
Abstract
Objective
Explore parents’ point of view about forgoing life sustaining treatment (LST) in terminal critically ill children and factors affecting their decisions.
Method
This was a qualitative study using in-depth interviews with parents whose child died between 6–12 months old in pediatric intensive care unit (PICU) of a university-affiliated teaching hospital. Interviews were audiotaped and transcribed. Data were analyzed using interpretive description method.
Result
A total of 7 parents of 5 children decided to withhold or withdraw LST. Five parents from 4 children decided to sign the do not attempt resuscitation (DNAR), and none choose to withdrew the LST, including mechanical support. Factors influenced their decision were communication, value of children, child best interest, intuition, religious belief, and emotions. Economic factors did not influence the decision-making.
Conclusion
Most parents decided to sign the DNAR, none choose to withdrew mechanical support. Communication was the most important factor that influenced parents to make a forgoing LST decision.
Introduction
In acute conditions, patients with critically ill condition need to be given aggressive treatment to sustain their life, then an evaluation of the clinical conditions should be done to decide whether the treatment should be continued or not. 1
In North American and European countries, the decisions to withhold or withdraw life sustaining treatment (LST) in the pediatric intensive care unit (PICU) was 20–55%. 2 Parents often find difficulties in deciding to stop curative intervention even when their children are in an end of life condition. 3
Indonesia has different cultures, majority of religion, and also different point of views about the value of child in a family compared to Western countries which will influence parents in making decisions. In Indonesia, a study about decision-making for withholding or withdrawing in PICU has not been done yet. There is a study based on family experiences in making decisions for critically ill adult patients in Ulin Banjarmasin Hospital’s intensive care unit (ICU), Indonesia, factors affecting the decision making process were: communication and discussion about child’s condition between parents and other family members, clear information from doctors or nurses about the actions to be taken, thoughts that the top priority was patients’ recovery, length of stay in the ICU, costs, and family involvement. 4
This study was conducted to answer the research question about parents’ decision making to forgo LST and influencing factors.
Methods
This was a qualitative study with case study design using in-depth interview with a purposive sampling technique in parents whose child died 6–12 months prior to the study. Interviews were audiotaped and transcribed, then the data were analyzed using interpretive description method.
Inclusion criteria were parents whose child had been in a critically ill condition, aged between 1 month and 18 years at the time of their death, and parents had discussed forgoing LST decisions for their child. Parents of critically ill children that lived outside of Special Region of Yogyakarta were excluded.
The trustworthiness of this study was established through careful data collection and analysis that ensured credibility and authenticity, using triangulations sources and data as well as debriefing.
This study’s setting was in a tertiary Pediatric Intensive Care Unit of Teaching Hospital in Yogyakarta, Indonesia with 10 beds capacity. There were 2 attending doctors, among who the researcher was one of them, and 6–8 residents on duty depending on the rotation.
We conducted semi-structured in depth interviews from February 2019 until September 2019 using an interview guide that included 8 questions regarding withdrawing LST. The first question was about the decision that parents took, and then followed by 7 other factors that affected parents’ decision making including communication, intuition, religious beliefs, child best interest, values of children, emotions, and financial burdens.5–10 Each interview took about 1.5 to 2 hours.
Data collection
The interviews took place at participant’s house.
Data analysis
The data were read and coded independently by the first 2 authors and 4th author (Nu, SS and RSP). Content analysis was conducted to the open-ended questions by marking and categorizing keywords and phrases to identify topics and issues of relevance to the parents. In face-to-face discussions between the primary coders, the coded responses were then grouped into broader thematic categories and labeled accordingly. After investigators had concluded the coding, identification of themes, and cross-validation in the second randomly selected set of interviews, as a further cross-validation, the transcripts were also examined in terms of frequency of the codes to ensure that the corresponding themes were pervasively present in the interviews with the parents.
Research ethics
The study protocol was approved by the Medical and Health Research Ethics Committee (MHREC), Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada as the institutional review board [KE/FK/1300/EC/2018].
