
Abstract
The Patients Changing Things Together (PATCHATT) programme supports individuals with a life-limiting illness to lead a change that matters to them. Individuals join a facilitated online peer support group to identify an issue they feel strongly about, plan for change and take action to bring that change about. The programme is developed and guided by a Programme Advisory Group with clinical and lay membership. This article charts the trialling of the patients changing thing together ethics pack, designed to support all members of the Programme Advisory Group in taking an equal role in ethical decision-making as they guide the programme's ongoing development. As a trial of its efficacy, the pack was used by the author to consider an ethical dilemma at the heart of the development of the Patients Changing Things Together programme, that is, is it ethical to offer a community palliative care programme which has the potential to bring participants harm as well as good? The author reports a strong ethical argument for offering this programme, while concluding the need for the Programme Advisory Group to make the final decision, using the Patients Changing Things Together ethics pack to consider the results of the evaluation of the programme's pilot. The article concludes that this pack provides an effective tool to guide ethical novices through the ethical complexities of developing a community-based palliative care intervention programme. It raises the issue that such inclusivity is achieved through a normative decision-making process which denies the fluidity and creativity which may inform the best ethical decision-making practice.
Introduction
There is an acknowledged need for innovation in palliative care. 1 The combination of an ageing global population and the development of new diseases such as COVID-19 renders current models of health care provision inadequate 2 to support individuals through the ‘total pain’ – the physical, mental, social and spiritual suffering – experienced by many at the end of life. 3 National Health Service (NHS) England's 4 Five-Year Forward View seeks to address this in part through building a social movement, shifting power to patients and citizens and improving health care capacity through community strength. The growth of patient and public involvement (PPI) in research and development projects exemplifies this mandate in action, with patients and the public working alongside clinicians and scientists to develop new health care approaches. However, research team membership brings particular challenges for individuals with a life-threatening illness. Despite the rhetoric of equal value and an asset-based view of patients as experts by experience, 5 the search for mode 1, scientific knowledge 6 remains privileged by research and development funding and hence activity. 7 The desire for full patient participation therefore often implies engagement in formal, lengthy research training programmes or academic qualifications, 8 excluding many palliative care patients interested in fulfilling such roles, due to complex health issues and decreased life expectancy. 9
This issue is pertinent to me in my role as a member of the Programme Advisory Group (PAG) developing the patients changing things together (PATCHATT) programme. Adults living with a life-limiting illness, supported through palliative care, often feel a sense of dislocation from their previous life and a diminishing sense of self. 10 Despite this, individuals often have a clear understanding of how their lives could be improved and what they still wish to achieve. The PATCHATT programme supports participants in leading a change that matters to them. Individuals join facilitated online peer support groups to identify an issue they feel strongly about, plan for change and take action to bring that change about.
Ethics within the PATCHATT programme
The PATCHATT programme has been designed by a PAG group comprising patients, carers, clinicians, academics and volunteers. As advised in the 2021 Medical Research Council/National Institute for Health Research (NIHR) framework, 11 its ongoing development and evaluation will continue to be guided by this group. PATCHATT is primarily a development programme rather than a research project, seeking to develop mode 2 knowledge to advance both conceptual understanding and practice in community-based palliative care. 6 There is therefore no requirement that patient, carer and volunteer PAG members have a detailed knowledge of the language and practices of research to enable them to contribute fully to the programme's ongoing development. However, the development process to date has raised various ethical issues. These have included the assurance of confidentiality, the provision of short-term support for change leadership which is then withdrawn, and the raising of participant expectations of change that may not be met. Imagining such issues will continue to arise as the programme expands, PAG members need a shared understanding of how to adopt a structured approach to ethical decision-making to ensure equality of voice and influence. The development of a tool, the PATCHATT Ethics Pack, seemed an appropriate way forward.
The PATCHATT Ethics Pack comprises a model and six stimulus cards, designed to give information and provoke deep reflection. It aims to enhance PAG members’ understanding of key foundations of ethical thinking, including moral positioning, normative ethical theories, principalism and structured approaches to ethical decision-making, implementation and evaluation. Published ethical thinking models provided a useful starting point for the pack's development. Park's work, 12 for example, highlights common stages in ethical thinking, namely, identifying the ethical problem, collecting information to help to develop alternative solutions, selecting and justification of the best way forward, developing an implementation plan and evaluating impact. The common identification of these stages as separate, linear, chronological steps 13 troubled me, however, as did the focus on process rather than on content. Following Park, 12 I wished to design a decision-making model which, while simplifying the reality of the messy process of ethical decision-making, nevertheless strongly supported iterative, cross-stage thinking. This aim was achieved through the development of the PATCHATT ethical decision-making model, shown in Figure 1.
