
Abstract
This article offers a critical analysis of the role of public health regulation on tertiary education in Aotearoa New Zealand and, specifically, the requirements and processes of Responsible Authorities under the Health Practitioners Competence Assurance Act for the accreditation and monitoring of educational institutions and their curricula (degrees, courses of studies, or programmes). It identifies and discusses a number of issues concerned with the requirements of such accreditation and monitoring, including, administrative requirements and costs, structural requirements, and the implications for educational design. Concerns with the processes of these procedures, namely the lack of educational expertise on the part of the Responsible Authorities, and certain manifested power dynamics are also highlighted. Finally, the article draws conclusions for changing policy and practice.
Keywords
Introduction
The provision of publicly-funded education and the practice of health professions are both highly regulated in many parts of the world. Within the context of Aotearoa New Zealand, education and health practice are located at the convergence of the New Zealand government’s interest in quality, accountability and public safety (Shaw and Donaldson, 2020). Further, the education of students within the health professions is positioned at the interface of education and health, making it vulnerable to any political and bureaucratic tensions between these two significant sectors. Traditionally, health professions have favoured vocationally-based training and have been somewhat suspicious of higher/tertiary-based education courses and programmes, a good example of this is nursing education (Robinson and Griffiths, 2007). This emphasis in effect viewed – and still views – learning and development as firmly embedded in practice settings, based on an apprenticeship-style model of learning. However, over recent decades, the education of health professionals has moved into the higher/tertiary education sector and developed an emphasis on evidence, knowledge, and critique (Tudor and Shaw, 2016). Tensions between these different approaches to training and education remain and relate as much to funding streams as to educational philosophy and professional identity. The education of health professionals is a particularly complex area because the legislation governing health professional practice extends to an interest in the design and delivery of education (Health Practitioners Competence Assurance Act 2003 [HPCAA or “the Act”] S118(c)). Finally, issues and challenges with regard to the design and delivery of pre-qualifying health professional courses were identified in the recent Health and Disability System Review (2020).
In Aotearoa New Zealand the education of health professionals occurs in the tertiary education sector. There are 17 Responsible Authorities (RAs) listed on the Ministry of Health website. As some of them oversee more than one discipline/profession, there are a total of 24 disciplines regulated by RAs under the HPCAA. Within the tertiary sector, most of the universities provide education to prepare graduates for some of these disciplines/professions and thus are required to meet the initial accreditation as well as subsequent monitoring requirements stipulated by RAs. In Aotearoa New Zealand the HPCAA establishes RAs as separate entities, responsible for establishing their own competencies and educational requirements. Other countries have taken different approaches to collaboration between the regulatory agencies ( Bogossian and Craven, 2020; Lahey Fierlbeck, 2016; Leslie et al., 2018). Of the New Zealand universities, Auckland University of Technology (AUT) provides education to prepare graduates for 14 areas of health professional practice – 12 of which are overseen by 10 RAs. As such, AUT is the largest education provider in the country. In 2019, AUT graduated approximately 1500 students into the health professions. Table 1 summarises the number of institutions accredited to provide pre-registration education and the disciplines AUT teaches predominantly within its Faculty of Health and Environmental Sciences. In presenting this Table, we are focusing firstly on the health discipline (as academic) and the profession; we are not implying that the RA has dominion over the discipline and/or profession (Tudor, 2016).
Disciplines/professions, relevant Responsible Authority (RA) and number of pre-registration programmes.
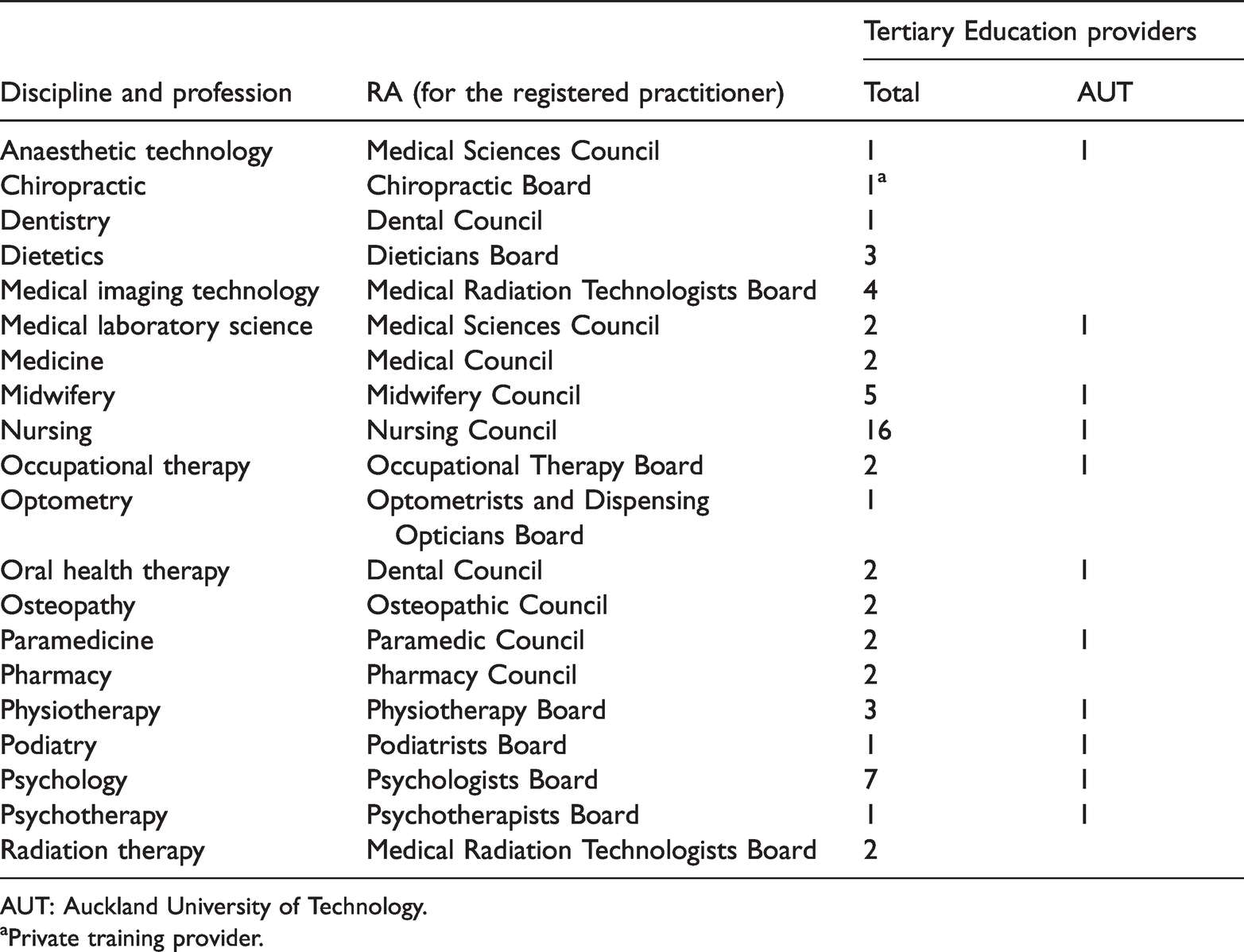
AUT: Auckland University of Technology.