Results
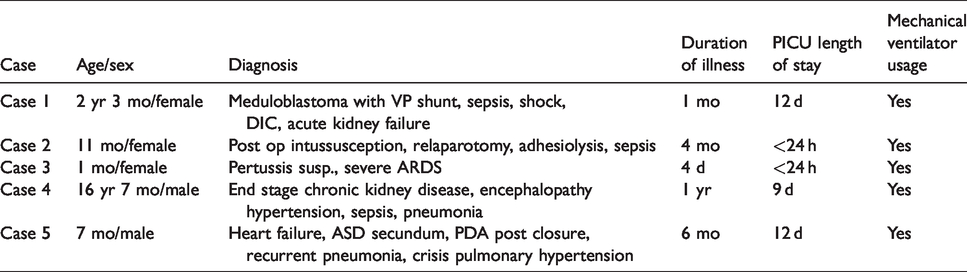
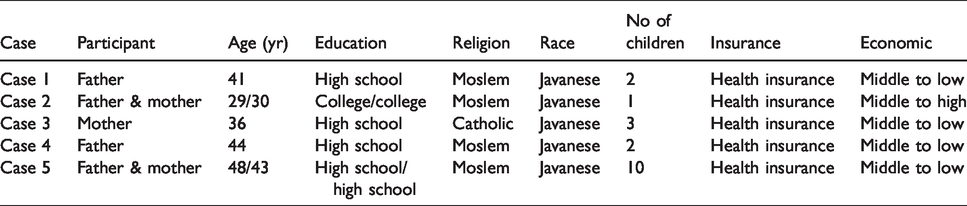
Clinical characteristics of children with demographics and characteristics of participants are presented in Tables 1 and 2.
Clinical characteristics of children.
Demographics and characteristics data of participants.
Qualitative analysis
Interview results
All interviews took place in the participants’ residency. Participant which consisted of both father and mother asked to be interviewed together. Most parents agreed to sign the DNAR (do not attempt resuscitation), while only one couple (father and mother) still wanted the cardiopulmonary resuscitation (CPR) if cardiac arrest happened to their child and refused to withhold or withdraw the LST. Parent from case 4 asked the doctor to continue the hemodialysis for his child even though the child himself stated that he did not want to undergo hemodialysis anymore nor renal transplantation when he was still fully alert. The parent did not want his child to be reintubated and asked DNAR if cardiac arrest happened. Parent from case 1 agreed to stop all medicines gradually, except some medicine for the palliative care. Not all parents agreed to withdraw mechanical ventilation.
From the responses to our 8 questions, we identified the following 7 themes and 16 subthemes describing important factors that affected parents’ decisions regarding withdrawing LST (Figure 1).
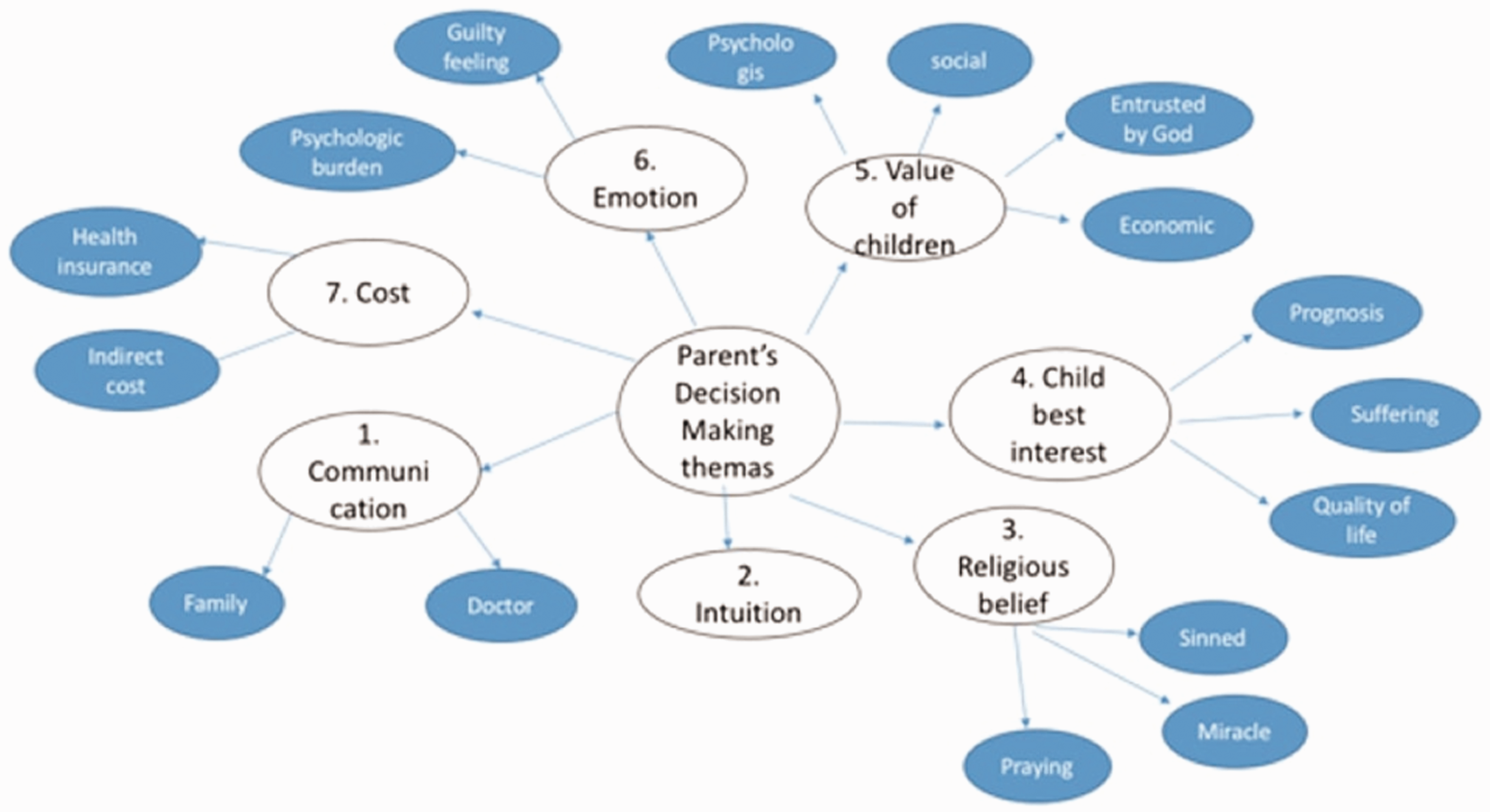
Themes and subthemes factors that influenced parents’ decision making to forgo LST.
Communication
During hospitalization, parents received counseling and explanations relating to the development of patients’ illness. The education was done several times by attending doctors or residents. Some parents said that the information was quite clear, however 2 parents stated that information from the doctor was unclear, therefore they chose to continue all treatments. Parent from case 1 felt the information was unclear in the beginning, so he asked for the maximum therapy for his child and after several counseling (the last counseling with attending doctor), asked the doctor to stop all the medicines gradually. “From the information given before, doctor said that there was still a positive response from my child’s body due to the medical equipment and medicines, so I held on to the treatments. But after hearing the information from the attending, I understood that although we continued the treatments, there would still be damaged to other organs, so I agreed to reduce the medicine.” (Father from case 1)
Intuition
Some parents claimed that inner senses would affect their decision-making.
