
Abstract
The Health (Regulation of Termination of Pregnancy) Act 2018 was commenced on 01/01/2019 in Ireland. The Act provides for legal termination of pregnancy under defined circumstances including for any reason at < 12 weeks gestation; and where two doctors agree there is ‘a condition affecting the foetus that is likely to lead to the death of the foetus either before, or within 28 days of, birth’. As such, abortion for congenital anomaly (CA) can occur at a number of time points, depending on the adjudged severity. Infants born with CAs frequently require significant medical intervention and account for a high proportion of admissions to paediatric intensive care units (PICUs). The purpose of this paper was to evaluate the number of infants with CAs admitted to an Irish PICU in the period before and after the implementation of the Act. All PICU admissions < 1 month of age to a single Irish paediatric hospital between 2012 and 2021 were analysed. CAs were recorded, and the periods before and after the commencement of the Act compared. We found a difference in admissions involving CAs, particularly those related to congenital heart disease involving single ventricle anatomy. It is plausible that this difference was as a result of improved access to abortion services following the implementation of the Act. This article explores the legal conditions related to the abortion of a foetus with a CA in Ireland, and the possible impact of the Independent Review of the Operation of the Health (Regulation of Termination of Pregnancy) Act 2018.
Introduction
Until 2019, legal abortion in Ireland was effectively restricted to women whose lives were at serious risk should the pregnancy continue. Despite this caveat, a number of women in this situation were denied termination of preganancy in the State, a situation that ultimately played out in the tragic and indefensible death of Savita Halappanavar in 2012. 1
Thus, Irish women had to travel abroad in order to access abortion services, approximately 170,000 doing so (mostly to England) between 1980 and 2016. 2 These included women carrying foetuses diagnosed with severe, or even fatal, congenital anomalies.
Following a referendum in 2018 to remove a prohibitive article from the Constitution (Art 40.3.3), new legislation was enacted that allowed for legal termination of pregnancy under broader, although still, limited circumstances. The Health (Regulation of the Termination of Pregnancy) Act 2018 (“The Act”) allows for legal termination in four circumstances: first, where two medical practitioners certify that there is a risk to the life, or of serious harm to the health, of the pregnant woman, the foetus has not yet reached viability, and the risk can be averted by termination of the pregnancy (section 9 of the Act (s9)); second, where the above threat to life or health occurs in an emergency situation and the certification of a single doctor is sufficient (s10); third, where there is a condition affecting the foetus that is likely to lead to its death before or within 28 days of birth (s11); and, finally, for any reason prior to 12 weeks gestation (s12). 3 It is these two latter situations that are of relevance to this paper.
Data from outside of Ireland clearly indicates that rates of both perinatal mortality and children being born with significant congenital anomalies (CAs) are impacted upon by ease of access, or its converse, to abortion services. Earlier diagnosis of anomalies has become possible through advances in prenatal screening, with the incidence of abortion for congenital anomalies increasing in the UK and the US as prenatal diagnosis has become both more widely available, and more sophisticated.4,5
Children born with severe CA have significant medical needs and may require surgery and/or intensive care support in the neonatal period. 6 As such, rates of neonatal admissions to intensive care due to CA are likely to be related to the rates of children being born with severe congenital abnormalities.7,8 We sought to investigate if the number of infants being admitted to paediatric intensive care units (PICUs) with CA has changed since the 2018 Act came into effect on the 1 January 2019. While it would not be possible to definitively establish a causal link between the introduction of the Act and and any change in PICU admission characteristics, nonetheless it is plausible that the option to have an abortion carried out in Ireland in particular circumstances might impact on the number of infants born with severe congenital anomalies, and thus being admitted to PICU.
Any trends identified by this study must be interpreted within the context of the legislation.
Abortion for CA can only lawfully take place within Ireland under two circumstances. First, where there is a diagnosis made within the first eleven weeks and three days, succeeded by an abortion following the mandatory three day waiting period; and second, where two medical practitioners have certified that there is ‘a condition affecting the foetus that is likely to lead to the death of the foetus either before, or within 28 days of, birth’. As a result the impact of the legislation on the rate of live births with CA, and by extension, the rates of neonatal admissions to PICU with such conditions, will only be apparent for the most severe forms of CA, or those amenable to early diagnosis. It also must be noted that our data comes from a single centre which is the largest provider of paediatric services in the State and, amongst other tertiary services, cares for all children requiring PICU admission for significant congenital heart disease (CHD) on the island of Ireland. As a result some admissions relate to children from Northern Ireland, which is a separate legislative environment.
