
Abstract
While the ethic of care has generally been regarded as an appropriate attitude for nurses, it has not received equal attention as a mode of ethical problem solving. The primary nursing model is expected to be aligned with the ethic of care because it emphases the nurse–patient relationship and enables more independent role for nurses in decision-making. The aim of this study was to examine nurses’ ethical decision-making in the context of primary nursing. Participants were seven nurses, and one physiotherapist from a geriatric rehabilitation unit of a public hospital in Finland. Data were collected through focus group interviews and qualitatively analyzed through Lyons’ coding scheme for moral orientations. The results showed that primary nurses employ empathic understanding and particularistic thinking when building relationships with patients and their families, and when assessing their needs for coping at home after discharge. Most ethical conflicts were related to discharge and were solved through balancing the ethics of care and justice considerations. It is concluded that care and justice are integrated in nurses’ everyday ethical decision-making. The ethic of care nurtures good patient–nurse relationships, while the ethic of justice is needed to address the fair delivery of care in the context of an aging population and diminishing public resources. Both ethics should be acknowledged in clinical practices and included in ethics education.
Keywords
Introduction
While the ethic of care has several philosophical roots, its popularity across various sciences can be traced to Carol Gilligan’s (1982) claim that there are two different moralities. The ethic of justice is centered on maintaining obligation, equity, and fairness through the application of moral principles, rules, and established standards, whereas the ethic of care is centered on maintaining relationships through responding to needs of others and avoiding hurt. 1 These moralities tend to perceive, interpret, and solve moral problems in different ways. Whereas justice sees them as opposing claims arising from rights and duties between individuals, care sees these as arising from tensions or ruptures in relationships. In justice reasoning, moral conflicts are solved through applying a hierarchy of rights and rules to determine which claim is the most justified. In care reasoning, moral problems are solved through considering the unique characteristics of persons and situations. In essence, justice reasoning seeks a universally applicable solution that can be applied to all similar cases, whereas care reasoning represents a particularistic mode of moral thinking that is based on the full description of the case at hand.2,3
In the field of nursing, Gilligan’s theory and related feminist moral philosophy4,5 were initially accepted with enthusiasm, as it theoretically captured the essence of caring embedded in patient–nurse relationships and explained the ethical difficulties nurses encountered in medically dominated healthcare contexts. 6 Scholars have seen the ethic of care as a promising approach to strengthen the voice of nurses in ethical discussions which has so far been dominated by justice-based theories. 7 According to the review of Woods, the attempts to build nursing-specified theories have so far gained mixed success. Within nursing, an ethic of care has been regarded as a recommendable attitude, but one that is inadequate to guide decision-making in practice. 6 Disappointing outcomes may be due to the fact that Gilligan is a psychologist presenting empirical observations, but has largely been interpreted as having presented a ready-made ethical theory. 8 However, few empirical studies explicitly employing Gilligan’s theory have pointed out that nurses use both care and justice considerations in ethical decision-making.9,10 Moreover, longitudinal studies among social and healthcare students have shown that they follow a developmental path of the ethic of care proposed by Gilligan11,12 and their level of care reasoning is reflected in their ethical decision-making. 13
The present article examines nurses’ ethical decision-making in clinical settings specifically in the context of primary nursing of elderly care. We argue that primary nursing might be aligned with the ethic of care by sharing emphasis on the patient–nurse relationship and heightened responsibility, requiring critical thinking and decision-making capacities. Thus, the scrutiny of the ethical conflicts that primary nurses encounter and how they solve them may reveal some of the essential dynamics of nurses’ ethical decision-making.