8
Father from case 1 actually had an intuition that his child could not make it but he rejected that feeling and still decided to give the maximum treatment. One parent had an intuition that their child was in a near death condition. “The point is, I looked at my child condition, and it was like… I often saw people in a near death condition, and my child was already in that condition.” (Parent from case 5)
Religious belief
The researcher found 3 subthemes about religious belief that affected parents in deciding to forgo the LST which were hope for a miracle, praying, and sin.
Some parents who already understood that their children were in a very severe and terminal condition still asked for maximum treatments because they believed and hoped for a miracle. Other parents prayed to God asked the best for their children. Few parents felt that children were mandates from God and parents had the responsibility to take care and raise their children. So, they felt that they committed a sin if they made a decision to stop the treatments including to withdraw the ventilator.
Child’s best interest
We found 3 subthemes for child best interest, which were prognosis, suffering and quality of life. All participants understood that their children were suffering and the prognosis were not good. But they felt like their children were still fighting their illness, so the parents asked the doctor to give all the maximum therapy for their children. However, if the doctor had already given the best care and the child had a cardiac arrest, parents decided not to give CPR. There was 1 participant who did not have the chance to sign the DNAR because the dying process happened so quickly (<24 hours). “Well I thought it was okay, because we'd given the best. I felt sorry for my child if she had to suffer and if we'd given her the CPR, she would have bled. So, I didn't want that. In the end, when the machine's setting was gradually decreased, the only thing I could do was holding her in my arms”. (Father from case 1) “I was worried, how would my child be when he grew up. Because I had a friend at school with a congenital heart disease who was still sick every month until high school” (Father from case 5)
Value of children
This study found that there were 3 values of children for parents: a) psychological value which included pride, amusement, encouragement, strengthen of marriage life, and as successor; b) children were entrusted by God, therefore parents were responsible for their children’s life (jihad); and c) economic value where parents believed that children brought good fortune and were an investment for when they were old.