Finally, the data obtained in this study might also be impacted upon by several significant issues arising out of the implementation of the 2018 Act. These matters, and how they might affect access to services, are highlighted in a recent, legislatively required, review of the Act 9 and include the mandatory waiting time, geographic variability in service provision, and difficulties in clearly defining conditions that are ‘likely to lead to the death of the foetus either before, or within 28 days of, birth’. The findings of the Review, and their relevance to abortion for CA, will be discussed.
Background
Abortion, law and foetal anomaly in Ireland
Prior to the foundation of the Irish state, section 58 of the UK Offences Against the Person Act 1861 made it illegal for a woman to ‘procure a miscarriage’ under penalty of life imprisonment. Under s59 of this Act, the same penalty applied to anyone found guilty of assisting the woman in procuring a miscarriage. The fundamental ethos, and effect, of the 1861 Act was thus to criminalise abortion in Ireland, and this remained in effect following the establishment of the Irish State in 1922. In 1937, Ireland adopted a formal written Constitution (Bunreacht na hEireann), which contained no specific provisions in respect of the prohibition of abortion. Rather Article 40, under the heading personal rights stated ‘All citizens shall, as human persons, be held equal before the law’. While this protection was generally considered to include the foetus, as indicated by the obiter remarks of Walsh J. in Magee v. Attorney General, 10 concerns arose that the non-explicit nature of the Constitutional article might make the provisions of the 1861 Act vulnerable to challenge. As set out by Murray CJ in Roche v Roche (a frozen embryo case), 11 both the English case of R v Bourne, 12 and the US Supreme Court decision in Roe v Wade, 13 were perceived as potential avenues through which the prohibition of abortion might be challenged.
In 1983, a referendum of the Irish people was held and the Constitution amended to include Art 40.3.3 (generally known as the 8th amendment), which stated: The State acknowledges the right to life of the unborn and, with due regard to the equal right to life of the mother, guarantees in its laws to respect, and, as far as practicable, by its laws to defend and vindicate that right.
A key purpose of the amendment was ‘to prevent the introduction of abortion either by legislation by the Oireachtas or by judicial decision’. 14
Two further amendments to the Constitution, the 13th and 14th, were passed by referendum which allowed for distribution of information regarding abortion services abroad, and the right to travel to procure a termination outside of Ireland, these changes following several high profile cases which came before the courts.15,16 International and European institutions were extremely critical of Ireland's legal stance with regard to abortion. In the cases of Mellett v Ireland and Whelan v Ireland, the complainants were both women who were carrying foetuses diagnosed with conditions considered invariably fatal. The legal environment at the time meant their options were to carry the pregnancies to term, or to travel to obtain an abortion. In both cases, the UN Human Rights Committee found that Ms Mellett's and Ms. Whelan's rights had been violated under the terms of the UN International Covenant on Civil and Political Rights, and that they had been subjected to inhumane and cruel treatment.17,18
Preceding Mellet, the European Court on Human Rights (ECtHR) had found that Ireland had breached the Article 8 rights of one applicant of three (A, B and C v Ireland) in respect of her inability to access abortion services in Ireland.
19
C was undergoing treatment for cancer when she became pregnant and could neither establish the risks of pregnancy to her ongoing treatment, nor identify a clear legal route to obtain an abortion despite an earlier Supreme Court judgment which had ruled that termination of pregnancy was lawful in the State in circumstances where there was a serious risk to the life of the mother.
15
On foot of the findings of the ECtHR, The Protection of Life During Pregnancy Act (2013) was passed, repealing Sections 58 and 59 of the Offences against the Person Act (1861), and legislating for termination of pregnancy in circumstances where a women's life was in danger, or where there was a serious risk of suicide. It did not, however, include situations of foetal abnormality (fatal or otherwise), termination of pregnancy for this remaining illegal until 2019. As stated earlier, s11 of the Health (Regulation of the Termination of Pregnancy) Act (2018) now contains a provision relating to abortion in cases where a likely fatal condition is diagnosed: A termination of pregnancy may be carried out in accordance with this section where 2 medical practitioners, having examined the pregnant woman, are of the reasonable opinion formed in good faith that there is present a condition affecting the foetus that is likely to lead to the death of the foetus either before, or within 28 days of, birth.
