
Abstract
Introduction
Borderline personality disorder patients are often subjected to inpatient compulsory care due to suicidal behaviour. However, inpatient care is usually advised against as it can have detrimental effects, including increased suicidality.
Aim
To investigate what motives psychiatrists have for treating borderline personality disorder patients under compulsory care.
Materials and Methods
A questionnaire survey was distributed to all psychiatrists and registrars in psychiatry working at mental health emergency units or inpatient wards in Sweden. The questionnaire contained questions with fixed response alternatives, with room for comments, about the respondents’ motives for practising compulsory care of borderline personality disorder patients. The responses were analysed quantitatively with descriptive statistics, and comments were analysed with qualitative descriptive content analysis.
Results
The psychiatrists’ views were divided on when it was justified to treat borderline personality disorder patients under compulsory care, as were their views on borderline personality disorder patients’ decision competence. When there was an assessed risk of harm, 53% were positive to compulsory care of decision-competent borderline personality disorder patients and another 31% because they considered the patients to be decision incompetent in such situations. Adding the risk of harm caused many respondents to alter their assessment of the patient from decision competent to decision incompetent.
Conclusion
The large variations in doctors’ opinions indicate that the care of borderline personality disorder patients is arbitrary. Further, the assessed risk of harm increases the use of compulsory care, even though such care is advised against in clinical guidelines, has questionable legal support, and could lead to an increased suicide risk over time.
Keywords
Introduction
Patients with borderline personality disorder (BPD) present a challenge to clinicians, especially those clinicians working at mental health emergency units or inpatient care wards.1,2 The very personality traits that characterize the disorder – rapid mood swings, emotional dysregulation, chronically fluctuating suicidal thoughts and actions, impulsiveness, problems when interacting with other people, black-and-white thinking, and regressive and eruptive behaviour – cause problems not only for the patients in society but also in the interactions with health care professionals.2,3
The suicidal and self-destructive behaviour often brings the patients to emergency care units and hospital wards, but at the same time, the ‘traditional’ psychiatric treatments of suicidal patients, that is, hospitalization, restraints, medication, etc., seem counterproductive when it comes to BPD patients.4–6 There have been numerous accounts of how BPD patients’ self-destructive and disruptive behaviour escalates during inpatient care, and therefore many clinical guidelines advise that hospitalization, monitoring, restraints, and, in general, overtaking of autonomy should be avoided or used with caution.7,8 A recent study has even indicated that crisis-service utilization, such as emergency-room visits and previous inpatient admissions, results in an increased risk for future suicide in patients with BPD – a negative side effect of such care. 6 At the same time, BPD patients are overly represented when it comes to inpatient care and compulsory inpatient care.9,10
To complicate matters further, there seem to be diverging opinions among psychiatrists as to whether the patients are decision competent, whether they should be hospitalized or not and, if so, for how long; whether they should be treated under compulsory care; and even whether they suffer from a severe psychiatric disorder or not. 1 Further, sometimes BPD patients themselves demand compulsory hospitalization in order not to self-harm,1,11 and occasionally clinicians practice compulsory care and prolonged inpatient care on BPD patients to avoid conflict or criticism.11,12
The Swedish Mental Health Act and BPD
A translation of the present version of the Mental Health Act can be viewed in Appendix 1.13,14 When deciding on compulsory care, the patient's best interests and need for care are to be of main importance. In the Swedish Mental Health Act, BPD is generally not considered a ‘severe psychiatric disorder’, which suggests that compulsory care is not a permissible treatment option (Appendix 1). However, it is also stated that personality disorders in combination with an ‘impulsive breakthrough of psychotic character’ – usually displayed as transient dissociative symptoms – can be viewed as a severe psychiatric condition, and therefore may be grounds for compulsory care (Appendix 1).
Decision competence and authenticity in BPD
While decision competence is not explicitly mentioned in the Swedish Mental Health Act, overriding the patient's desire to refuse care in the best interests of the patient is in the bioethical literature seen as ethically defensible only in cases in which the patient is no longer decision competent. 15 This stems from the ethical principle of respecting the patient's autonomous choices unless the patient fails in the ability to make such choices due to a lack of decision competence. 15 In contrast, not respecting a decision-competent patient's choice, in the spirit of parental beneficence, is called ‘hard paternalism’. 15 Decision competence comprises a series of abilities: the ability to understand relevant information, the ability to reason about treatment options, the ability to appreciate the situation and its consequences, and the ability to express a choice. 16 However, decision competence can be impaired by certain psychiatric disorders, such as confusion, thought disorder, and psychotic delusions. 17 When assessing decision competence, the burden of proof does not lie with the patient, who is assumed to be decision competent as the default position. Instead, the caregiver must prove that this is not the case. 18 Moreover, decision competence should be assessed independently of the outcome of the decision. 18
Drawing on clinical experience and a limited number of studies testing the mental capacity of BPD/personal disorder patients in inpatient and emergency settings, the evidence suggests that BPD patients are decision competent.19–21 However, decision competence in BPD patients has been debated, not the least because of the elevated suicide risk, with arguments that when in crisis BPD patients are not viewing things objectively, or are refusing treatment because they want to hurt themselves.22,23 These arguments have been used to support the notion that BPD patients in crisis are expressing a defective will, or, put differently, inauthentic will. Authenticity in this context is understood as making one's decision based on the person's deeper values and desires and has been argued to be a prerequisite for autonomous decision-making. 24 However, as the notion of ‘authentic will’ is so hard to express precisely, it is sometimes regarded with suspicion, and it has even been argued that when making decisions about compulsory care it is useless in practice. 24
Aims of the study
The aim of this paper was to investigate how psychiatrists perceive BPD patients’ decision competence, what motives they have for admitting the patients under compulsory care, and whether these motives are supported by the Swedish Mental Health Act.
