful expert group papers are also used. 12 For more diverse scenarios comment has been kept in line with current diabetes best practice.
Choice of insulin preparation: Basal insulin biobetters
There is no universal basal insulin therapy suited to the management of hyperglycaemia in all individuals. Here we will use a loose classification by situation of insulin use and type of diabetes (Table 2), but even then ignoring rarer situations of abnormal metabolism often associated with single gene defects. Useful groupings are (1) Ambulatory T1DM; (2) Ambulatory T2DM; (3) In-patient scenarios; (4) Insulin therapy in the context of other medical conditions.
Insulin therapy in the context of other medical conditions
This is self-evidently complex in itself but some unifying themes are seen. For example in people with hepatic cirrhosis the usual excess basal glucose production from the liver is severely impaired, so these people have little need for a basal insulin covering the interprandial and night periods, while often requiring high doses of meal-time insulins. High meal-time dose requirements are also seen in those on high-dose steroid therapy, and in pregnancy complicated by diabetes. In people with these conditions the basal insulin need is often low (sometimes absent in cirrhosis and with steroids), and needs to avoid the peaks seen after administration of NPH insulin, whose 12-h absorption profile is then unsuitable, with a peak absorption at around 4–5 h. 13 But, with the exception of pregnant women with T1DM, some insulin production is preserved in these conditions, so a perfect profile from an injected insulin is unnecessary, suggesting low dose insulin glargine 100 U/ml (available as biosimilar) is acceptable. Insulin glargine 100 U/ml is priced below the alternative insulin detemir (Table 3).
Biosimilar and recent biobetter insulins on the market in the UK, February 2023, with NHS indicative prices.
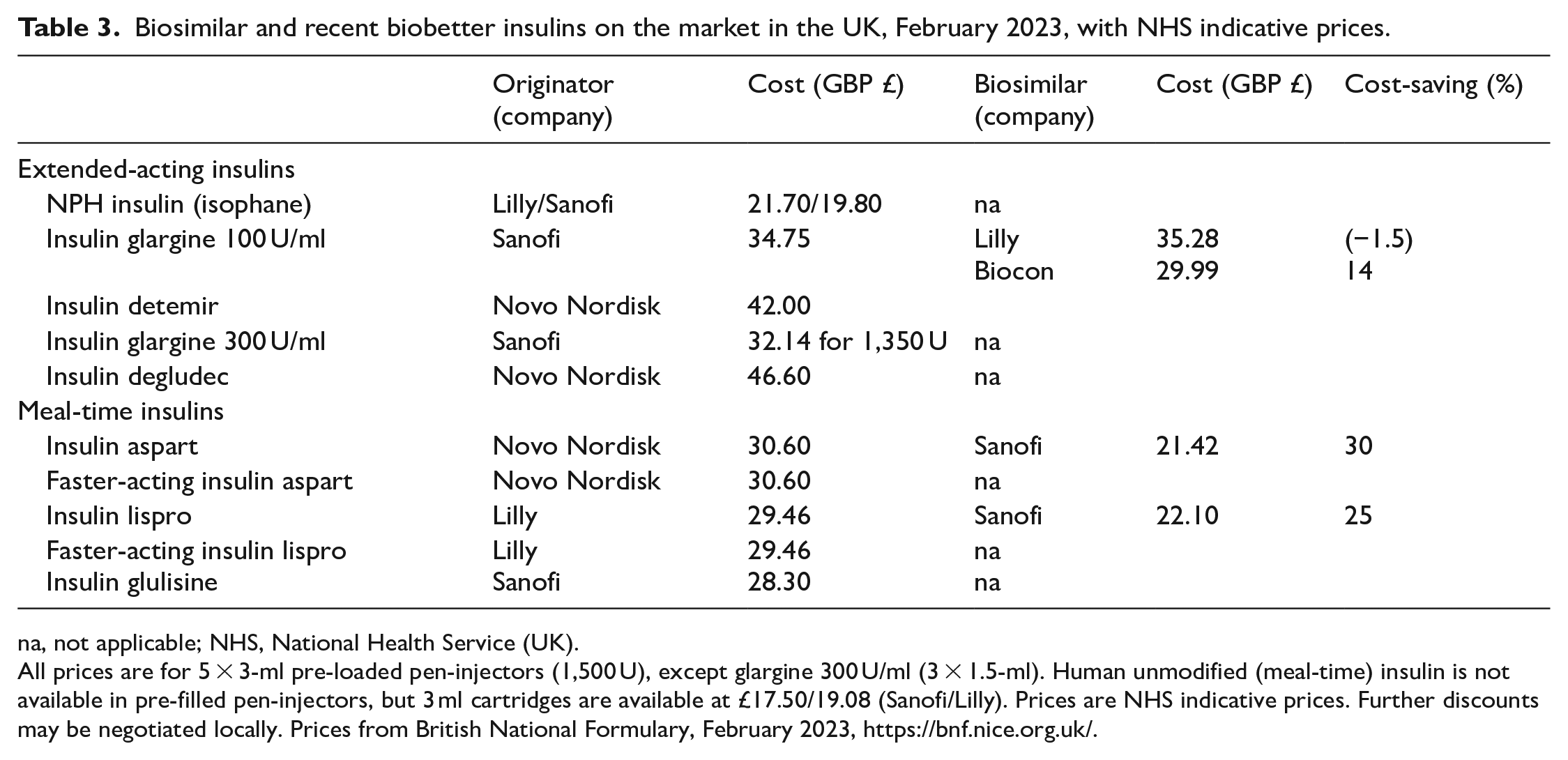
na, not applicable; NHS, National Health Service (UK).
All prices are for 5 × 3-ml pre-loaded pen-injectors (1,500 U), except glargine 300 U/ml (3 × 1.5-ml). Human unmodified (meal-time) insulin is not available in pre-filled pen-injectors, but 3 ml cartridges are available at £17.50/19.08 (Sanofi/Lilly). Prices are NHS indicative prices. Further discounts may be negotiated locally. Prices from British National Formulary, February 2023, https://bnf.nice.org.uk/.
