
Abstract
This article examines the ethical validity of using viability as the cutoff point for abortion in the Netherlands, in view of potential changes to the Dutch perinatal care guideline. According to the Dutch Penal Code, abortion is permitted until viability: the point at which a fetus can survive outside the womb with technological assistance. Since the law was enacted in 1984, viability has been set at 24 weeks gestational age. Currently, in the Netherlands, the treatment limit for extreme prematurity is also set at 24 weeks. The potential revision of the guideline could lower this threshold. Such a change could have implications for abortion in the Netherlands. We critically evaluate the use of viability within the Dutch context and offer recommendations for modifying the legal framework concerning abortion. We conclude that relying on any interpretation of viability is morally problematic for abortion regulation, as it is too indeterminate a concept to establish a threshold in a morally relevant way.
Abortion in the Netherlands: an introduction
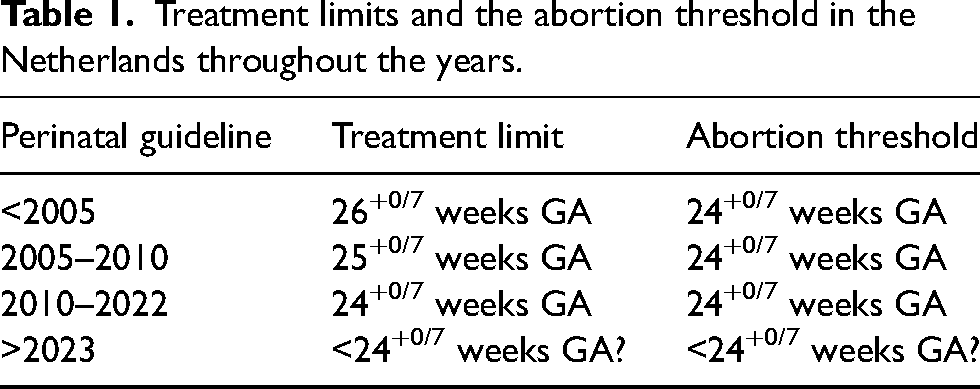
Recently, the legal regulation of abortion in the Netherlands has received renewed attention. This is largely because the Dutch treatment guideline on perinatal care in case of extremely premature birth is currently in the process of being revised. The current Dutch guideline, which dates back to 2010, restricts the provision of intensive care to infants born before 24 weeks and 0 days gestational age (24+0/7 weeks GA). 1 At present therefore, infants born below this 24-week threshold do, in general, not survive in the Netherlands. Internationally, the Netherlands is considered an outlier for its rather high treatment limit for extremely premature infants.2–5 The revision of the Dutch guideline may result in a lower threshold for providing intensive care, as this practice is already common elsewhere. The treatment limit may eventually be lowered to 23+0/7 instead of 24+0/7 weeks GA. This revision could have unforeseen repercussions for abortion because of how the legal framework is constructed in the Netherlands. The 24-week threshold is not only the threshold for providing intensive care for extremely premature infants but also the threshold for legal abortion. That is, Dutch law allows abortion until “fetal viability.” If the guideline on perinatal care for extremely premature infants is changed to apply a lower treatment threshold, the abortion threshold may also have to change to the same GA, to avoid legal and ethical inconsistency. Hence the renewed attention for Dutch abortion law and more specifically, for the use of viability as a basis for this law.
Abortion in the Netherlands is regulated by the Dutch Penal Code, the Termination of Pregnancy Decree 1984, and the Dutch Termination of Pregnancy Act 1981/84.6–8 Section 296, Subsection 1 of the Penal Code states that: “Any person who gives a woman treatment, when (s)he knows or has reasonable cause to suspect that this treatment may terminate the pregnancy, shall be liable to a term of imprisonment not exceeding four years and six months or a fine of the fourth category.” Concurrently, the law determines a nonpunishable form of termination of pregnancy in Section 296, Subsection 5: “The offence (…) shall not be punishable, if the treatment is performed by a medical doctor in a hospital or clinic in which such treatment may be performed under the Termination of Pregnancy Act.” The Explanatory Memorandum to the Act elaborates on two underlying aims of the Act: to protect unborn human life, and to provide assistance to women in an emergency situation because of an unwanted pregnancy. 9 Oddly enough, the Dutch legal framework for abortion means that the emergency situation of women is only relevant when the fetus is not viable.