Materials and methods
This study is based on a questionnaire survey about the views and values influencing psychiatrists’ decisions on compulsory care of patients with BPD – see Appendix 2.
Participants and distribution
In April 2018, a postal questionnaire was distributed nationally in Sweden in paper form to all (n = 857) psychiatrists and registrars in psychiatry working at mental health emergency units or in inpatient care wards in Sweden. Two reminders were distributed to nonresponders: the first after 10 days and the second (with a second copy of the questionnaire attached) after 20 days from the first dispatch. The list of informants, who fulfilled the requirements described above, and their addresses, was obtained from a national register of psychiatrists via the company IQVIA Solutions Sweden AB.
The questionnaire
The content of the questionnaire was mainly decided based on inputs from a previous interview study. 1 The questionnaire consisted of several claims with fixed alternatives about what motives the respondents find justifiable concerning compulsory care of BPD patients (see Appendix 2 for an English translation of the questionnaire). Specifically, it contained claims about compulsory care of decision-competent patients in situations with the risk of harm or inauthentic requests, compulsory care against a patient's best interests, Ulysses contracts (compulsory care on the patient's own demand), and the decision competence of BPD patients in an emotional crisis (but without comorbidity) and whether such situations motivated compulsory care. All claims were followed by the fixed response options ‘fully agree’, ‘agree to a large extent’, ‘agree to a lesser extent’, and ‘not agree at all’. The respondents also had the opportunity to leave short comments about the topics covered. The background variables collected were age, sex, professional experience in years, and possible influence on trust in the mental health care if BPD patients were subjected to compulsory care without it being in their best interests.
Data analysis
The registration and analysis program used was Epi Info 6. The results were presented as proportions with 95% confidence interval (CI). CIs not overlapping each other were considered statistically significant. The answers from the questionnaire were dichotomized so that ‘fully agree’ and ‘agree to a large extent’ were grouped together in one group and ‘agree to a lesser extent’ and ‘not agree at all’ in another. The background variables sex, experience in years, and change in trust in the mental health care were also analysed for all comparisons (see Table 1). The background variable ‘experience in years’ was dichotomized so that 1–15 (median = 15) years made up one group and 16–54 years the other.
General characteristics of the respondents.
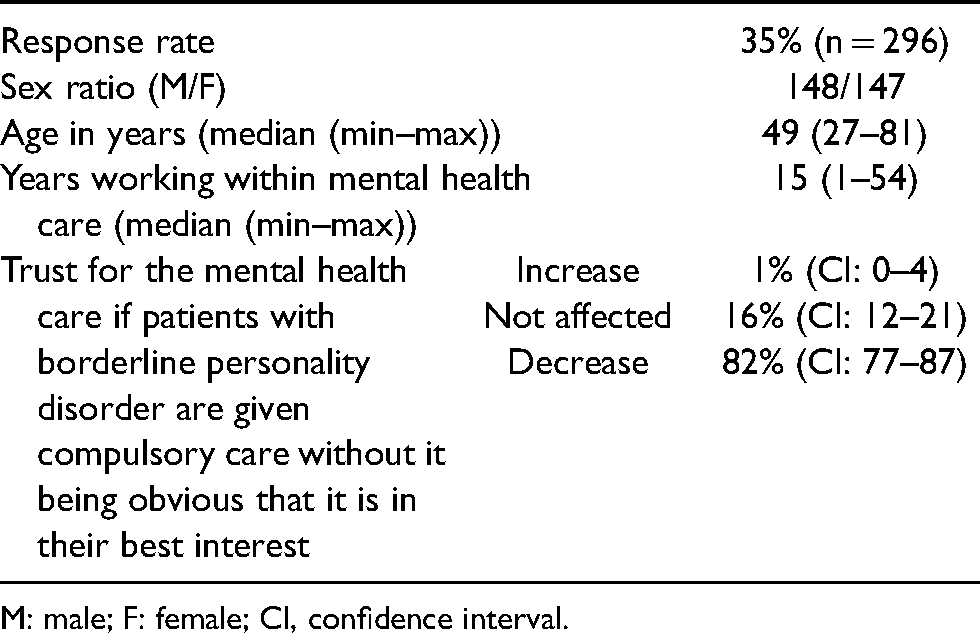
M: male; F: female; CI, confidence interval.
The responders’ comments were analysed using qualitative descriptive content analysis, as described by Sandelowski, 25 to extract subcategories, categories, and themes. First, the comments were read repeatedly to get an overall impression of the content. Next, meaning units and phrases expressing thoughts relating to the overall research questions were identified. The meaning units expressing similar ideas were sorted into subcategories. The related subcategories were then reduced into categories. Finally, the related categories were synthesized into overarching themes.25–27 The analysis was made inductively, with no predetermined categories.
Results
Summary of the main results
Fifty-five percent of the respondents thought that patients should lack decision competence to justify compulsory care, but more than 50% also justified compulsory care of decision-competent patients if they presented a danger to themselves or others. Forty-nine percent of the respondents thought it defensible to use compulsory care that was not in the patient's best interests – if the patient posed a danger to others. For BPD patients in crisis with the risk of self-harm, 84% were positive to use compulsory care – either because they considered the patients to be decision incompetent or because the risk of harm trumped that the patients were decision competent. The qualitative analysis of the respondents’ comments confirmed the large difference in opinions when it comes to whether the BPD patients are decision competent or not, if the BPD diagnosis should be used, whether suicidality by itself constitutes a ‘severe psychiatric disorder’, and if compulsory care of BPD patients has legal support. The comments also showed that compulsory care is sometimes used outside of the legal framework, for example, to facilitate the handling of patients or to protect the staff from potential criticism. The Mental Health Act was thought to leave room for various interpretations, and the respondents thought it difficult to assess a patient's decision competence.