Primary nursing model
Since the 1960s, primary nursing has been considered as the ideal model of care delivery that enhances the nurse–patient relationship and enables a more independent role for nurses in clinical decision-making. The assigned nurse assumes overall responsibility for patient care during the hospital stay and is answerable to the patient, the patient’s family, and to colleagues. Previous research shows that the model contributes to nurses’ increased senses of job control and autonomy. 14 Primary nursing enables a more holistic role for nurses across a caring process that is often fragmented in contemporary healthcare contexts. It drives nurses to address patients’ complex needs, rather than to perform specific job tasks under given structures. 15 In practice, the primary nurse builds a sound relationship with a patient, as well as develops and implements the plan of care for individual patients. The model is supposed to promote ongoing communication between the patient, family, nurses, and physicians, and to facilitate discharge planning. 16 In order to achieve a high quality of care, primary nurses need to work closely with colleagues and other professional groups. 14
Primary nursing is a method of delivering individualized care that is assumed to be especially suitable for older patients, 17 who are more often frail and vulnerable and so require a holistic approach to their management. However, few intervention studies in aged care settings do not clearly support the effectiveness of primary nursing in terms of patient well-being, maybe due to the limited incorporation of the model into practice. 18
The context of the study
Finland has the fifth oldest population in the world. 19 In order to arrest rising costs in public healthcare, the national legislation was revised in 2012 to support the independent living of older people, shifting the emphasis from institutional to home-based care. 20 This, as well as the varied financial resources of municipalities, frames healthcare professionals’ work in hospitals, as long patient stays are not preferred. On discharge, patients should be promptly located in home, assisted living, or nursing home environments. This change in direction poses further challenges to strengthening shared decision-making and collaboration among professionals within the care chain, and requires inclusion of family members in care planning and provision. 21
The present study was conducted in a geriatric rehabilitation ward of a public hospital in southern Finland. At the time of data collection the ward had 30 beds, patients were 75 years of age on average, with approximately an eight week average length of stay. Patients usually come from units of special care and are not yet able to cope outside the hospital setting. Hip and other fractures, worsened health conditions, and memory disorders are the general reasons for admission. The main aim of rehabilitation is to advance patients’ self-sufficiency in order to support their independent or assisted living for as long as possible. The staff adopted the primary nursing model in 2015 to ensure quality of care. Every patient is assigned a primary nurse who is responsible for developing and implementing an individual care plan through the hospital period, including networking with family members and other professionals, as well as planning and preparing the discharge process. The primary nurse is responsible for service needs assessments concerning the patient’s coping at home and preparing applications for institutional care placements. Decisions on discharge are made in weekly meetings by a multi-professional team comprising of physicians, nurses, physiotherapists, and a service manager.
The authors from a local university of applied science were invited to plan and carry out the project aiming at improving primary nursing practices in 2016. The project was triggered by difficulties experienced in the discharge process, and was co-planned with a head nurse and staff members.
The study
Aim and research questions
The study looks to examine nurses’ ethical decision-making in the context of primary nursing in a geriatric rehabilitation unit. The research questions are as follows: (1) What kind of ethical conflicts do primary nurses encounter; and (2) How do primary nurses solve ethical conflicts in the context of the primary nursing of older patients?
Research design
Participants were seven nurses and one physiotherapist on duty that were interviewed through a focus group method 22 by the authors. The physiotherapist was included, because she actively worked with the nurses on a daily basis. All the participants were female. Their mean age was 36 years, ranging from 23 to 63, and they have worked 11 years on average (SD = 12.6) in the healthcare field. Interviews were first conducted in three small groups to elicit individual ethical conflicts that were then further elaborated in the united group. The interviews consisted of broad questions concerning the nature of actual ethical conflicts, ways and strategies of problem solving, and the involvement of other people in the conflicts. Prompt questions were asked to elicit reasons for ethical decision-making: Could you describe the situation? What were the conflicts for you in that situation? What did you do? Do you think it was the right thing to do? How did you know afterwards that it was the right or wrong thing to do? 23 The interviews were lively conversations and the participants openly expressed their concerns and feelings.