Section 82a of the Penal Code states that: “Taking the life of a person or of an infant at birth or shortly afterwards shall include: the killing of a fetus which might reasonably be expected to have the potential to survive outside the pregnant person's body.” In the Explanatory Memorandum, Dutch lawmakers clarified that viability should be understood as the point in time at which a fetus can survive outside the womb, with medical technological support if necessary. 9 Yet, what it means to “survive” is not further specified; neither the duration of survival nor the quality of life after survival is discussed. This contrasts with the way viability is understood in, for example, the Japanese Motherhood Protection Act. There, viability is interpreted as “the quality or state of being able to live, grow and develop.” 10 Viability in the Netherlands, on the other hand, aligns with the interpretation of viability provided by the Supreme Court of the United States in Roe v. Wade in 1973, where viability is defined as “the interim point at which the fetus becomes (…) potentially able to live outside the womb, albeit with artificial aid.” 11
The Dutch Termination of Pregnancy Act was enacted in 1984. 8 This Act does not contain a definition of viability in terms of GA. The Dutch Ministry of Health, Welfare and Sport is responsible for concretizing the concept of viability by defining it as a certain GA. Thirty-nine years ago, the Ministry determined that the point in time at which fetal viability is reached is 24 weeks GA. The Explanatory Memorandum to the Act specifies that this GA is explicitly based on the consensus in medical science.9–12 Obviously, the medical consensus has shifted since 1984, given that babies born before 24 weeks now regularly survive.
Yet, the 24-week viability threshold has not been changed over the years. 24 weeks GA is still used as the viability (and thus the abortion) threshold in the Netherlands. 13 Yet, as we have written elsewhere, 14 the Dutch Burial and Cremation Act of 1991 does acknowledge the possibility of viability below 24 weeks GA. The Act defines stillbirth as a fetus born at a gestational age of at least 24 weeks or earlier if it survives for more than 24 hours after birth. 15
In principle, terminations of pregnancy later than 24 weeks are not possible in the Netherlands, although there is room for exceptions. Requests for the termination of pregnancy beyond 24 weeks are evaluated by the Ministerial Regulations of the Assessment Committee for Late Terminations of Pregnancy and Termination of Life in Neonates. 16 This regulation makes it possible to terminate pregnancies later than 24 weeks GA, on the basis of fetal abnormalities. The Regulation is applicable only when one of the following categories applies: (1) when the fetus is expected to die immediately after birth, and therefore considered not viable, and (2) when the fetus can be considered viable but has a condition which would lead to “serious and irreparable functional disorders.” 6 Around 5–10 cases of late termination of pregnancy are reported each year.17–19 Late Terminations of Pregnancy in the Netherlands are punishable by law unless one of the two categories applies, and a number of “due care criteria” are met. Whether this was the case is retrospectively assessed by the Assessment Committee.
The entire legal framework for termination of pregnancy in the Netherlands (Penal Code, Termination of Pregnancy Act, Termination of Pregnancy Decree, Regulation Late Termination of Pregnancy) is centered around the concept of viability. More specifically, around the viability limit of 24 weeks GA. Because of the current revision of the guideline on perinatal care for extreme prematurity, the entwinement of the regulations on abortion and prematurity in the Netherlands becomes very clear for the first time in the history of legal abortion (see Table 1).
Treatment limits and the abortion threshold in the Netherlands throughout the years.