Participants
The number of participants responding to the survey was 296 (148 females, 147 males, and 1 providing no answer); the response rate was 35% (see Table 1). Some questionnaires were not fully completed but each claim stated in the questionnaire was answered by a minimum of 94% of the respondents. Regarding trust, 2% responded that their trust would decrease if patients with BPD were given compulsory care without it being in their own best interests while only 1% responded that their trust would increase. There were no significant differences in trust between men and women or in relation to experience. Of the 296 envelopes containing filled-out questionnaires, only 137 were marked with an arrival date. The analysis concerning differences among early and late responders was only carried out for the responses with an arrival date. There were no significant differences regarding the main claims or background variables between early and late respondents.
Compulsory care of decision-competent patients
A majority, about 55% (CI = 50%–61%), of the respondents agreed that there must be a lack of decision competence to justify compulsory care. However, 52% (CI = 46%–58%) also stated that it is valid to use compulsory care for patients who are decision competent but who may harm themselves, and 51% (CI = 45%–57%) thought it valid if the decision-competent patient was assessed as harmful to others. There were no associations between the answering patterns and gender, experience, or trust (see Figure 1).
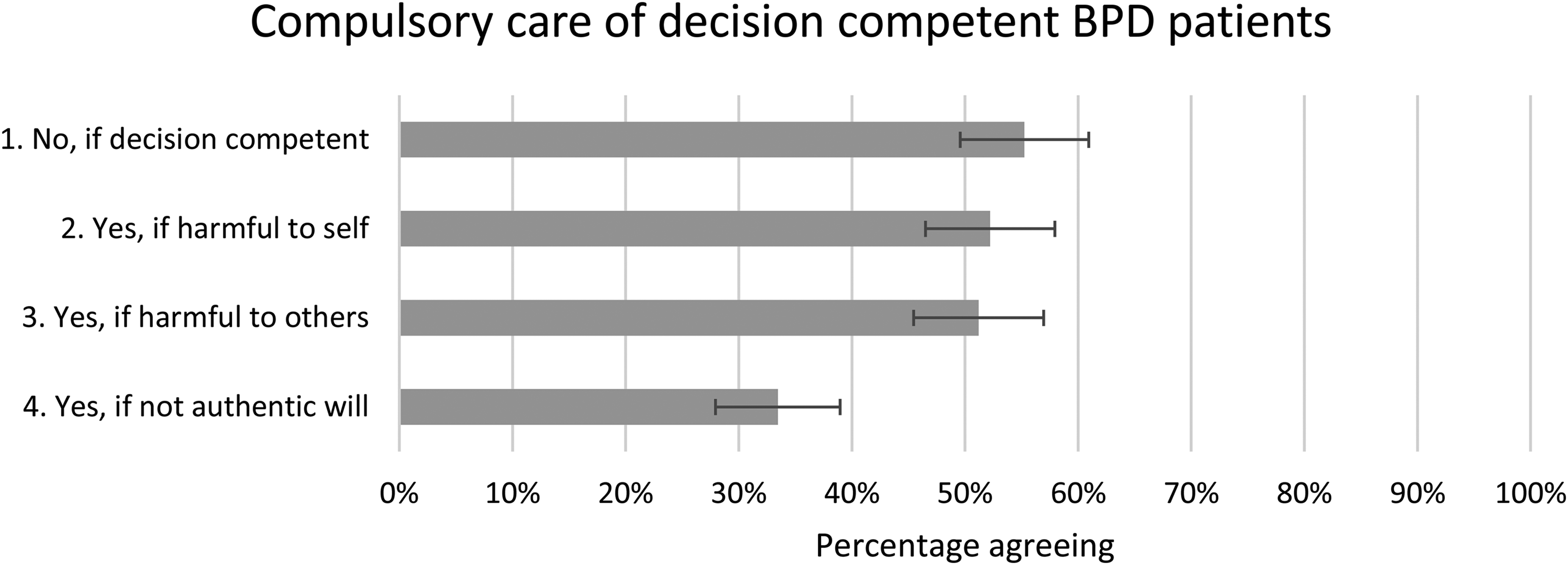
Compulsory care of decision-competent BPD) patients. The proportion of the respondents who answered ‘fully agree’ or ‘agree to a large extent’ with a 95% CI. CIs not overlapping each other are considered statistically significant.
Compulsory care against patients’ best interests
Almost half of the respondents, 49% (CI = 44%–55%), agreed that it is valid to give compulsory care against the patients’ best interests if they constitute a risk of violent behaviour towards other people. Significantly less of the respondents, 16% (CI = 12%–20%), agreed that it is valid if there are no other care options, and very few agreed with the rest of the statements. There were no associations between the answering patterns and gender, experience, or trust (see Figure 2).
