
Abstract
Cannabis is commonly characterized as the most normalized illicit drug. However, it remains a prohibited substance in most parts of the world, including Europe, and users can still be subject to stigmatization. The objective of this study is to assess to what extent and how cannabis users in different countries with different cannabis policies perceive, experience and respond to stigmatization. We conducted a survey in the Dutch coffeeshops among 1225 last year cannabis users from seven European countries, with national cannabis policies ranging from relatively liberal to punitive. Three dimensions of cannabis-related stigma were investigated (discrimination, perceived devaluation and alienation) and a sum score was used to reflect the general level of stigmatization. Perceived devaluation was the highest-scoring dimension of stigma and discrimination the lowest-scoring. The general level of stigmatization was lowest in the Netherlands and highest in Greece. This indicates that punitive cannabis policy is associated with stigma and liberal cannabis policy is associated with de-stigmatization. Besides country, daily cannabis use was also found to be a significant predictor of stigma, but gender, age, household type and employment status were not.
Introduction
For many decades, cannabis use has been associated with stigma (Becker, 1963; Erickson, 1976; Erickson and Goodstadt, 1979; Grinspoon and Bakalar, 1995; Kaplan, 1982). This changed from the mid-1990s onwards, with the introduction of the normalization thesis in social drug research. The normalization thesis suggests that recreational drug use has been de-stigmatized and is increasingly socially and culturally accepted by many members of the non-drug-using population and culturally embedded in wider society (Measham et al., 1994; Parker et al., 1998). A fundamental feature of normalization is that stigmatized or deviant individuals or groups become included in many aspects of everyday life, as their identities or behaviour become increasingly accommodated (Parker, 2005; Sandberg, 2012). Among all illicit drugs, cannabis has been described as the most normalized in various countries (Korf, 2006; Lee and Kirkpatrick, 2005; Osborne and Fogel, 2007; Parker et al., 1995; Sznitman et al., 2013).
Notwithstanding the ongoing discourse over cannabis normalization, it should not be neglected that normalization has always coexisted with cannabis prohibition, as cannabis remains illegal in most jurisdictions. Since the development of the normalization thesis, considerable attention has been paid to studying the relationship between cannabis-related stigma and normalization (Asbridge et al., 2016; Duff and Erickson, 2014; Sandberg, 2012; Hathaway, 2004; Hathaway et al., 2011; Measham and Shiner, 2009; Shildrick, 2002; Williams, 2016). Scholars have stated that cannabis use continues to be viewed as an aberrant activity, and that cannabis users still experience stigma (Erving, 2016; Hathaway et al., 2011; Reilly et al., 1998). Prohibitionist policies and the criminalization of cannabis places the users in a situation of deviance and exclusion (Suissa, 2001), with cannabis users experiencing fear of shame and status loss and internalizing guilt and discomfort because of perceived social disapproval of their usage (Hathaway et al., 2011). However, not all drug users experience stigma or not to the same degree and therefore are not all are equally stigmatized (Ahern et al., 2007). Similarly, cannabis users do not constitute a homogeneous category: not all the cannabis users experience stigma to the same degree and not all cannabis users are equally stigmatized (Duff et al., 2012; Liebregts, 2015; Miles, 2014).
Firstly, national cannabis policies are not equally prohibitive across the globe. Whereas an increasing number of countries have decriminalized cannabis, and Uruguay, Canada and a growing number of US states have even legalized it, many other countries persist in a prohibitionist policy (Decorte et al., 2020). Even within the EU with its open borders, cannabis legislation and enforcement practices show significant cross-national differences, ranging from relatively liberal to punitive (EMCDDA, 2017a). Therefore, differences in cannabis policies could play a role in the stigmatization of cannabis users.
Secondly, within and across countries sociodemographic characteristics may play a role in cannabis-related stigma. People’s actions are shaped by subjective awareness of gender positioning and by the way gender structures their social, cultural and political milieu (Campbell and Herzberg, 2017). Literature suggests that drug use is gendered in terms of subjective experiences (Measham, 2002). The use of cannabis by women is still perceived as more rebellious and is often met with disapproval reflecting cultural assumptions about deviant behaviour (Hathaway et al., 2016). Also, it has been noted that stigma and identity are differentiated by the socioeconomic status of the user, such as having a job or being unemployed (Bancroft, 2009; Seddon, 2005). Furthermore, the normalization thesis links drug-using behaviours to ageing and to maturation, with transitions in type of household (from living with parents to having your own apartment) and from student to employed (Aldridge et al., 2011; Duff et al., 2012; Lau et al., 2015).
Thirdly, cannabis-related stigma is often associated with patterns of cannabis use and particularly with frequency of cannabis use. Prior research suggests that high-use respondents take more risks and may experience stigma differently than less committed users (Hathaway, 2004; Kolar et al., 2018). Therefore, it can be hypothesized that frequent (for example daily) users experience more stigma than less frequent users. Alternatively, because, for daily users, cannabis is more likely to be part of their self-identity (Blevins et al., 2018; Liebregts et al., 2015), it could be argued that they feel and express a certain pride or consciousness that makes them less sensitive towards internalizing stigma.
