
Abstract
Conscientious Objection (CO) has become a highly contested topic in the bioethics literature and public policy. However, when CO is discussed, it is almost universally referred to as a single entity. Reality reveals a more nuanced picture. Healthcare professionals may object to a given action on numerous grounds. They may oppose an action because of its ends, its means, or because of factors that lay outside of both ends and means. Our paper develops a taxonomy of CO, which makes it possible to describe the refusals of healthcare professional with greater finesse. The application of this development will potentially allow for greater subtlety in public policy and academic discussions – some species of CO could be permitted while others could be prohibited.
Keywords
Introduction
One of the difficulties which arises when conscientious objection (CO) in healthcare is debated concerns definitions. Without these, parties talk at cross-purposes and obscure the realities underlying their disagreement. Very often, interlocutors (including these authors) find themselves debating CO as if is it should either be allowed or prohibited. However, this is manifestly incorrect. After all, even the most vociferous opponents of CO, such as Julian Savulescu, have written elsewhere that physicians should never participate in certain activities, such as ‘conversion therapy’. 1 And most confirmed supporters of CO (including these authors) would readily concede that there are at least some objections that should be prohibited (e.g. refusing to see a patient because of their sex or race). It seems evident, therefore, that at least some CO should be permitted and some prohibited. The challenge is determining which objections are permissible. Clear communication between interlocutors surrounding the definition and classification of CO is essential to this end.
Clinical medicine faces a similar challenge to that posed by CO when it comes to disease states. Many conditions, such as heart failure and anemia, must be broken down into sub-types in order for effective treatment solutions to be discussed, developed, and applied. After all, no physician would venture to say that anemia needs to be treated with X therapy, because the etiology of anemia is varied, and each underlying cause needs its own treatment. We believe that CO is no different. In order to create nuanced policy regarding CO, one must enumerate the types of CO.
To this end, we attempt: firstly, to define conscience and conscientious objection; secondly, to suggest a taxonomy of conscientious objection in healthcare; thirdly, to briefly explore the implications of these definitions and classification scheme in the ongoing CO debate. It is our contention that once reliable definitions and a taxonomy of CO are recognised, it becomes clear that certain uses of conscience are a necessary aspect of clinical practice because it is closely connected to clinical judgment. This paper is theoretical, and does not, therefore, consider extensively the political and practical aspects of CO, nor the merits of specific policies. Instead, our aim is to support and broaden further debate with ethical analysis and reflection.
Conscience
The ethicist and physician Daniel Sulmasy notes that many believe that conscience is “an intuitive moral sense that determines the rightness and wrongness of actions… a little voice whispering to each of us …”. 2 ,a This aligns with a typical dictionary definition of conscience as “a person's moral sense of right and wrong, viewed as acting as a guide to one's behaviour”. 3 This is sufficient for ordinary use, but not for specialised use in ethics. A divergence between ordinary and specialised word usage is hardly a unique phenomenon; ‘significance’ – for instance – carries a different meaning in common parlance than in the field of epidemiology and ‘dizziness’ generally possesses a different connotation for a clinician than for a layperson.
There is good reason to be sceptical of the value of CO if conscience is merely an impulsive or emotional response. The definition of conscience we provide, while respecting conscience’s place in common human action and experience, maintains that there is more to conscience than this:
b
Conscience is an act of reasoning whereby a general moral principle or disposition is applied to a specific situation by an agent in order to generate a judgement about how one should or should not act.
c
Conscience is primarily an act of the intellect because it is the instrument of practical reason. It exists because of our “meta-moral commitment to morality,” our “fundamental commitment or intention to be moral”. 4 While we instinctively know to seek the good and reject evil, this instinctive and irreducible first principle – often termed synderesis f – does not tell us what is moral. 11 Discerning good from evil entails the use of conscience, which unlike synderesis is not merely an inclination but an essential instrument of the practical reasoning that underpins the project of morality. Conscience, therefore, is at the centre of human conduct. It does not lie dormant until conflict or controversy arise. It is active in all practical reasoning, including all clinical reasoning, though we might only be aware of it when it engenders conflict.