However, this text has been the subject of much uncertainty, compounded by the threat of criminal prosecution of medical practitioners in cases of misdiagnosis. This has lead to the possibility of a particularly conservative approach to diagnosis, and defensive practice by relevant clinicians (see below). There is no provision in the Irish 2018 Act comparable to Section 1(1)(d) (Ground E) of the 1967 Abortion Act whereby abortion at any gestation is lawful if ‘there was a substantial risk that, if the child were born it would suffer from physical or mental abnormalities as to be seriously handicapped’.
Congenital anomalies
Congenital anomalies can result in significant levels of disability, illness and in-utero, infant or premature death in affected pregnancies. The European registry of CA, EUROCAT, amalgamates data from multiple European databases. It shows the prevalence of CA across all national registries. Included in their database was 203/10,000 births for the period between 2013 and 2019, Irish figures not deviating significantly from this mean (201/10,000 births). 20 Across Europe CA account for approximately 20% of foetal mortality and for a significant proportion of perinatal death in high income countries. 21 The WHO estimates that, worldwide, CA result in the death of 295,000 newborns per year before they reach 4 weeks of age. 22
The morbidity associated with severe CA can mean affected children may require multiple admissions to PICU. Mortality from CA as a percentage of neonatal deaths however is decreasing. While improvements in diagnosis and treatment are partially responsible, abortion following prenatal diagnosis has also contributed to this decline. 23 Termination also complicates the interpretation of data concerning the incidence of CA as sometimes stillbirths and abortions are not counted.
Methods
Following institutional Research Ethics Committee approval, all admissions to Ireland's largest PICU between mid-2012 (when an electronic healthcare record was introduced) and the end of 2021 were analysed. PICU data was extracted from the IntelliSpace for Critical Care and Anaesthesia (ICCA, Phillips) electronic healthcare records and anonymised. Data collected was limited to patient age at time of admission, and admission and discharge diagnosis as entered by relevant physician.
All patients aged < 1 month of age at time of admission were included. The admitting and discharge diagnoses were then examined to determine if there were any documented severe CA. These were coded based on primary organ system involved, the specific anomaly, secondary organ systems involved and any known genetic abnormalities. Cases of congenital heart disease were further subdivided into those with only one effective cardiac pumping chamber (single ventricle) and those with two on the basis that children with a single ventricle system have a significantly worse prognosis. 24 Infants for whom there was a definitive or presumptive diagnosis of trisomy 21 (Down syndrome) were also recorded on the basis that a diagnosis of trisomy 21 has been identified as a significant factor in decisions to terminate a pregnancy in other jurisdictions. 5
Admissions for the periods before and after the introduction of the 2018 Act were then compared. Pearsons test was used to determine if variables pre- and post- the implementation of the act were independent and a χ2 test was performed to examine if any observed differences between the two periods were significant, where significance was considered to be p < 0.05.
Results
Yearly admissions to PICU were largely comparable throughout the study period. Neonates accounted for 20% to 26% of all admissions (Table 1).
The number of paediatric intensive care units (PICUs) admissions per year.

Partial data for 2012.
Table 2 shows a year by year breakdown of anomaly subdivisions as a percentage of the total number of neonates with a congenital anomaly. The majority of neonates admitted to PICU had some form of significant congenital anomaly and this remained high throughout the time period examined.
Breakdown of proportion of neonatal admissions with anomaly, by organ system.
