
Abstract
Prehospital emergency medical care (EMC) personnel in South Africa are required to participate in continuous professional development (CPD) to maintain clinical competence. This study examined the scope and accessibility of CPD opportunities, focusing on relevance, lifelong learning, and quality assurance. A narrative review of South African and international regulatory documents and scholarly literature was conducted, supplemented by archival analysis of EMC CPD activities accredited by the Health Professions Council of South Africa between 2017 and 2020. Reflexive thematic analysis highlighted equity and adult-learning considerations. Findings revealed significant geographic disparities, with CPD concentrated in urban provinces. Activities were predominantly workshops and guideline updates, reflecting a narrow, compliance-driven model that limits collaborative, practice-based learning. Minimal practitioner involvement in topic selection and an emphasis on continuing education units further constrained contextual relevance and meaningful engagement. Quality assurance processes were inconsistent and largely dependent on the organiser. Drawing on adult education theories, including andragogy, constructivism, social learning, and self-directed learning, the study critiques current practices and proposes a practice-oriented, learner-centred framework. This reconceptualisation positions CPD as more than regulatory compliance, advancing equitable, lifelong professional growth with implications for educators, programme designers, and regulators.
Introduction
Continuous and rapid developments in all fields of healthcare have necessitated continuous professional development (CPD) to maintain and refresh healthcare professionals’ specialised skills and knowledge (Henwood & Taket, 2008). CPD is the constant process of maintaining, enhancing, and deepening knowledge and abilities, and of developing the personal characteristics required of highly skilled practitioners (Eddy et al., 2015; Gent, 2016). CPD should continue throughout the professional careers of healthcare professionals, who should be lifelong learners (Arunachallam, 2009; Howlett, 2019). By nature, the healthcare profession is dynamic, and CPD promotes professional relevance.
In South Africa, all prehospital emergency care practitioners (ECPs) must be registered with the Professional Board for Emergency Care (PBEC) of the Health Professions Council of South Africa (HPCSA). The HPCSA requires that all registered ECPs undertake CPD and prescribe core ethical values and standards for all healthcare professionals under its purview (HPCSA, 2016). This statutory body is responsible for ensuring registration eligibility and protecting the public interest by creating registers for ECPs, who must meet the prescribed standards of education and training, ethical behaviour, and scope of practice (HPCSA, 2017a). CPD, as a method to ensure quality assurance in the health sciences throughout a professional’s career, has changed at varying rates across the world, leading to substantial diversity in structure, standards, and monitoring (HPCSA, 2017a).
In 2017, the CPD guidelines of the HPCSA were updated to emphasise the need to address South Africa’s increasing healthcare demands (HPCSA, 2017a). To meet HPCSA registration standards, prehospital ECPs must comply with specific CPD requirements. There are two levels of CPD activities that prehospital ECPs can attend to meet the prescribed standards. These activities may have either non-measurable or measurable outcomes. Activities are presented on two levels of engagement. According to the regulator’s description, Level 1 CPD activities are once-off events. Continuing education units (CEUs) are awarded at a rate of 1 CEU per hour, with a daily maximum of 8 CEUs. Level 2 CPD activities produce measurable outcomes and include structured learning activities. Such learning and/or development activities are planned and provided by an accredited training institution (HPCSA, 2017a). An accredited assessor evaluates the learning activity and whether the required outcomes are quantifiable (HPCSA, 2017b). Some activities do not necessarily provide sufficient CEUs for a full year, and others are part of a structured learning programme (HPCSA, 2017a).
To maintain their registration as practitioners, prehospital ECPs must stay up to date through CPD (HPCSA, 2017c), as required by the Health Professions Act (Act No. 56 of 1974). Therefore, the HPCSA states that it … [e]ndorses CPD as the means of maintaining and updating professional competence, to ensure that the public interest is always promoted and protected, as well as ensuring the best possible healthcare service to the community, CPD should address the emerging health needs and be relevant to the health priorities of the country.
Despite this well-intentioned ideal, there is no ‘golden standard’ for measuring whether it has been achieved, except for the quantitative allocation of CEUs (HPCSA, 2017a). Most of the related research appears to be focused on the technical elements of CPD, and the literature on CPD was classified by Castleman (2007) into several categories, namely: • adult-learning preferences for CPD; • efficient approaches for obtaining CPD; • quality assurance/standards; • CPD regulations/policies; • technology availability for CPD; and • barriers affecting CPD.
Internationally, CPD systems differ; however, there are commonalities in content and methods that enable global standards for professional development (Health and Care Professions Council, 2017; Paramedicine Board of Australia, 2018; Qatar Council for Healthcare Practitioners, 2016). In Australia, paramedics must complete 30 notional hours of CPD per year. CPD has been standardised and may include interprofessional activities and portfolio use (Paramedicine Board of Australia, 2018). In Qatar, practitioners are required to obtain 40 CPD credits per year and to document their activities in an electronic CPD portfolio or e-portfolio (Qatar Council for Healthcare Practitioners, 2016). In the United Kingdom, CPD activities involve work-based learning, professional activities, formal education, or self-directed learning (Health and Care Professions Council, 2017).
Although attempts have been made to formalise CPD activities, the World Federation for Medical Education (WFME) (2015) raised the concern that accumulating points could become the primary goal of CPD. This concern relates to activities being defined in hours, which can be seen as a perverse incentive that may detract from the fundamental goal of CPD. Information about ECP CPD is provided sporadically and is limited, and it does not convey a holistic view of ECP CPD. Additionally, minimal literature on the structure and none on the content of CPD activities could be found. Therefore, this study aimed to address the following issues: What is the nature and extent of CPD activities available to emergency medical care (EMC) personnel in South Africa, and how do these offerings align with principles of accessibility, relevance, lifelong learning, and quality assurance?
Methods
Search Strategy
Data were collected from the following databases and search engines: Academic Search Ultimate, Africa-Wide Information, CINAHL with Full Text, ERIC, MEDLINE, PubMed, and Google Scholar. The search terms included ‘CPD paramedics’, ‘CPD’, ‘CPD policies for paramedicine’, ‘continuing professional development for paramedics’, evidence-based practice’, ‘CPD guidelines’, and ‘continuing professional competence’. These keywords were used with a Boolean search strategy (University of Southern California [USC] Libraries, n.d.).