Taxonomy of conscientious objection
Clarifications and definitions
We must note several things before proceeding further. First, the literature on conscientious objection, including this paper, tends to concentrate on the dynamic between doctors and patients. However, the conclusions of our paper could easily be applied to nurses, pharmacists and allied health professionals, who might find themselves refusing to do something they consider immoral, whether instructed by a physician, patient, or other person with whom they share a relationship of responsibility. Any definition of conscientious objection should include all members of the healthcare workforce.12,g Secondly, if medicine is understood to be the same activity fundamentally regardless of where and when it is practiced, the principles of medical conscientious objection should also apply to all jurisdictions, even those in the future. h Thirdly, as we will explore further below, conscience is at work in any decision involving practical wisdom and thus conscientious objection may apply to decisions not only about ends (e.g. what is to be achieved), but also about means (i.e. how to achieve a given end).
Thus, in summary, when moral reasoning conflicts with expectations or demands, a conflict of conscience arises. If an agent determines to follow his conscience and refuses what is expected, conscientious objection occurs.
i
This can occur in any realm of human endeavour, from Desmond Doss’ refusal to take up arms in war to Sir Thomas More’s dissent regarding Henry VIII’s marriage. The definition of CO we offer, though, is specified to healthcare:
Conscientious objection occurs when a healthcare professional – in the course of their duties – refrains from performing or participating in a legally permissible act when asked, expected, or otherwise pressured and incentivized because they judge that act to be contrary to what is right.
j
Objections concerning ends and objections concerning means
As alluded to above, conscience applies to both ends and means. However, objections to ends and means can be distinguished (i.e. one might object to the means but not the ends, or vice versa). Conscientious objection to ends, though, often gets more attention: abortion, participating in capital punishment, etc. Despite these cases often being interesting and useful to discuss, it gives the impression that conscience is only active in contested areas of healthcare and only involves those with religious or unusual moral commitments.13,k
Since conscientious objection flows from conscience, and conscience is necessary for all practical judgements, including clinical decision-making, it does not follow that it should be restricted to a narrow list of controversies. Even when there is no objection to the morality of ends, there are often objections to means or circumstances. A general surgeon may not object to surgical excision of tumours per se but could, under certain circumstances, believe it to be the wrong course in a given case, and therefore decline a patient or colleague’s request. A family physician may refuse to prescribe antibiotics despite the patient’s wishes, not because he opposes the treatment of their ostensibly viral infection, but because he deems antibiotics to be inappropriate under the circumstances. An intensivist might agree that a fragile elderly patient should receive treatment for sepsis, but simultaneously judge ICU interventions to not only be contraindicated but ethically improper and cruel. None of these doctors object to the ends in view (i.e. saving the patient’s life), but rather consider the proposed means pertaining to the action disproportionate, cruel, or even futile and thus wrong. The end might be right, but if the means are wrong, then so is the action in total. l
Objections on technical grounds (i.e. about efficiency or efficacy of certain treatments, diagnosis, prognosis) might see a clinician presented with an expectation to act in a way that he considers not just inappropriate but immoral (e.g. prescribing opioids to someone that he knows is diverting them for profit). Consequently, it is entirely appropriate to speak of conscientious objection which concerns something other than the usual list of controversies. Because conscience is necessary for the formation of every clinical judgement (which is a species of practical judgment), conscientious objection can arise even when ends are not in question.
Moral reasoning about means (and dissenting from improper ones), is the daily task of the healthcare worker. For instance, an orthopaedic surgeon may have no problem with prescribing opioids in principle or treating mechanical back pain. However, she may well object to prescribing opioids for mechanical back pain, judging it to be an inappropriate means. The patient might object that his pain is unpleasant and that there is nothing illegal about prescribing an opioid for it. The surgeon might explain her decision as follows: “Even though I am committed to helping you manage your back pain, I cannot prescribe you an opioid in good conscience, given the addictive potential of opioids and no evidence that they improve your condition in the long-run.” Indeed, we would probably doubt the moral character of a physician who would let themselves be pressured into prescribing an opioid as a means towards even the noblest of ends, if doing so was inappropriate.