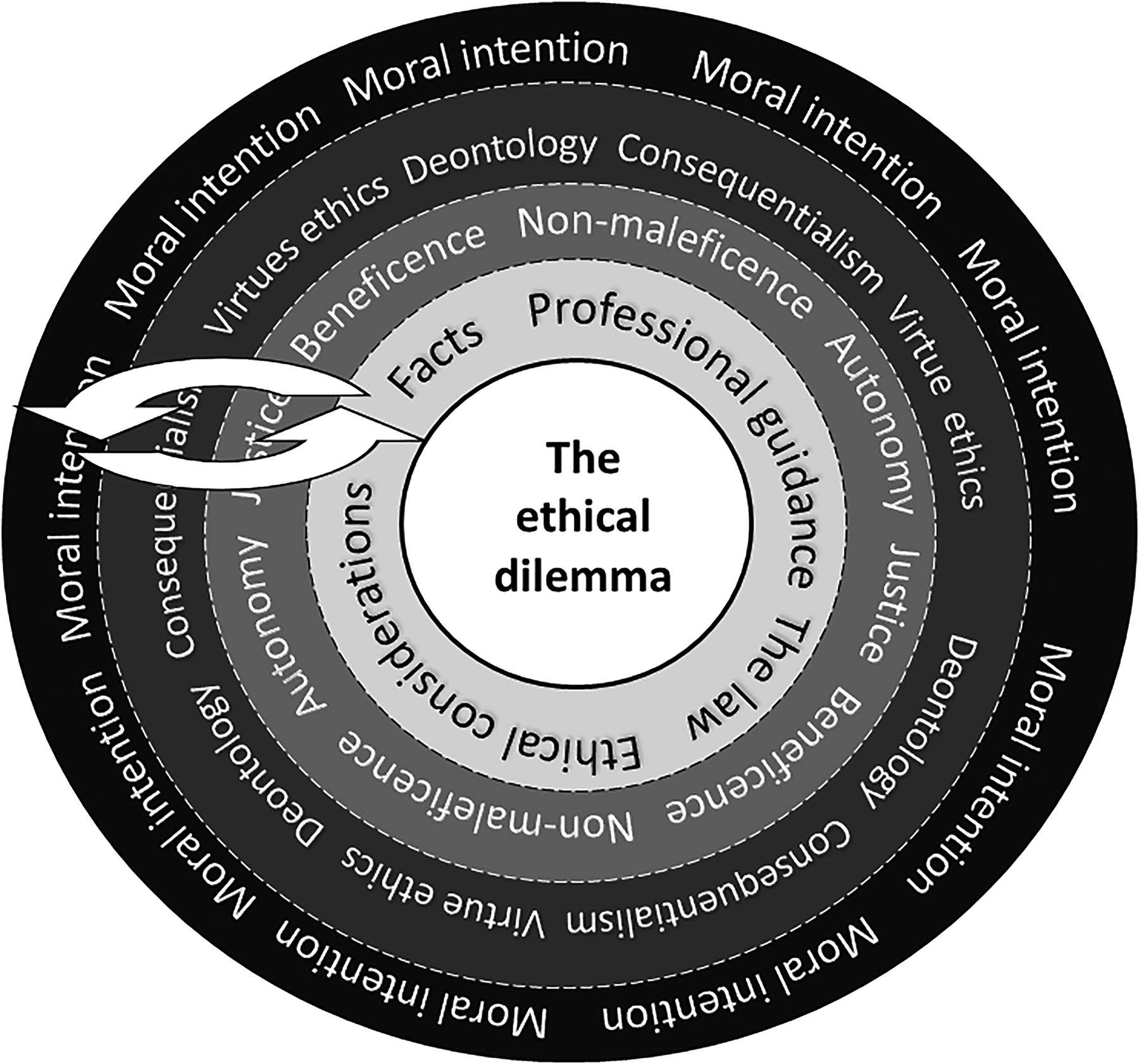
The Patients Changing Things Together (PATCHATT) ethical decision-making model (original figure by author).
The ethical dilemma sits as the centre of a series of concentric circles or wheel. The model invites users to start here and then move to the outside circle and progress inwards. In so doing, we should consider our moral intentions, drawing on normative ethical theories to inform our thinking, considering the relevance of principalism and adopting a structured approach to ethical decision-making based on facts, professional guidance, the law and ethical considerations pertaining to our dilemma. This structure suggests a formulaic approach to ethical decision-making which may rightly provoke scepticism. This is not the intention behind the development of the PATCHATT Ethics Pack. Instead, although artificially divided into stages, I concur with Campbell and McCarthy 14 in promoting a highly flexible use of such models, with stages revisited and reconsidered as the ethical argument develops. In the PATCHATT model, the concentric circles, the two-headed arrows threaded through them and the dotted, permeable lines between them have been designed to suggest this flexibility. However, the normative thinking which influences the model remains to be defended. I would argue that the relative value of supporting lay PAG participants in engaging fully with some form of ethical debate trumps concerns over promoting restrictive thinking. Although this may well be the case in the early stages of using the cards, I would argue that more fluid approaches to particular ethical dilemmas can be adopted once the elements and processes of a catholic approach to ethical thinking are made available to all.
Trialling the PATCHATT ethics pack
I wanted to trial the PATCHATT Ethics Pack myself before offering it as a tool to other PAG members. I therefore used the cards to guide me through my own exploration of a fundamental ethical dilemma associated with the PATCHATT programme, that is, should palliative care patients be offered the opportunity to design and lead change? This may not seem a particularly controversial issue. The PATCHATT programme appears to be fulfilling an established need and to be arising from the desire to do well. An understating of the breadth of the moral domain 15 and Bowman's 16 injunction to focus on more mundane ethical issues within community palliative care encourage a deeper evaluation, however. Change leadership has potentially far-reaching consequences. A participant in the PATCHATT programme may decide to contact an estranged family member to seek resolution prior to the end of life or try to change how their carers treat them. Both actions may bring potentially difficult emotional and psychological labour for the participant, at a time when they are most vulnerable. Inevitably, in some cases, the desired change may not occur. Is it therefore ethical to offer a programme that may lead to such potential harm for its participants? The value of the PATCHATT Ethics Pack in helping me resolve this dilemma would be a good indication of its potential efficacy to fellow PAG members when facing both this and other ethical dilemmas in the course of their work in guiding the future development of the programme.
The PATCHATT ethical decision-making model summarises one approach to decision-making. The remaining six cards that make up the pack each support the user's exploration of one stage of the decision-making process.
Card 1 – Exploring moral intention
The first card in the PATCHATT Ethics Pack facilitates an exploration of moral intention. This card draws on Beekman and Brom's 17 argument that ethical tools should help participants voice their values and ideals. The partisan and assailable nature of our moral positioning need to be acknowledged prior to a structured investigation of our ethical issue, to ensure that challenges to our views are welcomed rather than feared (Figure 2).