The structured methodology associated with narrative reviews provided evidence of a thorough literature search conducted according to predetermined criteria, enhancing confidence that the review’s results and conclusions were accurate and free of selection bias (Ferrari, 2015). Figure 1 depicts the screening and selection of articles obtained by the literature search. Flowchart of the literature selection process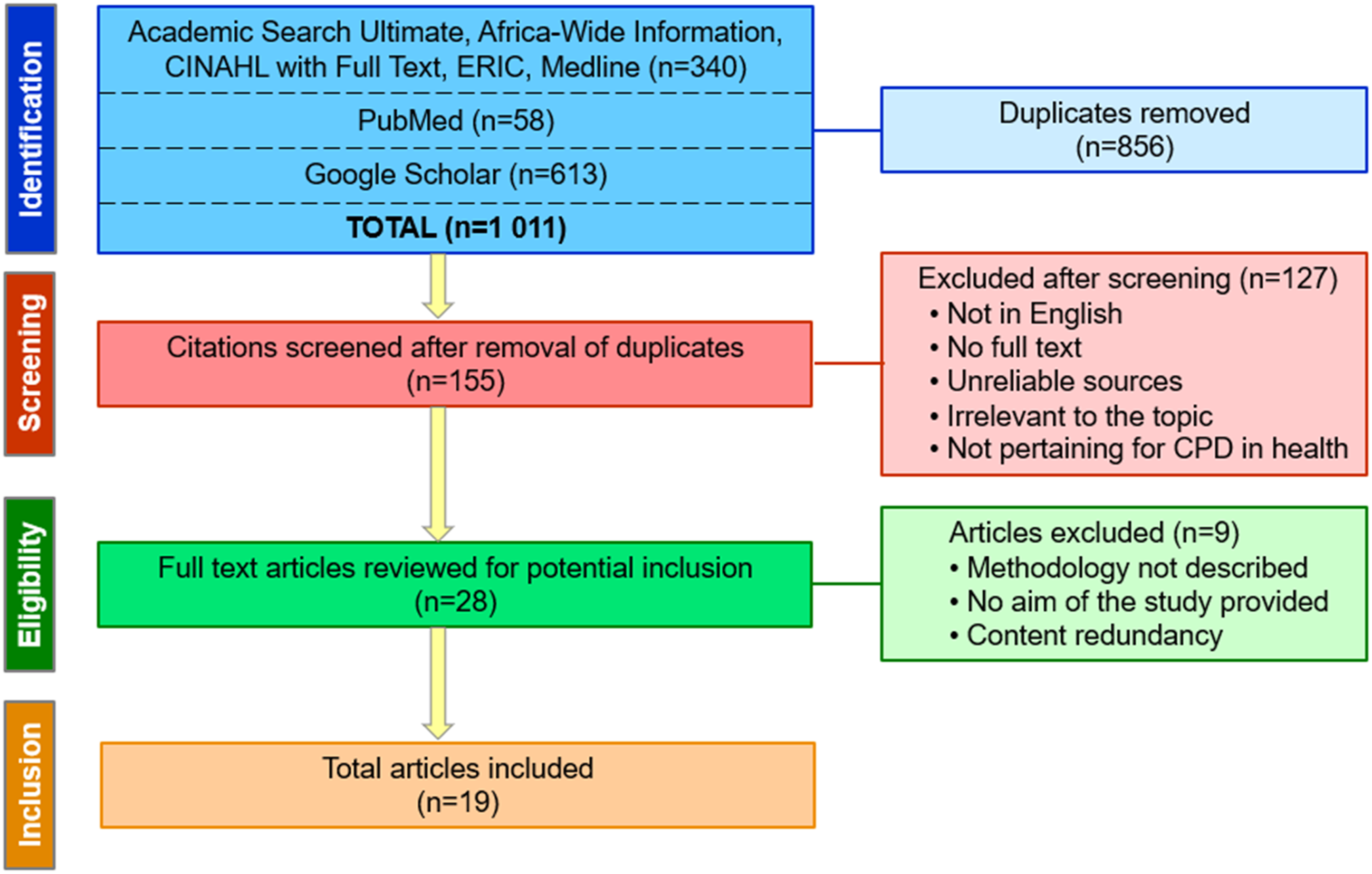
Article Selection
Due to the limited number of articles on EMC CPD, research on CPD in other health professions was included to characterise the available CPD activities. The literature search initially yielded 1011 sources. Duplicate articles were removed. The remaining articles (155) were reduced by applying the inclusion and exclusion criteria to the titles and abstracts. The full texts of the remaining publications were scrutinised, and 19 remained. Studies that met the following criteria were considered for inclusion: (i) reference to international and national regulatory CPD documentation for emergency medical services (EMS); (ii) relevant articles had to be full-text in nature; (iii) no date limitations were used; (iv) cover the topic of CPD for paramedics; (iv) discussion of CPD formats, CPD types, and CPD topics; and (v) had been published in English.
Data Collection
The articles retrieved by the search were filtered by first screening the title and abstract, then the full text. Finally, the reference lists of relevant articles were reviewed, and based on the inclusion and exclusion criteria, relevant sources cited by the articles were included. In addition to the articles reviewed, a narrative literature review was conducted to gain insight into approaches to CPD and how CPD is conducted across different contexts, using regulatory documents.
Analysis
This study employed reflexive thematic analysis as outlined by Braun and Clarke (2024), a theoretically flexible approach that emphasises researcher reflexivity and interpretive depth. This method enabled us to construct themes that reflect nuanced patterns of meaning in participants’ experiences of CPD in EMC. The EMC CPD Accreditors Annual Reports for 2017–2020 were obtained from the HPCSA and provided the details of CPD activities presented in the nine provinces of the country during the review period. Quantitative data from these reports were captured with IBM SPSS, version 27, and descriptive statistics – percentages and frequencies – were calculated.
Ethical Considerations
Approval to conduct this study was obtained from the Health Sciences Research Ethics Committee (HSREC) of the University of the Free State in Bloemfontein, South Africa (reference number UFS-HSD2020/1658/2710).
Reflexivity
The authors acknowledge their positionality as health professions educators and CPD committee members, which shaped the interpretive lens of this study. This insider perspective foregrounded issues of equity and adult-learning relevance, while maintaining reflexive awareness to avoid overemphasising regulatory viewpoints. Themes were developed through iterative coding and team dialogue to ensure transparency and interpretive depth.