Aim
The aim of this study is to assess to what extent and how cannabis users in different countries with different cannabis policies perceive, experience and respond to stigmatization. We conducted a survey among current cannabis users from seven European countries, with national cannabis policies ranging from relatively liberal to more punitive (see below). We hypothesize that a strict cannabis policy contributes to stigma, whereas liberal cannabis policy contributes to de-stigmatization and normalization.
Alternatively, the literature suggests that normalization is a societal process that is taking place across the western world (Pennay and Measham, 2016), so there might be not so much difference in stigmatization between countries with different drug policies. This would mean that the prevalence of cannabis-related stigma is largely similar across countries, and that differences in the stigmatization of cannabis users show similar patterns, which are associated with sociodemographic characteristics (gender, age, type of household, employment status) and/or frequency of cannabis use.
Theoretical framework: Deviance, stigma, discrimination, alienation and devaluation
When assessing cannabis-related stigma cross-nationally, it is important to define stigmatization and to specify how it is measured. Conceptually, stigma is strongly interlinked with deviance and labelling. In sociological theory, the concept of deviance can be traced back to Durkheim (1897), who argued that there can be no ‘normal’ in the absence of ‘abnormal’ or ‘deviant’. In the field of criminology, Becker (1963) introduced labelling theory as an approach to understanding deviant and criminal behaviour, and conceptualized cannabis use as a form of deviant behaviour. Labelling theory builds from the symbolic interactionist tenet that people define and construct their identities from society’s perceptions of them (Shulman, 2004). Once individuals have been labelled or defined as deviants, they often face new problems that stem from the reactions of self and others to the negative stereotypes (stigma) that are attached to the deviant label (Becker, 1963; Lemert, 1967). Goffman (1963) used the term ‘stigma’ to explain labelling, and defined stigmatization as a process that occurs through the social construction of identity whereby those who do not conform to being ‘normal’ are subject to the judgement of others. It occurs when an individual has an undesirable characteristic that is contrary to a societal norm or a shared belief regarding how individuals should behave (Stafford and Scott, 1986). Stigma is therefore dependent on the relationship between the specific discrediting attribute and the specific social context (Major and O’Brien, 2004).
Stigma may be divided into public stigma and self-stigma (Corrigan, 2004). Public stigma includes the negative beliefs individuals in society have about individuals from stigmatized groups (Corrigan and Watson, 2002). Self-stigma reflects the social and psychological impact of stigmatization (Bos et al., 2013). It refers to the internalization of negative stereotypes, discrimination and devaluation by others (Corrigan and Watson, 2002; Pattyn et al., 2014). Furthermore, self-stigma can be differentiated from perceived stigma, because ‘a person can be aware of such stereotypes without concurring with them’ (Pattyn et al., 2014: 232). Therefore, self-stigma refers to the self-adoption of a prevalent attitude or stereotype, whereas perceived stigma refers only to an individual’s awareness of such attitudes (Guarneri et al., 2019; Livingston and Boyd, 2010; Pattyn et al., 2014).
In this study we choose a user perspective and focus on perceived stigma and self-stigma, rather than on public stigma. More specifically, we investigate three dimensions of stigma experienced by illicit drug users: discrimination, perceived devaluation, and alienation (Ahern et al., 2007). Drug use discrimination can be defined as experiences of rejection attributed to drug use (Ahern et al., 2007; Krieger, 1999, Link et al., 1997; Link and Phelan, 2001). Perceived devaluation is a facet of perceived stigma and occurs when drug users believe that most people in the general public endorse common negative stereotypes about them (Ahern et al., 2007; Link et al., 1997). Alienation refers to the internalization of the views expressed in those stereotypes that drug users are marginal members of society (Ritsher et al., 2003).
Seven European countries with different cannabis policies
In the European Union, there is no harmonized European drug law, and there is little harmonization among the EU Member States in the laws penalizing unauthorized cannabis use (EMCDDA, 2017a). Significant differences remain between national drug policies in the EU. EU Member States largely retain their individual freedom and authority to decide on cannabis legislation and cannabis policy in their jurisdiction. The result is a variety of approaches within the EU, within a wide spectrum from liberal to punitive. In their national drug law, some countries treat all illicit drugs the same, others have two or more schedules and commonly define cannabis offences as a less serious legal matter. This variety of legislation and procedures within the EU reflects both the requirements as suggested by the UN Conventions and the ‘room for maneuver’ at Member State level (Ballotta et al., 2008).
Within the EU there are major differences not only in cannabis legislation (‘law in the books’) but also in law enforcement practices (‘law in action’). For example, regarding the supply of cannabis, a recent study reported great variation across EU countries in sentencing practices. According to a survey among national experts, expected median sentences for the supply of 1 kg of cannabis resin varied within the EU from 0 to 10 years, and from 0 to 12 years in the case of 10 kg. Expected median sentences were lowest in the Netherlands and highest in Greece, while a country such as Germany took an intermediate position (EMCDDA, 2017b). Together, the seven countries selected for our study represent the maximum variation in national cannabis policy within Europe. In terms of national cannabis policy (‘law in the books’ as well as ‘law in action’), variation refers to: the scheduling of cannabis (whether or not in a category separate from ‘hard drugs’); the legal status of cannabis use and possession for personal use; sentencing practices for dealing cannabis (see Table 1).