A different situation pertains in people with renal failure (dialysis is not discussed here) and with severe pancreatic damage including after radical pancreatectomy. In these conditions, insulin sensitivity can be very high, and dose requirements thus very low, for reasons not understood in renal disease and perhaps secondary to concomitant glucagon deficiency with pancreatic damage. In both, some kind of multiple injection regimen will be needed, usually meal-time + basal insulin. However, the doses and absorption profiles of the insulin need to be as optimal as possible if a semblance of control of hyperglycaemia without erratic hypoglycaemia is to be maintained, suggesting a role for optimised long-acting insulin analogues with stable 24-h PKs such as insulin degludec or insulin glargine 300 U/ml. Often medical therapy in such people is already complex, but in those who can adapt to and tolerate further extra burden, use of a pump for basal insulin supply can be useful, and indeed closed-loop therapy (‘artificial pancreas’) controlled by a glucose sensor. For all of these recommendations the evidence-base in terms of RCTs is absent, and thus the recommendations derive from RCTs in others with diabetes, coupled to knowledge of the PK/PD profiles of the insulins.
Insulin therapy in in-patients
While as many as 25% of in-patients may have diabetes, and the finding of new diabetes or hyperglycaemia is quite common, only a proportion of these people will require insulin therapy. The management of temporary insulin therapy, often intravenous, during major procedures or acute metabolic stress, or in people with T1DM during any period of prolonged fasting, is usually driven by local protocols and is not discussed further here. As an aside however, the use of closed-loop systems using glucose-sensor controlled subcutaneous insulin delivery has attracted some recent studies and publications, and may well see greater application in the next decade. However a particular warning, not well articulated in guidelines or articles or product information is needed here: subcutaneous glucose-sensing (including finger-prick blood sampling) will give falsely low results if peripheral circulation is compromised – indeed subcutaneous insulin absorption will also be affected.
Often insulin therapy is begun on general medical and surgical wards, or insulin doses may need rapid and radical change. In this situation, longer-acting insulin analogues can be difficult to handle, coming to steady state dosage over a number of days, a situation complicated if requirements are changing with the underlying medical condition/therapies. Here, twice daily NPH insulin comes into its own, as doses can be chosen and varied at double the frequency of even insulin glargine 100 U/ml (given once daily). Doses may need to be escalated rapidly, and again twice daily therapy enables this, initial doses being guided by the nature of the other medical condition(s) and perhaps intravenous requirements if coming off those. Rapid establishment of basal insulin requirement is needed to enable decisions to be taken on meal-time insulin therapy use or dosage.
