
Abstract
This article offers a critical exploration of the espoused purpose and implementation of accreditation of health professions programs in Australia from the perspectives of academics at an Australian university. It examines enactment of accreditation in supporting the development of work-ready graduates through outcome-based education. By drawing upon Yanow’s interpretive policy approach, this qualitative study identifies similarities in perceptions of accreditation across health professions and draws attention to key tensions that must be addressed in the pursuit of outcome-based education. Concerns related to the inflexibility of accreditors, time and administrative requirements, and processes for educational review and innovation are highlighted. The article concludes by offering suggestions for changing accreditation practices to ensure future-focused work-ready graduates.
Keywords
Introduction
Creating a safe and effective health workforce is essential to ensuring optimal health outcomes for individuals and communities served by health professionals (Frank et al., 2020). Health professions education programs must equip healthcare professionals to address current and future population health and health system needs. Accreditation has been positioned as a quality assurance process designed to ensure that the higher education sector graduates competent health professional students with the skills necessary to meet patient needs and the evolving needs of the healthcare sector (Frank et al., 2020; Van Zanten et al., 2012). Compliance with accreditation standards by health professions education programs therefore acts as a proxy for graduate competence and aims to instil public confidence in graduates’ abilities to provide safe and effective healthcare (Frank et al., 2020). Despite growing evidence related to the potential impacts of accreditation on graduate readiness and practice, evidence related to the process and administration of accreditation systems and policies and how this may inform future improvements to accreditation policy in the health professions is lacking (Tackett et al., 2019; Van Zanten et al., 2008).
Historically, accreditation systems have focused on quality assurance, risk management and meeting minimum standards. Within health professions education, effective accreditation is a key ingredient for managing inconsistencies in quality and risk that lead to unacceptable variations in graduate competence within professions (Asch et al., 2014; Frank et al., 2020). The need for standardised accreditation processes to ensure compliance with minimum standards was first highlighted by the 1910 Flexner report (Irby et al., 2010). More recently, accreditation has begun to observe a shift in focus from course structure and content to process and outcomes-based education (National Academies of Sciences, Engineering and Medicine, 2017). This was in response to the Carnegie report which called for reform of medical schools and for greater focus on standardising learning outcomes and competencies rather than structure and length of curriculum (Irby et al., 2010).
Evidence suggests that quality health professional education can have a strong impact on graduate outcomes as the educational setting greatly influences graduate practice patterns and abilities (Asch et al., 2014; Tamblyn et al., 2002). Emerging health professions accreditation research suggests accreditation has positive impacts on clinical and institutional outcomes. By reducing variation in education and improving quality of training, accreditation can influence factors such as curriculum innovation, learning environments and teaching activities which can influence graduate work-readiness (Halstead, 2020; Tackett et al., 2019). However, existing evidence on the role, elements and process of health professions accreditation on graduate work-readiness and quality, healthcare delivery, and patient outcomes is scarce (Frank et al., 2020).
Internationally, accreditation systems within and between disciplines are varied. The International Health Professions Accreditation Outcomes Consortium (IHPAOC) recently identified a common list of 10 core elements of accreditation systems and proposed a simple framework (Frank et al., 2020). There is currently no clear consensus or evidence as to which features of accreditation are essential to ensure quality outcomes in health professions education. Whilst accreditation is unlikely to be abandoned, the efficacy of accreditation remains largely unknown and of concern. For example, rapid developments in healthcare means health professions education needs to remain dynamic and continually evolving to support graduates who are future focused and ready to address these issues. Yet accreditation standards have remained unchanged for years, potentially creating a gap (Akdemir et al., 2021). A recent study in New Zealand also drew attention to concerns related to overlap with similar requirements by the tertiary education sector, a lack of educational expertise on panels and continued stipulation of clinical hours (input-driven standards) despite a lack of evidence that it corresponds to competence (Shaw and Tudor, 2021). It is only through in-depth understanding of the enactment of accreditation policies by health professions education providers that we can truly come to understand how accreditation currently supports the development of graduates to meet current and emerging needs of the health system and what changes may be necessary. Therefore, this study explores the experiences of health professions accreditation and its ability to support the development of safe and effective work-ready graduates through outcome-based education. More specifically this research responds to the following research questions: (i) What is the purpose of accreditation in the development of work-ready graduates and (ii) How are accreditation policies and processes enacted in health professions programs? The findings aim to inform improvements to health professions education into the future.