aPrivate training provider.
As seen in Table 1, while in Nursing, Psychology, and Midwifery, AUT is one of 16, 7 and 5 providers, respectively, in other disciplines it is one of fewer providers; in Anaesthetic Technology, Podiatry, and Psychotherapy it is the only provider. As such, AUT, its Health Faculty and, within that, its School of Clinical Sciences, is well placed to appreciate the processes and challenges of accreditation and monitoring.
The critique of the processes, costs, and value of RAs undertaking the accreditation and monitoring of educational institutions and health professional degrees, courses of study, or programmes (hereafter ‘courses’) is informed by the authors’ experiences of developing such courses for accreditation and participating in ongoing monitoring processes imposed by RAs in addition to those required within the tertiary education sector. Our experience and expertise, which includes being teachers/educationalists, academics, and managers, also extends to various advisory and consultancy roles relating to health professional courses offered beyond our own institution, and country. On the basis of our analysis and experience, we argue that elements of the educational accreditation and monitoring processes asserted by RAs are an inefficient and unnecessary burden on education providers and distract resources from the delivery of sound and innovative health professional education. In this context, we suggest it is timely to distinguish areas of expertise and influence in order to clarify the respective scopes of educational and health professional agencies in relation to educational design and quality evaluations.
Method and methodology
In order to undertake this analysis, we identified a number of relevant documents and texts, namely: the published criteria for programme accreditation (which are available on the websites of the respective RAs); notes from a meeting of education providers with one RA (personal and confidential); communication about accreditation and monitoring expenses for a short course for a specific region/population; communication from another RA seeking access to all students and staff (including entering classrooms), student files, and any clinical sites used for student placement (in the form of emails) during a programme monitoring visit; communication between staff at one institution about the information needed to be repeated in review documents (e-mails).
We are mindful of the anecdotal nature of some of the communications reported, and of the personal nature of personal notes. However, these documents were all carefully chosen to provide illustrations and snapshots of the issues we seek to analyse. We also appreciate the potential sensitivity of using such illustrations but have ensured that none of the people or organisations involved are identifiable in any of the examples that are not from published and publicly available documents. Our intention is to illuminate rather than criticise and we believe that providing such examples may help readers to connect with the issues and encourage reflection on their own experiences.
Having identified certain themes, we undertook a further analysis of the published criteria for programme accreditation, as well as an analysis of budget and expenditure in relation to accreditation and monitoring.
As employed academics at a New Zealand university, we are critics (see Education Act 1989, Section 162, and Background section of this article). As we were considering various forms of text, our method was that of an exegesis, by which the researcher seeks to explain and interpret the text in order to illuminate it. Arguably, the exegetical method (originally from Biblical studies) is a critical one, but, in any case, putting the context of our employment and role together with this method, we claim this as a “critical exegesis”, if not a “historical-critical exegesis” (Krentz, 1975). This is one that seeks: to present a body of facts; to illuminate the past, in this case, a political and administrative context; to understand the significance of events, in this case, legislation and policies, and to interpret them; and to understand motives as well as actions and policies.
It follows that our underpinning methodology is critical theory. In our case, and evolving from previous work together (Tudor and Shaw, 2016), it is critical theory based on critiques of power and control and, in our context, the premise that ‘teachers and curriculum have been subjected to intensifying policy regimes that attack academic freedom and discourage critical social analysis’ (Ross, 2018: 380). Thus, this present work and article is part of a wider and ongoing project of examining educational phenomena in the context of political and economic forces and policies (Rata, 2014). In practical terms, we used contextual positioning (Ralph et al., 2014) to consider ourselves in relation to the data (documents) before reading the texts.
Before we elaborate our analysis, we offer some brief background regarding the regulatory context of educational institutions and courses in legislation in Aotearoa New Zealand.
Background
Approval of educational institutions and courses under the Education Act 1989
Educational courses are offered by institutions of various types. The educational regulatory context in Aotearoa New Zealand addresses the approval and accreditation of both institutions and the courses they offer. Courses of study (usually degrees) designed for the purposes of educating students in the health professions are predominantly based in higher/tertiary education settings. New Zealand law outlines the characteristics of various types of educational institutions. Universities have five responsibilities including providing a repository for knowledge and expertise, research-informed teaching practice, and being a critic and conscience of society (Education Act 1989). Under Section 162 of the Education Act 1989 a university is defined as having the following characteristics: They are primarily concerned with more advanced learning, the principal aim being to develop intellectual independence: Their research and teaching are closely interdependent and most of their teaching is done by people who are active in advancing knowledge: They meet international standards of research and teaching: They are a repository of knowledge and expertise; and They accept a role as critic and conscience of society … (Education Act 1989)
Two regulators are responsible for setting and maintaining the standards for institutions offering tertiary education and qualifications in this country. Education providers are responsible to one or the other of these agencies, both of which are established under the Education Act 1989.