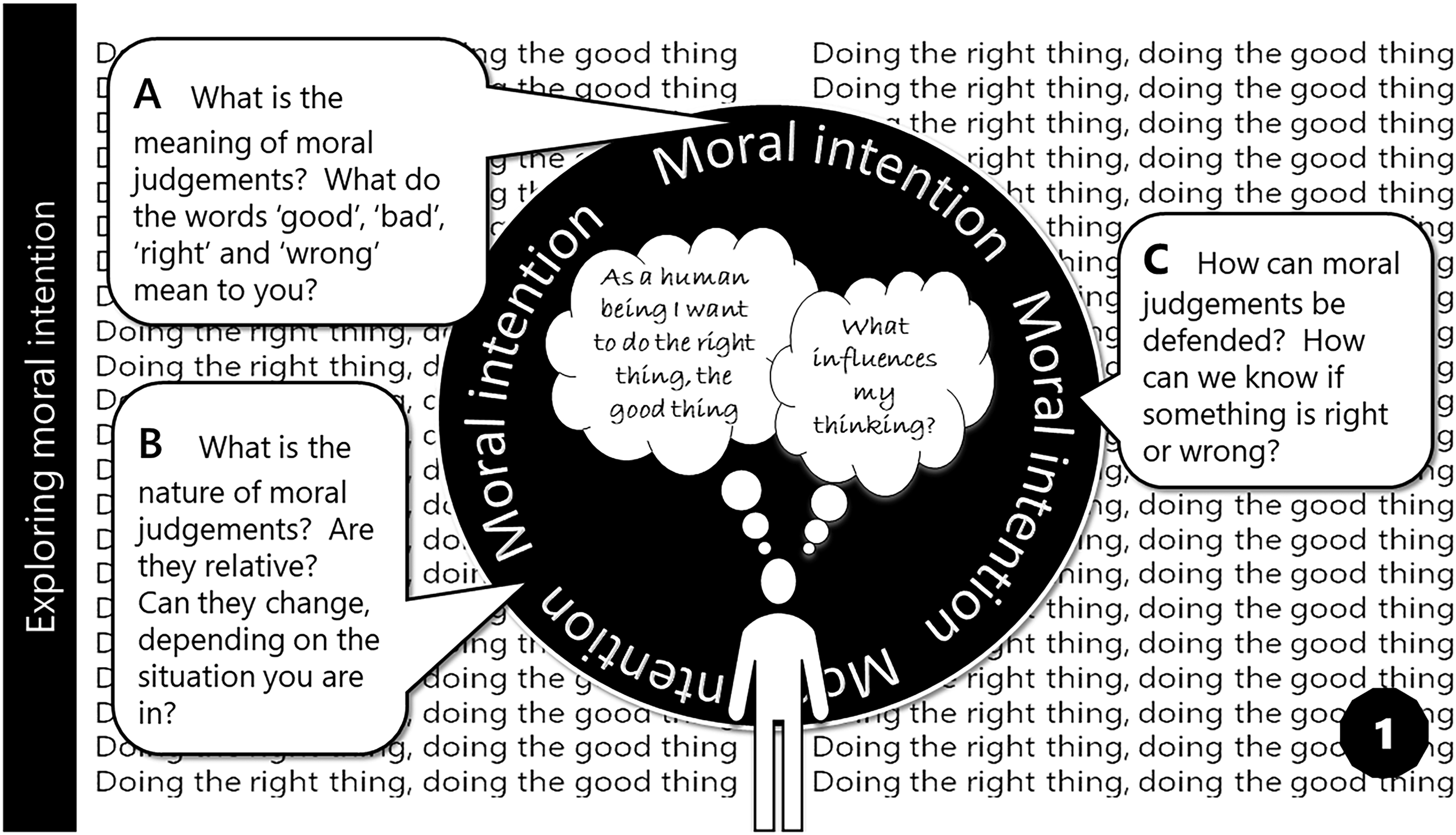
Card 1 – exploring moral intention (original figure by author).
Although sometimes challenged by experience, the basic human desire to do the right thing, the good thing forms the background to this card. Ayala 18 sees moral goodness as a biological attribute, with Pinker 19 viewing it as essential to human beings’ sense of worth. Often conflated, I differentiate between moral positioning, characterised by a desire to do good, arising from parenting, culture, society, moral standing and so on, and ethical positioning, arising from the consideration of principles which govern appropriate behaviour and help us to do the right thing, to do the good thing, in a given situation. The questions here are designed to provoke PAG members to consider the meaning of moral judgements they regularly make, what has shaped their moral positioning and how their moral intention might lead them to unfairly privilege certain ethical arguments.
The questions were useful in surfacing the origins of my own stance towards the PATCHATT programme. My moral intention is shaped by my catholic schooling, my need for approval and my desire to be seen as a kind, supportive person. I therefore see a good thing as something desirable which attracts approval, benefitting an individual or society. I see a right motive or action to be one that is just and fair. I acknowledge the relativity of my judgements, seeing my beliefs change according to circumstances. I wonder if I am drawn to develop the PATCHATT programme not through empathy or altruism but from a need for personal significance. A heightened awareness of this possibility hopefully enables me to guard against unfairly privileging certain ethical arguments.