In this article, we examine the ethical legitimacy of fetal viability as the threshold for abortion in the Netherlands. First, we discuss the multi-interpretable concept of viability. Then, we investigate how viability has been interpreted and applied in the Netherlands and how it is a pivotal concept for the provision of care for infants born extremely prematurely as well as for the regulation of abortion. Third, we show that for abortion regulation it is morally problematic to rely on any interpretation of viability, because it is too indeterminate a concept to be of use to establish an abortion threshold in a morally relevant way. Lastly, we provide recommendations for changing the Dutch legal framework for abortion.
The concept of fetal viability
The concept of fetal viability is complex and can be interpreted in many ways. Di Stefano et al. provide a helpful overview of different ways in which viability can be understood. 20 The authors differentiate between absolute viability (the GA at which the youngest extremely premature infant has ever survived), median viability (the GA at which around 50% of the infants born extremely prematurely survive with medical intervention, with or without disabilities), median intact viability (the GA at which around 50% of the infants born extremely prematurely survive with medical intervention, without disabilities), and natural viability (the GA at which around 50% of the infants survive without medical intervention, with or without disabilities). The variables between these interpretations are the number of infants that survive when born at X weeks GA, the use of medical technological support at birth, and the account of eventual disabilities. In all the above interpretations, viability is a “statistical property”: not every fetus will survive when born at the so-called limit of viability.
Except for natural viability, viability in these interpretations depends on advances in perinatal medicine, insights into fetal development, and pharmacological innovation. These are contextual variables. Globally, there are differences in the availability of resources, infrastructure, and knowledge. We will therefore add a new level of interpretational difference: viability can be understood either as “actual viability” or “viability in principle.”
Actual viability is the GA at which a country offers neonatal intensive care to extremely premature infants. Below this threshold, offering neonatal intensive care is considered medically futile, or simply not feasible, and therefore morally problematic. Actual viability depends upon (a) the national availability of resources, infrastructure, and knowledge and (b) treatment guidelines for perinatal care at the limit of viability. Of course, (b) also depends upon (a). That is, guidelines are dependent upon the available resources; if a country does not have the resources to provide intensive care, the national guideline will presumably not advise to do so. Because (a) and (b) differ between countries, actual viability also differs between countries. For example, actual median viability is around 22 weeks GA in Sweden and Japan, and around 26 weeks GA in Nigeria.2,21–23 The limit of viability is typically lower in high-income countries than in low-income countries. 24 Besides resources, treatment guidelines can also be influenced by societal and cultural values. In the Netherlands, for example, values such as independence and quality of life may explain the “higher” treatment limit for extreme prematurity. 25
Viability in principle (as opposed to actual viability) is independent of (a) and (b). In Zaitchik's words, what we call viability in principle does not rely on the “medical technology actually available to the particular fetus in question [but the] medical technology in principle available, perhaps only somewhere else in the world and only to the wealthy.” 26 Viability in principle takes no notice of the “deliverability” of the fetus. 26
For a schematic representation of the different interpretations of viability, see Figure 1.