Methods
Study design
Policy analysis provides a way for understanding how and why certain policies are made and implemented, and their effects, and has been recommended as a method for developing evidence to support advocacy efforts that can lead to better population health outcomes (Browne et al., 2018). While there are many ways in which policy can be analysed, 10 this study of the ‘lived experience’ of health professions accreditation processes and their purpose in supporting the development of safe and effective work-ready graduates through outcome-based education is informed by an interpretive perspective (Schwartz-Shea and Yanow, 2012; Yanow, 2000). For Yanow, interpretive policy research ‘focusses on the meanings of policies, on the values, feelings, or beliefs they express, and on the processes by which those meanings are communicated to, and “read” by, various audiences’.12 Conceptually, Yanow’s approach has four intertwined steps, as follows: (1) identify the artefacts (language, objects, and acts) that carry meanings relevant to the study, (2) identify relevant participants/communities, (3) identify the discourses (specific meanings) being communicated, and (4) identify the points of conflict and their conceptual sources (i.e. different interpretations) (Yanow, 2000). Under such a perspective, the central question is ‘how is the policy issue being conceptualised or “framed”’ (Fischer, 2003), which shifts the analytical focus from ‘facts’ to ‘meanings’, with meanings having important consequences for how issues are understood and subsequently addressed. In essence, our study explores the meanings academics attach to the health professional education accreditation processes in which they are involved and their feelings related to the purpose of and how well the accreditation standards reflected current and emerging needs of the health system and population health. Yanow’s interpretive approach was therefore deemed to be appropriate for this study.
Yanow’s approach enabled us to explore the experience of implementation of accreditation policies rather than accreditation policy content. This study was approved by the Monash University Human Research Ethics Committee (project ID 23725).
Setting and participants
The setting for the research was the Faculty of Medicine, Nursing and Health Sciences and Faculty of Pharmacy and Pharmaceutical Sciences at Monash University, Melbourne, Australia, which offers pre-registration education to students across disciplines including dietetics, medical imaging and radiation sciences, medicine, nursing and midwifery, occupational therapy, paramedicine, pharmacy, physiotherapy and psychology. Education programs across all of these disciplines are subject to regular accreditation. In Australia, there are two main accreditation systems in operation: (1) The National Registration and Accreditation Scheme (NRAS) and (2) the National Alliance of Self-Regulating Health Professions (NASRHP). NRAS oversees accreditation of professions registered with the Australian Health Practitioner Regulation Agency (AHPRA) through individual profession boards. Australian Health Practitioner Regulation Agency; National registration and accreditation Scheme, 2019 This includes chiropractors, dental practitioners, medical practitioners, nurses and midwives, occupational therapist, optometrists, osteopaths, paramedics, pharmacists, physiotherapists, podiatrists, and psychologists.
NASRHP oversees professions that individually manage accreditation systems through their professional organisations (National Alliance of Self-Regulated Health Professions, 2017). This includes dietetics, speech pathology, exercise physiology and audiology. Following a recent review by NRAS calling for more streamlined accreditation standards and processes, three professions (including Aboriginal and Torres Strait Islander health practice, Chinese medicine and medical radiation practice) are working together in the NRAS harmonising project to coordinate their accreditation standards and processes (Woods, 2017).
Cognisant of this policy context, we recruited a purposive sample (Patton, 2002; Robinson, 2014) of course coordinators and faculty staff who had experienced accreditation in the past 5 years and could provide critical insights into the faculty’s current experience of and response to accreditation systems across health professions offered by the faculty. This included members of the Faculty of Medicine, Nursing and Health Sciences Quality Assurance Team which provides support in an as needed basis to staff during their professional accreditation through the provision of up to date universitywide data and policies. Participants were identified by members of the research team and invited to participate in a telephone or virtual one on one or group interview. Invitations were sent via email correspondence in March 2020. This aligns with Steps 1 and 2 of Yanow’s approach, whereby the artefacts that carry meaning and relevant participants/communities were representatives from pre-registration health professions at Monash University with applied knowledge and experience of accreditation policies and procedures in their respective disciplines (Yanow, 2000). Clear outlines of the aims and objectives of the research were included through the use of an explanatory statement. Snowball sampling (Robinson, 2014) was also used with participants offering suggestions for other potential participants upon completion of their interview.