Card 2 – Clarifying the ethical dilemma
The second card in the pack is designed to support PAG members in clarifying the nature of the ethical dilemma which has obscured their view of the good and right thing. A question may arise, for example, over the criteria for joining the PATCHATT programme – who ‘counts’ as a patient living with a life-limiting illness? Is it our judgement to make or that of the potential participant? Is this an ethical dilemma around the right to define an individual's status or an attempt to pragmatically limit programme numbers? (Figure 3)
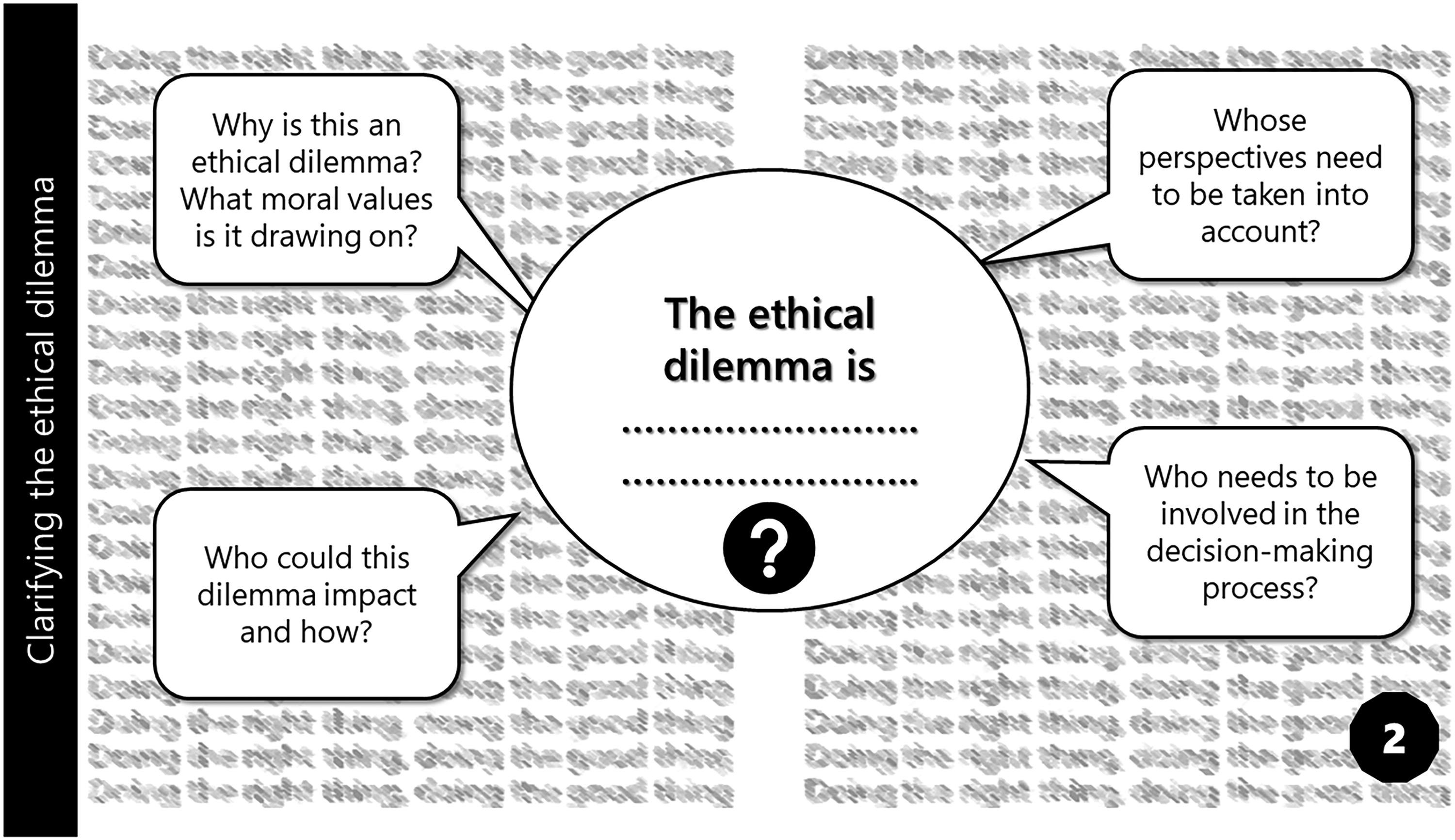
Card 2 – Clarifying the ethical dilemma (original figure by author).
My current dilemma is, is it ethical to develop and offer a PATCHATT programme to those with a life-limiting illness? There could be a gut reaction to this question, seen as legitimately occurring in the ‘Assess’ stage of Manson et als.’ 20 ethical decision-making model. Although potentially valid, I would argue such a decision is best reached through a supportive, structured approach to ethical decision-making. Card 3 begins this process.
Card 3 – Drawing on normative ethical theories
Normative ethical theories ‘formulate and defend a system of fundamental moral principles and rules that determine which actions are right and which are wrong’, 21 (p. 9) a useful approach to identifying moral challenges and developing sound arguments and conclusions. 22 The third card supports an introduction to such theories (Figure 4).
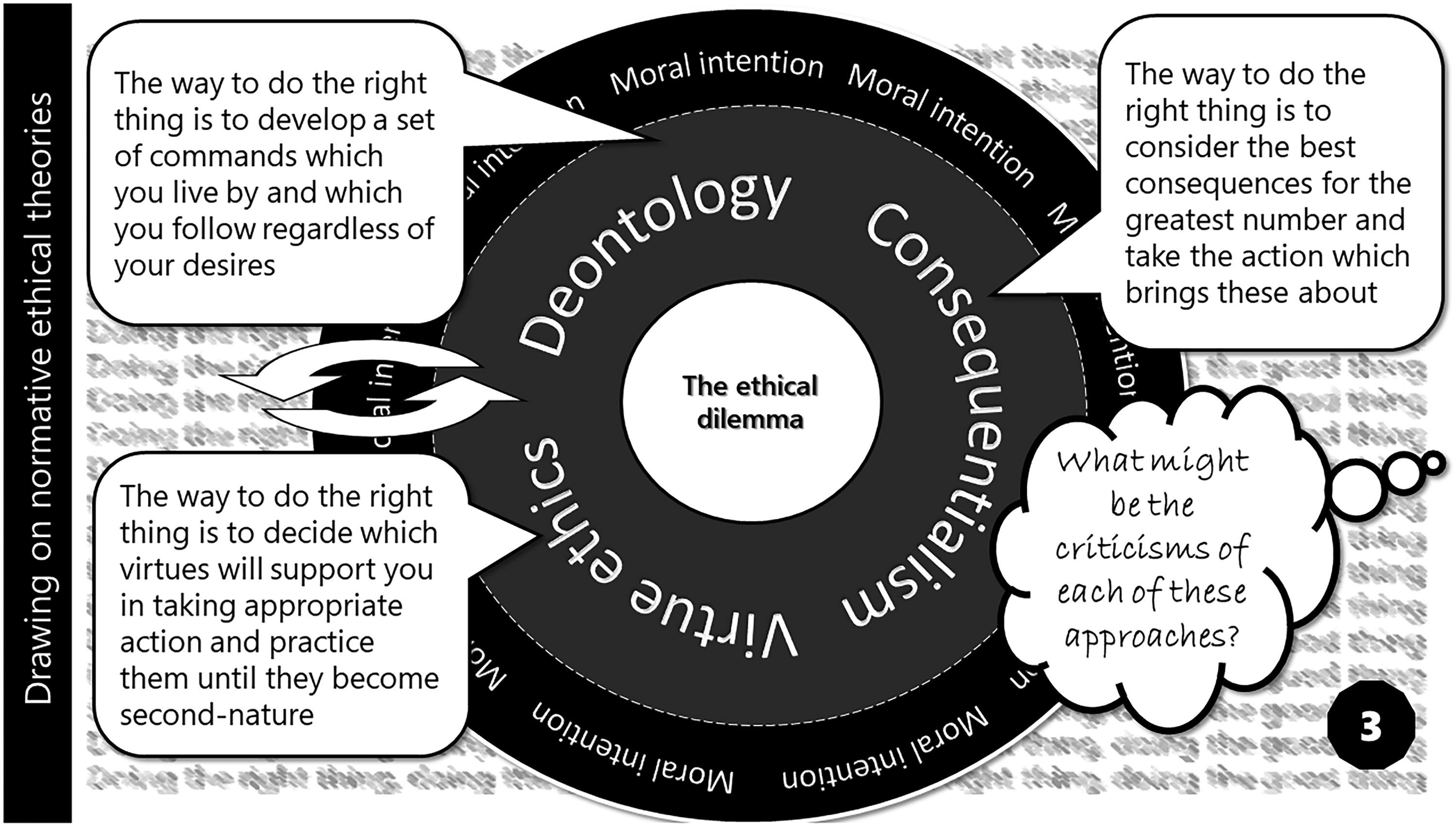
Card 3 – Drawing on normative ethical theories (original figure by author).