The provision of in-patient support by the diabetes team has a history of many decades, but only more recently has it been endorsed by funders as obligatory. One advantage here is that the diabetes specialist nurses involved can be part of the team that provides insulin therapy support for out-patients and the community, allowing early and more seamless discharge of people beginning insulin therapy in hospital or requiring large changes in insulin dose while there.
Basal insulin therapy in ambulatory T2DM
This is the area of diabetes practice most often addressed in diabetes glucose-lowering therapy guidelines and consensus statements.10,12 As T2DM accounts for over 90% of prevalent diabetes, and as people with diabetes will be on insulin therapy for around half of their diabetes lifetime, usually after oral and other agents can no longer give optimal metabolic control, it also accounts for the highest proportion of insulin users. Combination with continued metformin is usual. A basal-insulin-first approach was promoted from Oxford in the late 1970s (though widely used already by many) and gained traction with RCTs of once daily insulin glargine 100 U/ml and insulin detemir some 20 years ago.14,15 Alternatives would be premix insulins, meal-time insulins, or meal-time + basal insulin regimens, all of which give considerably more hypoglycaemia without formal evidence of other gain. 7 Further basal insulin alone can set the scene for multiple injection regimens as endogenous pancreatic insulin supply further declines, or for a combination injection regimen with a GLP-1RA.12,16
Indeed globally GLP-1RAs, themselves mostly injectables (an oral semaglutide is now marketed), have increasingly displaced basal insulin as first injectable when acceptable glucose control can no longer be achieved with lifestyle plus oral agents, and with the added advantage of some cardiovascular risk protection in those with extant CV disease. Unlike insulin, GLP-1RAs, available as weekly injections, do not require precise dose titration according to self-measured finger-prick plasma glucose levels, do not themselves cause hypoglycaemia, and result in weight loss rather than weight gain. 16 As a result they are easier to commence than insulin (for both user and physician), although the cost-savings from reduced clinical interactions, less self-monitoring and less hypoglycaemia, will not on average outweigh the much higher acquisition cost.
Available choices for beginning a basal insulin are human-sequence NPH insulin (isophane), insulin glargine 100 U/ml, insulin detemir, insulin glargine 300 U/ml and insulin degludec.10,11,17 These are likely to be joined in the next 2 years by the weekly insulins insulin icodec and insulin efsitora alfa (basal insulin Fc).18,19 Given once daily, NPH insulin, if started before glucose control has deteriorated too greatly, can achieve the same HbA1c as insulin glargine 100 U/ml or insulin detemir, but does give more hypoglycaemia.14,15 This gives rise to division between those who interpret the evidence-base narrowly, and knowledge-based-medicine clinicians who face users of insulin. The hypoglycaemia referred to here are plasma-glucose-confirmed symptomatic events, and are thereby of subjective origin and as such not acceptable to some regulators. Further a symptomatic event, though it can be distressing and inconvenient, is usually easily managed within a few minutes, and therefore has little impact on quality of life measured over a year. Accordingly the gain from reduced hypoglycaemia has little impact on the incremental cost effectiveness ratio, certainly not enough to offset the additional cost of insulin glargine 100 U/ml (Table 3) 10 Clinicians (and patient associations) would however argue that ignoring hypoglycaemia breaks the contract of ‘first do no harm’, while less of the side effect makes the argument for starting insulin easier, and therefore reduces time exposed to harmful hyperglycaemia. Further comparative measurement of HbA1c is flawed where hypoglycaemia is improved – it averages glucose concentration and therefore will be artificially lower with NPH insulin, disguising the harmful greater hyperglycaemic exposure.