Universities themselves, and the courses offered by them, are overseen by Te Pōkai Tara Universities New Zealand (TPTUNZ) through the Committee on University Academic Programmes (CUAP), which lists ‘quality assurance matters in the universities’ and ‘course approval and moderation procedures” as two of its functions (TPTUNZ, 2020). The CUAP oversees a rigorous course approval process and sets standards for ongoing quality management which are monitored by way of comprehensive audit and review cycles. The education of health professionals is based on curricula which reflect the interests of both academia and the professions (Powell and Walsh, 2017). In this country, these are represented by TPTUNZ and its CUAP and the RAs which, as governmental agencies, effectively convey policy as they require conformity with national standards (Ralph et al., 2015, 2017).
The New Zealand Qualifications Authority (NZQA) defines its responsibilities as including ‘setting standards for qualifications in tertiary education’ by ‘monitoring and reviewing standards for qualifications’, and by making rules to support ‘national consistency’, outside the university sector. The NZQA has processes for the registration of education providers, accreditation of courses, approval for providers to deliver courses, and the monitoring of them (NZQA, 2020) and, therefore, accredits and monitors health professional education programmes outside the university.
Both these statutory agencies – TPTUNZ and NZQA – have requirements for quality including educational practice (the design and delivery of qualifications); the resources required to deliver courses (staffing, buildings, library access); and content expertise (currency and appropriateness of staff, consultation with the relevant sector). The need for quality systems, nationally agreed and recognised standards, and organisations to approve and monitor qualifications is not disputed. What is disputed – or what needs to be critiqued and questioned – is the complexity, expense, and overlap of the accreditation and monitoring of educational institutions as it is currently undertaken by RAs, in addition to the work of NZQA and TPTUNZ.
Approval of educational institutions and courses under the Health Practitioners Competence Assurance Act 2003
In 2003 the HPCAA repealed 11 statutes governing 13 professions, and included midwifery and osteopathy, since which two other professions have met the criteria for incorporation into the Act (psychotherapy in 2009, and paramedicine in 2020). The main criterion for a profession seeking registration under the Act is that it poses a risk to the public, for a critique of which with regard to the admission of psychotherapy, see Tudor (2017). This legislation enables RAs to define scopes of practice, and to register and monitor practitioners. The various RAs report to the government through the Ministry of Health. In relation to educational institutions and courses, the HPCAA enables RAs to prescribe the qualifications required for scopes of practice, to accredit and monitor educational institutions and degrees, courses of study, or programmes (S118(a)); and to set standards for clinical competence, cultural competence, and ethical conduct (S118(i)).
The word ‘enables’ is significant here in that, while the Act gives RAs this authority, Section 12 of the Act (prescription of qualifications) does not prescribe how or the extent to which they accredit and monitor such institutions and/or courses. This section of the Act is also significant in that it allows RAs in the health sector to accredit and monitor institutions and/or courses in the educational sector which, however, are already accredited and monitored by educational regulators TPTUNZ and/or the NZQA.
Analysis of health professional courses’ accreditation and monitoring requirements
The requirements and processes for course accreditation and monitoring are complex and involve considerable resources; as well as a good deal of stress for the educators and managers involved (Davis, 2018). In the light of our own experience (as teachers/educators, paper and programme leaders, academic leaders, and managers, and as members of academic committees at all levels of our own tertiary institution) and the identification of a number of accreditation-related issues across undergraduate and postgraduate health professional degrees, we sourced and analysed various documents (see method and methodolgy above). In this part of the article, we focus on our analysis of the requirements of accreditation and monitoring, under which we identify four themes: (a) administrative requirements, (b) costs, (c) structural requirements, and (d) educational design. In the subsequent part of this article we present our analysis of the processes of accreditation monitoring, following which we discuss both, and present our suggestions for policy reform to address the identified problems.
Administrative requirements
The requirements of the approval (the TPTUNZ CUAP) and accreditation and monitoring (the RAs) of health professional education/training courses are complex and time-consuming, and warrant consideration and critique. Extensive and detailed documentation is assembled and submitted, often with many hard-copy duplicates; some RAs require 10 such copies.
Duplication occurs when the educational quality agencies and the RAs have similar requirements. These relate to physical resources, the qualifications of staff, and the capacity to deliver the course and carry out fundamental educational processes (see Table 2).
Examples of health professional courses offered by AUT that have similar criteria for Responsible Authority (RA) accreditation and monitoring.