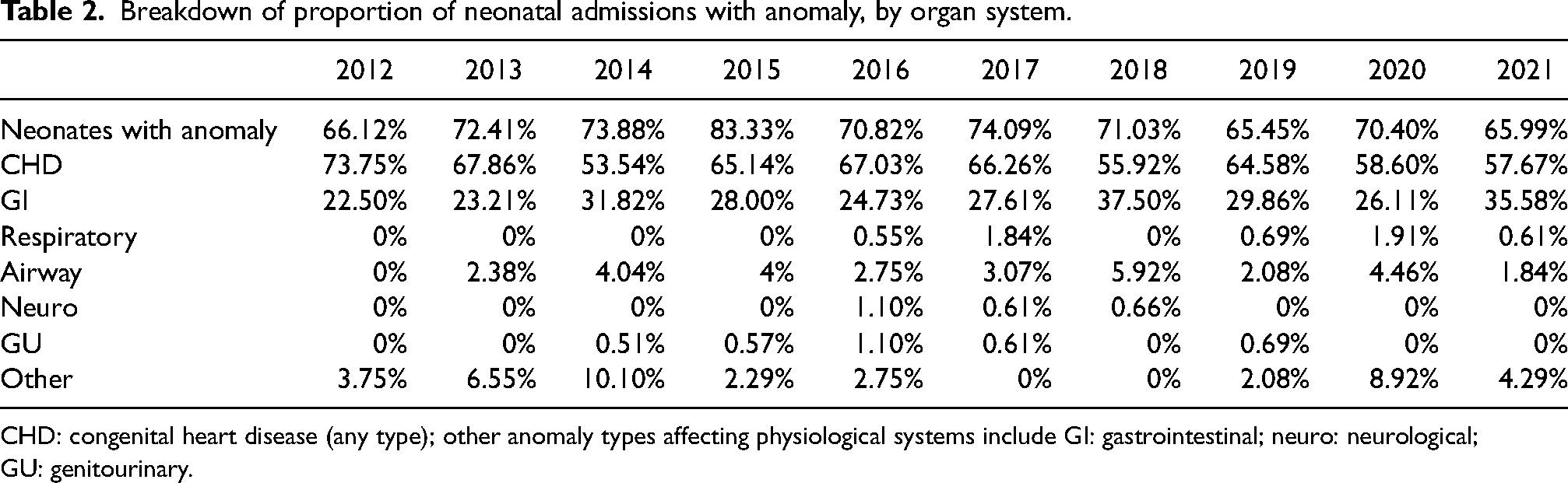
CHD: congenital heart disease (any type); other anomaly types affecting physiological systems include GI: gastrointestinal; neuro: neurological; GU: genitourinary.
Table 3 shows a comparison of the period before implementation of the 2018 Act and after implementation.
Comparison of pre/post introduction of health (termination of pregnancy) Act 2018.
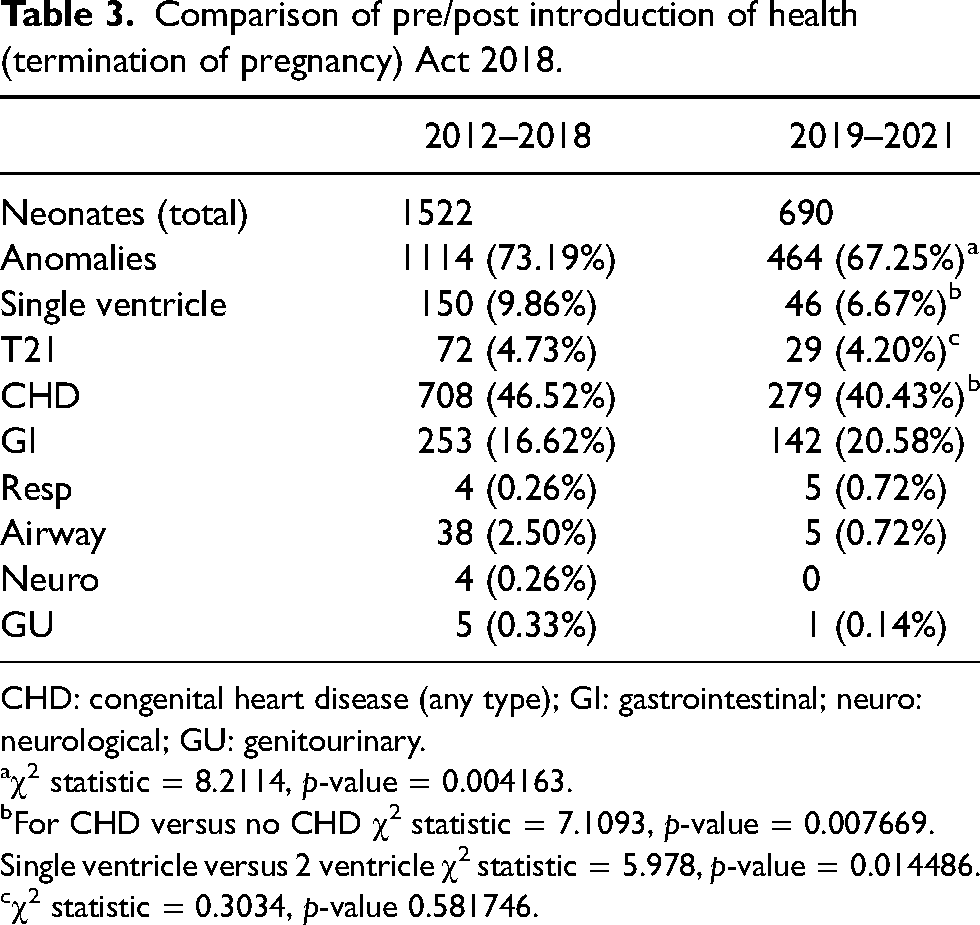
CHD: congenital heart disease (any type); GI: gastrointestinal; neuro: neurological; GU: genitourinary.