In practice people on NPH insulin are more likely to come earlier to multiple injection therapy (or need addition of a GLP-1RA), because the inappropriate absorption profiles will become more problematic as their endogenous insulin secretion wanes. Consensus statements centre on the use of long-acting analogues as first choice. 12 Even formal guidelines allow for once daily glargine use in another circumstance – where more than one injection a day is required and a third party is needed to administer this.10,20
Basal insulin use in T1DM
Around 50% of insulin secreted in a non-diabetic person is used for control of basal glucose production from the liver – without it and when denied carbohydrate intake glucose concentrations rise to around 12–13 mmol/l (without other metabolic stress such as infection). As a disease of absolute insulin deficiency, people with T1DM therefore require basal insulin replacement as part of their therapy regimen. Failure to deliver adequate insulin into the circulation towards the end of the night (‘dawn phenomenon’) is long recognised. 21 It is a function therefore of insulin absorption profiles, exacerbated by stress hormone circadian rhythms in the context of underlying inadequate metabolic control, and is not found in non-diabetic adults. 22 It occurs in T2DM as well as T1DM, but is more pronounced with more extreme endogenous insulin deficiency. Full 24-h basal insulin delivery, without peaks during the night (which result in dose reductions due to hypoglycaemia), is then the appropriate clinical response.
The insulins available for people with T1DM are as for T2DM (see immediately above). However the decisions surrounding choice are made more critical and complicated by the much higher hypoglycaemia event rate (incidence >90% in a year, rate very variable but at level 2 (<3.0 mmol/l) approximately 1 per month), 6 and much higher impact of severe hypoglycaemia (needing third part help, approximately yearly) and serious hypoglycaemia (needing (para-)medical intervention). Absence of endogenous insulin secretion means that 24-h coverage is important, and that is not comprehensively achieved by insulins detemir and glargine 100 U/ml. While the knowledge base is quite strong (e.g. these insulins are effective, and the comparative hypoglycaemia incidence/event rates understood) the RCT evidence-base is relatively weak, being based on studies optimised for their ability to deliver the protocol rather than higher quality clinical judgements at the individual level. Again much of the hypoglycaemia data is subjective, and gathered to different and changing standards, in the context of open label comparisons due to differences in the pen-injectors used for each insulin. A further context here is that the advent of continuous subcutaneous insulin infusion (CSII, ‘pumps’), continuous glucose monitoring, and then of closed-loop (‘artificial pancreas’) systems, all of which are now endorsed or in the process of being endorsed by funders for use in some people with T1DM,23,24 means that any much cheaper insulin injection regimen will be cost-saving. Further the availability of injected meal-time insulin analogues (discussed below), with shorter more physiological meal-time PK/PD profiles, means that basal insulin coverage needs to be more complete, notably during the night and at the end of the afternoon and evening, or rather at times more distant from the last meal-time insulin injection. Accordingly the multiple injection market in T1DM was quick to switch to the combination of meal-time analogues + insulin glargine 100 U/ml (or sometimes insulin detemir) for people on injection therapy, supported by the evidence-base both for HbA1c and hypoglycaemia.25,26 However, substitution of glargine 100 U/ml by glargine 300 U/ml or insulin degludec has been slower, partly again due to weak or absent evidence of HbA1c advantage. Insulin degludec does however offer advantage over glargine 100 U/ml in regard of nocturnal and severe hypoglycaemia. 27 True 24-h basal insulins are endorsed as available for adults with problems with conventional long-acting analogues.9,28
A special situation can arise in the first year or so after diagnosis of T1DM. If at the time of diagnosis there is metabolic stress, for example from infection or ketoacidosis, the compromised insulin secretion may be further impacted by glucose- and lipid-toxicity. Relieving these with exogenous insulin then allows temporary recovery of endogenous insulin secretion, occasionally even to the point when insulin injections are no longer needed for a short time. More commonly it may be possible to maintain glucose control for up to a few months using basal insulin alone, particularly in adults. There is no evidence-base for choice of insulin, but it would seem logical to use an insulin giving near 24-h coverage, such as insulin glargine 100 U/ml or insulin detemir, in these people with continuing endogenous insulin secretion.
Providing basal insulin supply by pumps and closed-loop systems uses meal-time insulins from a reservoir. This is discussed in the section on those insulins below. Portal rather than peripheral insulin might seem more physiological too, but is not available clinically, while hepatoselective insulins have proved adverse and have been abandoned. 18
Choice of insulin preparation: Meal-time insulin biobetters
Designer rapid-acting insulin analogue injections in T1DM
Rapid-acting insulin analogues were the first example of the use of genetic engineering to produce a biobetter, 3 although the terminology at the time was ‘designer’ insulins. Insulins aspart and lispro utilise small switches of amino acid residues towards the end of the B-chain of the insulin molecule, so as it has less propensity to form hexamers, a form too large for absorption into the circulation after subcutaneous insulin injection. Evidence of better (lower) meal-time glucose excursions is convincing, though evidence of lower HbA1c somewhat marginal, perhaps because of the amelioration of hypoglycaemia as discussed above. 29 In people with T1DM when used in combination with a first-generation basal insulin analogue (as is logical pharmacokinetically) improvement in HbA1c together with improvement in incidence of hypoglycaemia can be demonstrated.25,26 As discussed above, the market quickly adopted this approach in T1DM, where the combination of hyperglycaemia and hypoglycaemia creates a huge unmet need, using a meal-time analogue injection before each main meal.