Results
This section presents the results of the narrative analysis of EMC and other healthcare professions’ CPD literature, followed by an evaluation of CPD activities offered from 2017 to 2020, as outlined in the HPCSA’s EMC Annual CPD Accreditor Reports.
Regulation of CPD
Regulators in the United Kingdom, Australia, and Qatar are responsible for guiding their healthcare professionals in CPD (Health and Care Professions Council, 2017; Paramedicine Board of Australia, 2018; Qatar Council for Healthcare Practitioners, 2016). The regulations in these countries are often flexible, especially in countries where recurring medical certification is established (Lincoln & Guba, 1985). It is challenging to compare CPD systems across countries due to differences in processes and the entities responsible for service provision and accreditation. However, regulators seem to be moving toward credit-bearing relicensing and the use of portfolios for self-recorded CPD activities. Healthcare personnel are required to submit CPD portfolios when audited by a regulator. However, little is known about how the CPD portfolios are uploaded to the regulator (Health and Care Professions Council, 2017; Paramedicine Board of Australia, 2018; Qatar Council for Healthcare Practitioners, 2016). Internationally, it is standard practice for regulators to place the responsibility for CPD on individual healthcare personnel.
In South Africa, the HPCSA CPD committee, which comprises representatives from various professional boards, is responsible for developing and monitoring CPD policies (HPCSA, 2017a). These policies outline the requirements for prehospital personnel to participate in CPD activities such as workshops, formally arranged hospital meetings or updates, organised teaching and learning ward rounds, mentoring and/or supervision, peer supervision, breakfast meetings or presentations, case study discussions, conferences, symposia, morbidity and mortality meetings, refresher courses, short courses without measurable outcomes, or international conferences (HPCSA, 2017a). CPD activities can be presented through lectures, in seminar breakaway rooms, using computers, via the internet, email, data, and overhead projectors (HPCSA, 2017c).
HPCSA CEUs required per EMC registration category (HPCSA, 2017a)
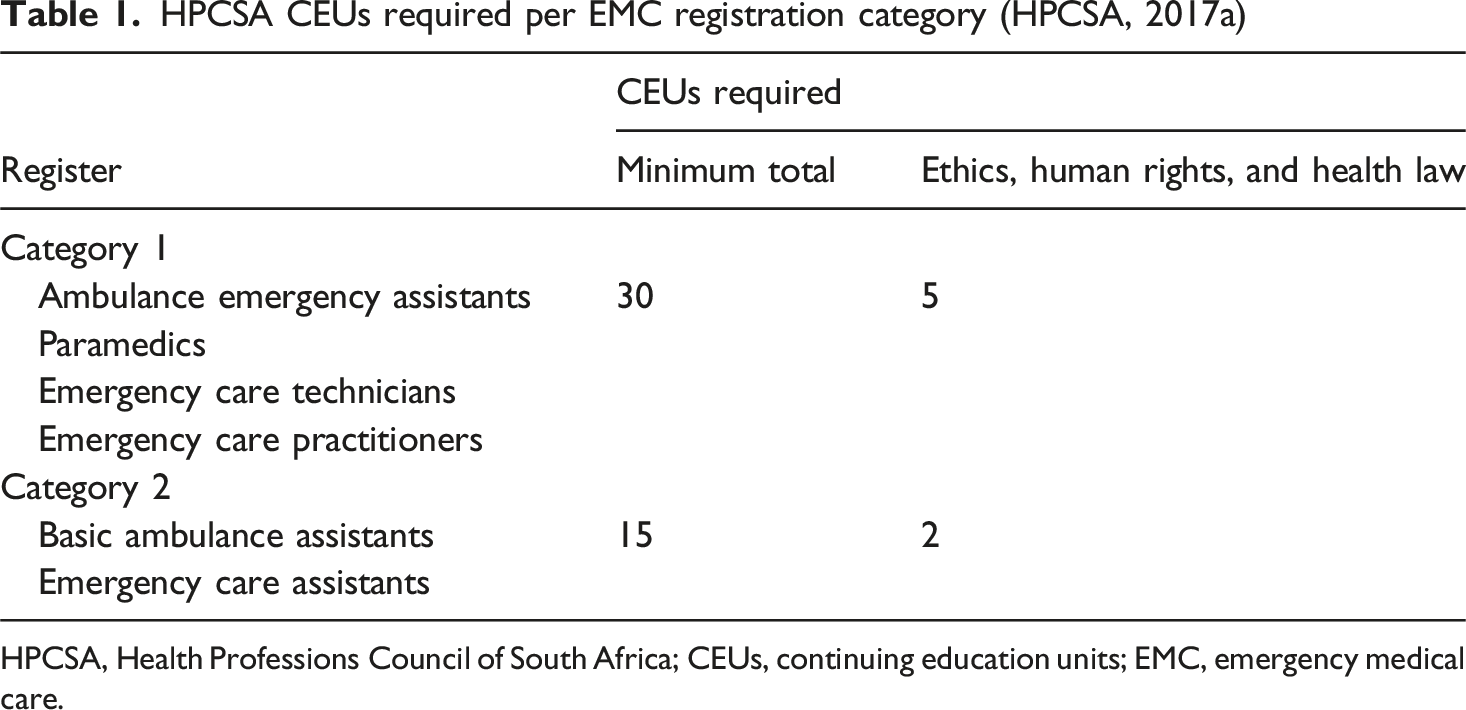
HPCSA, Health Professions Council of South Africa; CEUs, continuing education units; EMC, emergency medical care.
Modes of CPD Delivery and Their Impact on Practice
Continuous professional development includes a variety of educational activities aimed at maintaining, developing, and enhancing knowledge, skills, and professionalism to provide safe and effective clinical services (Alsaleem et al., 2020; WFME, 2015). Clinical experience over time does not necessarily develop higher-level skills, professionalism, or knowledge (Bower et al., 2010); therefore, deliberate lifelong learning remains an essential component of developing clinical knowledge and professionalism among healthcare personnel (Martin, 2006).
Several types of activities are used to implement CPD and make it more dynamic, adaptable, and outcome-oriented (Martin, 2006). CPD incorporates various educational modes to meet learners’ needs, including live, face-to-face conferences, internet streaming, flipped classrooms, external courses, scientific journal clubs, workshops, seminars, symposia, and simulation-based medical education (Filipe et al., 2014). Assuming these learning opportunities are accessible, healthcare personnel should take advantage of them for CPD (Filipe et al., 2014).