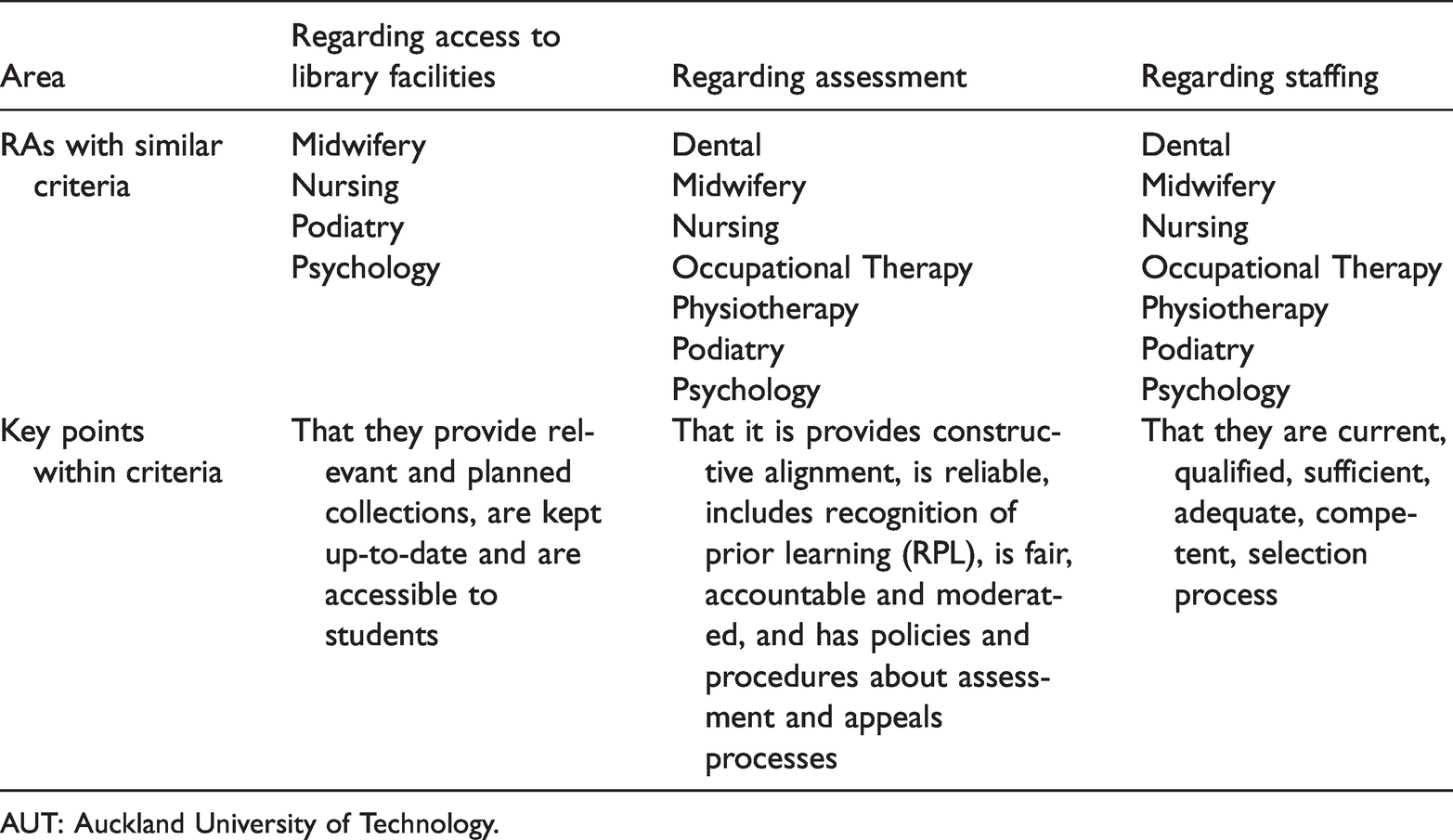
AUT: Auckland University of Technology.
It is, of course, reasonable for any higher/tertiary education provider to accept that the quality criteria required by TPTUNZ and the NZQA will address fundamental requirements such as resources, educational practices and staffing within their approval, accreditation and monitoring processes. It is the duplication of such information, however, that is a problem as there are standard requirements which are repeatedly provided to all RAs. These include details about resources, educational design and quality processes such as staffing policies, the library collection and student support systems. The re-assembling of this information (which, also, may be required in an updated format since the previous visit of the accreditation panel) is costly and time-consuming, and would not be necessary if the RAs instituted a model that standardised the format across the sector and considered options for addressing duplication and unnecessary resource requirements (Friedman et al., 2017). Interestingly, regarding library facilities, the RAs appear more concerned about their physical existence (and during onsite visits often want to be shown around the library), while the CUAP is more concerned about students’ electronic access to libraries.
Costs
There is a considerable cost to the organisation in collating and providing the required information to panels, though the most obvious cost is that of the visit itself. The fees relating to approval/accreditation and monitoring are gazetted (in the New Zealand Gazette) but require further scrutiny in terms of the monitoring term and whether the fee is standard/maximum or a daily rate. When providers offer more than one course that requires monitoring by the same RA, negotiations are required for the panel processes to be consolidated. Institutions often try to embed their own educational monitoring requirements, such as periodic reviews, into the formally scheduled RA panel visits in order to reduce duplication within the organisation. The complete breakdown of these costs, based on a search of notices published in the New Zealand Gazette, and other information published on the websites of the 17 RAs (as of 31August 2020) is summarised in Table 3.
The costs of accreditation of health education courses by Responsible Authorities (RAs) under the HPCAA 2003.