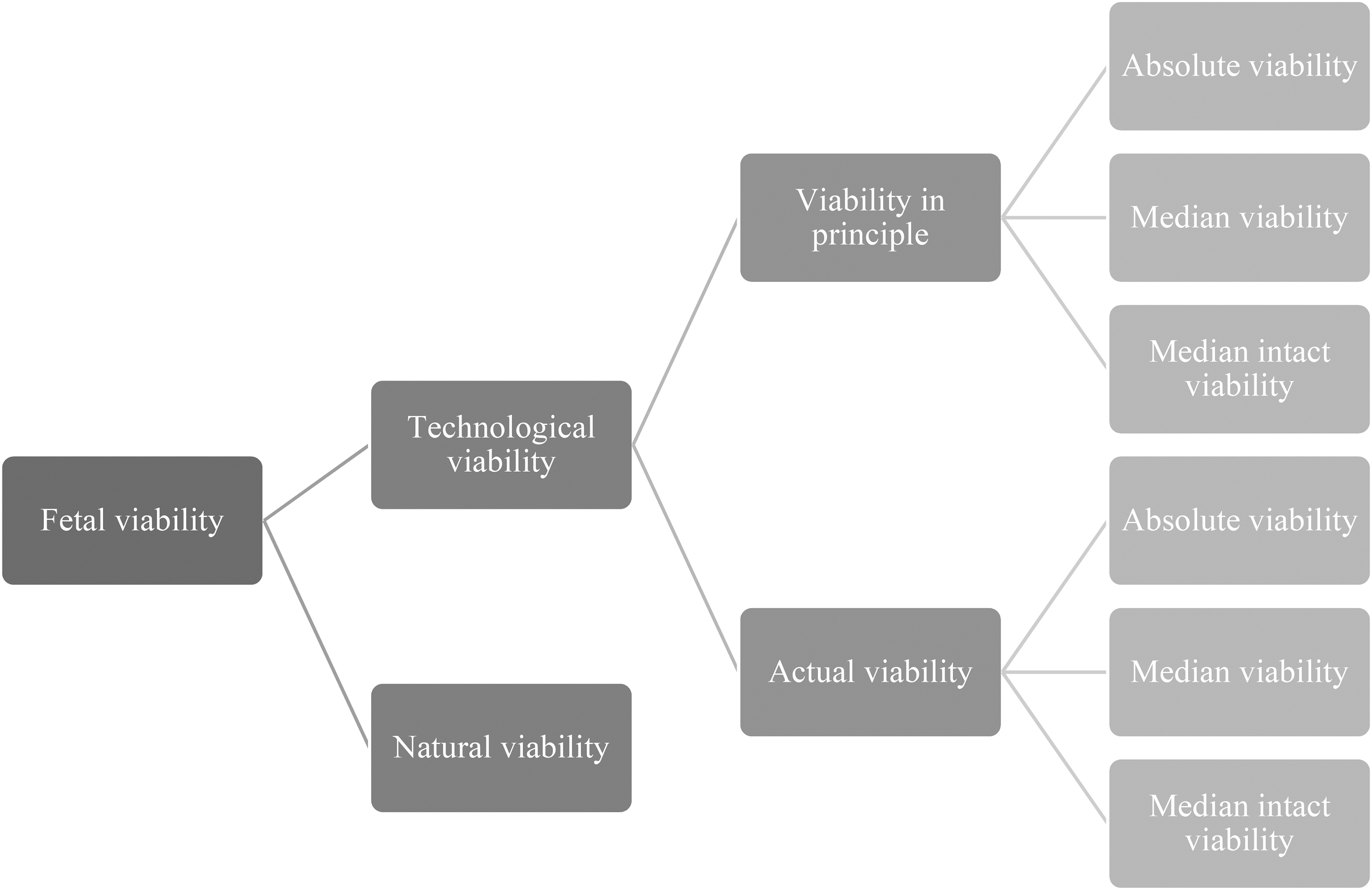
Interpretations of fetal viability.