Findings revealed that didactic (lectures and presentations) and interactive sessions (discussion groups, hands-on training, problem-solving, interactive workshops) can change professional practice (Filipe et al., 2017). High-quality learning environments can be a motivating factor for practitioners to attend CPD activities (Cervero et al., 2017). According to Martin (2006), any activity that involves an outcome-based approach to learning and in which the practitioner has reflected on practice and identified suitable activities to encourage development can be defined as CPD. CPD is a universal term for many learning activities that incorporate both formal and informal methods of instruction in the health profession.
While formal approaches to education, such as courses and workshops, have historically been preferred, transforming healthcare personnel’s behaviour and/or improving patient outcomes requires a combination of formal and informal methods (Accreditation Council for Continuing Medical Education [ACCME], 2022). Research among Irish advanced paramedics confirmed that the concept of practical-type learning was a preferred approach and an effective way to ensure skills are retained (Knox et al., 2013). This differs from other professions, such as medicine, which favour journal reading, conferences, and lectures (Schostak et al., 2010). According to Howlett (2019), skills proficiency must be maintained through planned, regular CPD.
Other literature suggests that CPD planning should take into account how professional learning occurs, what learning needs are, and what practitioners are interested in (Kjaer et al., 2014; Knox et al., 2013). Adult learning, like adult development, is a personal process (Allen, 2007). Adults learn in a variety of ways. They learn best when their learning is relevant to their practice, problem-oriented, provides a plethora of knowledge, they are actively engaged, have opportunities to communicate with their peers, and can apply what they have learned (Knowles et al., 2015).
Allen (2007) explained that behaviourist, cognitive, social, and constructivist learning methods are some of the ways adults learn. Behaviourism focuses on conditioning behaviour. An observation associated with demonstration and participation in simulation may improve clinical behaviour (Ertmer & Newby, 2013). Cognitive learning is an active style of learning that entails combining new information with existing knowledge, interpreting the data, and reorganising it into new insights or knowledge. Constructivism links learning to experience and is interactive and student-centred (Ertmer & Newby, 2013). Social learning theory emphasises interactions among social settings, individuals, and behaviour, and is a way for healthcare personnel to obtain information and develop competence by observing or receiving training from others (Hwang et al., 2022). All of these approaches apply to and are used in ECP CPD, depending on the outcomes that a CPD activity aims to achieve.
Quality Assurance
Continuous professional development is considered essential to ensuring high-quality healthcare. Due to public expectations of the medical profession and evolving health needs, the relevance of CPD is gaining importance (Baumgartner et al., 2020). The literature found that when planning CPD activities, quality assurance should be aligned, as both have a significant impact on the quality of care and patient safety (Agha, 2022). Quality assurance must be developed and monitored regularly. Examples of quality assurance are monitoring the quality of the lecture, the CPD facilitator, and the learning environment. Maintaining high-quality standards extends beyond merely tracking the number of CPD activities (Van Vuuren & Nel, 2013). The responsibility for quality assurance can lie at various levels, including with accreditation bodies, which can ensure that procedures, formats, topic relevance, outcomes and/or competencies, assessments, and learning environments are of high quality (WFME, 2015). This approach could reduce regulatory burden and provide an additional layer of control.
CPD Facilitation
Continuous professional development ought to be considered part of the medical education continuum, and the medical facilitator should be involved in the development of CPD, teaching methods, and outcomes evaluation (Filipe et al., 2017; Mack et al., 2016). According to research findings (Mack et al., 2016), CPD facilitators range from full-time university employees to voluntary healthcare professionals. CPD facilitators should have formal qualifications in teaching, assessment, communication and planning. Although there are tools for evaluating educators at medical schools, no formal tools for evaluating CPD facilitators were reported (Mack et al., 2016). Teaching styles should involve relevant learning techniques and behaviours. Curriculum design, attention to learning styles, and the development of academic expertise are ways to ensure effective learning (Dash et al., 2020).
According to Grasha’s model (Grasha, 1994), five teaching styles can be used by CPD facilitators: (i) expert: the educator is the expert and knowledgeable about the topic; (ii) formal authority: the educator stresses acceptable and stringent rules in guiding students; (iii) demonstrator: the educator acts as a role model and motivates students to employ one approach process that is probably effective in the educator’s perspective; (iv) facilitator: the educator leads and directs students by asking questions and exploring possibilities; and (v) delegator: the educator expects students to work independently – this teaching style is more blended to enhance learning. However, according to Dash et al. (2020), there is no ‘best method’ of teaching in medicine.
CPD Content
Kjaer et al. (2014) provided evidence that healthcare personnel’s primary motive for choosing particular activities was their interest in the content presented. Research emphasised the relevance of context-based learning, meaning that the content format and the type of CPD activities must reflect the daily work of healthcare personnel (Baumgartner et al., 2020; Kjaer et al., 2014).
However, the documented experience is that the topics were often impractical and obsolete, and did not include interprofessional education to develop interprofessional communication and teamwork (Zereshkian et al., 2021). One study found that the topics were selected by the organisations hosting CPD events, rather than by service providers responsible for planning, designing, and developing the education (Sherman & Chappell, 2018). This practice presented significant constraints regarding identifying appropriate topics for CPD activities. In the UK, Australia, and Qatar, commercial industries have an interest in the design and presentation of CPD activities (Health and Care Professions Council, 2017; Paramedicine Board of Australia, 2018; Qatar Council for Healthcare Practitioners, 2016), while in other countries, industries with commercial interests are excluded from the educational design process of CPD due to ethical concerns. Globally, few CPD activities are interprofessional, limiting their potential to enhance collaborative practice among healthcare personnel. Nonetheless, interprofessional CPD is gaining increasing support (Sherman & Chappell, 2018). The findings underscore that CPD activities often prioritise CEU accumulation over meaningful learning. This raises concerns about CPD genuinely improving practice, or merely fulfilling regulatory requirements. Practitioners’ limited involvement in topic selection further undermines contextual relevance.