All participants said that children meant everything. One parent who had 10th child who was born with a congenital heart disease and had been hospitalized 7 times within 7 months was still proud and felt happy to see their child sometimes smiled. They felt that their son's presence brought lots of prosperity and that he was a gift entrusted by God. They took good care of him. “Children are everything, for me it’s a jihad. Jihad was not only in a war, we don’t have to go anywhere to do jihad. I believe that what we do furiously to give the best for our children’s life is a jihad.” (Father from case 1).
Emotion
In making a decision about withholding or withdrawing therapies for the critically ill child, parents feared that they would feel guilty if they had to withdraw the ventilator which could result in accelerating the dying process of their child. That feeling of guilt would not go away and become a psychological burden for the rest of their lives. “I accepted and understood that my child's condition was very severe. But, if I’d agree to unplugged the ventilator I would have felt guilty, wouldn’t I? I would felt the burden (psychologically).” (Father from case 4)
Cost (financial burden)
All the medical bills of the patients in this study were covered by national health coverage. Although there was indirect costs for parents to support their child’s life during their stay at the hospital, but all participants stated that money was not an issue.
Discussion
In this study, the results about forgoing LST decision making varied among parents. In terminal stage of critically ill children condition, at first all parents wanted to provide maximum therapy. After several counseling and the parents realized that maximum or aggressive therapy didn’t bring any good and only worsen the child’s condition, some parents decided to sign the DNAR, although there were still few parents that didn’t want to sign it. This might be due to better parents’ comprehension about their child’s condition, attitude of accepting reality (resignation) or it might be because parents had gone through several emotional stages. 11 There were parents who decided to continue hemodialysis therapy and other medicines even though their own child had already known that the disease was terminal and did not want to continue the therapy, including hemodialysis. In Javanese society, there is a culture called obedient, which includes conformity and obedience, where parents usually become role models. 12
This study found 7 themes for factors that affected parents in decision making. Parents’ decision about forgoing LST was influenced by how the doctor gave an explanation about the child's actual condition. This result was similar with Hafifah’s study which was conducted with adult patients. 4 It also applied to doctor’s explanation about prognosis that was sometimes unclear or even not explained. Therefore, parents still had high expectations for the improvement of their children and decided to ask for maximum therapy. This is consistent with the findings from Cook and Lim.9,10 In making a decision, parents were also affected by their intuition. Although the doctor said that the patient was already in a terminal stage and very unlikely to recover, because of parents’ strong intuition that the child would recover, parents refused to forgo the LST. This is in accordance with the study by Michelson. 8 All participants, both Moslem and Catholics, while believing that withholding or withdrawing LST is not prohibited by their religions, they still believed in the existence of miracles, had a fear of committing a sin, and prayed and surrendered to all God's will; this study’s findings are in line with the previous study by Superdock. 13 Child’s best interest theme included prognosis, suffering and quality of life as factors that are considered by parents in making decisions after seeing that the maximum treatment didn’t give any improvement nor removed the pain. In our study participants asked to continue mechanical ventilation even though they knew their child would have poor quality of life.
Value of children was a dominant factor for parents in making a decision to continue all the treatments and refuse to forgo LST in any condition because children meant everything and there must be a struggle to survive. In Javanese culture, family, including children, is the most important concern in the world. Children provide emotional well-being as well as a core in social orientation. 14
There were guilty feelings and psychological burden on parents if they decided to withdraw the ventilator that was still attached to their child because they would feel like they were the one who caused their child’s death. Meanwhile, cost was not a concern even if the child needed to be treated for a long period of time. Although there were still some indirect costs, all the medical bills were covered by the health insurance. This finding differed from study by Michelson that stated that cost/financial burden affected parents’ decision-making in withholding or withdrawing LST. 8 This difference could be caused by cultural diversity, in which Indonesia, including, Javanese ethnic, has a mutual cooperation and sharing manners where friends, neighbors, and especially the extended family will help to ease the burden of their relatives who are in trouble. 15
Conclusions
Most parents decided to withhold LST as in DNAR for terminal critically ill children while refusing to unplug mechanical ventilation as withdrawing LST. Communication, child’s best interests, religious beliefs, and intuition greatly influenced parents in deciding to forgo LST. Value of children and emotions were factors that influence parents not to decide forgoing LST, while financial burden did not affect the decision-making. Further investigation needs to be done to explore factors improving effective communication between doctor and parents.
Study limitations
This study had limited number of subjects. Interviewer’s role as one of the attending doctors who directly treated the patients could cause bias for this study.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for the preparation of this manuscript was provided by the RSUP DR. Sardjito (HK.02.03/XI.2/19047/2018).