Viability in the Netherlands
In the Netherlands, viability has been an important concept for extreme prematurity as well as abortion, although from contrasting perspectives. For the case of extreme prematurity, it refers to the point at which it is considered medically meaningful and ethically desirable to offer intensive care. Viability functions as a necessary but not sufficient condition for offering intensive care treatment. That is, if a fetus is not deemed viable, it is medically futile to offer intensive care treatment. However, if a fetus is deemed viable, it is not necessarily medically meaningful to offer intensive care; the possibility of survival is not the only consideration for deciding to offer intensive care treatment. According to research involving parents and healthcare professionals with experience of extremely preterm birth, factors such as the infant's (long-term) health outcomes and the quality of life for the family are also highly important for periviability decision-making. 27 In a recent study by Edmonds and colleagues, parents shared their perspectives on what was crucial when deciding on the management of periviable birth. Important considerations mentioned included “the best interest of their infant,” “having a healthy baby,” or “avoiding pain and suffering.” 28
For abortion, viability is used as the legal cut-off point for legal prosecution in case of pregnancy termination. In the past, however, viability has always been defined as a different GA for both neonatal care and abortion. In the Dutch history of abortion, the meaning of the 24-week GA cut-off in relation to the definition of viability has evolved over time. In 1984, when the Termination of Pregnancy Act was enacted, no infants born at 24 weeks GA survived in the Netherlands. At that time, the Dutch Ministry of Health, Welfare and Sport seemed to understand viability as viability in principle: at that moment, somewhere in the world, infants born at 24 weeks GA were surviving outside the pregnant person's womb. At present, however, around half of the extremely premature infants born at 24 weeks GA survive in the Netherlands, with medical technological support, with or without disabilities. 21 In the Netherlands, the meaning of viability seems to have evolved, implicitly, from absolute viability in principle in the 1980s (at that time, somewhere in the world, the youngest survivor of extreme prematurity was born around 24 weeks GA), to actual median viability in the 2020s (at present, around 50% of Dutch infants born at 24 weeks survives).
The Dutch framework for abortion, and care practice at the limit of viability are intrinsically linked. On the one hand, keeping a certain fixed interpretation of viability results in a continuous change of the corresponding GA—due to innovation in perinatal care. On the other hand, keeping a certain fixed GA for viability results in a change in the corresponding interpretation of viability (see Table 2).
Viability and interpretations of viability.
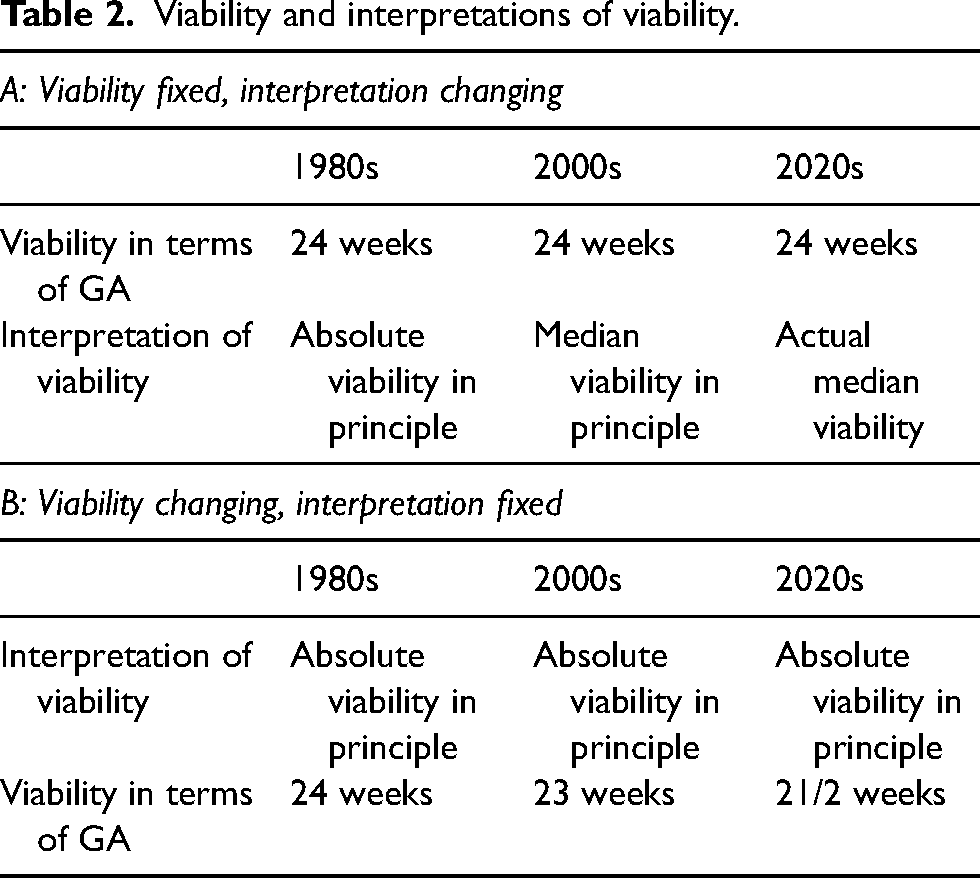
Although these shifts in meaning have caused little debate so far, a revision of the guideline on perinatal care would likely change this, because determinations of viability in cases of perinatal care and abortion would differ explicitly. Concretely, a fetus of, say, 23 weeks GA would be considered viable in one medical context (perinatal care) and not viable in another (abortion). Since viability in extreme prematurity functions as a necessary condition for offering treatment, a lower treatment limit seemingly implies a lower abortion threshold.