Systemic and Practitioner-Level Barriers to CPD Engagement
The literature review identified many reasons for healthcare personnel failing to attend CPD activities, the most common being lack of time, fatigue because of having to work shifts or related to staffing shortages, working in rural areas with poor infrastructure, financial issues, lack of transport or access, fear of engaging in CPD, poor or no internet access, the level of educational activities, and unprofessional teaching styles experienced with previously attended events (Adefuye et al., 2020; Chakhava & Kandelaki, 2013; Hobbs et al., 2021). The study highlighted that presenters’ lack of postgraduate qualifications, dissatisfaction with CPD activities, and the learning environment and resources were significant barriers (Hobbs et al., 2021). One study reported an overall lack of advertising and that CPD events were inaccessible (Zereshkian et al., 2021). Unless a variety of advertising methods are used, practitioners may not be aware of activities that may influence attendance and impede the acquisition of new knowledge and competencies.
CPD Assessment
Internationally, regulators require healthcare personnel to maintain a CPD portfolio of evidence (Health and Care Professions Council, 2017; Paramedicine Board of Australia, 2018; Qatar Council for Healthcare Practitioners, 2016). In Qatar, healthcare personnel are required to upload records of their CPD activities through an e-portfolio platform every 2 years (Qatar Council for Healthcare Practitioners, 2016). Australian and UK regulators require healthcare personnel to keep their portfolios in hard copy or electronically (Health and Care Professions Council, 2017; Paramedicine Board of Australia, 2018).
Analysis of Statutory Body Records
Approved EMC CPD Activities Per Province (HPCSA EMC CPD Accreditors Annual Report 2017–2020) (Information Provided by the HPCSA)
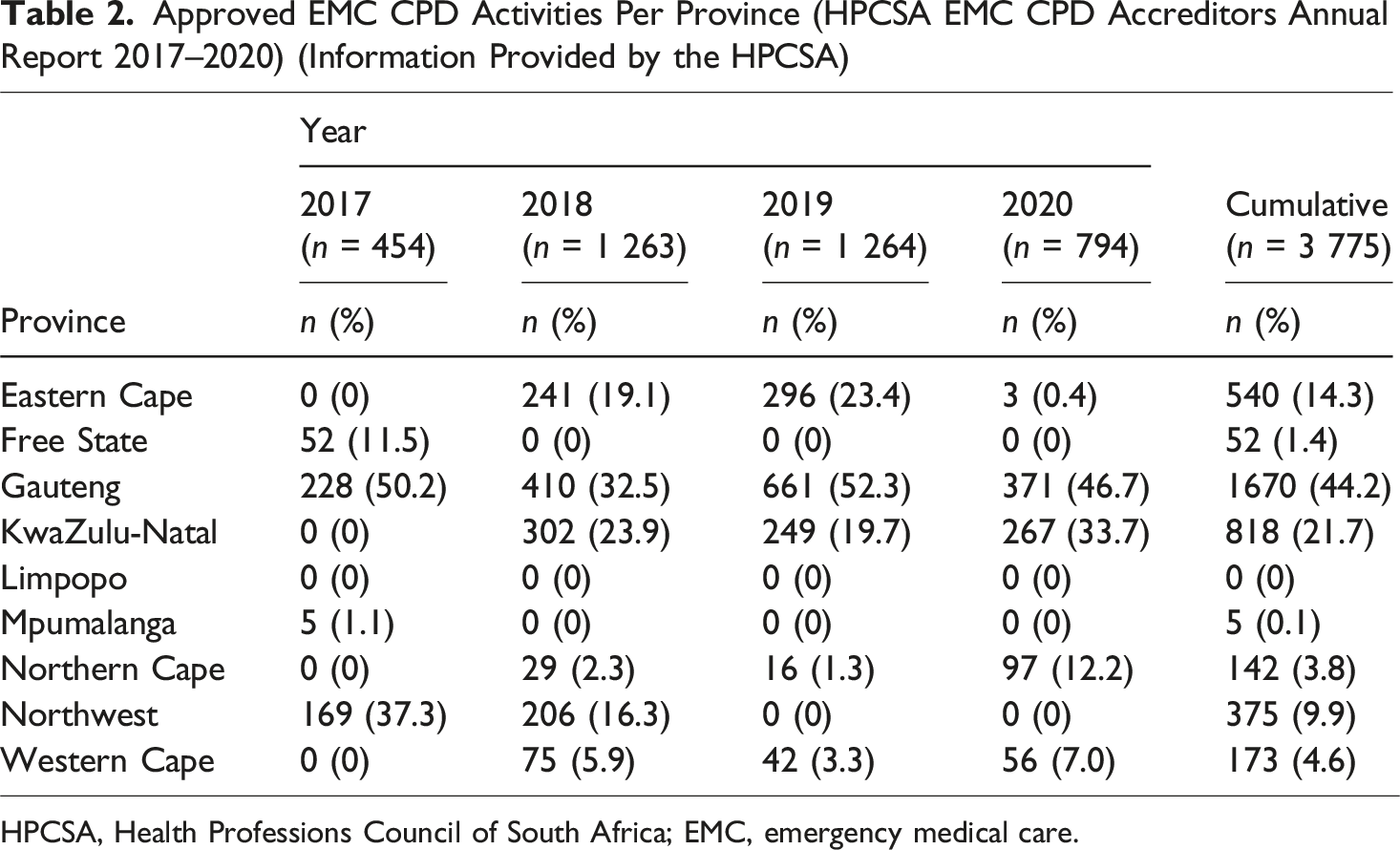
HPCSA, Health Professions Council of South Africa; EMC, emergency medical care.
Typology of EMC CPD Activities
Different types, formats, and topics of EMC CPD activities are discussed in this section.