This reveals a close relationship between conscience and clinical judgment. m Clinical judgment is equal to the sum of moral reasoning, technical competence, and scientific knowledge. Some have attempted to drive a wedge between these, arguing that objections which concern technical means are not properly conscientious objection. 15 This is mistaken because any medical decision, though it can be formally distinguished as containing a moral and a technical aspect, exists as one act which is the fruit of one global judgment; the moral and the technical cannot be separated, though they can be distinguished. Every clinical decision is based on values—x is good, y is bad—so there can be no purely technical decision in clinical medicine. n Evidence may suggest that prescribing benzodiazepines to elderly patients for sleep is hazardous; it takes resolute moral judgment to refuse to prescribe it when under pressure to do so from a patient with insomnia and their family. Conscientious objection is at work both when the morality of means and when the morality of ends is in question.
The process and result of objection to ends or means are the same: both are arrived at when the demands of conscience conflict with external demands. The decision to conscientiously object to means is usually called clinical judgment o —and this is what it often is—but it should not be forgotten that every clinical judgment is a moral judgment specified to a clinical situation. The moral principle is primary, even in the most routine of clinical judgments, because every clinical judgment is a decision about how to direct one’s care towards a patient’s health (which involves a pursuing benefit and avoiding harm).
While our approach delineates CO by the aspect of an intervention that is objectionable (Table 1), Mary Neal has proposed a parallel framework for classifying CO based on professional and legal standards. 16 Her method categorizes interventions according to the degree of acceptance that they hold within the medical community. Her first category – paradigmatically proper medical treatment – describes interventions whose therapeutic benefit is essentially unchallenged (e.g. antibiotics for bacteremia) and that are performed on consenting patients. 16 ,p However, some interventions, while acceptable for a physician to perform, “[exist] at the boundary of the spectrum of the proper… due to absent/contested therapeutic benefit and explicit or implicit appeal to ‘public good’ factors”. 16 Neal calls this latter group liminal proper treatment. 16 Under Neal’s schema, physicians may object to liminal proper treatments (a category in which she includes practices like infant male circumcision and euthanasia), but not to paradigmatically proper medical treatment. Neal’s proposal seems to contrast with the approaches of other ethicists, like Julie Cantor and Julian Savulescu, who essentially contend that physicians should be willing to perform or facilitate any intervention that is a legal option, even if employed with some controversy in the medical community.17,18
Taxonomy of conscientious objection. If an objection is on moral grounds it can be classified as objection to ends or objection to means.
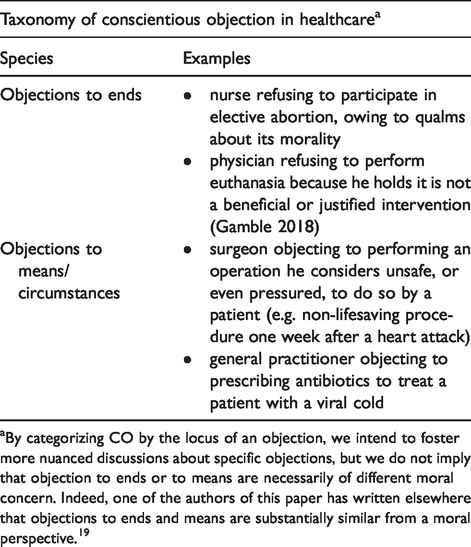
aBy categorizing CO by the locus of an objection, we intend to foster more nuanced discussions about specific objections, but we do not imply that objection to ends or to means are necessarily of different moral concern. Indeed, one of the authors of this paper has written elsewhere that objections to ends and means are substantially similar from a moral perspective. 19
Subspecies of conscientious objection to means
Some examples of conscientious objection to means have been described above. These concern the overtly technical aspects of clinical practice. There are, however, other grounds for conscientious objection to means (see Table 2). For example, it is well-recognised that healthcare professionals should only do what they are competent to do. 20 Hence, a conscientious healthcare professional, even if they have no objection to the ends or means per se, should refrain from an action when they are not competent to perform it. q Doing otherwise might be motivated by noble intentions, but a conscientious healthcare practitioner will recognise the limits of their practice.
Subspecies of conscientious objection to means.