Focusing on three normative theories, the card summarises the essence of each approach through simple statements. It then invites PAG members to engage with a critique of each approach. In my example, considering the rectitude of offering the PATCHATT programme, a deontologist argument would suggest that, given the intrinsic value of all human beings and the irrelevance of consequences of actions, a programme focusing on promoting individual fulfilment must be a good thing. Consequentialism challenges this conclusion, however, suggesting a calculation of consequences and a determination of the greater good to be a necessary process. Virtue ethics, focusing on the ‘character of the moral agent’, 23 (p. 292) rather than the action, promote an analysis of the virtues or vices which compel us to offer the PATCHATT project, fuelling concerns over motivations. The range of moral perspectives provided by normative ethical theory influenced the development of Beauchamp and Childress's 21 principalism, a structure for ethical reasoning in practice 24 and the focus of the fourth card in the PATCHATT Ethics Pack.
Card 4 – Exploring principalism
Concentrated around the four principles of autonomy, beneficence, non-maleficence, and justice, principalism was designed to offer an approach to ethical thinking compatible with most individual, societal and religious belief systems. Card 4 summarises each core precept, supporting PAG members’ understanding of their relevance to ethical decision-making practice (Figure 5).
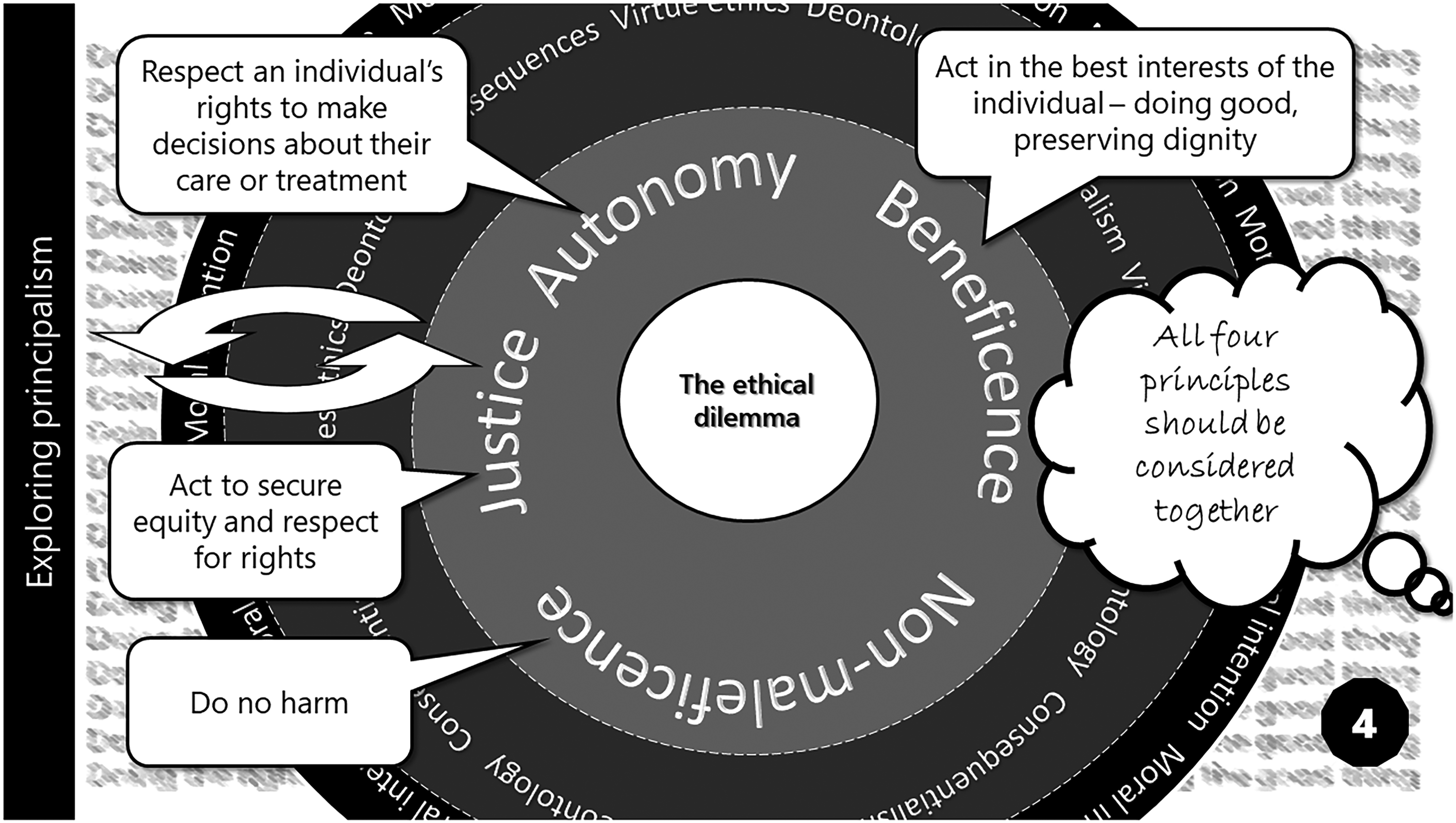
Card 4 – Exploring principalism (original figure by author).