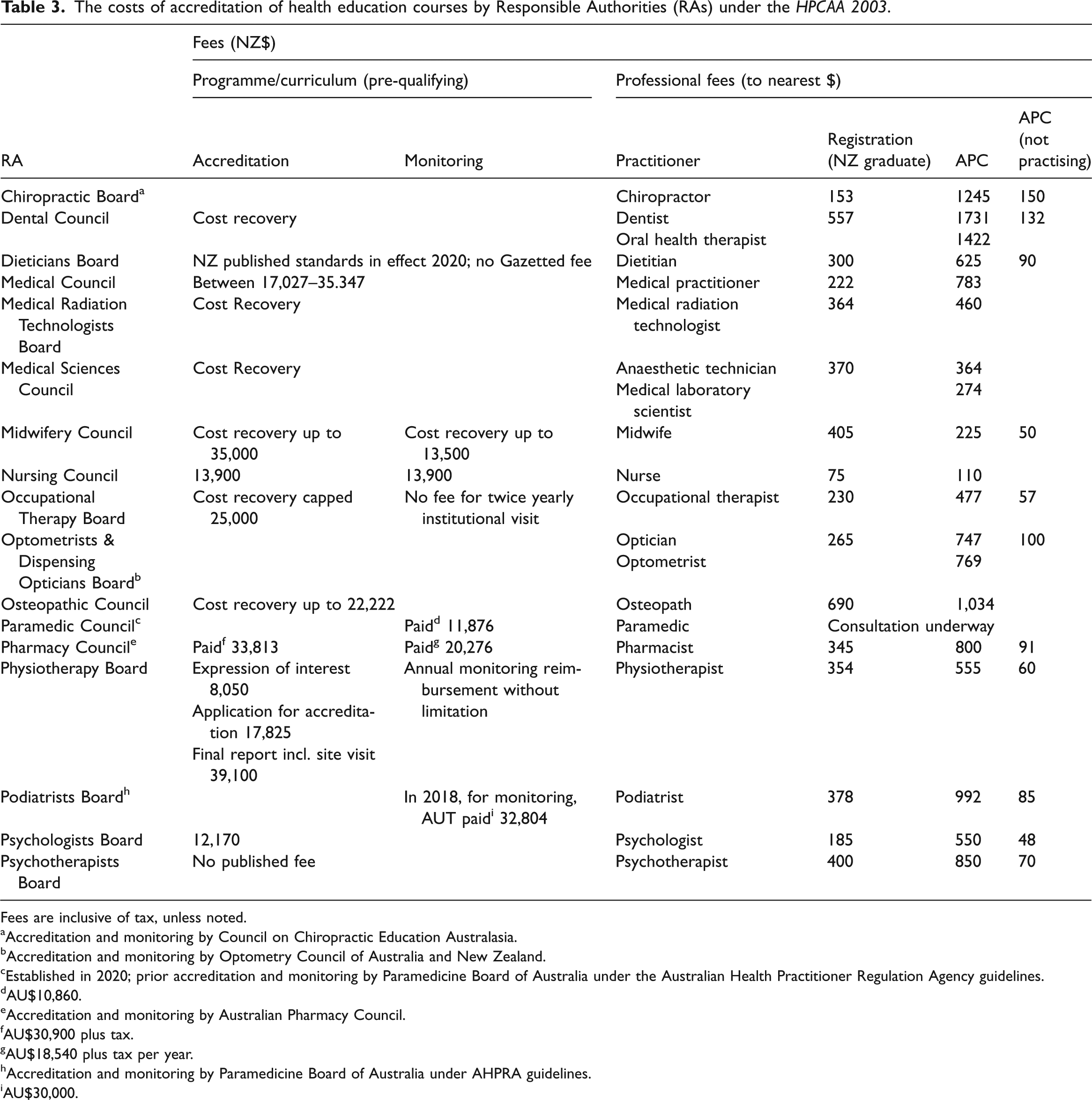
Fees are inclusive of tax, unless noted.
aAccreditation and monitoring by Council on Chiropractic Education Australasia.
bAccreditation and monitoring by Optometry Council of Australia and New Zealand.
cEstablished in 2020; prior accreditation and monitoring by Paramedicine Board of Australia under the Australian Health Practitioner Regulation Agency guidelines.
dAU$10,860.
eAccreditation and monitoring by Australian Pharmacy Council.
fAU$30,900 plus tax.
gAU$18,540 plus tax per year.
hAccreditation and monitoring by Paramedicine Board of Australia under AHPRA guidelines.
iAU$30,000.
Some costs could be reduced by insisting that the schedules are as efficient as possible, such as reducing travel time and including two courses in the same visit or day. Nevertheless, the overall cost to the taxpayer is considerable when the number of institutions offering the courses is considered. For example, there are approximately 16 schools of nursing in Aotearoa New Zealand and the longest period between accreditations is five years. When the cost of a two-day visit every five years is calculated for 16 undergraduate nursing courses, the overall cost every five years is NZ$444,800 – just for the monitoring visit fee. The ongoing panel-related monitoring costs for the Faculty of Health and Environmental Sciences at AUT in 2018 alone were budgeted at almost NZ$180,000.
While the RA fees for accreditation and monitoring are the most easily quantifiable expense, there are many other associated costs. The schedule of fees set by RAs have the potential to limit the ability of educational providers to deliver courses, especially those smaller providers in the private sector; we know of several such providers in one sector that have ceased trading since the advent of the state registration of its practitioners. We are aware of one situation in which a fully accredited provider was prepared to travel from a main centre to a province to offer established practitioners education about a specific clinical skill. The relevant RA required that the educational provider seek a further full accreditation to teach this specific skill on this other site; the cost was so prohibitive that the education provider was unable to do so, with the result that a very significant public health need was unable to be met.
Structural requirements
Some accreditation and monitoring criteria refer to the status and position of the profession within the educational institution. For example, the criteria outlined by the midwifery, occupational therapy and podiatry RAs specifically refer to the profession being positioned as ‘distinct’ from others within the institution. This implies a structural expectation of education providers which does not fall under the mandate to prescribe qualifications and accredit and monitor institutions (HPCAA Section 118). Opinions or assertions about the structure of an organisation and the location or role of a profession within it are political positions rather than educational imperatives or monitoring mandates. Such requirements or even suggestions reflect an understanding of territory and boundaries which runs counter to the international emphasis on interprofessional education and collaborative practice.
Educational design
The curricula of health programmes are often tightly prescribed by RAs. This almost always includes a specific number of clinical hours, and sometimes how they are scheduled. For example: The programme provides a minimum of 1100 clinical experience hours for all students, with all students being entitled to 1500 clinical experience hours in which to demonstrate competence. Simulation hours cannot be included in clinical experience hours. (Nursing Council of New Zealand (NCNZ), 2002/2020: 62) Extended clinical experience of 360 hours minimum is included in the final semester of the programme to enable the student to meet the Council’s Competencies for the registered nurse scope of practice (December 2007) and as preparation for transition to practice. (NCNZ, 2002/2020: 62).