Viability as the criterion for (dis)allowing abortion
To understand what it means to base abortion regulation on viability, consider the following hypothetical cases of extreme prematurity and abortion. In these cases, abortion regulation is based on actual viability.
Person A and Person B are both 23 weeks pregnant. A lives in high-income country X and B lives in low-income country Y. In country X, viability is set at 24 weeks GA. In country Y, viability is set at 29 weeks GA; highly specialized care is lacking. A and B both deliver their baby at 24 weeks GA. A's baby survives. B's baby does not. If B would have been on vacation in country X at the time of labor, her baby may have survived. In this case, an extremely premature baby dies because of the lack of availability of medical technology. In the case of extreme prematurity, the availability of medical technology matters: it determines what can be done for an extremely premature infant. The availability of resources, infrastructure, and knowledge is morally relevant in case of extreme prematurity.
Consider now that country X and country Y both have actual viability as their abortion threshold. Given the available medical technology, the abortion threshold in country X is set at 24 weeks GA and in country Y it is set at 29 weeks GA. A and B both find out that they are pregnant at 24 weeks GA. They both want to terminate their pregnancy. For B this is no problem. A, however, is not allowed to have an abortion. Oddly enough, the possibility for A to have an abortion is linked to the available medical technology of country X, but the available medical technology has no relation to the possibility of terminating the pregnancy. The availability of resources, infrastructure, and knowledge is, prima facie, morally irrelevant in the case of abortion.
Given that a request for abortion is not a request for providing neonatal care, the availability of said care is a morally arbitrary criterion for (dis)allowing abortion. It does not matter whether the fetus would have received neonatal care if it was born extremely premature in deciding whether having an abortion should be allowed. In other words, basing the admissibility of abortion on actual viability (as appears to be the case in the Netherlands) is morally problematic as the availability of medical technology is irrelevant to the proper establishment of the limit to abortion. Other authors have made similar points.26,29 One author writes that “No one would want to say that by flying from Cambridge to Calcutta a woman suddenly gained the right to destroy a formerly ‘viable’ but now ‘pre-viable’ fetus, or that the fetus suddenly ceased to be a person or human, or that it suddenly lost a ‘right to life’.” 26
Now this objection might be worked around by opting for a different interpretation of viability, which is independent of the (national) availability of resources, infrastructure and knowledge, and treatment guidelines for perinatal care at the limit of viability, that is, either viability in principle or natural viability. Before we are in a position to evaluate these options, however, we need to consider why viability is deemed morally relevant for abortion in the first place.
In the literature, the main argument in favor of viability as a morally relevant cut-off point for abortion, is that it indicates the point in time at which a fetus can survive independently of the pregnant person's body. 30 That is, referring to the illustrious thought experiment of Thomson, the point at which the “detaching” of the fetus no longer equals the “killing” of it. 31 Our discussion of viability has already shown that this point in time is notoriously hard to determine. Accordingly, independent survival suffers from the same problems as viability when it comes to determining an abortion threshold: it can be understood as actual or in principle, technological or natural, etc. To be viable is to be able to survive independently and vice versa. But the problem here is that we have used one underdetermined concept to explain another underdetermined concept. No insights are gained.