Interview procedure
The semi structured interview logic was developed by the research team, informed by a preliminary review of the literature and experiences of research team. A single member of the research team (SM) performed all interviews and obtained verbal consent from all study participants at the beginning of the interviews. Interviews explored recent experiences of accreditation, including strengths, frustrations, opportunities and threats. They also explored interviewees' perceptions about the purpose of accreditation and how well the accreditation standards reflected current and emerging needs of the health system and population health. Interviews were conducted via Zoom videoconferencing technology between March and June 2020. Interviews lasted from 40 to 75 minutes and were audio recorded. All interviews were professionally transcribed and SM reviewed all transcripts against the audio recordings to verify accuracy.
Data analysis
In this study, Yanow’s interpretive approach was applied to explore the ‘meanings’ rather than ‘facts’ being discussed by participants in their interviews (Yanow, 2000). Steps 1 and 2 of Yanow’s approach (as described above) resulted in the generation of the interview transcripts. Steps 3 and 4 were applied by focussing on the concept of ‘symbolic language’ to analyse the ‘language’ and ‘meanings’ being communicated in participants’ interviews and potential points of conflict (Yanow, 2000). First category analysis was applied, whereby sections of the interview text were coded to create categories. Three of the transcripts were coded by all members of the research team to create the categories. This framework was further refined by three members of the research team based on in-depth analysis of two interviews each (SM, CP, and JM). During the process, the researchers focused on identifying the meanings being communicated, similarities between codes within categories, and differences between interviews in meanings described. The researchers then came together to interpret the categories and the purpose and process espoused by accreditation standards and processes. The researchers discussed the potential ‘meanings’ communicated by the participants and identified explicit and implicit areas of conflict. Data analysis was assisted by QSR-NVivo 11.
Results
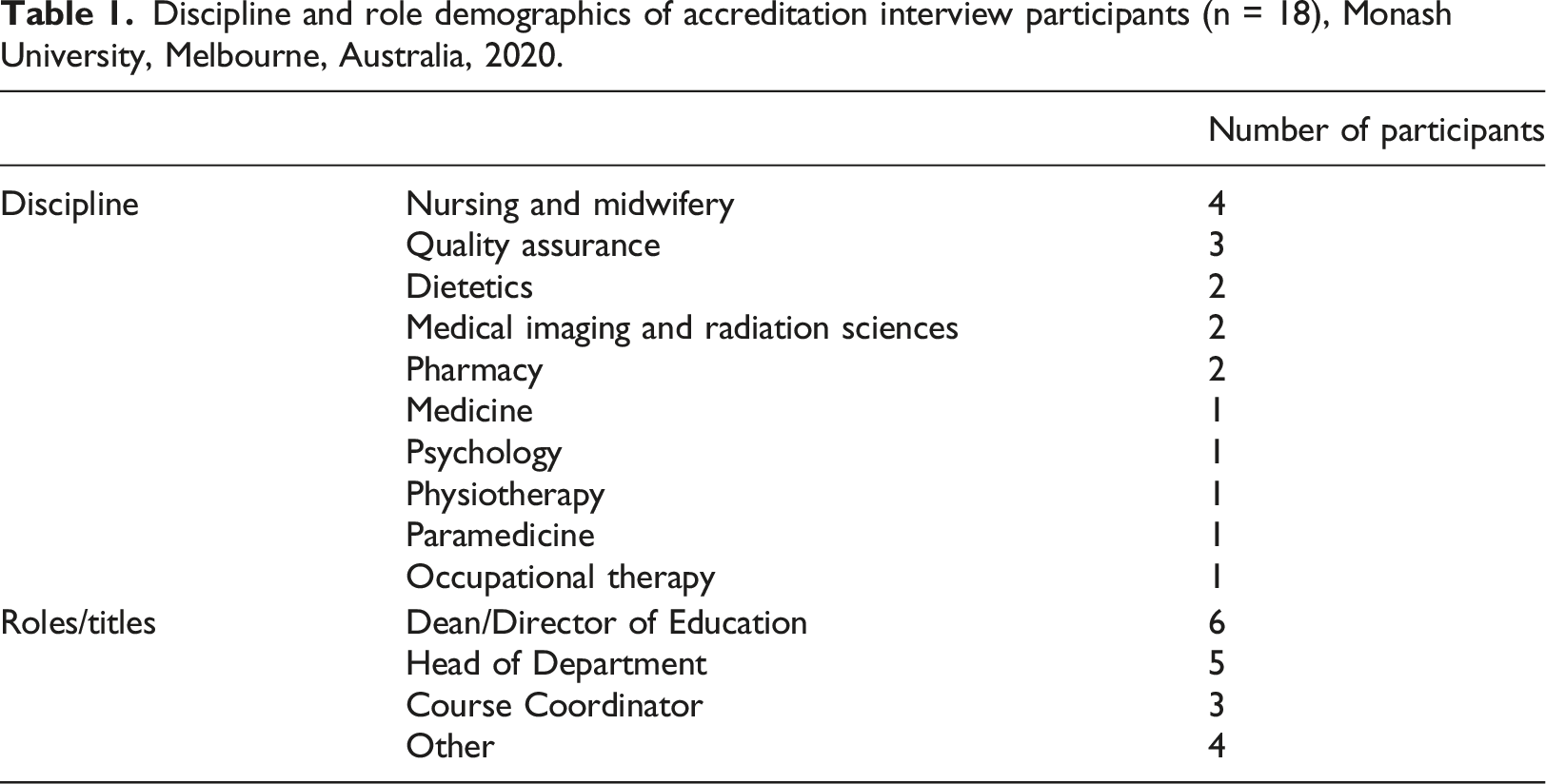
Discipline and role demographics of accreditation interview participants (n = 18), Monash University, Melbourne, Australia, 2020.