The interview workshops were audio-recorded and transcribed verbatim. The overall duration of the audio data was 4 h and 23 min, yielding 78 transcribed pages (font Times New Roman 11, single line). The data were analyzed by directed content analysis 24 that was conducted to categorize, reduce, and describe data in terms of meaningful themes using Lyons’s coding scheme 23 as a framework. The analysis was conducted by the first author and checked by the second author. To enhance the validity of the study, the initial results of the analysis were presented and discussed in the project’s successive workshop, involving 22 nurses in the unit. To support the credibility of analysis, quotes from the focus group interview are given in the “Results” section. The quotes were translated from Finnish to English by a native English-speaking interpreter.
Ethical considerations
The study was conducted as a part of established co-operation between the hospital and the University of Applied Sciences, in accordance with the guidelines of the Helsinki declaration (2013). The research plan was approved by the ethics committee of the Federal of Universities of Applied Sciences on 1 June 2016.
Subjects volunteered to participate in the study as a part of the development project and no compensation for participation was provided. The researchers highlighted that the participants’ anonymity would be secured and any personal information would not be disclosed to their managers. All participants received written and verbal information about the study and signed to indicate their informed consent.
Results
Empathic understanding and particularistic thinking as tools of ethical reasoning
According to Lyons’ coding scheme, care reasoning is defined as seeing others in their own situations and contexts, and responding to them in their particular terms. In the analysis, these two aspects of thought were redefined as particularistic thinking and empathic understanding. They formed an overarching theme across all of the group conversations. Empathic understanding can be seen as a basic attitude that builds rapport in nurse–patient relationships. In turn, it is based on particularistic thinking that recognizes patients’ subtle needs beyond symptoms and overt behavior, as the following quote exemplifies: A patient (…) who becomes institutionalised is, on the one hand, the kind of person who gets used to certain routines and is afraid of change, even if it is just a small change, such as another nurse on duty (…) This creates a feeling of insecurity if you suddenly have to go to another place. Yeah, home visits, there you can already see pretty much how the patient is able to move around in there… And if the patient even recognizes the home anymore (…) If necessary, home care is requested to come on-site. And conducting interviews is precisely what we do, we ask the family members to fill in the family surveys. We attend the discharge meetings, too, we discuss issues in a multi-professional