Overview of cannabis policy in the seven countries of study.
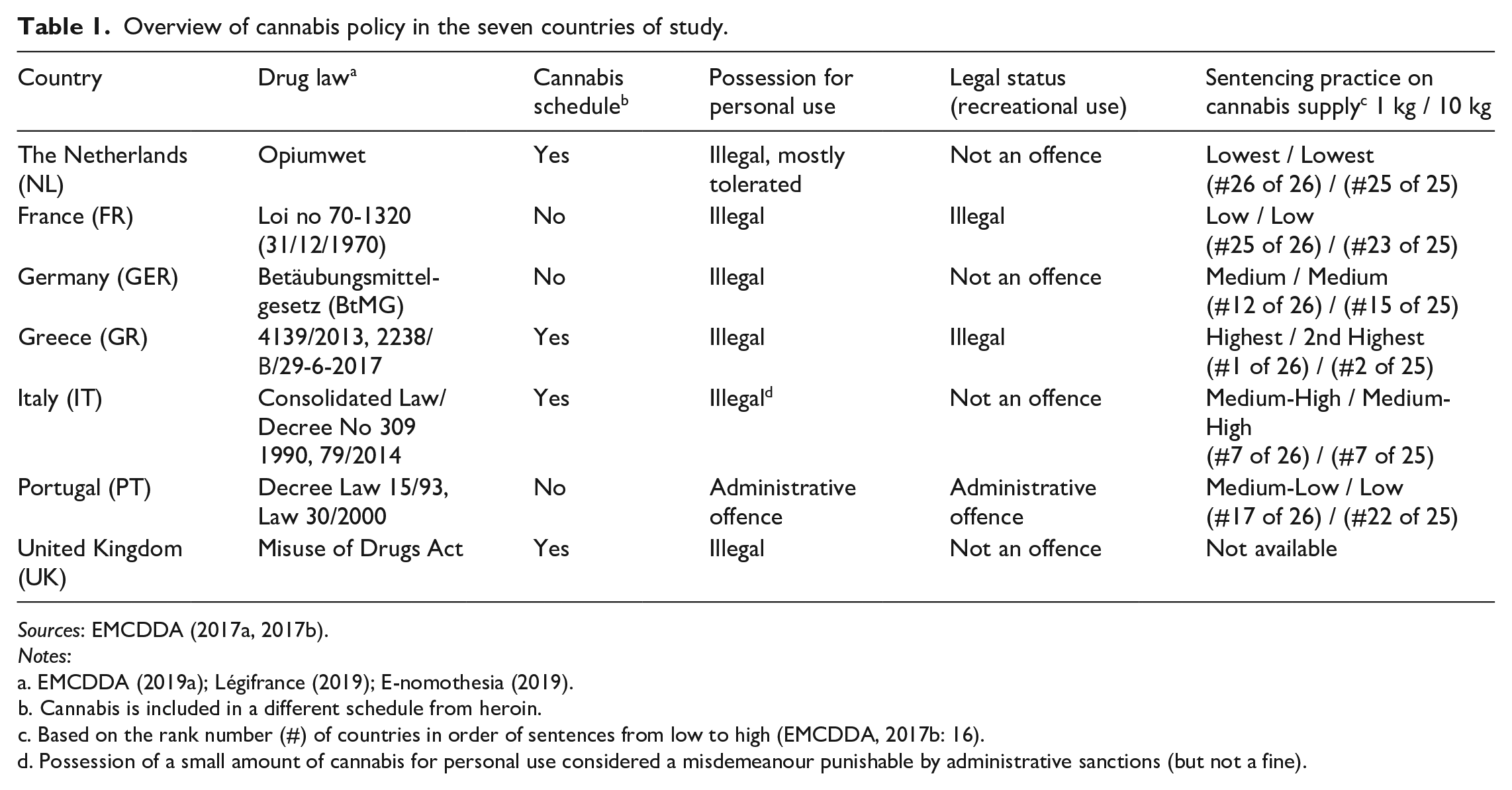
Sources: EMCDDA (2017a, 2017b).
Notes:
Cannabis is included in a different schedule from heroin.
Based on the rank number (#) of countries in order of sentences from low to high (EMCDDA, 2017b: 16).
Possession of a small amount of cannabis for personal use considered a misdemeanour punishable by administrative sanctions (but not a fine).
On a continuum from liberal to punitive, we placed the Netherlands on the liberal side and Greece on the punitive side. In the Netherlands, cannabis policy can be characterized as the most liberal at the consumer level in the EU. Although cannabis is officially an illicit drug, there are hundreds of so-called coffeeshops, that is, café-like settings, where adults (18 years or older) can buy and use cannabis under strict conditions (Van Ooyen-Houben and Kleemans, 2016). Portugal, which introduced a policy of decriminalization from 2000, is probably the country with the next most liberal cannabis policy. At the other end of the continuum, Greece has the most punitive cannabis policy in our study. Germany and Italy appear to take an intermediate position, and cannabis policy in France and the UK can be characterized as closer to the punitive end of the continuum.