The biobetter development process subsequently produced formulation changes (i.e. with no further changes to peptide structure) which further reduced the propensity to hexamerisation, and/or improved access of the insulin molecule from the subcutaneous tissue depot into the vasculature. Again there was clear evidence of improvement in post-prandial meal-time glucose excursions. In people on insulin these are over double at peak the physiological excursion, with a reduction when using the new analogue formulations to around two-thirds higher. 30 But peak glucose excursions are only seen for a short time perhaps three times a day, so indeed HbA1c was little improved, and inconsistently so between studies. Further hypoglycaemia in the hour after injection actually increased (as might be expected), albeit at a time of low hypoglycaemia risk. Where cost is matched to first generation meal-time analogues, the insulins are endorsed for use, 31 but clinical adoption has been limited.
Development has not stopped in this area, and further formulation changes have resulted in studies showing even faster, and therefore more physiological, insulin absorption and control of glucose excursions from three small companies new to the area. 18 Phase 2 and phase 3 clinical trials are awaited.
Designer rapid-acting insulin analogue injections in T2DM
The same analogues, and later newer formulations, have demonstrated the same advantage in terms of lower meal-time glucose excursions as discussed above for T1DM. 30 But advantages for overall glucose control are even more difficult to demonstrate, probably in part because people with T2DM have very significant insulin reserve even when they get to the stage of requiring a full meal-time + basal insulin regimen. The residual endogenous insulin secretion in effect buffers to some extent mismatches in the insulin absorption profile, and erratic subcutaneous insulin absorption.
As a result it makes little resource sense to use more expensive analogue insulins when moving to a multiple injection regimen in this group. However three factors, not grounded in RCT evidence, push in that direction. Where glucose control remains problematic on meal-time human, and in particular if post-prandial glucose excursions or late post-prandial hypoglycaemia are a problem, then a trial of a switch to a meal-time analogue is reasonable. Secondly, T2DM is not a homogeneous metabolic condition, and some people with it, notably of a thinner or more elderly phenotype, have insulin sensitivity and secretion closer to people with T1DM, and might be expected to benefit in line with that group. Thirdly, use of insulin therapy requires expertise, and this is particularly true of multiple injections regimens, where insulin dose adjustment in the face of erratic meal-time and insulin profiles requires both knowledge and experience. In this circumstance many diabetologists and diabetes specialist nurses focus on one type of meal insulin and one basal insulin, a choice dictated mostly by people with T1DM.
Insulin in pumps, including in closed-loop systems
The insulin used for subcutaneous pumped insulin will be a soluble short-acting ‘meal-time’ insulin even for basal glucose control. The principle is simply then that insulin is continuously supplied 24 h a day from the pump. The technology is currently used mostly in people with T1DM. It is endorsed for the most part by funders, 23 notably in children.
Logically the choice of the meal-time ‘bolus’ of insulin delivered by these pumps should differ little from that of meal-time insulin injections discussed above. And if insulin absorption from subcutaneous tissue was perfectly smooth and unchanging, then any soluble insulin would be suitable to provide basal insulin supply. However insulin absorption is very erratic, and there is some evidence that the first-generation analogues are more consistently absorbed than human insulin, that is that some of the variability is due to the dynamic equilibrium between hexamers and the absorbed monomers. Accordingly, to make best use of the expensive pump and cannula technologies, an analogue has generally been the choice for pump insulin since the time they were introduced.
With closed-loop systems different arguments come into play, essentially because of the delay in sensing changes in plasma glucose from sensors under the skin, coupled with the delay in insulin absorption rate change when the pump delivery rate is changed. Logically then the control algorithms, which anyway struggle to cope with these changes, will work better with the more-rapidly absorbed insulins. Again there is little evidence to support this in practice, but given the overall expense of the systems making best use of the technology seems logical.