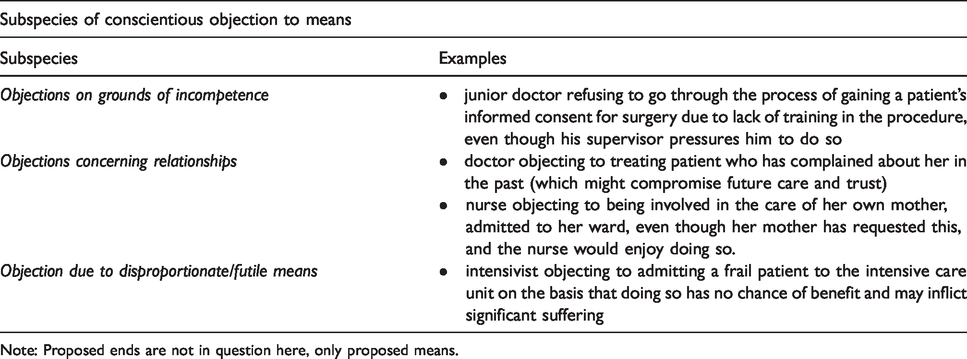
Note: Proposed ends are not in question here, only proposed means.
Since there are degrees of incompetence, this subspecies of conscientious objection is circumstantial. But in many cases, it would generally be recognised as immoral, and not just unprofessional, for a health professional to exceed their competencies. If one attempted something outside of their capability, such an act would not just be wrong because it may violate a professional code (a form of positive law), but because it wilfully jeopardises another human’s wellbeing and is a basic flouting of beneficence. r When a clinician conscientiously resists pressure to perform an action that they lack competence to perform, they are – by our definition above – engaging in a kind of conscientious objection. s
Another subspecies of conscientious objection typically overlooked in the literature concerns relationships with and characteristics of patient. A world-renowned surgeon might object to treating a patient who previously filed a complaint against him, but who now seeks his services again. If the doctor feels unable to remain appropriately detached from the situation, it is plausible that he may object to being involved in the patient’s current care. The clinician who judges that it is not in the patient’s interest to be their doctor because of such a conflict of interest or emotional bias (even if the patient disagrees), is engaging in a subspecies of conscientious objection to means.
Conscientious objection due to personal amity is in keeping with professional guidance about avoiding treating friends and relatives. 20 For example, a nurse might conscientiously object to caring for a friend admitted to the ward on which she works. This can be conscientious if she understands why it is usually wrong to look after friends and loved ones in one’s professional capacity, even though she emotionally wants to do so. As per our definition, there is mismatch between an agent’s judgment and an external or internal force enjoining him to go against that judgement. Some might object that this is merely “professionalism.” However, professionalism is merely another category of moral reasoning, for it concerns what one ought to do given certain professional duties. A decision that invokes moral judgement is a matter of conscience by necessity.
Non-conscientious objection
Having considered two species of conscientious objection (to ends and that to means), as well as several subspecies of the latter, we now consider objections in clinical practice which are not made on the basis of conscience. These non-conscientious objections arise when one declines to perform or participate in an act when neither the ends nor the means/circumstances are in question (see Table 3). For instance, a physician may object to providing a service because the patient (or their care plan) cannot pay for the service, or because the logistics of providing such a service are inconvenient or not sufficiently lucrative. 9 Even though a moral principle is not at stake in these cases, we do not argue that all instances of non-conscientious objection are unacceptable.
Non-conscientious objections. When neither ends nor means are in question then the objection cannot be classified as conscientious.
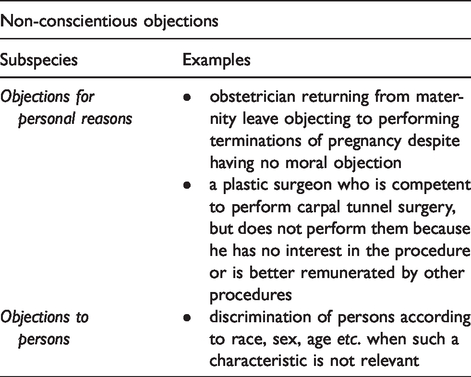
A healthcare professional may object to a given procedure for personal or private reasons. An obstetrician, for example, might object to performing surgical abortions having recently given birth herself and finds it distasteful under the circumstances. The objection is based on private concerns about distress rather than explicit moral reasoning. Indeed, she has no qualms about the means or the ends and has even performed abortions in the past. However, she objects because, at present, she finds performing the act undesirable. t Personal and private reasons such as this, while not being conscientious, are not necessarily unreasonable.