Methods
Participants and procedures
In the period February–October 2019, we conducted a survey among a convenience sample of 1225 last year cannabis users aged 18–40 years and living in one of the seven countries in this study. Participants could be either Dutch, or tourists in the Netherlands, or people who had recently moved to the Netherlands (within two weeks prior to participation in the survey). Participants were recruited and interviewed inside or in the vicinity of coffeeshops (that is, close to the entrance) in the Netherlands, mostly in Amsterdam (41/46 coffeeshops). Coffeeshops attract not only domestic customers but also tourists from abroad who buy and use cannabis during their stay in the Netherlands, and in many cases also use cannabis in their home country (Van Ooyen-Houben et al., 2014). Although, according to the official guidelines, access to coffeeshops should be restricted to residents of the Netherlands, it is at the discretion of the local authorities to decide whether this criterion is applicable to the coffeeshops in their community, and most communities (including Amsterdam) do not implement that criterion (Korf, 2020). Therefore, coffeeshops offer a unique opportunity to find current drug users from many different countries (Korf et al., 2016).
Although the age range of visitors in Dutch coffeeshops is wide (18 to 65+ years), a large proportion of coffeeshop visitors are under 30 (Nabben et al., 2016; Van Ooyen-Hoube et al., 2014). To ascertain variation in age, we aimed at 40 percent of respondents in the age group 30–40 years. To ensure gender diversity, female coffeeshop visitors were purposely oversampled to make up about one-third of the sample. Taking into account the representation of country of residence in previous coffeeshop surveys (Korf et al., 2016), country population size and distance from the Netherlands, target numbers per country were set at around 200 respondents from each of France, Italy, Germany, the UK and the Netherlands, and half this number for Greece and Portugal.
Participants signed a consent form, which explained the purpose of the study and assured the respondents’ anonymity. Consent forms and questionnaires were available in seven languages. The fieldwork and interviews were conducted by the first author, together with research assistants who were fluent in the respondents’ language. Participants could choose between a print version or an online version.
Measures
To capture stigmatization, six items were derived from a study among illicit drug users by Ahern et al. (2007) and specified for cannabis: two items from the discrimination scale (‘Did some of your friends reject you because you use cannabis?’ and ‘Did some of your family reject you because you use cannabis?’), two items from the perceived devaluation scale (‘Most people believe that someone who uses cannabis is dangerous’ and ‘Most people think that someone who uses cannabis is unreliable’), and two items from the alienation scale (‘Do you sometimes avoid people because you think they might look down on you because you use cannabis?’ and ‘Do you feel you have to prove yourself because you use cannabis?’). The response options to these items were yes/agree [1] or no/disagree [0]. Exploratory factor analysis failed to recreate the three-factor structure found by Ahern and colleagues, probably because not all items from their study were included – we used only items that we assumed to be potentially applicable to cannabis users, and we left out items (for example, homelessness) that primarily relate to hard drugs and ‘problem users’. However, the six items did show a satisfactory internal consistency (Cronbach alpha = .584). We therefore used the sum score of these items [0–6] to reflect the level of stigmatization experienced by our respondents.
The background characteristics used in the analyses were country, gender, age, household, employment and daily cannabis use. The categories for gender were female, male or other, but ‘other’ was omitted from the statistical analyses owing to small numbers. With respect to household, three categories were recognized: (1) living alone, (2) living with a partner (with or without children) or with housemates, and (3) living with parents. Employment was also divided into three categories: (1) student (enrolled in school, college or university, with or without a side job), (2) employed (including self-employment), and (3) unemployed (neither student nor employed). In accordance with the European standard, daily or near daily (further on, daily) cannabis use was defined as the use of cannabis on 20 days or more in the previous 30 days (EMCDDA, 2019b). For Dutch respondents, this was the 30 days prior to the interview; for non-Dutch respondents, this was the 30 days in their home country before arrival in the Netherlands).
Analyses
First, associations between country and other background characteristics, individual item scores for discrimination, perceived devaluation and alienation, and a stigmatization sum score were assessed using χ2 tests for nominal and categorical measures and Anova for age and stigmatization sum score. Then six separate logistic regression models were calculated for individual items and a linear regression model for the stigmatization sum score. ‘Country’ was entered as an independent variable, and models were adjusted for age, gender, household type, employment status and daily cannabis use. For the regression analyses, country, gender, household and employment were recoded into dummy variables, and the first category (The Netherlands, female, living alone, and student, respectively) served as the reference group.
Findings
Table 2 depicts the sociodemographic and cannabis use characteristics of the total sample and by country. In accordance with the selection criteria, close to one-third of the total sample were female participants, two-thirds were male, and a small percentage defined themselves as ‘other’. As targeted, the age of participants ranged from 18 to 40 years (mean age: 27.0), with 40.2 percent aged 30–40 years (not shown in the table). No significant cross-national differences were found for gender.
Sociodemographic and cannabis use characteristics, and stigma measures.