Another complexity for education providers is that the RAs have different definitions of a clinical hour. For some, reflection and debrief between clinical sessions is included, while others have indicated that close to 60 minutes of interaction between patient, student and educator constitutes an hour of learning. There is no evidence that a specific number of hours or ‘time served’ corresponds with clinical competence (Coyle, 2007). There is also no evidence that scheduling a specific number of hours at particular points in a course is essential for clinical learning and preparation for practice.
The use of simulation in health professional education courses has been debated for many years. The most comprehensive research into simulation in health professional education (Hayden et al., 2014) recommended that a proportion of simulated learning is suitable for inclusion in clinical learning components of courses. The Podiatry Board has acknowledged simulation as an ‘emerging innovation for developing clinical competencies’ (Australian and New Zealand Podiatry Accreditation Council, 2015: 14). While the NCNZ recognises simulation in the criteria that states, ‘students have access to simulation learning resources in order to prepare them appropriately for clinical experiences to ensure the safety of health consumers, students and staff’ (NCNZ, 2020: 65); it clearly discounts simulation in relation to calculating the total number of clinical hours.
Education is informed by both content and educational process. As a result, there is a reasonable expectation that the curriculum and learning experience will be evidence-based and developed and delivered by educators with appropriate expertise. It is also reasonable to expect that any state-funded higher/tertiary education provider in Aotearoa New Zealand that is accredited by NZQA or TPTUNZ will be delivering courses and implementing quality systems that ensure they meet the expectations set out in the Education Act 1989.
Analysis of health professional courses’ accreditation and monitoring processes
Having analysed the requirements of the accreditation and monitoring procedures, we turn our attention to the processes involved, which we identify as concerning: the emphasis on minutiae, the educational expertise of the authorities and panels and the power dynamics involved in the whole procedure(s).
The lack of educational expertise of the RAs and panels
As the RAs assert their role in relation to educational courses, they assume varying degrees of educational expertise. However, there is often little evidence of sound educational evidence or expertise underpinning their work; and, indeed, there is no requirement for RAs to have any educationalists, teachers or trainers on their boards.
The changes to delivery of undergraduate midwifery degrees in Aotearoa New Zealand is a poignant example. A number of years ago, the length of pre-qualifying midwifery education was extended from three to four years. A decision was made by the Midwifery Council that the four academic years needed to be delivered in three calendar years. There appeared to be no educational rationale; rather, a drive to increase the size of the workforce quickly. At the time, a number of tertiary health education providers had serious reservations and at least one withdrew from offering midwifery education. A number of years later, it is clear that this model of delivery placed enormous stress on staff and students and negatively impacted on the success rates of students and, therefore, the numbers of graduates entering the workforce. This was an example of an RA requiring changes to educational practice, not with regard to education but in order to meet another purpose, in this case a workforce issue.
Following submission and consideration of the documentation regarding the course (curriculum, facilities, quality etc.), a panel visit normally takes place. Generally, panels comprise members of the RA along with representatives from the particular health sector and other education providers. Some accreditation and monitoring panels include an Australian representative because some RAs have delegated their accreditation and monitoring to Australian organisations (i.e. podiatry and, prior to 2020, paramedicine). Other RAs have contracted their accreditation and monitoring procedures to larger local (national) RAs (i.e. Osteopathy and Paramedicine). While panel members work hard and are, for the most part, well-intentioned, there is often a lack of educational expertise on the panels, which is apparent when members refer to how they were educated (sometimes decades earlier) as the basis of their evaluation of the documentation, procedures and discussion. During one monitoring visit a member of a panel suggested that she could share the curriculum from her own institution. However, apart from the question of intellectual property, as the institute in question was geographically and contextually far removed from the tertiary institute being monitored, this offer demonstrated a poor appreciation of boundaries, a lack of regard for the local course and minimal insight into the role of a panel member.
One way in which this lack of educational expertise gets played out is in a compensating overemphasis on minutiae. Higher/tertiary education providers recognised by either NZQA or TPTUNZ to manage the design and delivery of educational courses already associated administration (arguably too much). However, we are aware of course monitoring documents from RAs that require administrative minutiae such as a ‘desk file’ (literally a hard-copy guide as to how to run the office or, in this case, the administrative tasks relating to a course). Other RAs state very specific details about the delivery of the educational course and the student journey (see Table 4).
Requirements of Responsible Authorities (RAs) and responses.