So why do scholars consider independent survival morally relevant to determine abortion thresholds? Usually, because it is construed as a necessary condition or marker of personhood, or some other form of moral status from which the right to life follows. Now given the (near-)synonymity of independent survival and viability, can independent survival function as such a condition or marker?
In light of the above, an actual interpretation of independent survival is out of the question. Just like actual viability, it would be determined by the (national) availability of resources, infrastructure and knowledge, and treatment guidelines for perinatal care at the limit of viability, with all the ethical consequences detailed above. On other interpretations of viability, independent survival fares no better, but for different reasons.
Recall that every interpretation of viability is to be understood as a statistical property. It usually ranges from 21 weeks GA (absolute viability—N = 1) to 34 weeks GA (natural viability—around 50% of infants survive without medical intervention, with or without disabilities), but can logically be extended even further. For interpretations of viability that rely upon long-term survival, even birth does not equal viability, as infants sometimes do not survive (the first days after) delivery. Furthermore, because of advancements in neonatal medical technologies, it is imaginable that infants born before 21 weeks GA can one day be “viable.” Over the years, younger and younger extremely premature infants can receive intensive care at birth and survive. 32 One day, we may reach an absolute biological limit of viability. Irrespective of medical science, fetal organ growth and development will take a minimum of time. 32 However, innovative medical technological inventions might even then lower the limit of viability. An example of this is artificial amniotic sac and placenta technology often referred to as artificial womb technology. 33 In the future, this innovation might make it possible for fetuses to be independent of the pregnant person's body earlier than they currently are.
Furthermore, there is no logically compelling reason to limit concepts of viability to 50% of infants rather than, say, 60%, 75%, or even 90% of infants surviving without medical intervention, with or without disabilities. Now in view of this extensive range of interpretations, it is unclear how a concept as indeterminate as viability could serve as a marker or condition of determinate concepts like personhood, or the right to life. There is no compelling moral argument to prefer one moment in the viability range over another (although there can be legitimate pragmatic or political reasons to choose one). Viability, therefore, cannot serve as a moral basis to decide whether a fetus is (to be treated as) a person. As a result, independent survival loses its moral relevance as a cut-off point for abortion.
For extreme prematurity, the availability of neonatal care and the percentage of extremely premature survivors are morally relevant. We are in favor of relying upon technological actual viability for this field of health care. For abortion, however, contextual factors such as the availability of technology but also the personalized prognosis of viability for the fetus are not morally relevant. It does not matter whether the fetus would have received neonatal intensive care if it was born extremely premature in deciding about the permissibility of abortion. The point in time that is usually considered morally relevant for abortion is when the detaching of the fetus no longer equals the killing of the fetus, that is, the possibility of independent survival. Given the (near-)synonymity of independent survival and viability and the underdetermined nature of both concepts, independent survival cannot serve as a morally relevant criterion. If the argument does not work with viability it will also not work with independent survival.
Changing the Dutch legal framework for abortion
Scholars have put forward that viability is not an ideal abortion threshold as it is morally problematic, conceptually and or practically ambiguous, and a slippery slope toward an abortion ban.26,29,34,35,36,37 It has also been suggested that the viability threshold implies an unjustified conflation between the fetus’ interests and the pregnant person's duties. Already in 1995, Gert pointed out that the viability threshold is peculiar in relation to the pregnant person's duties: “As long as [the fetus] needs you, you are not responsible to it; when it doesn't need you anymore, you are.” 37 After viability, however, the pregnant person no longer needs to carry sole responsibility to pursue the fetal interest of surviving; technology can promote this interest as well. Yet, in more recent literature, it has been argued that inducing birth for post-viability abortions brings about another conflict, one with the pregnant person's autonomy; “(…) The process of birthing a fetus makes use of the body of the pregnant person in significant ways. (…) Just as it is sometimes morally permissible to choose to have an abortion rather than continue a pregnancy, it is sometimes morally permissible to choose to have an abortion rather than undergo an induction or cesarean.”38 Still, a viability-based abortion threshold could overall be the “least bad” option, out of all similarly “bad” options. We are convinced, however, that—especially for the Dutch situation—there are better options.