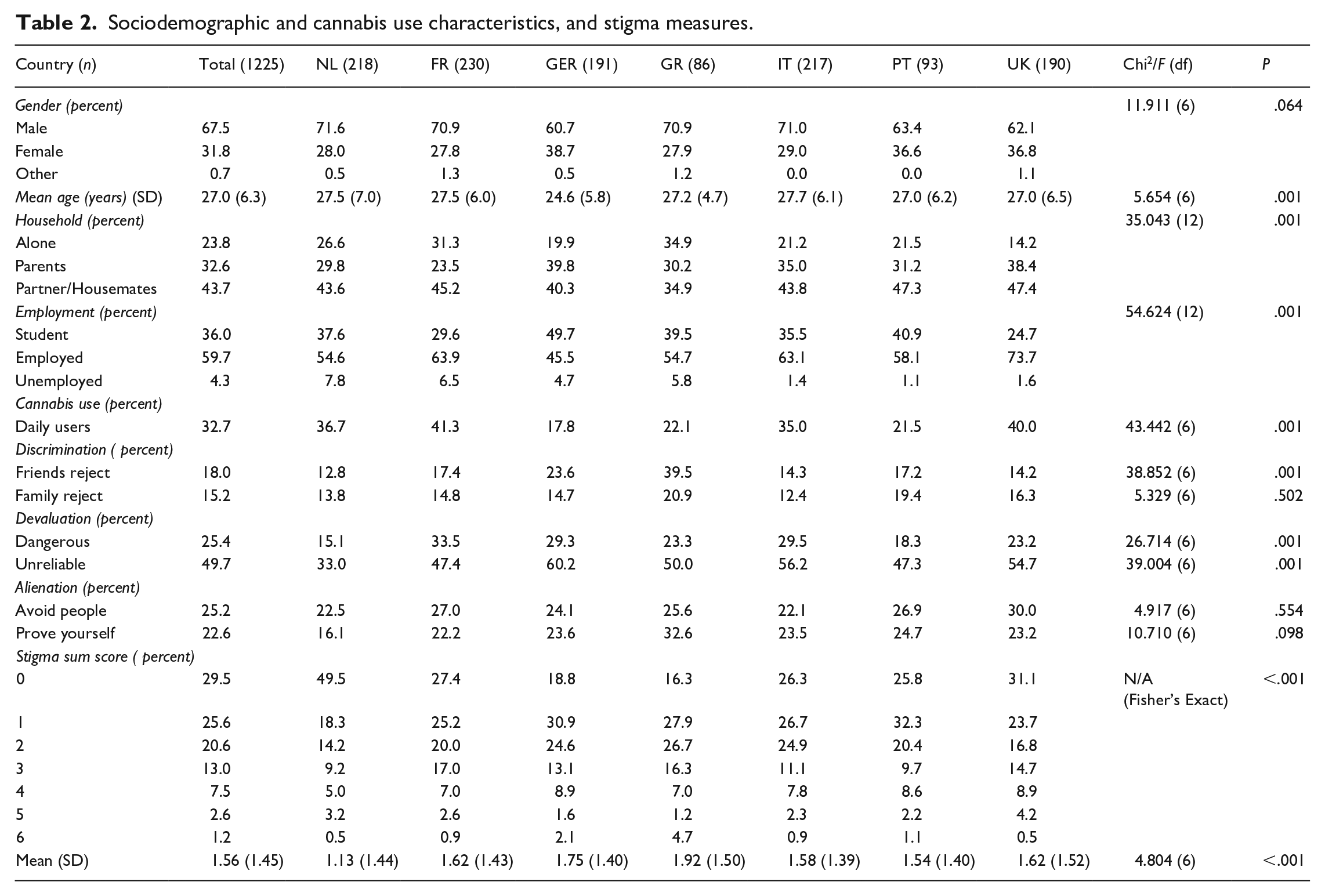
Concerning household type, close to one out of four respondents were living alone, one out of three were living with their parents and less than half of the total sample were living with a partner or housemates. Regarding employment status, 6 out of 10 participants were employed, more than one-third were students, and unemployed represented less than 5 percent of the total sample. Finally, close to one-third of respondents were daily cannabis users. In cross-national comparison, French respondents were least often living with their parents and most often daily cannabis users; Greeks were most often living alone and least often living with a partner or housemates; Germans were most likely to live with their parents, to be a student and to be a non-daily cannabis user; and UK participants were most often employed.
Table 2 also shows three domains of stigma (discrimination, perceived devaluation, alienation), and the stigma sum score of the total sample and by country. In the total sample, the discrimination items scored lowest, with close to one in six participants stating that they had been rejected by friends, and about one in seven that they had been rejected by family. Perceived devaluation scored higher, with one-quarter of the total sample reporting that most people believe that someone who uses cannabis is dangerous, and as much as half of all participants affirming that most people believe that cannabis users are unreliable. Alienation took an intermediate position, with one-quarter of participants stating that they avoid people because they think that they might look down on them because they use cannabis, and slightly fewer participants who say that they feel they need to prove themselves because of their own cannabis use. In cross-national comparison, no significant differences were found for one of the discrimination items (‘family reject’) and for the two alienation items (‘avoid people’, ‘prove yourself’). Greek participants most often reported that they had been rejected by friends (discrimination). Dutch respondents scored lowest on both perceived devaluation items, while French participants most often thought that people think that cannabis users are dangerous, and Germans more often thought that people believe that someone who uses cannabis is unreliable.