It is not envisaged that principalism will be applied at this stage to the specific ethical dilemmas faced by PAG members. The four principles will instead be used as part of the structured approach to ethical decision-making stimulated by card 5 below. I will therefore trial them by applying them to my own dilemma at that point.
Card 5 – A structured approach to ethical decision-making
My ethical decision-making process usually combines logical argument with gut instinct. This card both systemises this process and adds to it, offering a recognised structured approach, drawing upon facts, professional guidance, the law and principalism to address an ethical dilemma (Figure 6).
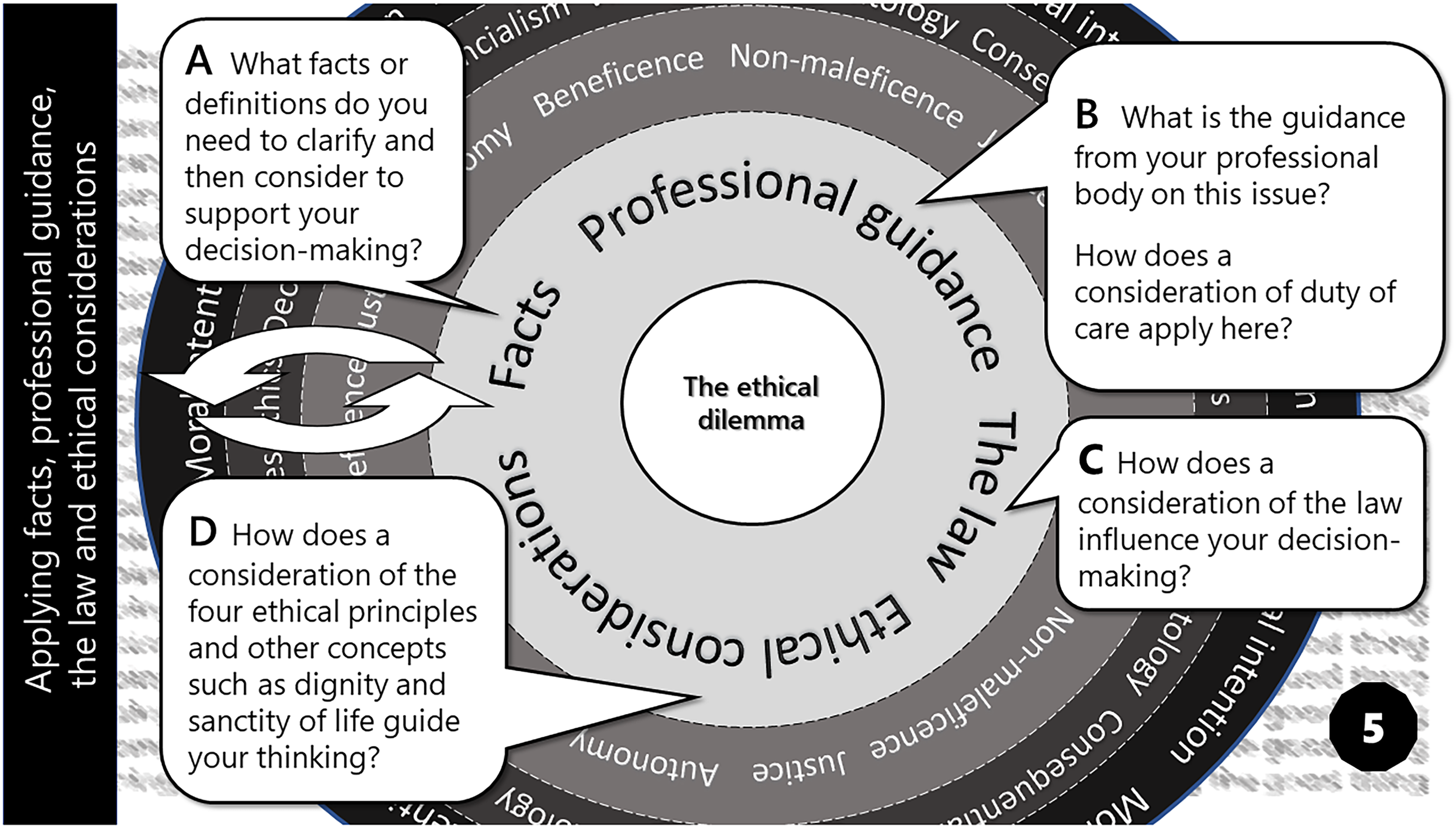
Card 5 – A structured approach to ethical decision-making (original figure by author).
Facts
PATCHATT participants will be individuals experiencing serious health-related suffering, 2 associated with the need for palliative care, who wish to be supported to bring about change. Linked to user-led research, which offers patients the opportunity to improve their own lives and contribute to social and political change, 25 PATCHATT prioritises patients’ agendas and values-led action above the development of generalisable knowledge.
Professional guidance
Research principles have some relevance to the PATCHATT programme. The Economic and Social Research Council 26 prioritises maximising research benefit while minimising potential harm, a priority endorsed by the General Medical Council (GMC).27,28 The British Psychological Society Code of Human Research Ethics 29 prioritises respect for the rights and dignity of participants, an emphasis mirrored by the GMC, 30 which highlights supporting patients’ self-care, listening to and responding to their concerns and preferences as good medical practice. The focus on a patient-partnership approach is particularly helpful to our thinking on the PAG, as is the GMC research principles’ 28 underlining the need to provide clear information to enable informed consent, a discrimination-free approach and respect for patient diversity.
The law
While legality does not assure morality, the UK policy framework for health and social care research, produced by the NHS and four health departments, 31 enumerates principles and responsibilities that take account of relevant UK legislation. Although generally covered by the professional guidance referenced above, the priority of individual safety over the interests of science and society is an important addition.
Ethical considerations
The PATCHATT ethical decision-making model (Figure 1) uses Beauchamp and Childress's
21
four principles as a structuring device for ethical decision-making.
Respect for autonomy
I take autonomy to mean self-governance, the ability to make meaningful, belief-based, coercion-free choices. To respect someone's autonomy is to acknowledge individuals have the capacity to determine their destiny. Violating autonomy treats individuals as means to an end, as a way of achieving one's own goals.