Biosimilar insulins – impact and use
Human insulins, including unmodified (meal-time) human insulin and NPH insulin, have been available since the 1980s from diverse manufacturers, each being developed and registered as a new medication entity. Insulin was ever a biological medicine, a definition which includes all proteins, but the concept of biosimilars as applied to insulin really only developed after other biological medicines became available, notably erythropoietin. The regulatory framework was largely formulated after problems with copies of that latter medicine. As patents have expired on insulin glargine, insulin aspart and insulin lispro (all multi-billion dollar per year global markets), copies of these have become attractive targets, and a biosimilar framework for insulin adopted in all the more sophisticated markets. 4 The need for this was emphasised by problems in countries without such frameworks, such as Mexico and India. 32
Those frameworks are sufficiently rigorous to provide assurance that biosimilar insulins available to us can be used in the same way as their named proprietary (‘originator’) products.4,33 Because, as discussed above, insulin requirement is highly variable between individuals, and because insulin absorption is highly variable within individuals, it would be difficult to distinguish preparations from different companies. Accordingly, when starting an insulin it can be selected on the basis of acquisition cost (Table 3), provided the administration system (the pen-injector) is equally user-friendly.
A different situation pertains however to substitution, that is, the switching of a named insulin to another proprietary brand. The first problem is that biosimilarity is not product bioidentity – our PK/PD and phase 3 studies do not have the power to confirm that population effects are identical, never mind identical in all individuals. Further users of any insulin often have a love-hate relationship with it – day-to-day variability being such that it is a perverse medical partner at best, but of course one that the user is forced to live with, and then develops a dependence on ‘knowing’ their insulin. It is largely for this reason that in the UK it is advised that insulins are prescribed by proprietary name.9,17 Accordingly, while substitution for a biosimilar can be made, it has to be supported by careful counselling, increased self-measurement of plasma glucose and even special cautions over at-risk activities like driving. There is then a health cost to such substitution.
Unlike Europe, Canada and UK, in the USA interchangeability has been mandated (by the US Congress), meaning that pharmacists can change the supply of a prescribed insulin to an approved biosimilar without reference to the prescriber. Two insulin glargine biosimilars are so licensed by the US FDA.
When a generic version of a drug becomes available, the price often falls by around 90%, essentially determined by manufacturing and supply costs. However, for biosimilars there are significant pre-clinical and clinical development costs, and accordingly the price advantage is much smaller, as yet only around –30% at best in the UK (Table 3). However this may also reflect a still very narrow manufacturing base (low competition), due to technological difficulties around fermentation processes while maintaining Good Manufacturing Practice. As yet only Biocon outside Europe and the US produces approved insulins, and then only from 2022 – though Chinese competition is known to be close behind.
Conclusion
Advances in purification, design and manufacturing have led to a variety of insulins (biobetters) being available for clinical use. The variety is driven by attempts to meet the glucose control needs when using what remains a far-from-optimal medication. Insulin dose and appropriate insulin regimens also vary widely between the clinical scenarios in which they are used, and to some extent choice of any particular insulin preparation is governed by those, and individual user experience. There is no insulin or insulin combination that fits all, even in standard areas such as ambulatory care. Expertise in matching regimens and circumstances to individuals is therefore important, but also has to be matched by something not discussed in this article, notably appropriate expertise in deployment including quality user education. 12 With the advent of biosimilars there are opportunities for cost-savings without detriment to health care outcomes, in particular in new insulin starters. However these cost-savings are not large in the context of support technologies for self-glucose monitoring, and 24-h support by diabetes teams.
Footnotes
Acknowledgements
This article is unfunded. The author thanks colleagues in clinical practice, academia and industry for fruitful in-depth discussions over four decades, but has not discussed this specific article with any third party.
Declaration of conflicting interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author has been involved in the development of most of the insulins discussed above, and he or institutions with which he is associated have received funding in that regard, and additionally for related research studies and/or lecturing. This includes Biocon, Eli Lilly, Gan & Lee, Novo Nordisk and Sanofi but also manufacturers of competing glucose-lowering products namely AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Janssen, Merck (MSD) and Servier.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.