Analysis of the participant interviews identified tensions that exist within the ‘purpose’ of accreditation and within the ‘process’ of accreditation in the development of safe and effective work-ready graduates.
Accreditation purpose
Participants were in broad agreement about the overall purpose of accreditation, namely, ensuring quality of graduates and quality of health professional programs. This included the quality of staff, teaching and learning resources underpinned by evidence based best practice, and the academic experience graduates receive. The quality of graduates was also explained to be related to ensuring graduates met relevant competency standards to practice through standardisation and benchmarking. Graduates could therefore be deemed safe and fit for purpose, and eligible for registration to be employed to meet the current and emerging healthcare needs of their patients and the community. Council’s job is to review programs and ensure that the outcomes are at least a minimum standard and allow it, I guess, some confidence to the public around the quality of … graduate[s]. (Participant A)
Tensions however were reported to exist for some participants as to whether or not accreditation systems were actually achieving their intended purpose of developing safe and effective work-ready graduates. Whilst graduates from an accredited course may be deemed ‘work-ready’, concerns related to the variation in graduate readiness were raised. This often related to the issues commonly cited with input- versus outcome-focused education and competency standards, and a focus on clinical hours. I could say that the intent of accreditation obviously is to protect the public from harm, … I am not certain that the process itself necessarily ends up with the best outcome as possible… there are some weaknesses, within the process I… think it does lead to variability perhaps intended variability and graduate outcomes. (Participant N)
Participants also described the role of accreditation as helping to ensure graduates displayed and represented the core values of their professions in order to maintain its reputation and social accountability and play a role in improving health outcomes in the community by providing quality healthcare upon graduation. For Health Professions programs, I think one of the benefits is you know really… I like that idea of social accountability. I mean if you have an obligation to that, what you’re doing is actually linked to improving Health Care the world, then you know that sort of …gives you focus on what really matters. (Participant B)
Accreditation process
Participants described similar key steps of the process of professional accreditation. These similarities appeared to exist whether governed by NASP, NASRHP, or the NASRHP harmonising project.
Accreditation was reported to require significant investment of staff time and resources. Typically, in a 5-year cycle, planning commenced well prior to a new program accreditation or re-accreditation deadline. This involved initiation of accreditation proceedings by the accrediting board, identifying key milestones or tasks to be completed, staffing requirements, and, in some cases, scheduling of regular accreditation team meetings.