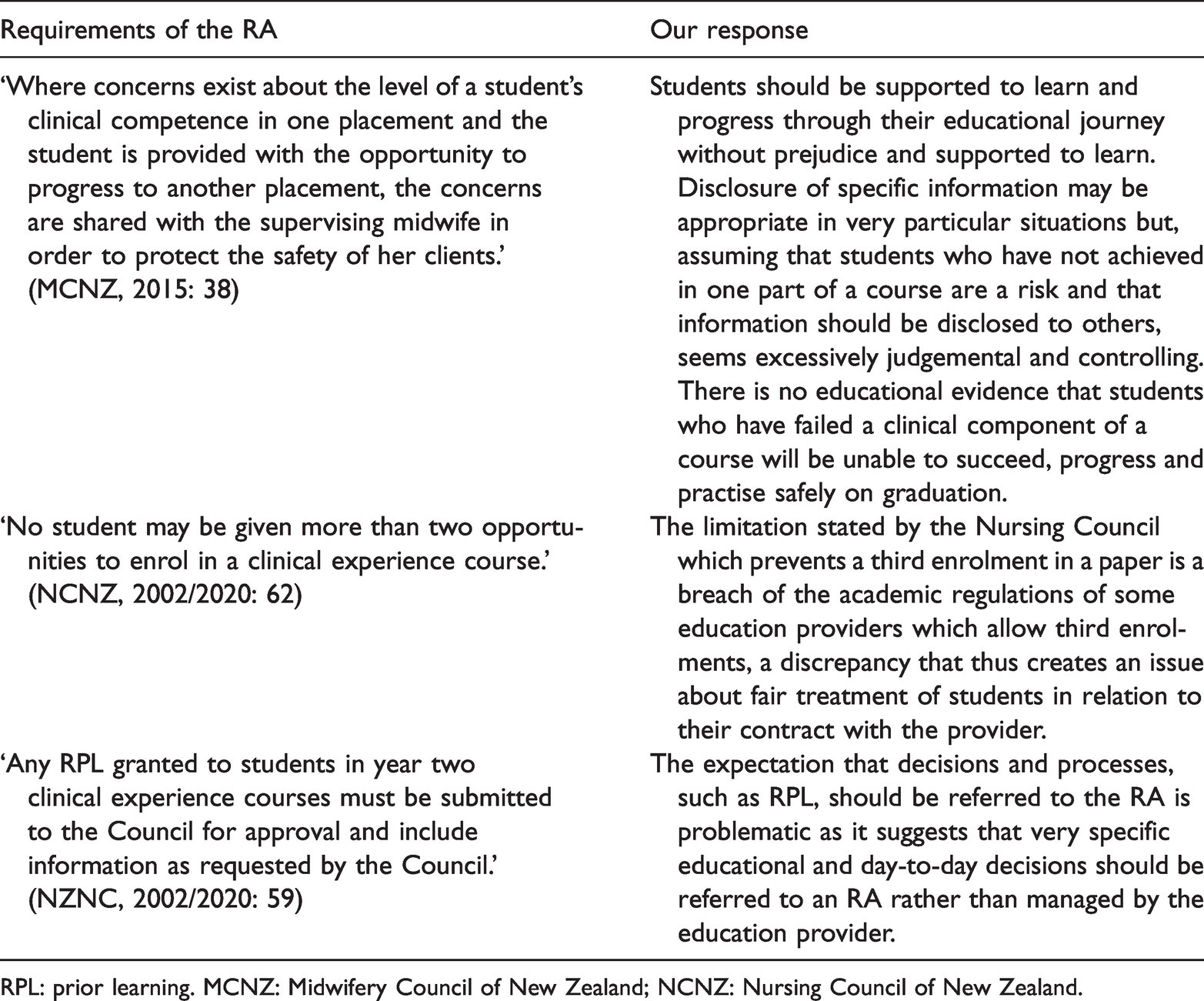
RPL: prior learning. MCNZ: Midwifery Council of New Zealand; NCNZ: Nursing Council of New Zealand.
Power dynamics
Our reading and analysis of the documentation and texts, as well as our experience as educators and managers appearing before accreditation/approval and monitoring panels for health professional education courses, reveals some subtle and not so subtle power dynamics which represent certain discourses about regulation.
Cultural
Education and health care organisations within Aotearoa New Zealand are obliged to recognise and respect culture. Te Tiriti o Waitangi establishes the basis for this obligation which is supported in legislation and expectations about the design and delivery of state-funded education and health care and employment. The concept of “cultural safety” in health professional education and practice has its home in this nation (Ramsden, 2002). One education provider received questions from an overseas member of a panel, prior to a monitoring visit, asking how it ensured cultural competence. The provider responded with reference to Te Tiriti, legislation, and practice in our health and education sectors and, specifically, the Faculty and course. Despite this, the same question was asked at the panel visit. The lack of appreciation of context, the disregard for the answer that had been provided, and the process of explaining the response in the presence of tangata whenua was itself represented a lack of cultural sensitivity. This illustrates the need for panels to be appropriately constituted and briefed, particularly when such visits are so expensive.
Policing
The nature of regulated practice and education means that organisations and individuals need to interact with one another and, in doing so, they may not always agree. Usually, this is done in a collegial and respectful way. There is, however, in the accreditation/approval and monitoring process, a risk that power and, specifically, ‘power over’ may be asserted or acted out. A startling example of this occurred during one meeting when a member of the council of one RA said to a group of leaders from educational providers, ‘We are the police … and must be obeyed.’ Such a comment not only demonstrates a complete lack of regard for the educators and the institutions they represent but also constructs the RA in a policing role.
Another example of this dynamic and discourse was when a member of an NZQA panel asserted that an education provider had ‘breached a rule’ when its Academic Board changed the order in which two papers were delivered within a health professional education curriculum. The panel member went on to explain that they had been involved in writing this rule (referring to it as a ‘beautiful rule’), and that they believed that changes to learning outcomes within courses constituted curricula ‘creep’ which was unacceptable and required NZQA notification and approval – which was not the case.
We have experienced a tendency for panel members to behave in a manner that suggests they are seeking to disprove the education provider, and to do so through an interrogative style of questioning (which represents a certain method), based on an adversarial model of assessment and monitoring (the methodology). These include individual panel members announcing that they will seek to ‘re-mark’ individual student assignments during an accreditation visit to test moderation practice; expecting to be able to ‘walk into’ any clinical setting or classroom they wish during the period of the visit to ‘spot check’ the quality of the educational experience, and to access the files of individual students.
Discussion
From the above analysis, we identify four points for discussion, which we summarise as: (a) consolidation and efficiency; (b) expertise and competition; (c) collaboration and inter-professionalism; and (d) engagement and parallel process.