way, where doctors and physiotherapists and head nurses and all are present (…) There is also a service manager who guides and advises them on follow-up matters. So we all work in cooperation, we do not make the decision alone (…) Of course, when we make a referral for a service needs assessment (during patient assessment) it also includes some free text, so the opinion of the primary nurse becomes clear. It also includes the opinions of family members and the patient, but also the nurse and the multi-professional team, on whether the patient is still capable of coping at home or not.
Ethical conflicts in primary nursing practice
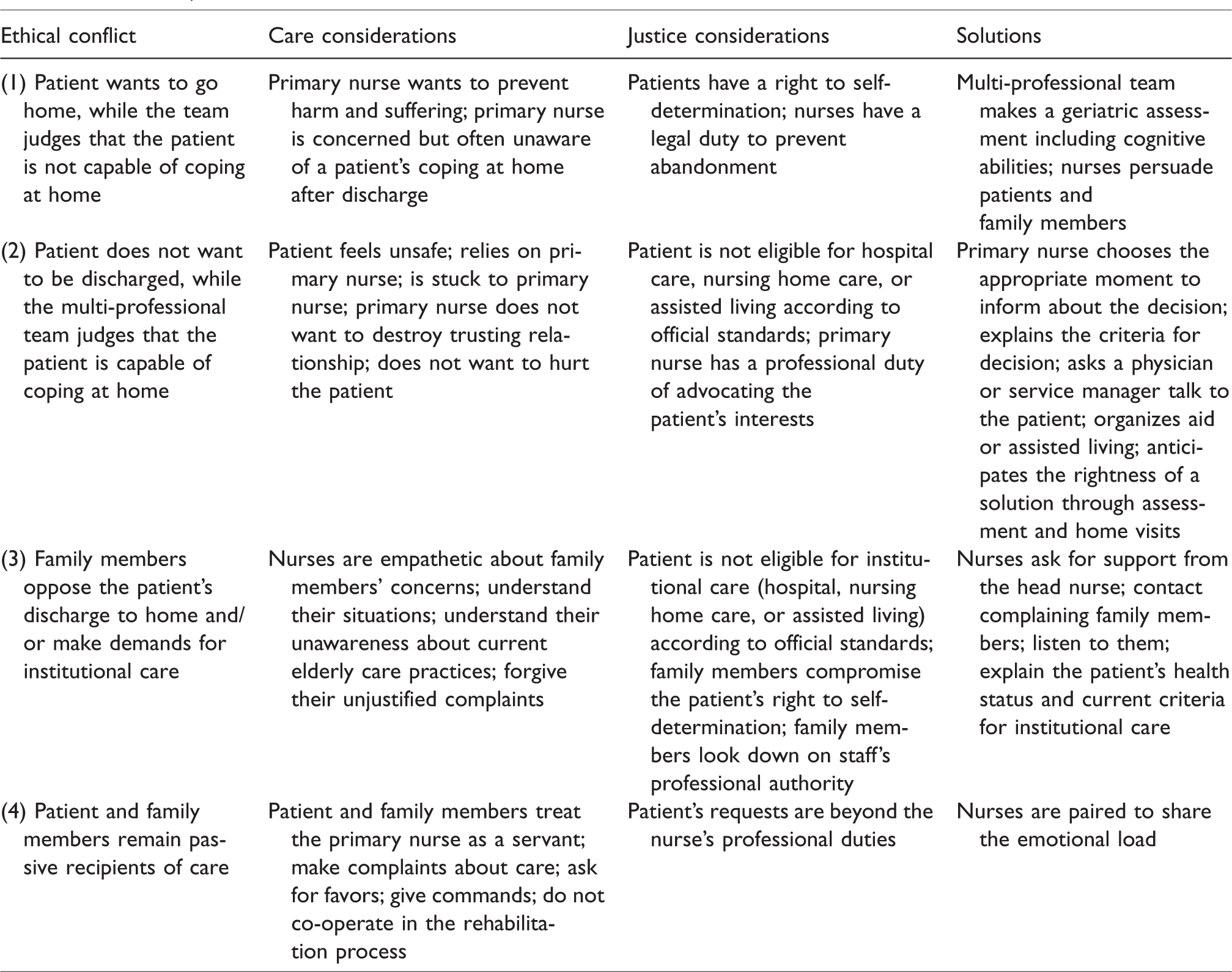
Participants brought up four types of typical ethical conflict, three of which were related to the decision-making about patient discharge and one to the patient–nurse relationship. Table 1 summarizes care and justice considerations and proposed solutions for each conflict. Conflict 4 directly addressed the nurse–patient relationship that is disturbed by a growing number of patients who do not comply with the role of being “cared-for” but rather impose themselves as customers by treating primary nurses as servants and asking for favors. According to the interviews, this is a relatively recent phenomenon obviously coupled with a cultural change in “care culture.” Due to space limits, further analysis of this conflict has been omitted from this paper. Next, we introduce the remaining three ethical conflicts to illuminate primary nurses’ ethical decision-making.
Care and justice considerations across ethical conflicts.
Patients want to go home when they are not capable of coping at home
Some patients want to leave the hospital, even though according to a multi-professional team assessment they are not yet capable of coping at home. These patients are not fully aware of their limited functional abilities, usually due to memory disorders. The ethical conflict arises as whether to respect the patient’s right to self-determination and allow them return to home, even though it may pose a risk that the patient’s state may deteriorate and they will soon be back in hospital. For me, there was maybe a feeling that we cannot do it, the nurses and our doctors, all of us, that we cannot let the patient go. That then the next day the patient will be back in hospital again with a new fracture. So what is there to do (…) Is it, in a way, also a question of respecting the right to self-determination or is it, in a way, abandonment? Then there is the fact that we have clear guidelines and indicators that provide a framework for us. In a way, it is easy to rely on them (…) you must try staying at home before going directly to an institution. I cannot say whether the decisions have been correct or not, I really do not know, it is difficult to say (…) But, of course, you continue to think about your own patient, or patients, the most, that ‘what if?’. And then you always talk about it with the other primary nurse.