Participants’ attempts to describe the time commitment of preparing the reporting documentation as well as planning for the site visits revealed tensions related to the differences in interpretations of the accreditation standards and the level and type of evidence required, that is, university program staff and accreditation panels/bodies. Participants described experiencing challenges with regard to knowing what types and amount of evidence the accreditation panel required, and differences between the advice given by the accreditation body during preparation of the report and for site visits, compared with the advice given by the accreditation panel representatives. On some occasions, interpretation of the standards even varied within the appointed panel which was made up of a mixture of clinicians, educationists and independent members. There is no such thing as an objective value free understanding, they’ve all got hidden assumptions, hidden values and they are very contested and the understanding that different people have of what a particular standard might mean and what level of evidence you need to provide to convince the committee that you’ve met that standard is difficult. (Participant I)
Tensions regarding standards being too prescriptive also existed. Accreditation standards that were too prescriptive and detailed about applicant attributes or course content appeared at odds with the philosophy of an outcome-based education and were criticised for not being responsive enough to evolving healthcare needs. I don’t know that necessarily accreditation has always kept up with that… being able to move with the times, just because you know Healthcare adjusts, advances occur, you know what needs to be in, what needs not to be in. (Participant R)
Site visits were described by all participants with varying levels of enthusiasm. The structure, duration and focus of site visits were generally described similarly across the different professions. Concerns related to selection of accreditation panels were unearthed during these discussions. The appointment of unqualified panellists who lacked training and experience as a healthcare professional or accreditor and those with clear conflicts of interest, such as representing a competing university from the same state of Australia, were key areas of concern which threatened the credibility of the accreditation review process. The accreditation panel seeking information related to matters that were deemed the responsibility of the university, such as governance matters or level of qualification, were also cause for concern and confusion. Participants often described scenarios of duplication of the information being sought by both external professional accreditors and internal university-based accreditation proceedings. They’re supposed to come from universities that are not your competitor. … last time the academic was from Victoria which is our direct competitor and I wasn’t in this role then but apparently, we could have objected to that. But when [we] tried to object they said well, we can’t get anyone else. So, it’s her or you don’t get reviewed. (Participant O)
Accreditation, as a process, was perceived as a burden for many participants, a task to be endured rather than embraced. Accreditation was observed to be a costly exercise in terms of the fees required to cover the accreditation and associated site visits by the appointed review panel as well as staff time. Requirements associated with reporting and site visits created another set of tasks for participants and their colleagues to complete on top of their existing roles and responsibilities. Tasks associated with accreditation were divorced from everyday responsibilities, adding to workload pressures. In this way, accreditation was reported to be a ‘tick box’ activity within some disciplines, a task to be completed and moved on from, rather than a process promoting reflection, critical analysis and review. I think it’s perhaps that’s one of the things that irritates me about some of the sections in the accreditation is that…It seems a tick box. It doesn’t seem to bear any, have any significant bearing on quality and you can produce a document and tick a box, but it might not be what you’re doing. (Participant R)
This reductive approach to accreditation by some disciplines led to concern on its potential impact on innovation and stifling curriculum development. This led some participants to question broader understanding within their disciplines of both the accreditation standards and the overall purpose of accreditation.
Interestingly, accreditation was embraced by some disciplines where accreditation could be used to their advantage to advocate for resources such as infrastructure and personnel. For others, accreditation fostered opportunities for self-reflection and quality improvement, to map their current program in order to explore repetition and gaps and identify opportunities for innovation. Those that appeared to perceive accreditation as an opportunity for innovation also embraced current accreditation systems and saw them as an opportunity for collegiality rather than competition between program providers. Accreditation posed opportunities to learn from other universities to strengthen programs and optimise graduate experiences and outcomes for the benefit of the professional as a whole. I want all graduates to be good. Of course, I want the ones I’m working with to be really great, but I don’t want any graduates to be bad because that doesn’t help the profession and it doesn’t help the public. (Participant B)
In contrast, for some participants, accreditation posed potential threats to their competitive edge and curriculum innovation. When you show your competitor your entire curriculum, you kind of leave yourself open for them to say ‘those are great ideas, let’s improve our course even more’, and ‘we don’t know what their great ideas that we could adopt are so it didn’t feel right to me’. (Participant O)
Discussion
Using stories of the lived experiences of the enactment of accreditation policies and systems across 10 different health professions at an Australian university, participants described similarities in perceptions of the purpose of accreditation and the steps involved in the process. Participants described the role of accreditation as helping to ensure graduates displayed and represented the core values of their professions in order to maintain its reputation and social accountability. Tensions related to competition between universities and the inflexibility of accreditation bodies around input- versus outcome-focused education were also identified as factors which influenced participants’ experiences and conceptualisation of accreditations’ value and the future directions for health professions education program accreditation. Our findings provide important insights for accreditation policy provides and universities enacting these policies given the transferability of the findings due to our information rich and diverse sample.