χ2 statistic = 8.2114, p-value = 0.004163.
For CHD versus no CHD χ2 statistic = 7.1093, p-value = 0.007669.
Single ventricle versus 2 ventricle χ2 statistic = 5.978, p-value = 0.014486.
χ2 statistic = 0.3034, p-value 0.581746.
Discussion
Our data shows a significant proportion of neonates requiring PICU admission within the study institution have one or more CA requiring significant medical intervention, and identifies several trends. First, there has been a decrease in the number of neonates with CA presenting to PICU as a percentage of all neonatal admissions (73% vs. 67%) since the introduction of the 2018 Act. Analysis indicates that change reaches a point of statistical significance, and also that these variables are not independent. Second, the majority of neonates with an identified congenital anomaly admitted to the PICU had some form of congenital heart disease (CHD), in keeping with the study being performed in a national cardiac centre. There has been a fall in the proportion of these patients since the implementation of the Act (46.5% vs. 40.5%), and this is unsurprisingly mirrored in the the group with single ventricle physiology (9.8% vs. 6.7%). The percentage of neonates with a presumed or confirmed diagnosis of trisomy 21 was similar across the two time points relevant to the study (4.7% vs. 4.2%).
Given the methodology employed, it is not possible to ascribe causative factors to any variations in the data. However, the Act has undoubtedly had a significant impact on the landscape of abortion within the State. When specifically considering CHD, there is compelling data from other jurisdictions that abortion services that are both legal and accessible, in conjunction with accurate prenatal testing, results in fewer live born neonates with complex CHD without any change in the overall number of CHD diagnoses. A retrospective analysis from Denmark showed that as the accuracy of prenatal testing increased the number of live born infants with major CHD decreased due to higher rates of termination. 25 It would follow that this may also be the case in Ireland following on from legislative change. The consequent adjustment in patient characteristics and their requirement for significant medical intervention in the neonatal period may ultimately affect PICU resource use and the structure of neonatal care.
While the change in rates of admission of neonates with CA could be described as being modest, the data must be viewed in the context of the number of women who travelled from Ireland to access abortion services elsewhere in the years preceeding the Act. This was a particularly restrictive time for women in that it privileged those with the means to travel. The UK 1967 Abortion Act is significantly more liberal than the Irish legislation, and as a consequence, Irish women continue to travel to the UK for abortion services, particularly those accessing these services under the provisions of Ground E. While the number of women travelling to England and Wales from Ireland for abortions has declined significantly, the proportion of abortions performed under Ground E has increased, up to 50% in 2021. 26
Despite the availability of local abortion services in Ireland, there still appear to be significant differences between the the UK and Ireland in terms of the number of children born with CA. In 2020, the relative prevalence of CA was approximately 212/10,000 live births (Ireland) and 170/10,000 live births (England and Wales). The prevalence of abortion (/10,000) for foetal anomaly was 35.7 in Ireland, and 49.2 in England and Wales. This variation may reflect differing social, cultural or moral perspectives between the two jurisdictions, or may be indicative of legislative differences, or perhaps challenges to service access in Ireland.