Patients want to stay in hospital, while the multi-professional team judges that they are capable of coping at home
Within this typical ethical conflict, patients do not want to leave the hospital or return home because they lack self-confidence in their coping abilities. They ask the primary nurse to advocate their wish to stay in the multi-professional meeting that makes decisions on discharge. Usually these patients are in relatively good physical shape, but due to previous falls or sudden medical episodes they feel unsafe. They are also prone to cling to their primary nurses due to their vulnerable state and run the risk of hospitalism.
This ethical conflict has several dimensions. On one hand, the primary nurse empathically understands the patient’s fears, but on the other, she knows that according to the criteria and her own professional judgment, the patient should already be capable of performing daily activities at home. The ethical conflict lies between the ethics of care and justice: how to respond to the patient’s psychological needs and simultaneously uphold the official standards for hospital care provision? The conflict is complicated by the fact that according to the prescribed duties of the primary nurse, she is obliged to advocate for the patient’s interests (justice). She also does not want to destroy a trusting relationship and hurt the patient’s feelings by betrayal (care). Yeah, the professional staff (…) thinks that the patient could return home but, on the other hand, the nurse also understands the patient, what it is that makes the patient not want to go home and why he or she feels unsafe. And then there is the fact that you try to justify that opinion, when the patient has to be transferred but, on the other hand, you feel bad for the patient, that you should not betray his or her trust. Because, as the primary nurse, you are the patient’s advocate. It somewhat depends on the case, on what the patient is like, you have to consider where you are at. If you say something at the wrong time that may torpedo it (…) kind of just add to it – the anxiety and other things. So… the issue must be handled, it just has to be. And how do you say it. You need to be able to justify it, although often, if family members or the patient are really difficult, we will have a doctor come and discuss it (…) However, usually all agree in the end (…) You are not left with a feeling that you have forced anyone to go anywhere. So you cannot say that the right decision was made, but an agreement of some kind was found, anyway. We ended up applying for a place in assisted living, but it just came to my mind whether we are taking a place from someone else who is in worse shape. Even though, as the primary nurse, I understand that, of course, the family members and the patient are really worried about coping, especially due to previous falls.
Family members oppose a decision on a patient’s discharge to home
An ethical conflict arises when the multi-professional team has made a decision about instituting a discharge process that is opposed by family members, typically by the patient’s children. In conjunction with the head nurse, primary nurses are often involved in disputes with family members who wish the patient to stay in hospital for longer, or to be moved into residential or nursing homes. Nurses cannot go along their wishes if the patient’s condition does not meet the criteria for a prolonged stay in hospital or institutional care. Sometimes family members’ wishes also contradict the patient’s desire to live at home and undermine their right to self-determination.
Employing the ethic of care framework, nurses try to empathetically understand the actual situation of the patient’s spouse and children. First, children are usually in the rushed middle-age of life with multiple responsibilities in their families and workplaces, and at the same time they try to keep an eye on their vulnerable parents living on their own. Therefore, the parent’s admission is in some ways a relief and frees them temporarily from stressful care-taking. Sometimes those situations have of course been really hard for the family members for a long time at home, so they can be really tired. Then (…) they feel that it is a kind of salvation that now he or she is in treatment. Because it is definitely psychologically stressing if you are having a really hard time, for example, a patient with dementia at home who needs constant care. And the spouse is a family caregiver. It is not very easy. We have a really, like, sort of a long history that if you are ill, you are in hospital, or that if you cannot cope at home, you are taken into a nursing home (…) Here we see that this will change and has already changed a lot. But people out there do not understand that it cannot continue in the same way anymore, that everyone would live in an institution at some point. It has changed and is changing all the time here.