Accreditation was perceived by participants as being poised to ensure continuous quality of both health professions education programs and their graduates. This finding is consistent with previous studies exploring the intended purpose and goal of accreditation by the International Health Professions Accreditation Outcomes Consortium (IHPAOC). This consortium describes accreditation as evaluation of education against specified standards that ensures high quality education such that the future healthcare workforce is adequately prepared to meet community health needs (Frank et al., 2020). Scepticism as to whether or not this was in fact the case was also expressed by participants due to observed variations in graduate work-readiness. Input-focused competency and accreditation standards were perceived to lead to this doubt. A recent review of the Australian National Registration and Accreditation Scheme (NRAS) explored issues associated with ‘work readiness’ and called for the adoption of outcome-based approaches to accreditation (Woods, 2017). The review proposed that process or input-driven elements should only be used when robust evidence supporting their use exists. The experiences captured by participants in this study are therefore consistent with recent shifts towards outcome-based education and calls for action to be braver in embracing outcome-focused education and less reliant on input-focused competency standards (Rosenberg, 2018; Shaw and Tudor, 2021).
Exploration of the process of accreditation highlighted nuances or tensions in enactment of policy driven procedures. Key tensions related to varied interpretations of accreditation standards by education providers, accreditation panels and accreditation bodies; prescriptive input-focused accreditation standards; duplication of information sought by external professional accreditors with that of internal education provider accreditation proceedings; unqualified panellists and the resource intensive episodic nature of accreditation. These tensions may impact upon the effectiveness of accreditation. For example, varied interpretations of accreditation standards may lead to different applications of the standards whereby curriculum and content delivery varies, leading to wide variation in graduate knowledge and skill levels, and overall graduate competence and safety. Additionally, unqualified panellists may authorise accreditation of health professions programs that do not meet minimum expected standards, potentially jeopardising both the quality of graduate and patient safety. Similar tensions and dissatisfactions with accreditation systems have previously been described elsewhere (Amaral and Norcini, 2023; Blouin and Tekian, 2018; Frank et al., 2020; Shaw and Tudor, 2021; Taber et al., 2020) However, in this study, the process of accreditation appears to have been divorced in some professions from the underlying purpose of accreditation. Accreditation was reduced by many participants to a task to be completed episodically as a ‘requirement’ for registration rather than embraced as an opportunity to promote innovation and continuous quality improvement both within an individual program and across the health profession. Innovation and continuous quality improvement have been extensively reported as key underlying benefits of accreditation in health professions education (Alrebish et al., 2017; Frank et al., 2020; Taber et al., 2020; Woods, 2017), yet our data suggest that stakeholders rarely embrace the process for this purpose. Internal university review processes may be the mechanism for which this continuous improvement occurs as a safer environment to highlight areas for development, however, dissemination of these findings would need to be carefully considered. Moreover, for accreditation to work as intended, the process itself must be accepted and those seeking accreditation must feel safe to engage in the process of quality improvement (Blouin and Tekian, 2018). These findings therefore provide further evidence of the need for accreditation agencies to explicitly communicate the goals of accreditation in relation to quality assurance, curriculum innovation and continuous quality improvement. Accreditation authorities should aim to ensure standards are not seeking to duplicate processes and information sought from existing tertiary education policies as described previously by Shaw and Tudor (2021). We would also suggest that consideration by accreditation authorities of more frequent revision of accreditation standards and incorporation of standards that provide opportunity for the delivery of dynamic and evolving curriculum (i.e. outcome-focused) may improve enactment and therefore the efficacy of accreditation policies in the future. If embracing more dynamic and outcome-focused standards, education providers and accreditation authorities will need to be mindful of the potential not only for innovation but for different interpretations of standards. It would therefore be reasonable to expect greater training requirements for accreditation authorities, reviewers and education providers upon implementation of revised standards.
This study was not without limitations. The perspectives of accreditation captured in this study represent those from a single institution with a key stake in the accreditation process across a variety of health professions so may differ from other institutions and those not as closely aligned to the process. Given the sample of academics from this single institution, the transferability of the findings to accreditation policy internationally may be limited to Australia. Accreditation policies related to the health professions represented in the study were also not explicitly analysed.
Conclusion
This study found similarities in the experiences of academic professionals involved in health professions accreditation processes and their purpose in supporting the development of safe and effective work-ready graduates. Tensions including competition between universities and the inflexibility of accreditation bodies around input- versus outcome-focused education were revealed in the processes that aim to support the development of safe and effective work-ready graduates. This influenced participants’ conceptualisation of accreditations’ value. The findings provide crucial insights for potential changes by accreditation authorities to policies and processes such as increased investment in reviewer recruitment and training, training for education providers and more frequent revision of accreditation standards. Changes such as these may assist enactment of accreditation policies by education providers and ensure innovations in education are not stifled in the pursuit of work-ready graduates.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Faculty of Medicine, Nursing and Health Sciences, Monash University Learning & Teaching Grants 2019.