Types of EMC CPD Activities
Type of Approved EMC CPD Activities (HPCSA EMC CPD Accreditors Annual Report 2017–2020) (Information Provided by the HPCSA)
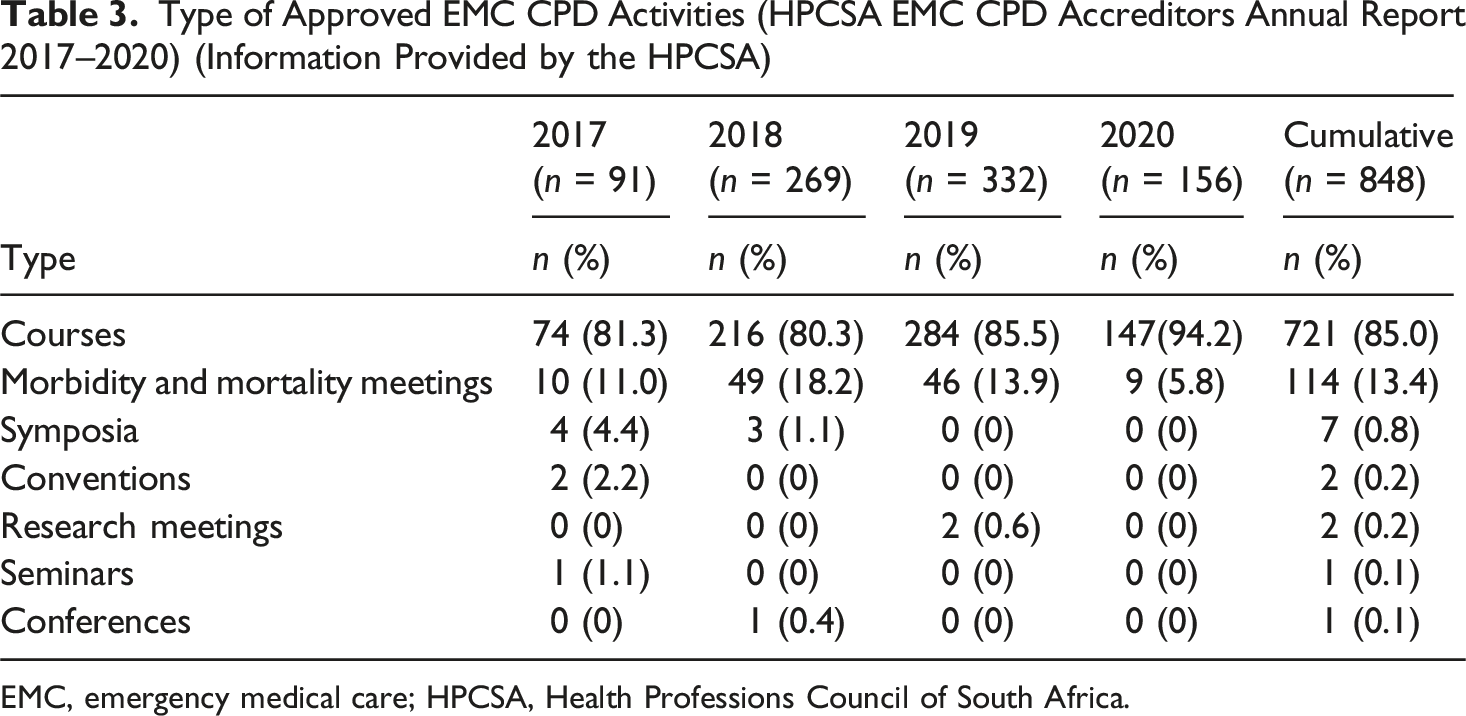
EMC, emergency medical care; HPCSA, Health Professions Council of South Africa.
Format of EMC CPD Activities
Format of Approved EMC CPD Activities (HPCSA EMC CPD Accreditors Annual Report 2017–2020) (Information Provided by the HPCSA)
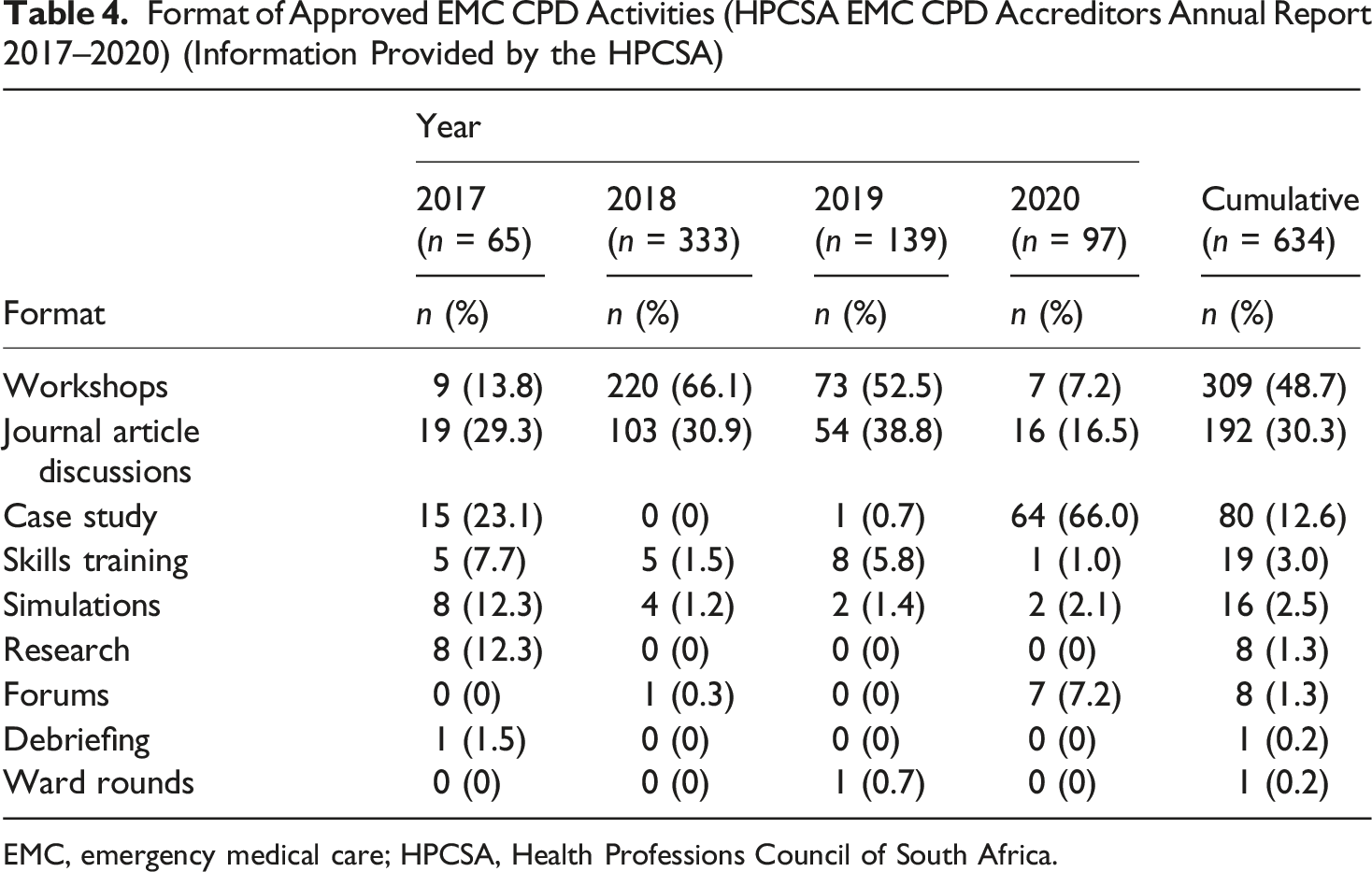
EMC, emergency medical care; HPCSA, Health Professions Council of South Africa.