Another moral ground for abortion in the Netherlands
As explained, the Dutch legal framework for abortion aims to serve two principles: protecting unborn human life and relieving the emergency situation of the woman. These aims result in a viability-based abortion threshold; only abortions of viable fetuses are punishable by law. We have shown that a viability-based abortion threshold is morally problematic. It is beyond the scope of this article to fully develop a normative alternative framework for an abortion threshold. Yet, in what follows we will outline what are morally relevant grounds for developing such a framework, namely, the autonomy of the pregnant person to decide what happens to her body and the fetus’ interest to survive.
Whatever abortion threshold is chosen, it should weigh or balance the interests of its two stakeholders, both the fetus and the pregnant person. From the viewpoint of autonomy, the pregnant person's interest is to have the option to abort open for as long as possible. In this way, their opportunity to exercise autonomy is maximized. The fetus’ interest is to survive, and thus to be protected (we leave questions about whether there are circumstances in which it would be better for the fetus not to be born unaddressed). If we consider only the interests of the pregnant person, abortion should be permissible throughout the entire pregnancy. The same goes for the protection of the fetus. If we consider only the fetus’ interest to be protected, abortion should be banned. Assigning relative weight to these interests (respect for the autonomy of the pregnant person to decide what happens to her body and the protection of life) constitutes a relevant moral ground for abortion regulation.
It could be argued that this moral ground is, like viability, subject to interpretation. This is correct. Unlike viability, however, the weighing of both interests is morally relevant for the moral justification of an abortion threshold. That is, if we consider when it is justifiable to terminate a pregnancy and thereby terminate the life of one subject to promote autonomy, prevent harm, or promote the good of another subject, it is paramount that the stakeholders’ potential gains and harms register on a moral scale. Internationally differing interpretations might raise practical concerns but are not ethically problematic. The corresponding GA for the point of balance can be influenced by differing sociocultural values and convictions related to reproductive autonomy, personhood, and the right to life. Just as different countries have different speed limits but similar reasons for having these limits in place, we think that having different points of balance is not problematic as long as they take into account the relevant moral grounds. Deciding about the abortion threshold thus may have an empirical component. An abortion threshold that is based upon a balance between the interests of the pregnant person and the interests of the fetus has a defensible moral ground and is therefore preferable to one based on viability. a
Conclusion
In the Netherlands, viability has been an important concept for extreme prematurity as well as abortion. Yet, we have shown that viability can be interpreted in many ways. For extreme prematurity, viability should be interpreted as technological actual viability. For abortion, however, it is morally problematic to rely upon this or any other interpretation of viability. This leaves the Netherlands with the following choice of policy options in view of the proposed revision of the guideline on perinatal care for extreme prematurity. The 24-week GA abortion threshold in Dutch law was based on absolute viability. If this interpretation of viability is to be retained the Dutch abortion threshold should be lowered. If this is deemed undesirable, the Dutch could either abandon viability as a marker for personhood or opt explicitly for another interpretation of viability in the case of abortion. Another option would be to change the basis of Dutch abortion regulation entirely. A set GA could be incorporated into the Penal Code or the Termination of Pregnancy Act. Or another moral ground for abortion can be introduced: the balancing of the interests of the pregnant person and the fetus—which would be our recommendation for the Dutch practice.
Footnotes
Acknowledgments
We extend our sincere appreciation to Elizabeth Chloe Romanis and Samantha Halliday for their invaluable contributions to this article in sharing their constructive thoughts, engaging in productive discussions about the topic, and providing insightful legal perspectives. Thanks also to the anonymous reviewers of our article for their constructive feedback.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by ZonMW: On the limits of perinatal viability: ethical challenges of personalized counseling and the artificial placenta (40-00703-97-19039), and MRACE Erasmus MC.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.