Nurses try to solve their ethical conflicts from both care and justice perspectives. They anticipate and prevent controversies by careful listening and showing an understanding of their difficult situations. They explain the official admission criteria for different forms of care that are regarded as impartial rules constituting fairness in society. Ethical decision-making is ultimately justified by arguments of impartiality, enabled thorough individual assessment and evidence-based knowledge.
Discussion
The aim of this study was to examine primary nurses’ ethical decision-making in a geriatric rehabilitation unit by employing Gilligan’s framework for the ethics of care and justice. 1 The results indicate that care-based ethical reasoning is deeply grounded in primary nursing practice with older patients. The named nurse develops a trusting relationship with her patient and takes responsibility for planning and implementing care and preparing the discharge process. Empathic understanding builds rapport between the primary nurse and her patients and their families, and makes caring a morally valid enterprise. Particularistic thinking plays a critical role in care planning and needs assessment, as the primary nurse gathers nuanced knowledge on her patient’s unique characteristics and situations. This contextual knowing empowers nurses to have input in clinical and ethical decision-making in the multi-professional context of rehabilitation. While physicians are legally accountable for decisions on discharge, primary nurses feel morally responsible for these decisions because they are answerable to their patients. The ethic of care forms both an attitude and a mode of ethical problem-solving in primary nursing. Its prescriptivity is not derived from rules, norms, or principles but from idiosyncratic care situations bound by patients’ particular identities, time, and place, and therefore it cannot be replaced by the ethic of justice. 2 The results are in line with a recent study showing that nurses favor relational ethics in clinical situations. 25
The results simultaneously show that the ethic of justice is of equal importance in contemporary primary nursing practices because they are framed and constrained by rules of care delivery. The primary nurse also has a prescribed duty to advocate for the patient’s rights and defend her concerns in multi-professional decision-making that in turn is guided by public standards for care delivery and leans on the principle of the equal treatment of citizens. The standards behind discharge decisions are justified by way of evidence-based knowledge and are agreed within the multi-professional team. However, the difficulty of this ethical conflict lies in adapting decisions to meet patients’ authentic needs. Frail patients are chronically in a vulnerable state and family members are concerned about their ability to cope. The ethical validity of decision-making is considered from both justice and care perspectives. The justice perspective evaluates on what grounds a decision is justified and whether official standards for the hospital and institutional care are upheld. Within the care perspective, it is evaluated as to what extent the decision may pose risk to the patients’ welfare; increase their burden, hurt, and suffering; and how these risks are successfully minimized. How the discharge process is finally worked out constitutes the ultimate evidence of ethical decision-making.
Results from this small-scale study are consistent with previous qualitative studies9,10 pointing out care and justice are integrated in nurses’ natural decision-making. Considerations of care and justice are often contradictory, but they can also support each other. The principles of justice need to be interpreted and implemented in idiosyncratic care situations yielding tailored solutions that accord to patients’ needs. The results also indicate that primary nursing as a model of care delivery enables nurses’ responsibility in decision-making that may relieve moral distress nurses experience due to hierarchical nurse–physician relationships. 26
The nature of ethical conflicts brought up in this study reflects a significant development trend in Western countries: aging population and diminishing economic resources. This trend is coupled with the contemporary rise of neo-liberalism and the new public management ideology that regards care as a commodity among others. Nurses are increasingly challenged to address social and cultural inequalities in their daily work, and this means that relational care- and social justice-based approaches need to be fused in the moral deliberations and actions of nurses. 27 It is important to include the social ethics perspective in the nurses’ ethics education to meet recent challenges. The ethics of care and justice need to be integrated into the complex decision-making practices of all healthcare professionals.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was conducted in Competent Workforce for the Future Project (303608) funded by the Strategic Research Council (SRC) at the Academy of Finland.