Regarding the delivery method and format shown in Table 4, workshops were the most commonly presented activity between 2017 and 2019. However, in 2020, during the COVID-19 pandemic, the data showed a significant shift, with case studies recorded as the most frequent format (n = 64). This surge in formats such as case studies, which are easily adaptable to an online or virtual discussion setting, coincides with a sharp drop in face-to-face formats such as workshops (down from 73 in 2019 to only 7 in 2020), pointing to an immediate, context-driven transition to remote learning models necessitated by public health restrictions.
Topics of EMC CPD Activity
Topics of Approved EMC CPD Activities (HPCSA EMC CPD Accreditors Annual Report 2017–2020) (Information Provided by the HPCSA)
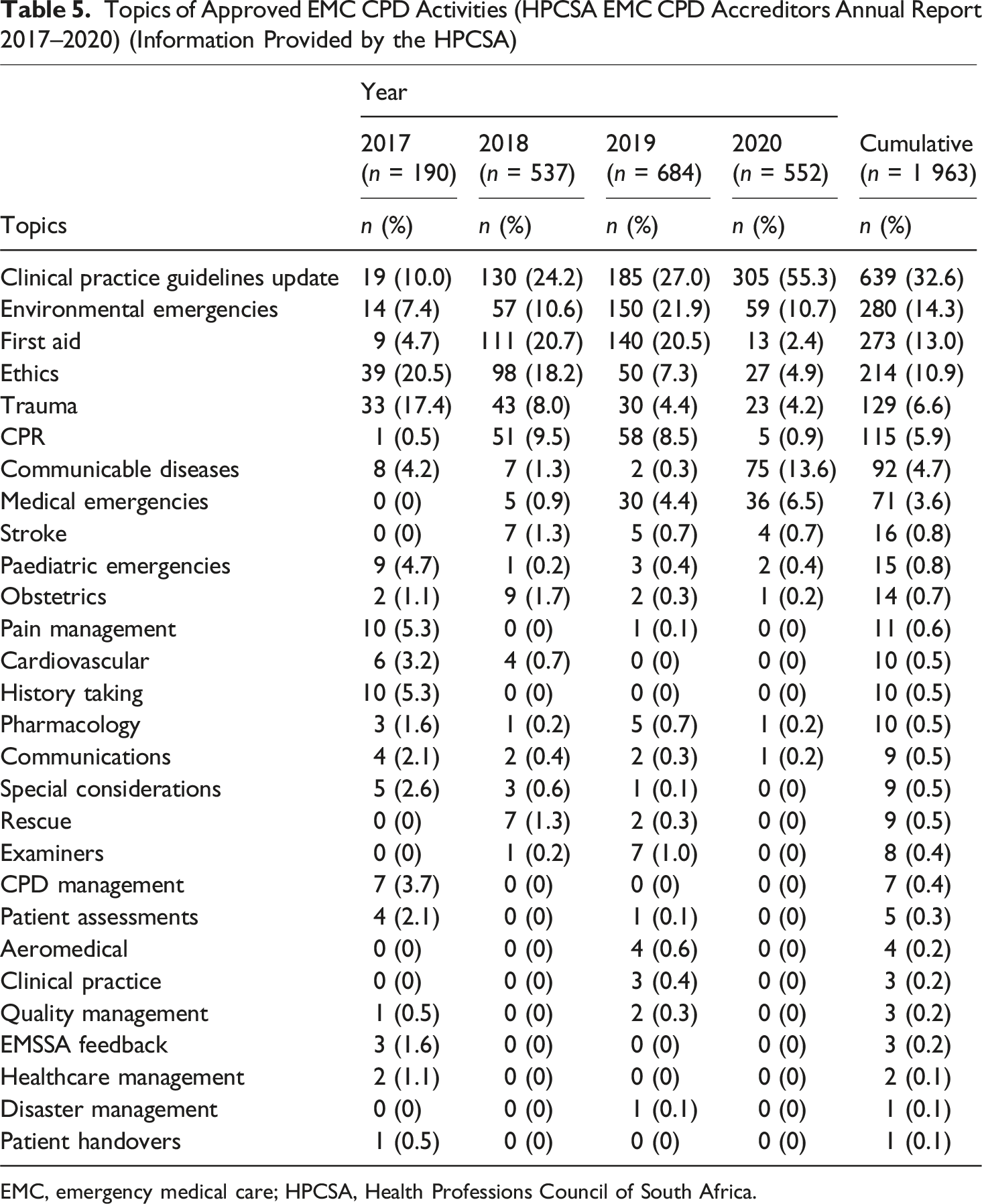
EMC, emergency medical care; HPCSA, Health Professions Council of South Africa.
The predominance of technical updates supports a recurring theme across the data, namely CPD as a mechanism for maintaining clinical currency rather than fostering reflective practice or broader professional growth. This observation aligned with the WFME’s (2015) concern that CEU-based systems may incentivise attendance over meaningful engagement. To enhance the relevance and educational value of CPD, planning processes should incorporate practitioner input and reflect the complexity of real-world emergency care. This includes addressing ethical reasoning, communication, and collaborative competencies, areas that remain underrepresented but are essential to effective, contextually responsive practice.
Discussion
This study moved beyond descriptive mapping of CPD practices by critically engaging adult education theory to interpret systemic inequities and compliance-driven cultures in EMC. The literature review established that statutory bodies, in South Africa and abroad, govern and regulate CPD compliance for healthcare personnel registered with them. Subsequently, the competence and knowledge of healthcare personnel are ensured, and they are eligible for relicensing and can practice lawfully. Generally, CPD hours are recorded, with several countries using an hour-based credit system (Health and Care Professions Council, 2017; Paramedicine Board of Australia, 2018; Qatar Council for Healthcare Practitioners, 2016).