21
On receiving an invitation to join a PATCHATT group, an individual would decide whether to participate or not. The autonomous choice seems assured. However, many potential participants would learn of the programme through their clinical palliative care provider. Those not wishing to join may be concerned about possible offence and implications for other treatment offers,
32
thus compromising free choice. Beauchamp and Childress's
21
view of information and understanding as key to autonomous action suggest written confirmation of freedom of choice, plus the opportunity to discuss issues, may reassure potential participants and support autonomous decision-making.
Positioning participants as agential leaders of change challenges traditional conceptualisations of patients as ‘objects’ of medical gaze. 33 (p.137). Within PATCHATT, patients are experts by experience, 5 sharing a common experience of a life-limiting illness and palliative care. However, the relational and intellectual power which positions patients as inferior can be deeply entrenched. 34 Overt addressing of power differentials would allow all participants to share and challenge views confidently 35 in an atmosphere of mutual respect and reciprocity.
A key strategy within PATCHATT is participant choice of change-making agenda. I concur with de Raeve's 36 view that using palliative care patients to support a pre-set agenda violates their autonomy, challenging the deontological categorical imperative that humans be acknowledged as intrinsically valuable, rather than a means to an end. However, an alternative reading of this level of engagement and agenda control would find a challenge to autonomy. The principle that participants are both the architects and enablers of change requires high levels of participation. Participant choice of their level of engagement with a programme, held as a key principle in PPI, 37 is therefore constrained within PATCHATT. The desire to support autonomy may therefore imply the need for the PAG to amend the programme design post-piloting to include various participation routes, depending on participant choice.
Such a choice may change as illness progresses.
38
To preserve autonomy, any change in the level of participation should be participant-led, rather than initiated by the PAG as over-protective programme leaders, an issue recognised in Stevens et al.'s study.
39
Beneficence
At its simplest, beneficence means doing good . The obvious question raised is, good for whom? Beauchamp and Childress
21
describe beneficent actions as contributing to patients’ welfare, furthering their legitimate interests. The PATCHATT programme seeks to do good through offering participants the opportunity to create change, guided by their own moral intention. Numerous studies report patients’ enthusiasm to use their experience of illness and the health care system to contribute to service improvement.
34
The beneficence of the PATCHATT programme therefore seems assured. However, it could be argued that desired action does necessarily equate with sound action. We might engage in an activity which we afterwards regret, or which does us harm. Froggatt et al.'s
40
study notes a range of positive patient impacts from PPI, including gaining new knowledge and confidence and appreciating making a difference, while Cotterell et al.'s
41
participants felt supported in living well and reaching the state of human flourishing, a feeling McArthur
42
attributes to helping shape the world.
As I have argued elsewhere, PPI also offers participants the opportunity to connect with others with a terminal illness, giving a sense of belonging, understanding and comfort. 43 Individuals can choose to embrace the changed identity their illness brings, through positively interacting with others in a similar position. 44 Negative impacts of PPI are also reported, however. These include the physical and emotional nature of the work and difficulties in identifying impact, 34 sometimes leading to in-project attrition. 45 The intersect between autonomy and beneficence becomes vital here. Presented with appropriate facts, PATCHATT participants can exercise their autonomy in making the choice that benefits them.
The patient's best interest is only one aspect of beneficence. Potential benefits of the PATCHATT programme for society also need to be considered. It has been argued, for example, that patient involvement improves the relevance and implementation of research,
45
with the NIHR
46
determining that all service-users should be aware of and involved in research by 2025. The PATCHATT programme could have a key role to play here. Indeed, the 2016 Care Quality Commission,
47
building on a 2013 NESTA report,
48
recommends the development of the voluntary sector, community and peer support programmes to improve autonomy and reduce NHS costs. However, I am persuaded by the Declaration of Helsinki principle that considerations of participants’ well-being trump the interests of science or society
49
and so reassert this as my main consideration.
Non-maleficence
The principle of non-maleficence, the imperative to not harm, could be met by deciding not to offer the PATCHATT programme. If the programme is not offered, it cannot harm. However, maleficence must be balanced with beneficence, the imperative to do good.
21
Having argued above that the PATCHATT programme will do good, the argument for its non-maleficence must be made.
An important issue is, who defines harm, patient or health care professional? Evidence of differing clinician and patient understanding of the patient experience,
50
coupled with an intention to promote participant agency, suggests prospective PATCHATT participants should make their own decisions. However, this does not negate the PAG's responsibility to develop robust ethical standards to mitigate unintentional harm.
34
The innovative character of the PATCHATT programme means the nature of such unintentional harm is unknown. However, PPI evidence shows patients can suffer lack of worth,
41
excessive emotional labour
40
and stress from inappropriate power differentials.
35
The Economic and Social Research Council's
51
recognition that it is neither possible nor desirable to avoid all risk is helpful here. The principle of non-maleficence could be met by acknowledging and sharing potential risks within the programme and developing mediating strategies.
Justice
The principle of justice refers to fairness and is also linked to entitlement; something is just when it is fair and deserved.
21
The issue of fair access to the PATCHATT programme is a dominant concern. The programme has been specifically designed for those with a life-limiting illness, overcoming the usual issue of PPI access for this vulnerable group. However, I am aware of the challenges in marketing the programme to diverse populations, both in relation to socioeconomic and illness groups and geographically. Failure to overcome this issue could deny the programme's benefits to potential participants.
Card 6 – Deciding, implementing and evaluating
The final card in the PATCHATT Ethics Pack prompts a review of thinking and a decision on the ethical dilemma under consideration. It looks forward to the implementation and evaluation of the action decided upon. Here, in theory, at least, the right and good thing to do have become clear again (Figure 7).