The Irish government recently commissioned an independent review of the operation of 2018 Act,
9
which identified that: it would appear that the legal framework governing termination of pregnancy services is not in alignment with Ireland's human rights obligations insofar as sections 9–11 lack sufficient clarity as to when and how they apply, and application of the law under sections 9–12 … potentially create barriers to access.
9
In respect of s12 (unrestricted abortion < 12 weeks) the Report highlighted several issues germane to this paper. These include the ‘uneven distribution and shortage of services’ requiring women to travel to access a providing GP. There are unreliable referral pathways for ultrasound scanning services, failures to be ‘respectful to women's wishes to see the screen or not’, uncertain ‘pathways for referral of women to hospitals for early termination of pregnancy’, while ‘access to hospital care is in part reliant on a small number of staff’. The contentious, yet mandatory, three day wait between the first and second appointment compounds these problems, particularly for women who are time constrained by the Act: This disproportionately affects women who may not realise that they are pregnant until later in the first trimester or who may have delayed in seeking care, or who may have timed out due to failure of previous treatment to terminate the pregnancy … It can be particularly problematic for marginalized and vulnerable service users where organizing multiple appointments may be challenging.
9
Non-Invasive Prenatal Testing (NIPT) is not a standard part of the Irish public screening service. Even those women who may engage with NIPT may easily time out of the legal abortion window given the effective opportunities and testing possibilities in the jurisdiction. In addition, many foetal anomalies are simply not amenable to diagnosis within the first trimester, effectively removing the legal possibility of abortion for all but the most severe of these.
In respect of the provisions concerning fatal foetal abnormalities (FFA) in the Act, the Report contends that: Section 11 lacks clarity as to how and when it applies, save in straight-forward cases. It can be difficult to implement in practice, even in cases where the condition may be fatal and associated with severe morbidity and/or disability. “Fatal foetal anomaly” is not a medical term. There is not any definitive list of conditions where death occurs in utero or within 28 days of birth.
9
The Report continues, suggesting that subjective nature of interpretation of FFA, ‘together with the prospect of criminal sanction and adverse media scrutiny, risks the practice of defensive medicine, which has likely led to women being denied care to terminate their pregnancy in Ireland’. 9 There are further infrastructural issues that also affect this issue. Screening for structural foetal abnormalities and genetic chromosomal anomalies is required to underpin the operation of s11 of the Act. The former is carried out by ultrasound, women being offered scans at two points in time. Most significant CA, if diagnosed prenatally, are identified at an ultrasound scan at approximately 20 weeks gestation. 27 However, there is substantial geographic disparity in respect of the public availability of specialised foetal ultrasound screening. 15 Of the 19 maternity units in the country not all offer routine ultrasound anomaly scans at 20 weeks gestation. 28 This contrasts with the internationally recognised minimum schedule for ultrasonography in pregnancy which recommends an ultrasound scan in the first trimester and a detailed anomaly scan between 20 and 22 weeks gestation. In a review of services from 2016 only 64% of pregnant women were found to have been offered a 20-week anomaly scan. 28 Furthermore, the Review highlights concerns that the State has failed to provide the perinatal clinical genetics/genomics service required to provide expert guidance on the appropriate implementation of testing and the interpretation of test results, and to provide counselling to parents on the associated outcomes.
Conclusion
Our data suggests there has been a modest reduction in live births with significant CA since the introduction of the 2018 Act as represented by the numbers of these infants presenting to PICU. It is plausible that the introduction of locally available legal abortion under the terms ascribed in the 2018 Act has led to this decrease. The recommendations of the Report on the 2018 Act, if implemented, may lead to further reduction in the number of live births with congenital anomalies, particularly if there is improved access to effective prenatal screening, the expansion of genetic services, the abolition of the three-day mandatory waiting period, clarification of the grounds for the diagnosis of likely fatal foetal conditions, and decriminalisation. However, it may also be the case that many woman carrying a foetus with a CA who cannot avail of a legal abortion in Ireland currently travel to England and Wales. Thus, implementing the recommendations of the Report may have a greater effect on the geographical location of the abortion than on the number of live births of infants born with a CA. This is uncertain, however, and revisions to the Act and its implementation, alongside increasingly available and accurate prenatal diagnostic techniques, may well yet have a significant impact.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.