When taken together in the sum score, 29.5 percent of the total sample stated that none of the six items applies to them, ranging from 18.8 percent of the Greeks to 49.5 percent of the Dutch, and only a few respondents (1.2 percent) answered in the affirmative for all six items. On the scale 0–6, the average sum score for the total sample was 1.56 (SD = 1.45). The level of stigmatization was lowest in the Netherlands and highest in Greece (Table 2).
Table 3 depicts the results from six models of binary logistic regression. Models 1 and 2 cover the domain of discrimination, Models 3 and 4 the domain of perceived devaluation, and Models 5 and 6 the domain of alienation. In cross-national comparison, ‘country’ did not predict one of the discrimination items (Model 2, ‘family reject’) and one of the alienation items (Model 3, ‘avoid people’). Germany was the only country with significant differences for all four other models. Model 1 indicates that Greeks were 4.8 times and Germans 2.4 times more likely than Dutch participants to have been rejected by friends. In Model 3, participants from France, Germany and Italy were more likely (2.9, 2.3 and 2.2 times more than Dutch participants, respectively) to think that people believe that cannabis users are dangerous. Model 4 shows that participants from all other countries were more likely than the Dutch to think that people believe that cannabis users are unreliable. Germany was the strongest predictor (odds ratio: 3.1); for the other countries the odds ratio ranged from 1.9 (Portugal) to 2.6 (Italy). Finally, in Model 6 participants from all other countries besides France were more likely than the Dutch to want to prove themselves because of their cannabis use. Greece had the strongest predictive power (odds ratio: 2.8). The other countries’ odds ratios ranged from 1.7 to 1.9.
Regression models for discrimination, alienation, perceived devaluation and stigma.
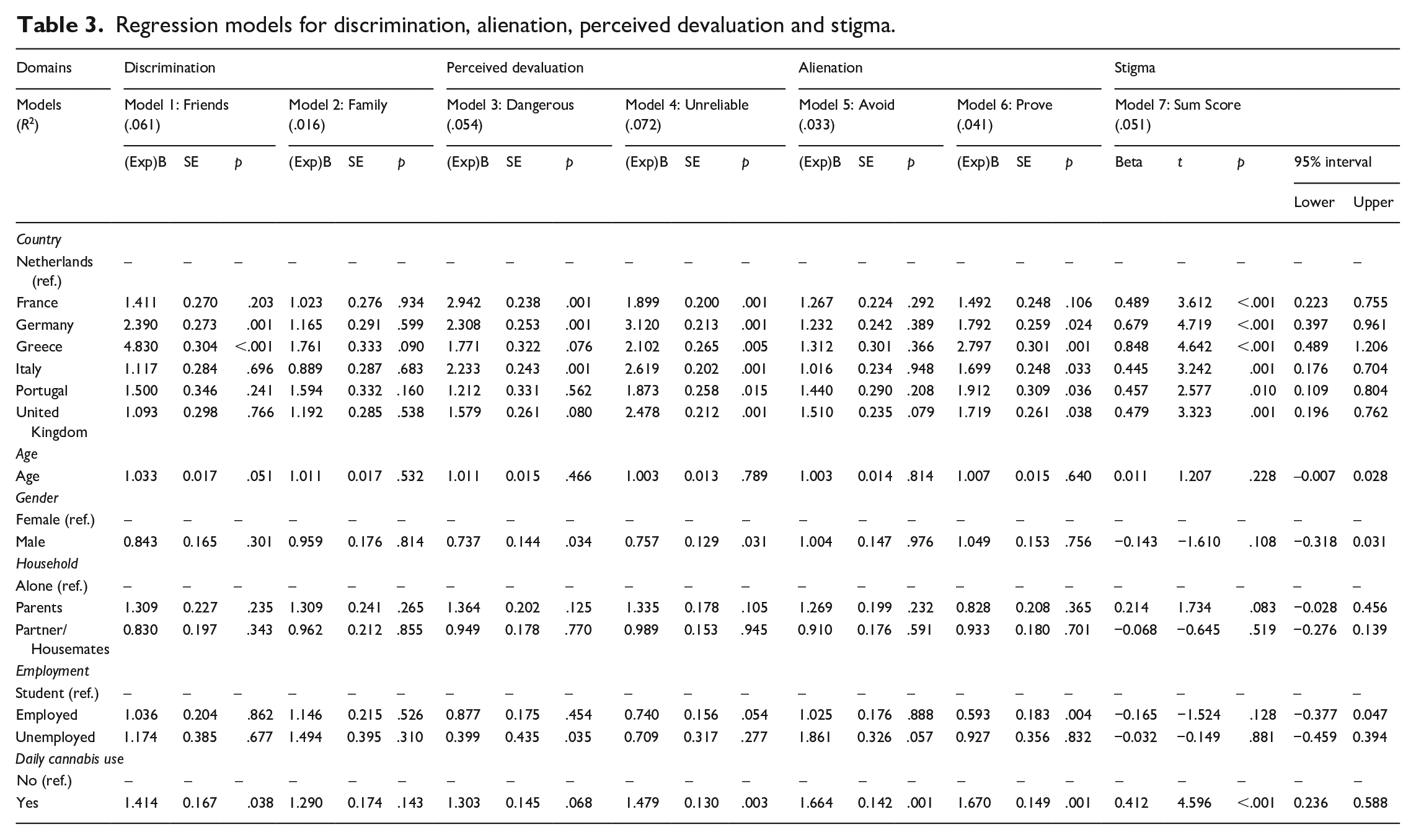
Regarding sociodemographic variables, age and household type did not predict any of the three dimensions. In addition, none of the other sociodemographic variables predicted the outcome of Model 2 (‘family reject’) and Model 5 (‘avoid’). Gender significantly predicted only perceived devaluation, with male participants being more likely than women to report perceived devaluation (Models 3 and 4). Finally, unemployed participants were more likely than students to think that people see them as dangerous (Model 3), and the employed were more likely to feel they have to prove themselves because of their cannabis use (Model 6).