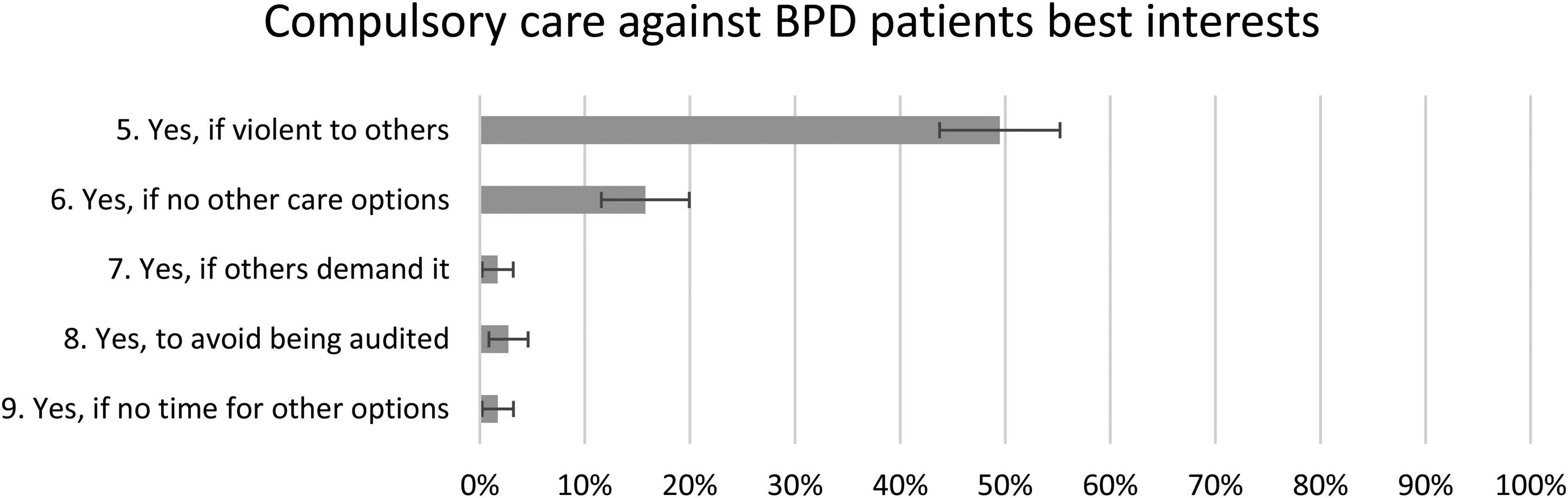
Compulsory care against BPD patients’ best interests. The proportion of the respondents who answered ‘fully agree’ or ‘agree to a large extent’ with a 95% CI. CIs not overlapping each other are considered statistically significant.
Compulsory care on decision-competent patients’ own requests
Only 5% (CI = 2%–7%) agreed it is reasonable to give compulsory care on decision-competent patients’ own requests. However, this number grew to 25% (CI = 20%–30%) and 36% (CI = 31%–42%), respectively, if the patient at the same time is rapidly fluctuating in feelings/impulses or if the care can protect the patient's life. Sixty-five percent (CI = 60%–71%) responded that compulsory care on decision-competent patients’ own requests does not agree with the Mental Health Act while 59% (CI = 53%–64%) agreed it has detrimental effects on the patient's ability to handle negative feelings and impulses. There were no associations between the answering patterns and gender, experience or trust (see Figure 3).
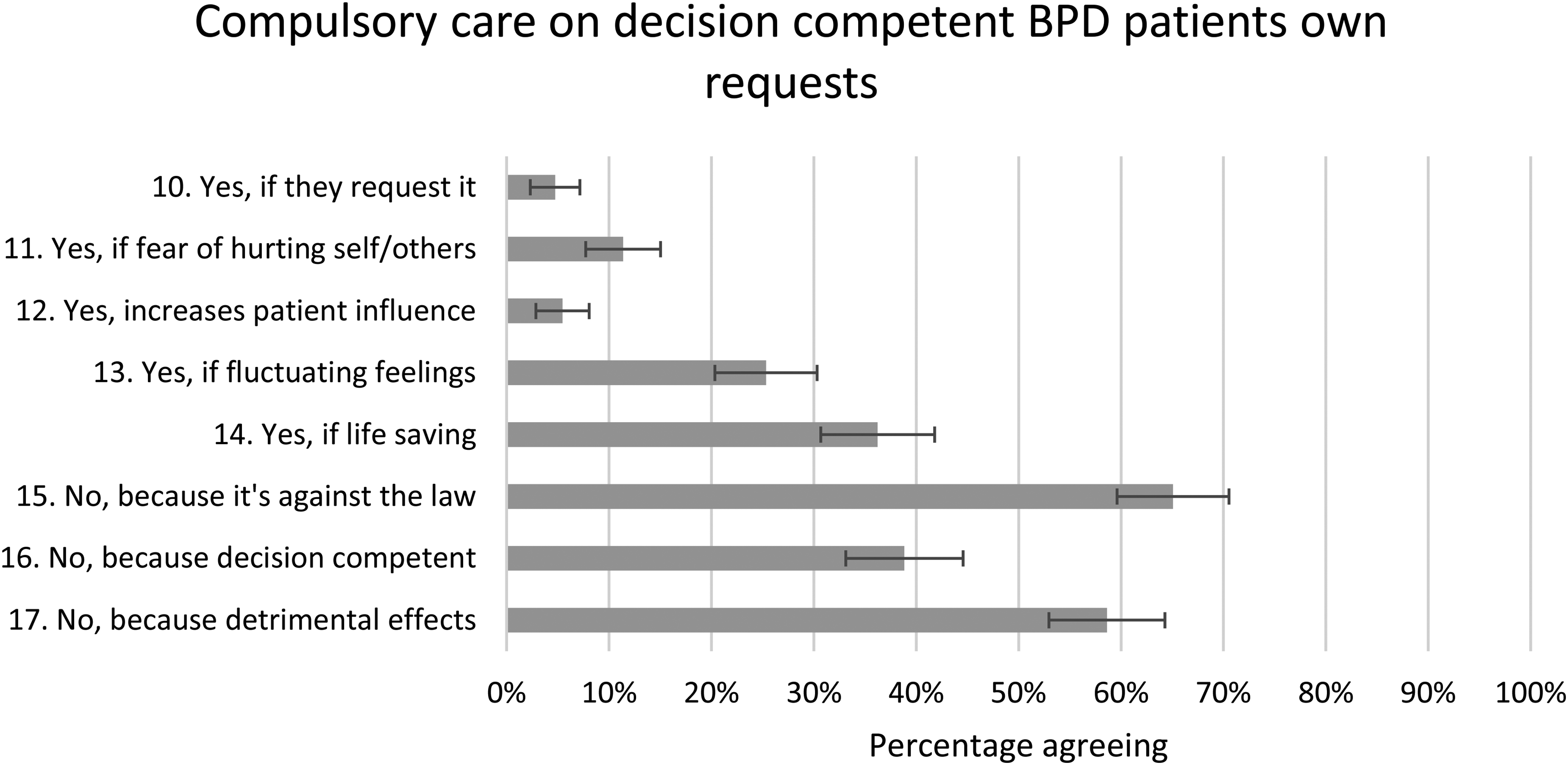
Compulsory care on decision-competent BPD patients’ own requests. The proportion of the respondents who answered ‘fully agree’ or ‘agree to a large extent’ with a 95% CI. CIs not overlapping each other are considered statistically significant.