Firstly, the development, delivery, and evaluation of health professional education requires both educational and discipline-specific expertise. Regulatory agencies in both the fields of educational provision and practitioner regulation have a mandated interest in these courses of study and the institutions that deliver them. The concept of consolidating administrative practice of RAs in the form of a secretariat has been discussed for some time and, in 2009, a report to the Minister of Health recommended that efficiency gains could be made by amalgamating RAs (Ministry of Health, 2009). Such efficiencies could include the management of Annual Practising Certificates (APCs) across all health disciplines/professions. The 2019 revision of the Act (section 116) formalises the concept of amalgamation and introduces regular reviews of RAs (section 122) with specific reference to efficiency. The accreditation of monitoring of educational courses could be more efficiently managed in such a model by centrally holding generic information about each educational institution such as their human resources policies, regulations and, for instance, details of library resources.
Secondly, the RAs constituted under the HPCAA are involved in the approval/accreditation and monitoring of health professional education; yet some of the criteria by which they are mandated overlap with similar requirements that have been integral to the tertiary education sector for some time. This tension regarding expertise and competition was illustrated to one of the authors when they were told that, in order to teach on an academic programme, they had to be a registered health practitioner (not a registered teacher/educationalist). The expertise of educational institutions can be relied upon to develop education that is evidence-based and delivered in a manner that safely and fairly teaches and assesses students against competencies set by the RAs. Transparent quality assurance processes demonstrate their practice and, if designed appropriately, could meet the needs of the various compliance agencies and prevent duplication. Ideally there would not be any sense of competition between providers and regulators (or amongst regulators) about educational practice. The expertise of education providers is the design and delivery of education while the expertise of the RAs is in regulation of health professionals. Respecting and sharing this expertise has the potential to enhance the professions, educational practice, and the communities that are served by graduates.
Thirdly, the manner in which these processes are carried out is complex and expensive and, as we have argued, lacks sound educational rationale. Internationally, there is an emphasis on interprofessional education and collaborative practice. Such approaches, which encourage cross-sectorial engagement, are demonstrated when student learning experiences involve the educational providers taking a key role in modelling health care provision. This has been demonstrated in Sweden for many years with the provision of interprofessional clinical learning in ‘training wards’ (Wilhelmsson et al., 2009). It is also illustrated in a Canadian approach (Mann et al., 2009). It is time to challenge the rock–paper–scissors relationships between regulatory authorities, health education and the role of universities as critic and conscience of society, respectively, and instead co-create new, collaborative space between educational institutions and professional associations/bodies in the health sector.
Fourthly, this discussion raises organisational (territorial) and philosophical issues as well as practical ones as there is significant duplication between some RA requirements and those of the educational agencies approving/accrediting and monitoring qualifications. Duplication results in considerable inefficiencies, expense and overlap, particularly for providers offering a number of courses and requiring the oversight of more than one RA. From a philosophical perspective it is wise to model student/teacher engagement on the dynamics we value between practitioners and patients. In a similar way the evolution of health professional education would benefit from genuine engagement between sectors and fields of expertise, rather than RAs or particularly powerful groups of practitioners asserting they have the answers and others should follow their guidance. The establishment of a more collaborative model between professions could assist with interprofessional aspirations (Bogossian and Craven, 2020). Lahey and Fierlbeck (2016) have outlined both top-down and bottom-up approaches to such collaboration.
The Faculty of Health and Environmental Sciences at AUT is uniquely positioned within Aotearoa New Zealand to appreciate the complexities of both the health and education sectors. This complexity is not new and one the Faculty is committed to engaging with. Our experience of the accreditation and monitoring carried out by RAs, in addition to the quality management requirements of the university sector and the clinical disciplines with whom we constantly engage, is challenging for a number of reasons. The education of health professionals would benefit from an approach between agencies and across sectors that was informed and managed in a way that reduced duplication, and profiled and valued best practice.
Future directions
Based on our analysis and discussion, we identify four directions for health – and a healthier – education for health professions in Aotearoa New Zealand. We also suggest that these directions and related policy development represent a ‘right touch’; that is, a ‘light touch’ (Professional Standards Authority, 2015). An administrative structure which enables RAs to agree on and manage generic criteria for all education providers offering health professional curricula (degrees, courses of studies or programmes) and, thereby, reduces the cost and administration for the educational institutions and the RAs and, ultimately, for students and the taxpayer. The question for policy development in this regard is whether health professions are willing to think and act more generically and to let go, and perhaps to forgo a certain (over)specialisation. In our own institution, this was represented by the proliferation of courses on research in a number of health disciplines in preference to one or two courses on research methodologies and methods that are applicable across all health disciplines. A clear distinction between educational infrastructure and quality provided by tertiary institutions, and quality assurance agencies (in Aotearoa New Zealand, TPTUNZ, the NZQA, and RAs). In terms of policy development and planning, this requires ministries of health and education discussing and agreeing about their respective roles in this regard. Another option would be to combine such ministries and departments, though, interestingly and perhaps significantly, there are very few examples of this (one exception being the Ministry of Education and Public Health in Brazil, 1930–1953). A limitation (within the HPCAA, with regard to current section 118(a)) of the RAs’ power to define educational practice – being an example of making a clearer distinction between health and educational policy and practice, which would be more consistent with current international practice with regard to policy development. An appreciation of and respect for the different, heritages, expertise and roles of all parties contributing to the accreditation of health professions curricula. Within the context of Aotearoa New Zealand this should of course involve Māori as tangata whenua – and we make this point specifically as the HPCAA does not explicitly refer to Te Tiriti o Waitangi. The policy development in this regard, both in Aotearoa New Zealand and in other countries (such as Australia, Canada and the United States), would involve a radical repositioning of all policy, including education and health, so as enhance the authority of indigenous people(s) over their lives, as outlined in relevant treaties and in the United Nations’ (UN) Declaration on the Rights of Indigenous Peoples (United Nations, 2007) (specifically Articles 14, 15, 17, 21, 23-25,and 29).
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.