Another species of non-conscientious objection is based on irrelevant patient characteristics. What is relevant in one setting (e.g. age in paediatrics) can be irrelevant in another (e.g. race in ophthalmology). It is often easy to recognise when an objection to persons is on irrelevant grounds; that is to say, the person’s characteristics have no reasonable bearing on the situation. These objections are based on animosity, and do not concern the medical morality of goals or means.
Implications
Defining conscience in an appropriately technical manner refutes the contention that it is the preserve of the religious or eccentric. Anyone committed to acting rightly—which hopefully includes most healthcare professionals—is by the same token committed to employing conscience. Relegating the operation of conscience to a list of disputed services—something which both opponents and proponents of conscientious objection commonly do—is not in keeping with the nature of conscience and healthcare. There has been a general failure in the debate to move beyond controversial-list-thinking and reckon with the necessary operation of conscience in all clinical judgment.
This implies that any proposal to restrict conscientious objection to a narrow set of actions is misguided. If conscience is required by every healthcare provider in every clinical decision, conflicts of conscience can arise in every clinical decision. The close relationship between clinical judgment and CO suggests that the two stand by the same principle of practical reason. Though it is possible to distinguish between species of CO, and to distinguish the technical from the moral aspects of a clinical decision, it is impossible to separate the two, since every global judgement is about means and ends. Both means and ends must be correct for an action to be correct in total. Surely it is not only the disputed areas of healthcare which involve the doing of good and harm. u
Someone familiar with healthcare will acknowledge that every clinical judgment entails a moral judgment about what is good for a patient; however, they may wish to argue that conscientious objection to ends is not driven by beneficent intent. They could contend that when it comes to ends, conscientious objection is merely a mechanism of self-protection which subordinates the interests of the patient. 22 For instance, it has been argued that physicians who object to abortion are only seeking to alleviate religious/moral considerations and are neglecting the pregnant woman’s wellbeing – who arguably faces little medical risk from the procedure but potentially significant psychological and social distress without it.23,24,v
In response, we note that conscientious objection, properly exercised, whether it arises in response to ends or means, is always to do with whether an act is good—beneficent. When one objects to means, one thinks that proposed means conflicts with the requirements of beneficence and should therefore not be performed. The same process underlies conscientious objection to ends, except it is the end which is considered in conflict with the requirements of beneficence. A surgeon who refuses to perform female genital mutilation (FGM, i.e. “female circumcision”) on a consenting patient in a region of the world where it is legal, objects to it because such an act in his view violates the requirement of good health, even if the procedure has low physical risks. Indeed, the act of FGM is an inherent violation of health, for it mutilates a healthy body and intentionally deprives the patient of its proper function. 12 In other words, by performing FGM, a physician does not merely anticipate but actually intends physical harm (or at the very least employs this harm in the causal pathway) to achieve some other good, such as social approval. Thus, notwithstanding patient consent and social approval in certain cultures, such an action is inherently malfeasant. Judging a medical end to be beneficial requires an objective judgement of health – not just patient consent; and if health is not found in the end of the action, the ethical performance of that action would be undermined.
It is a mistake, therefore, to believe that conscientious objection to ends is not concerned with beneficence. On the contrary, a judgement about beneficence and maleficence is at its heart. w
Conclusion
The ethical analysis and framework we have presented demonstrate that conscience is intertwined with practical wisdom and is an intrinsic part of the work of healthcare professionals. The species of CO we have enumerated reveal that morality and values in healthcare are not only related to a few controversial ends, but to all ends and means in medicine, and the relationships between them.
The taxonomy we have presented will feasibly permit a more nuanced discussion of CO, where the issues surrounding and policy solutions for each species of CO can be discussed separately. Such a conversation is an important task. After all, CO will not go away, even if specific belief systems rise or fall. CO exists because humans have an innate awareness of the need to seek good and avoid evil, yet still arrive at disparate intellectual conclusions about what is right and wrong. Thus, if tolerant and amicable solutions are to be developed for CO, conversations on CO in healthcare need to continue with a more integrated understanding of practical reason and an awareness of broad involvement of conscience in medicine. We hope our paper contributes to this end. x
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.