Compulsory care and decision competence of BPD patients
Thirty-one percent (CI = 25%–36%) of the respondents agreed that from strong emotional breakthroughs BPD patients demonstrate that they are not decision competent and compulsory care may therefore need to be used to protect them from themselves. Fifty-three percent (CI = 48%–59%) responded that the patients are decision competent but may still need compulsory care because they constitute a danger to self or others. Only 4% (CI 2%–6%) thought that compulsory care was not justified because the patients are decision competent and another 4% (CI = 2%–7%) because compulsory care can have detrimental effects. When comparing against background variables, men were significantly more inclined than women to consider BPD patients to be decision incompetent (39% and 23%, respectively). Apart from this, there were no associations between response patterns and the background variables sex, experience, or trust (see Figure 4).
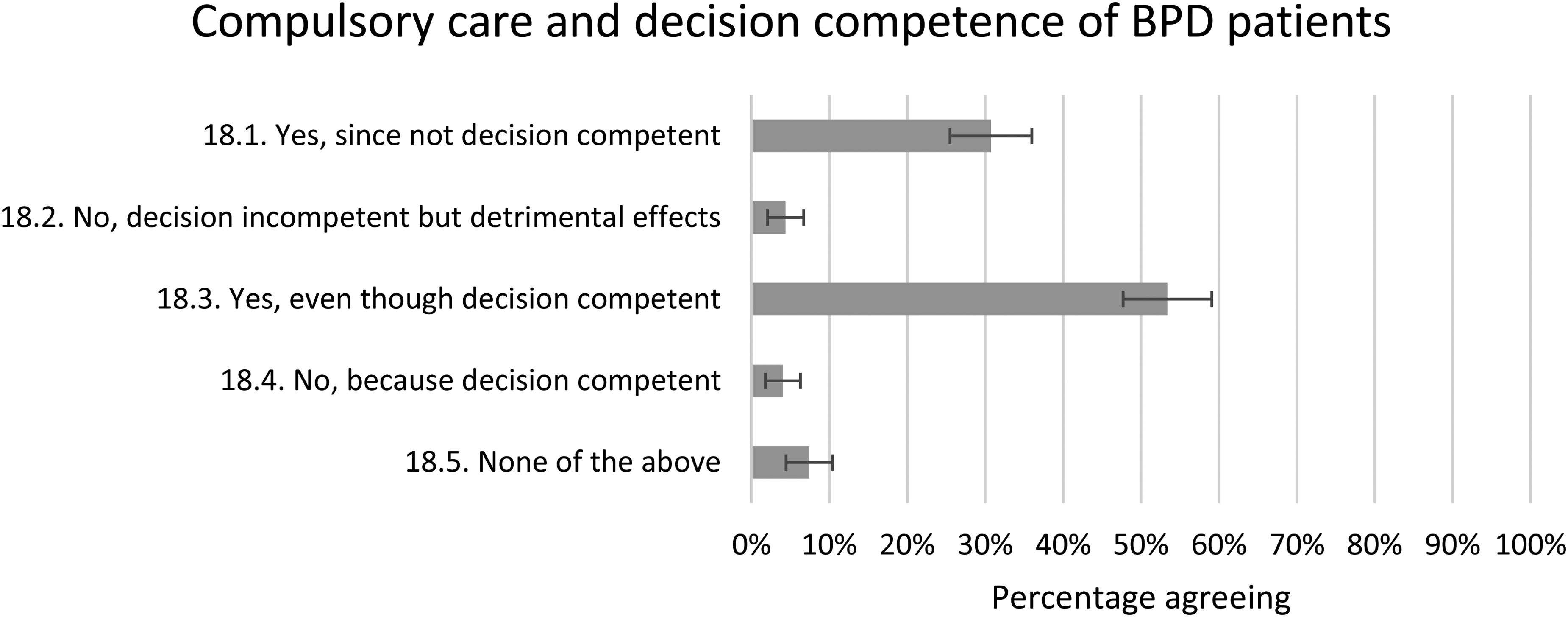
Compulsory care and decision competence of BPD patients. The proportion of the respondents who answered ‘fully agree’ or ‘agree to a large extent’ with a 95% CI. CIs not overlapping each other are considered statistically significant.