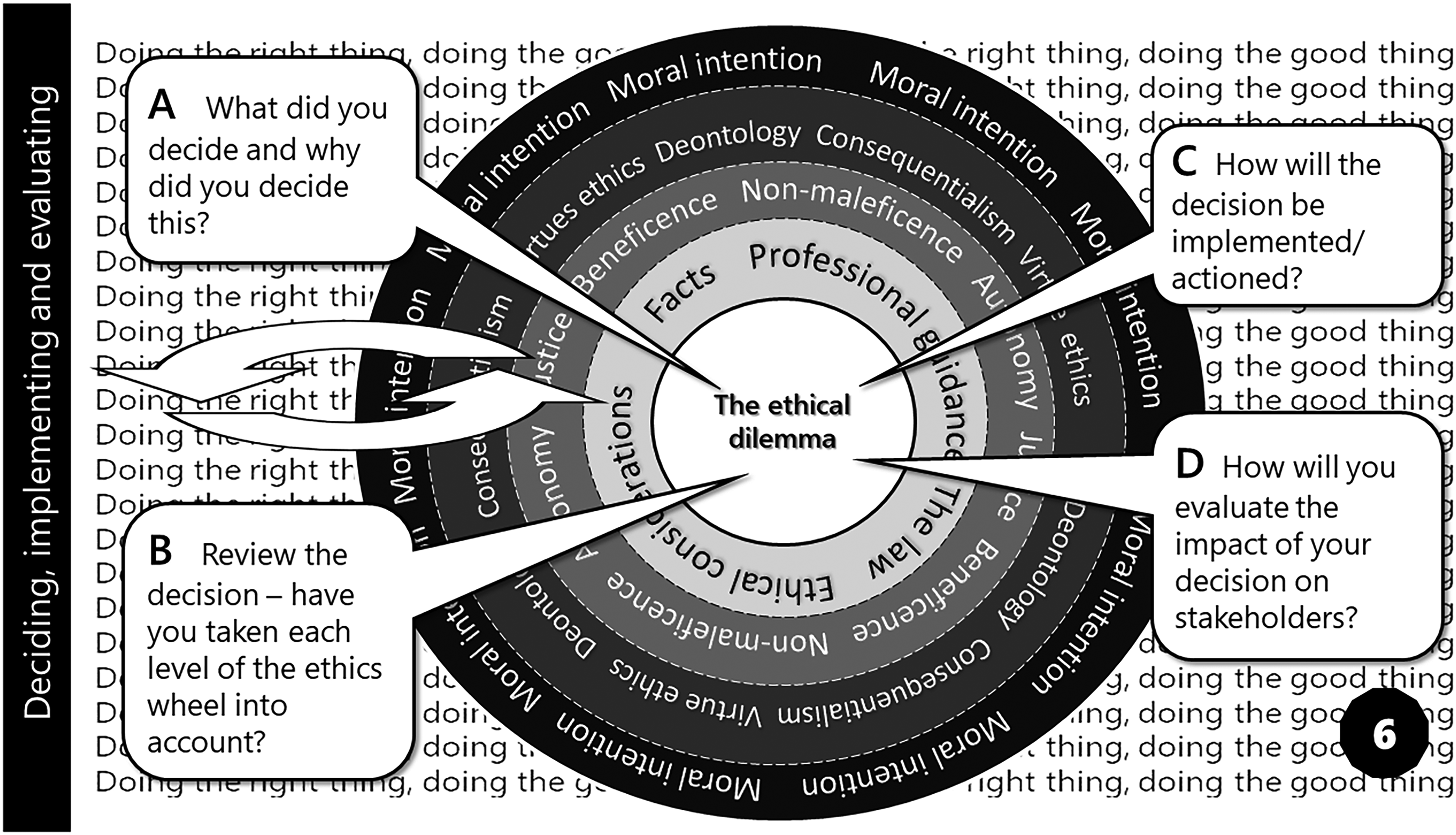
Card 6 – Deciding, implementing and evaluating (original figure by author).
Despite considering questions A and B on this card, clarity around my own ethical dilemma remains elusive. Evaluating the arguments for offering the PATCHATT programme shows the potential for clear benefits and likewise the potential for harm. Given the assessment of benefits and harms when not made by individuals themselves is notoriously difficult, 14 a focus on autonomous choice would overcome the stalemate. If the programme is not offered, the potential benefits would not be available. If individuals have free choice in whether to join the programme, they can undertake a risk assessment based on their unique circumstances and make an appropriate decision.
A consideration of the concept of dignity lends weight to this argument. Variously defined, I use dignity to mean a sense of self-worth and self-respect. The PATCHATT programme seeks to support individual dignity by enabling participants to retain a sense of normalcy and control and to leave a legacy, aligning with Chochinov et al.'s model. 52 Thus participants will be able to express their ‘dignity in action,’ 53 having control of their own narrative through values-based change-making, while also making a difference to the lives of others. 35
In terms of my own ethical dilemma, I believe there to be a strong ethical argument to move forward with the piloting of the PATCHATT programme. The PATCHATT Ethics Pack has been useful in both providing insights into and extending my restricted ways of thinking. Ethical safeguards need to be put in place, however. The PAG will therefore be called upon to make the final decision on the ethical rectitude of offering the PATCHATT programme, using the PATCHATT Ethics Pack to consider the results of the pilot's evaluation.
Conclusions
Within the PATCHATT programme, individuals with a life-limiting illness are conceptualised as assets, leaders of change who will enhance not only their own sense of agency and quality of life but also that of their fellow participants, through peer support and the potential for service-level change. The ethical complexity of establishing such an innovative approach to palliative care is rehearsed above, hence the need for full engagement with all members of the PAG in all decisions. From my trial of the PATCHATT ethics pack, it appears to provide tools that will support PAG member autonomy in ethical decision-making, through levelling understanding of ethical issues 54 and thus ensuring informed, inclusive ethical debate. While some research and development teams have similar inclusive aims, the length of research training required can exclude patients with a life-limiting illness from a full team membership. The PATCHATT cards appear to promote an inclusive, accessible yet thorough approach to ethical decision-making, without this need for lengthy training. This inclusivity is undoubtedly achieved by providing a less than ideal, normative approach to ethical decision-making. However, the formulaic process, clearly defined in terms of steps in the PATCHATT Ethics Pack, promotes the broad engagement needed to develop innovative community-based palliative care practice, albeit at the expense of the fluidity and creativity which may inform the best ethical decision-making.
Footnotes
Acknowledgements
I would like to thank Dr Samantha Lund, Medical Director, Royal Trinity Hospice, London, UK, for her inspirational lectures which sparked both my interest in and understanding of medical ethics.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.