Furthermore, frequency of use significantly contributed to the prediction of four dimensions of stigmatization (odds ratio: from 1.4 to 1.7). Compared with non-daily users, daily users were more likely to have been rejected by friends (Model 1); to think that people see cannabis users as unreliable (Model 4); to avoid people because they think they might look down on them because they use cannabis (Model 5); to want to prove themselves because of their cannabis use (Model 6).
Table 3 also shows the results from the linear regression analysis to predict the stigmatization sum score (Model 7). Compared with the Netherlands, respondents from all other countries showed significantly higher levels of stigmatization: the model predicts that the stigma sum score is about half a point higher for Italians (0.45), Portuguese (0.46), British (0.48) and French (0.49), 0.68 points higher for Germans and 0.85 points higher for Greeks. None of the sociodemographic variables contribute to the prediction of the stigma sum score, but daily cannabis use does. The stigma sum score is 0.41 points higher for daily users than for non-daily users.
Discussion and conclusion
The aim of this study was to assess to what extent and how cannabis users in different countries with different cannabis policies perceive, experience and respond to stigmatization. More specifically, we investigated three dimensions of stigma experienced by illicit drug users: discrimination, perceived devaluation and alienation (Ahern et al., 2007).
The differential contribution of countries to the model predicting stigmatization largely confirmed our hypothesis that the level of cannabis-related stigma increases with the stringency of cannabis policy. As expected, taken together in the sum score, stigmatization was higher in all other countries compared with the country with the most liberal cannabis policy (the Netherlands). Also, the level of stigmatization was relatively low in Portugal and relatively high in Greece, which was categorized as the most punitive country in our study. However, what comes as a surprise is that the degree of stigmatization reported by participants from Germany was similar to the level reported by those from Greece. Overall, the results indicate that most cannabis users in this study do not experience high degrees of discrimination, perceived devaluation or alienation. However, there were differences between the three domains of stigma. Discrimination was the domain that scored lowest, whereas perceived devaluation scored highest.
Regarding discrimination, most participants (more than four out of five) had not experienced rejection by family or/and friends because of their cannabis use. Interestingly, in the binary logistic regression analysis, neither country nor any of the sociodemographic variables or frequency of use predicted rejection by family. However, two countries predicted the other dimension of discrimination (Model 1). The fact that Greeks were 4.8 times more likely than the Dutch to experience rejection by friends confirms a striking difference between the most liberal and the most restrictive country in our study. Remarkably, Germany is the only other country that predicts rejection by friends. Even though Germans did not report this dimension of discrimination as often as Greeks, they were 2.5 times more likely to experience it than the Dutch.
Perceived devaluation was the most frequently reported dimension of stigma, with almost half of the respondents stating that people think that cannabis users are unreliable, and one in four reporting that most people believe that someone who uses cannabis is dangerous. This confirms that cannabis users are still associated with negative stereotypes, albeit less strongly with danger, as used to be the case in the era of ‘Reefer Madness’, and more with personality traits such as laziness and a lack of motivation (Meier and White, 2018; Mortensen et al., 2019). Recent research has shown that in public opinion the terms ‘irresponsible’ and ‘lazy’ are among the five characteristics most highly associated with cannabis users (Mikos and Kam, 2019). As to differences between countries, binary logistic regression indicated that users from France, Germany and Italy were more likely than Dutch respondents to say that most people believe that cannabis users are dangerous. Also, participants from all countries were more likely than the Dutch to report that people think that cannabis users are unreliable. Germany was the strongest predictor (odds ratio: 3.1).
Regarding the prevalence of alienation, there were no cross-national differences, which suggests that participants’ responses to stigmatization, whether passive (avoidance) or active (prove yourself), are not related to national cannabis policy. Moreover, when controlling for other sociodemographic variables and cannabis use frequency in binary logistic regression analysis, no cross-national differences were found in predicting avoidance. However, this was not the case for ‘prove yourself’: participants from Germany, Greece, Italy, Portugal and the UK were more likely than the Dutch to have experienced this type of alienation. As hypothesized, Greece was the strongest predictor (odds ratio: 2.8).
Interestingly, in the logistic regression models, sociodemographic variables generally did not contribute to the prediction of the three domains of cannabis-related stigma. Contrariwise, daily cannabis users in this study were more likely than less frequent users to have been rejected by friends (discrimination); to report that most people think that cannabis users are unreliable (perceived devaluation); and to experience alienation (avoidance and proving themselves because of their cannabis use).