Analysis of the responders’ comments to the questionnaire
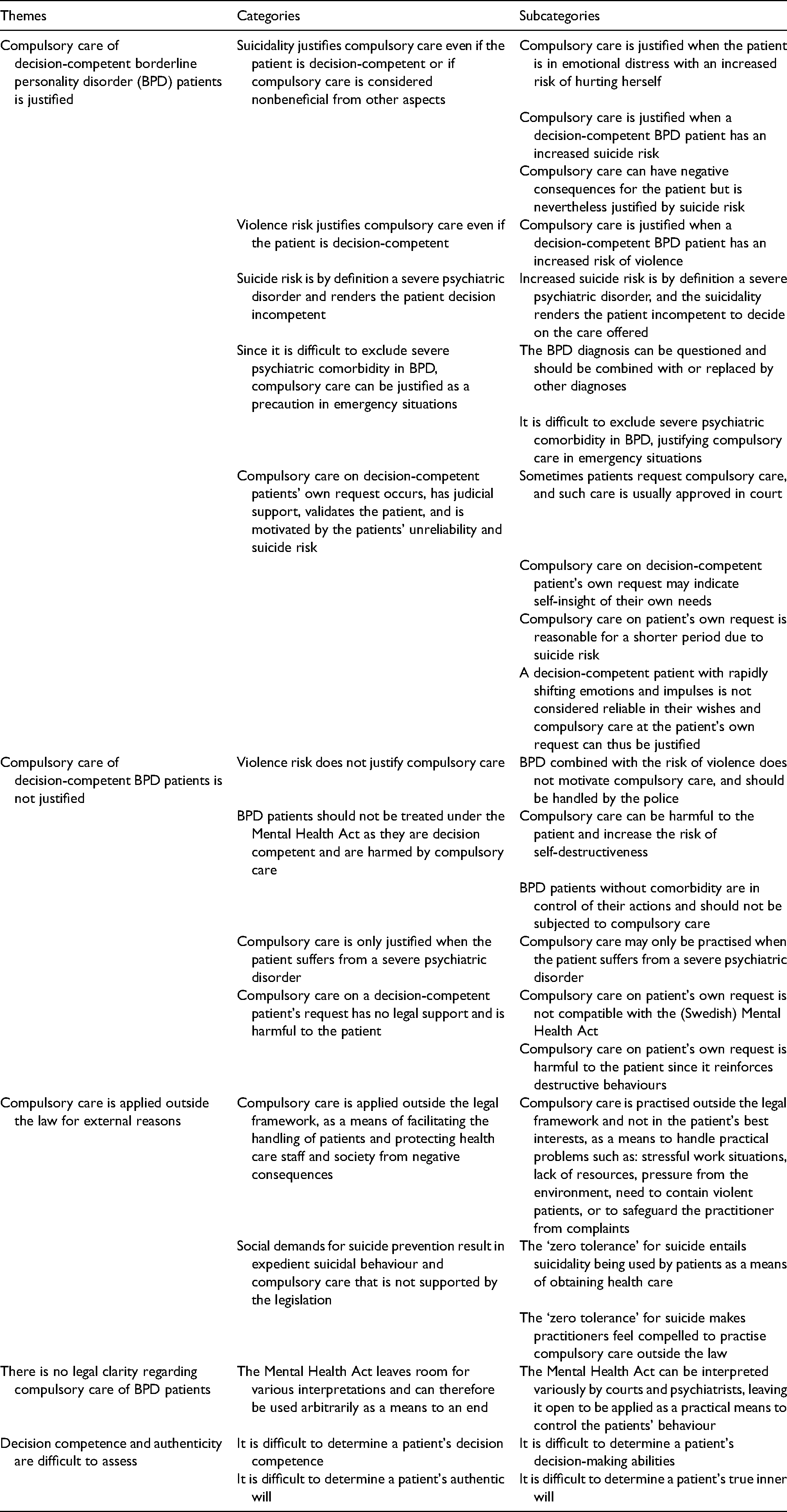
The responders were free to make comments in adjunction with the claims in the questionnaire. These comments were collected and analysed using qualitative descriptive content analysis, resulting in sets of subcategories, categories, and themes. The themes and categories are described in Table 2.
Analysis of the respondents’ comments to the questionnaire. The analysis is based on 168 meaning units, extracted from the comments of 92 respondents. The meaning units have been organized into subcategories, categories, and themes. The full analysis, with references to the anonymized respondents supporting the statements, has been provided to the editor in a supplementary file.
Discussion
The main finding in this study was the divided opinions among doctors in mental health care concerning when it is justified to treat BPD patients under the Swedish Mental Health Act – the respondents’ answers were split in half on several questions, with almost as many for as against. The opinions differed regarding when the patients are considered decision competent, if decision competence should rule out compulsory care, if the assessed risk of harm justifies compulsory care of decision-competent patients, how the Swedish Mental Health Act is interpreted, if the patients should receive compulsory care that is not in their best interests, whether the BPD diagnosis should be used at all, and if it is justified to treat patients through compulsory care when they ask for it themselves. Further, the results point to an argumentative dissonance among many of the respondents when it comes to risk assessment – when a decision-competent patient was assessed as harmful to self or others, this thwarted previously stated principles of respecting the autonomy of decision-competent individuals.
Eighty-four percent thought it justified to use compulsory care of BPD patients in a crisis when there was a risk of self-harm, even if 53% considered the patients to be decision competent in such situations. Thus, for the majority of respondents, the risk of harm trumped autonomy when deciding on compulsory care. Below, we discuss the results in more detail.