In terms of complying with the requirements of the credit system over a 2-year cycle, the literature does not discuss knowledge gained, but it suggests that attendance or completion of CPD activities might be considered simply another ‘tick box’ to meet the minimum compliance requirements of regulators (Kjaer et al., 2014; Macdougall et al., 2017). CPD should be self-directed and patient-centred to encourage prehospital professionals to be more enthusiastic about acquiring new knowledge and mastering new skills, rather than merely ticking the box to meet the minimum requirements (Dowds & French, 2008; Filipe et al., 2017).
Over the past years, ECPs in developed countries have spent considerable time participating in traditional CPD activities, such as conferences, seminars, symposia, and workshops (Macdougall et al., 2017), similar to South African ECPs. It is worth noting that the literature represents different opinions on the best way to provide CPD and how learning occurs (Macdougall et al., 2017). Given the variety of methodologies used to ensure CPD, CPD activities can positively impact healthcare personnel’s performance and patient outcomes when delivered in an interactive learning environment and through an outcome-based approach.
However, it should be noted that shortcomings occurred despite EMC CPD Accreditors’ Annual Reports showing that EMC CPD activities have taken place in South Africa. It was not recorded (i) who the target audience was; (ii) which educational methods were used; (iii) how many prehospital personnel had attended the EMC CPD activities; (iv) on what level EMC CPD activities were presented; (v) in what learning environment the EMC CPD activities were conducted; and, specifically, (vi) the presenters’ specialities concerning the EMC CPD presentations.
According to the WFME, CPD should address the content of sciences, evidence-based medicine, and practice experience (WFME, 2015). This highlights the importance of quality assurance for CPD activities, regulators, and EMC CPD accreditors to ensure that these activities align with healthcare personnel’s needs. Quality CPD entails more than only improving evidence-based patient care; it also includes professional development (Baumgartner et al., 2020).
One of our main research findings was that some provinces in South Africa reported either no EMC CPD activities or inconsistent EMC CPD activities. The fact that the majority of EMC CPD activities between 2017 and 2020 were provided in more affluent areas, and some provinces reported no activities, aligned with barriers to EMC CPD activities reported in comparable research, such as a lack of available resources and infrastructure, working in rural areas, and the quality of facilitation (Adefuye et al., 2020). Factors that prevent healthcare personnel from participating in CPD activities can inform the design and planning of future CPD programmes (Adefuye et al., 2020).
This study’s data showed that the most common format for EMC CPD was workshops, and the least common were skills training, simulations, and ward rounds analysed. This is contrary to the findings of other studies, which reported that practical types of learning were the preferred method of maintaining competence (Wallace & May, 2016). The literature indicates that certain activities may not be offered due to resource, infrastructure, and facilitator limitations, as well as financial constraints.
Several topics were covered in CPD activities in South Africa between 2017 and 2020, mainly updates to clinical practice guidelines, which relate to the capabilities and medications adopted by the regulator. In addition to updates to clinical practice guidelines, there was no evidence of how EMC selected its CPD topics, which raises questions about their value and relevance.
The implications of these findings differ across stakeholder groups. For adult educators, the study highlights the need to embed learner-centred and problem-oriented approaches into CPD design, ensuring relevance to practitioners’ daily work. For CPD designers, the results emphasise integrating adult-learning theory into delivery modes and balancing formal and informal learning opportunities. For regulators, the findings underscore the importance of moving beyond compliance metrics toward frameworks that promote equity, contextual relevance, and meaningful lifelong learning. Together, these differentiated implications provide a foundation for reconceptualising CPD in EMC as a lifelong, learner-centred professional development system rather than a compliance-driven exercise.
Taken together, these findings suggest that CPD in EMC requires reconceptualisation not only as a regulatory mechanism but as an adult-learning system. A practice-oriented framework is therefore proposed to guide equitable, learner-centred CPD.
Recommendations
Implementing policies and guidelines should improve understanding and monitoring of CPD and reduce the complexity of CPD processes. Recordkeeping should involve a user-friendly online system. Various contextually relevant EMC CPD formats, types, and topics should be represented, complement each other, and enhance the learning process. Effective teaching and learning methods that incorporate adult-learning theory, taking into account how learning occurs and the time and professional responsibilities involved, should be employed. Infrastructure should be accessible to ensure knowledge acquisition, attitude and competency development, and practical training.
Study Limitations
Due to limited literature on prehospital EMC CPD, related CPD literature reviews for other healthcare professions were included in the analysis. The study was subject to the biases inherent in narrative reviews. Nevertheless, we attempted to mitigate this bias by including information on the databases searched, the authors, journals, years, titles, aims, and findings of the studies, as well as the screening process used. Further research should incorporate the needs of healthcare personnel in future ECP CPD offerings.
Conclusion
This study highlights systemic inequities and compliance-driven practices in EMC CPD. Interpreted through adult education theory, including andragogy, constructivism, and social learning, these findings underscore the need to reconceptualise CPD not merely as a regulatory requirement but as a learner-centred system of lifelong professional growth. A practice-oriented framework is proposed, comprising practitioner-led topic selection, blended delivery modes, interprofessional integration, and consistent quality assurance. For educators, this framework embeds learner-centred approaches; for CPD designers, it integrates adult-learning principles into delivery; and for regulators, it shifts the focus from CEU accumulation to equity and meaningful engagement. Future research should explore EMC practitioners’ perceptions and needs regarding CPD formats, topics, and delivery, and conduct longitudinal studies to assess whether learner-centred models improve professional growth and collaborative practice. By reconceptualising CPD as an equity-driven, learner-centred system, South Africa can help shape global standards for lifelong professional development.
Footnotes
Acknowledgements
We thank the HPCSA for enabling access to reports of EMC CPD activities in South Africa; and Dr. Daleen Struwig, medical writer/editor, Faculty of Health Sciences, University of the Free State, for technical and editorial preparation of the article.
Ethical Considerations
Approval to conduct this study was obtained from the Health Sciences Research Ethics Committee of the University of the Free State (reference number UFS-HSD2020/1658/2710).
Author Contributions
BPS conceptualised the study and collated and analysed the data. RB and NN guided the study conceptualisation and provided ethics oversight, and all authors contributed to drafting the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health and Welfare Sector Educational and Training Authority (HWSETA) of South Africa.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available from the corresponding author on reasonable request.