With the three domains of stigmatization brought together on a stigma scale (sum score range 0–6), the average score of 1.56 (SD = 1.45) indicates that overall cannabis-related stigmatization is low to moderate. The differences found between countries confirm our hypothesis that strict cannabis policy is associated with a higher degree of stigmatization whereas less punitive policy is associated with a lower degree of stigmatization of cannabis use and normalization, except for Germany. Indeed, cannabis users from the Netherlands, the country with the most liberal cannabis policy at the consumer level in the EU, experience the lowest level of stigma, followed by Portugal, which has a relatively liberal policy as well. Also, at the other end of the cannabis policy continuum, in Greece, the most punitive country in our study, the level of stigmatization was much higher. In short, in can be concluded that cannabis policy plays a significant role in the construction of perceptions of, experiences with and responses to stigmatization. However, what remains an intriguing question is why cannabis-related stigma in Germany was at a similar level to that in Greece. One explanation could be that German cannabis users are more aware of the current illegal status of cannabis in their country, owing to the lively political debate at both the federal and the local level on decriminalization and legalization (Stöver et al., 2019), and/or to the proximity to the Netherlands and its coffeeshop policy. Future research is warranted to unravel the atypical case of Germany.
In addition to national cannabis policy, frequency of cannabis use strongly explained differences in stigmatization, with daily users experiencing a much higher degree of stigma than non-daily users. This confirms previous studies concluding that cannabis-related stigma is often associated with patterns of cannabis use and particularly with frequency of cannabis use (Hathaway, 2004; Kolar et al., 2018).
An important limitation of this study is that participants constituted a convenient and not a normative sample. Daily users in this study were over-represented. It is estimated that around 1 percent of adults in the EU are daily cannabis users (EMCDDA, 2019b), but this amounted to almost one-third in this study. Our results cannot be generalized to a broader population. As for the external validity, it cannot be assumed that it is a representative sample of cannabis users as a whole. Given that daily users reported higher levels of stigmatization than less frequent users, we expect that this study overestimates cannabis-related stigma and assume that it will be lower in normative statistical representative samples of current cannabis users. Another limitation is that we used only a selection from the items in the original scale (Ahern et al., 2007), and specified them for cannabis. We did so because the original scale was used for a much more heterogeneous population of drug users, including dependent problem users (of hard drugs). Nonetheless, additional items might improve the validity in the measurement of cannabis-related stigma. Moreover, the ‘discrimination’ items were exclusively focused on discrimination from friends and family. The results might have been different (that is, higher levels of reported discrimination) if these questions had been about experiences with neighbours, strangers, employers, etc. Another potential limitation of this study is that, because we focused on differences between countries, we did not ask about the provinces/regions/states (Länder) of residence. As a consequence, we did not consider regional variation across Germany, where some states (Länder) have more restrictive attitudes and penal practices towards cannabis users than others. Also, we did not ask about the specific residence (rural or urban setting), which might affect perceptions of stigma. Furthermore, we investigated only perceived stigma and self-stigma (Corrigan and Watson, 2002) and thereby focused on the perspective of users. Findings on perceived stigma might be affected by the fact that the survey was conducted in the Netherlands, the most liberal country in this study. For participants outside the Netherlands, the experience of the liberal Dutch policy regarding cannabis use could have reinforced a potential contrast in comparison with their own country of residence and subsequently affected their responses to stigma questions. For that reason, during the process of recruiting the participants and administering the questionnaire, we emphasized verbally and also written on the questionnaire that the questions refer to the situation ‘in your country’ and ‘before you arrived in the Netherlands’. Further research in the general population is needed to assess to what extent and how stigmatization as reported by cannabis users corresponds to public stigma, that is, the beliefs that individuals in society hold about cannabis users (Corrigan and Watson, 2002).
Notwithstanding these limitations, this study has responded to the call for further examination of cannabis-related stigma and further exploration of the extent and nature of normalization across different countries with different cannabis policies. Our findings that not all cannabis users in this study experience a low degree of stigma confirms that cannabis users should not be understood as a homogeneous population.
The cross-national similarities and differences in cannabis-related stigma that resulted from our comparative analysis largely support a core element of the normalization thesis, namely that at societal level normalization encompasses liberal shifts in drug policy (Parker, 2005). However, even though stigmatization was lowest in countries with the most liberal cannabis policies in Europe, stigmatization was not fully absent. If stigmatization is understood as complementary to normalization, elaborating the extent to which and how cannabis users apply norms and follow self-regulation rules can contribute to a better understanding of stigmatization and de-stigmatization.
Footnotes
Acknowledgements
We wish to thank Marie Agergaard, Elliott Bloem, Beatriz Carvahlo, Timothy Dörr, Alexandre Jeunet, Dinos Karakassis, Zofia Kostrzewa, Boris Pinksterboer, Lily Pitters, Mikhail Sivolap, Fedor Taggenbrock, Jaap Wallet and Niklas Zimmermann for their assistance in fieldwork and data-collection.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is an extension to the IDPSO-project, conducted by a European consortium of the Católica Porto Business School (Portugal), Paris School of Economics, Université Paris I (France), MIPA (Italy) and Bonger Institute of Criminology, Law School, University of Amsterdam (the Netherlands). For the Dutch part, including the data-collection for this paper, a grant (# 63200000106) was received from ZonMw (the Netherlands Organisation for Health Research and Development).