Compulsory care of decision-competent BPD patients
Fifty-five percent did not find compulsory care of decision-competent BPD patients to be justified. When it was added that the patient constituted a risk of harm to self or others, some respondents seemed to change their minds as a small majority were in favour of compulsory care of those patients, even when they were decision competent. This inconsistency is highlighted by the fact that 43% of the participants who responded that they were against compulsory care of decision-competent patients were nevertheless in favour of it if the patients risked harming themselves. In conclusion, they seem easily swayed when there was a risk of self-harm, which suggested a paternalistic outlook since harm avoidance then gets to trump respect for autonomy. Interestingly, the respondents considered being a risk to others an (almost) equally valid reason.
Altogether, risk assessment seems to be of importance not only for deciding on compulsory care but also for assessing the decision competence. This could be precarious as presently there are no validated methods to predict an individual's suicide risk with enough accuracy to make it clinically relevant.28,29 It has, therefore, been advised against making clinical decisions in mental health care based on risk assessment. 28 In fact, if risk assessment trumps medical need in clinical decisions, the low positive predictive value and limited sensitivity of suicide risk assessment could entail that the ‘wrong’ patients get prioritized by health care, which, inadvertently, could lead to more suicides. 30 Moreover, decision competence is supposed to be assessed independently of the outcome of the decision, including severely negative ones, as incompetence implies some flaw in information processing rather than disagreement with the decision. 18
Risk of harm to oneself or others does not by itself constitute grounds for compulsory care, according to the Swedish Mental Health Act, but it is to be considered in the weighing of need for residential care. Unless the patient suffers from a ‘severe psychiatric disorder’ and refuses the offered care or is unable to express a considered opinion on the matter, risk assessment is not sufficient to legally motivate compulsory care.
In the light of the objections above, it is difficult to explain the respondents’ sway in opinion only by looking at the legal text or the scientific support for risk assessments. A paternalistic concern could be one explanation – presupposing, then, the questionable idea that compulsory inpatient care of BPD patients is lifesaving.4–6 Yet another explanation could be fear of litigation or other types of professional criticism if the patient comes to harm or harms someone else. The latter reason might be further enhanced by society's expectations on mental health care to prevent all suicides, no matter whether the patient is decision competent or not, and that the caregiver is to be blamed if a suicide occurs.1,31 These motives surfaced in the analysis of the respondents’ comments in this study (Table 2).
Compulsory care against the patient's best interests
Forty-nine percent of the respondents agreed that it is valid to give compulsory care, even if it is not in the patient's best interests, if the patient constitutes a risk of violence to others. This is, at least seemingly, inconsistent with the fact that 82% answered that their trust for mental health care would decrease if compulsory care is given when it is not in the patient's best interests. One can speculate if clinicians feel imposed with potentially contradictory objectives: that clinicians should always act in the best interests of the patient but at the same time always act in the best interests of society. One way to deal with such potentially contradictory objectives is to always act as to reduce whatever harm that seems most imminent, be it in the interests of the patient or of the society.
Compulsory care on decision-competent patients’ own requests
Compulsory care on the patient's own request has no support in the Swedish Mental Health Act, which could explain why very few respondents (5%) agreed that it is reasonable to practise compulsory care on decision-competent patients’ own requests. But even though very few agreed that it is reasonable to give compulsory care if the patient is afraid of harming herself or other people, the respondents agreed to a much larger extent when it was added that the patient is emotionally unstable or that the treatment is potentially lifesaving. One obvious difference between the former two and the latter two scenarios is that the latter imply that the assessment of the patient's psychiatric condition and need for care has been done by the psychiatrist instead of the patient. Once again, a substantial proportion of the respondents seem to express a paternalistic attitude towards patients.
Compulsory care and decision competence in BPD patients
Eighty-four percent of respondents agreed that there are situations of emotional crisis, without significant comorbidity but with the risk of self-harm, where compulsory care of BPD patients is justifiable. However, they did not fully agree on the matter of BPD patients' decision competence: while 31% of the respondents stated that BPD patients are not decision competent in such situations, 53% stated that they are.
The answers reflect the lack of consensus concerning the decision competence of BPD patients found in the literature. Still, most clinical assessments and studies so far point to BPD patients being decision competent.19–21 One explanation why about a third of the respondents assess BPD patients as decision incompetent could be that they think compulsory care is in the patient's best interests in certain situations. Then, to justify their normative conclusion on compulsory care, they let their conclusion affect their factual beliefs about the decision competence of the patient, through a sort of backward reasoning. 32 Another possibility is that authenticity is confused with decision competence in these situations, that is, that the caregiver believes that the patient's ‘genuine’, authentic will is distorted when being in an emotional turmoil, and that this is interpreted as decision incompetence. 22 This contrasts with the more explicitly paternalistic idea, supported by more than half of the responders, which says that BPD patients are decision competent but should still be treated under compulsory care to protect themselves and others from harm.
As of yet, there is no support for the claim that BPD patients are decision incompetent just because they are in a crisis or are suicidal. Further, there is little support for saying that BPD patients benefit from being deemed decision incompetent in such situations. On the contrary, there could be detrimental effects from (compulsory) inpatient care and overtaking of autonomy.7,19,21,22,33 One reservation to the latter statement could be if the patient has entered a transient psychotic state, where there is strong reason to believe that the patient is both genuinely decision incompetent and in high need of medical intervention. In our questionnaire, however, we have referred to BPD patients in crisis without any significant comorbidity.
Despite the possibly detrimental effects of inpatient care and overtaking of autonomy,7,19,22,33 and the presumed decision competence of BPD patients,19–21 <5% of the respondents chose the alternative of refraining from compulsory care because the patient was decision competent, and another equally small percentage chose to refrain from compulsory care because of its detrimental effects. This points to a widespread belief among psychiatrists that compulsory inpatient care of BPD patients is lifesaving, despite lack of support for this belief in the scientific literature – and that this supposedly lifesaving intervention trumps respecting the autonomy of a decision-competent patient.
An interesting detail in this study was that male psychiatrists seemed more inclined to view BPD patients as decision incompetent than female psychiatrists. If this mirrors an implicit bias concerning how male doctors value the capacity of female patients (most BPD patients in mental health emergency units are female), we remain agnostic.
How clinical decision-making could become more consistent and ethically defensible
As previously described in the field of value-based medicine, 34 medical decision-making is increasingly based on complex and conflicting values. This leads to differences in how caregivers interpret symptoms, choose treatments and diagnose patients, and can explain why the same caregiver can act inconsistently depending on the situation. The results of this study are in line with the problems that arise from conflicting values in medicine. One way to solve the problems described in this study could therefore be to introduce value-based medicine in Swedish mental health care. By teaching caregivers to explore and then analyse ethical issues around different ethical principles, decision-making in mental health care could become more equal and ethically defensible.
National variations
When comparing the number of patients who receive residential compulsory care per 100,000 inhabitants in Sweden, substantial regional differences can be seen. For example, in 2017 this number was 152 in Stockholm (the county with the highest number) and 50 in Värmland (the county with the lowest number), according to the statistical database of the National Board of Health and Welfare concerning psychiatric compulsory care. 10 It is unlikely that these statistical differences are entirely derived from regional differences in mental health. Instead, at least a part of the difference can probably be explained by differences in assessments by the caregivers, both at the institutional and personal levels. This national variation indicates that compulsory care is practised unequally in Sweden.
Limitations
The 35% response rate of this study can be considered problematically low. Yet, it is consistent with our experience of health care staff's increasing reluctance to participate in questionnaire studies in the last few years. One can speculate if this reluctance is secondary to the increased flow of information in both society and health care. However, for controversial topics, or if little empirical work has been done on the subject previously (both being true for this study), lower response rates are generally accepted. 35
The questionnaire is not validated. However, it is based on an earlier interview study. 1 Further, a pilot was also done before the questionnaire was completed to provide a better foundation for the design of the questionnaire.
Conclusion
The doctors in the Swedish mental health care profession expressed divided opinions on most questions regarding when compulsory care of BPD patients is justifiable. This suggests that the offered care depends on the individual doctor's personal views, opening up for arbitrariness and inequity in clinical practise.
For BPD patients in a crisis with the risk of self-harm, 84% were positive to use compulsory care – either because they considered the patients to be decision incompetent in such situations (31%) or because the risk of harm trumped that the patients were decision competent (53%). This indicates that striving for risk reduction is considered more important than respect for autonomy in such situations and that the increased risk of harm can be interpreted as a sign of decision incompetence.
Drawing on the respondents’ comments, societal expectations on mental health care to prevent harm, together with a fear among caregivers to be subject to criticism, lead to expedient interpretations of the Swedish Mental Health Act and a disregard of the negative effects that compulsory inpatient care can have on BPD patients – including an increase of suicidal behaviour.
In all, risk prevention seems to be the most important factor for a majority of doctors when they decide on compulsory care of BPD patients – more important than clinical guidelines or legal provisions – even if risk assessments have limited clinical value in predicting suicides and compulsory care has not shown to reduce suicide risk. Unintentionally, this ‘risk-aversive’ practise seems to increase the use of nonbeneficial compulsory care and can increase suicide risk for BPD patients over time.
Ethical considerations
According to sections 3–6 and 13 of the Swedish Ethical Review Act concerning research on human subjects, 36 an ethics approval and an informed consent are needed if the research concerns sensitive personal data, personal data concerning delinquency, physical interventions on research subjects, is performed with potentially harmful methods, concerns biological material from humans, or physical interventions on deceased humans. As this study concerned the health care staff's views on the care of BPD patients, included no sensitive personal data, and no patients were involved, the project was not of sensitive nature and did not need to be ethically reviewed according to the Swedish Ethical Review Act. 35 All the participants in this study were informed in the cover letter that their participation was anonymous and voluntary (see Appendix 2). We confirm that all methods were carried out in accordance with relevant guidelines and regulations.
Supplemental Material
sj-docx-1-cet-10.1177_14777509211040190 - Supplemental material for Psychiatrists’ motives for compulsory care of patients with borderline personality disorder – a questionnaire study
Supplemental material, sj-docx-1-cet-10.1177_14777509211040190 for Psychiatrists’ motives for compulsory care of patients with borderline personality disorder – a questionnaire study by Antoinette Lundahl, Johan Hellqvist, Gert Helgesson and Niklas Juth in Clinical Ethics
Footnotes
Acknowledgements
We gratefully acknowledge the support from the Swedish Foundation for Humanities and Social Sciences (Riksbankens Jubileumsfond), (Grant number P11-0510:1) and Region Stockholm.
Authors' contributions
AL, NJ, and GH contributed to the conception and design of the study. AL, JH, and NJ collected data. AL, JH, NJ, and GH participated in the qualitative and quantitative analyses in the study and contributed to the interpretations of the results. AL wrote the first draft of the manuscript, which was then revised together by JH, NJ, and GH. All the authors have approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Riksbankens Jubileumsfond (grant number P11-0510:1).
Data availability statement
All the authors confirm adherence to the FAIR data sharing policy and can be contacted to present original data from the anonymized questionnaires. The anonymized questionnaires are locked in a safe at the Stockholm Centre for Healthcare Ethics, Department of Learning, Informatics, Management and Ethics, Karolinska Institutet, Stockholm, Sweden. The full qualitative descriptive content analysis of the comments in the questionnaire is also available from the authors, with references to the anonymized questionnaires. Statistical data are kept in an Excel file, which can also be provided by the authors.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.