
Abstract
In old subjects, the effect on visual performance of the interaction between the spectral power distribution of street lamps and the different types of intraocular lenses (IOLs) is unknown. Contrast threshold (CT) and reaction time (RT) were analysed in off-axis vision at mesopic illumination conditions provided by high-pressure sodium and metal-halide lamps, using a Maxwellian view optical system. Four groups of subjects participated: 10 young subjects, 20 elderly subjects with cataracts and the same subjects after cataract surgery were divided into two groups, 10 subjects implanted with a blue light-filtering and 10 subjects with a non-blue light-filtering IOL (NBIOL). Age-related cataract impairs detection and reaction capabilities; tasks that are nevertheless improved after surgery. The type of lamp does not affect both tasks in the case of the blue light-filtering IOL group, but it does in the NBIOL group. When comparing the two lenses, no detrimental effect of the blue light filter is observed in both tasks. In conclusion, at representative night-driving conditions, the spectral power distribution of the street lamp does not have a clinically relevant effect on visual tasks such as CT and visual RT in pseudophakic subjects, regardless of the type of IOL implanted.
1. Introduction
When driving after dark, the driver is faced with a variety of visual tasks with different light levels, from photopic (car headlights) through mesopic (road and adjacent areas) to scotopic range (beyond the roadside). 1 This variation, which the visual system has to cope with, justifies, among other factors, that the study of driving performance and the ability to drive safely at night becomes a topic of potential relevance. Basically, the resulting pedestrian and driver’s accident rates are reported to be higher at night than during the day for many reasons, including fatigue, alcohol and perception errors.2–4 These perception errors, that is, misjudgement of speed and distance and ‘looked, but failed to see’ situation, are particularly high in low-light conditions, when visibility is reduced. Although it is difficult to link visibility to the number of collisions, it is clear that driving is a complex task in which visual processes play a crucial role. 5 These compelling reasons justify the need for adequate illumination, being high-pressure sodium (HPS) and metal-halide (MH) lamps among the most widely used in public lighting and whose use is widespread in psychophysical experiments. Although the implementation of light-emitting diode (LED) technology as lighting systems is increasing and forecasts are positive, the percentage of LED penetration is awaited to be below 40% through 2022. 6 The presence of street lamps places night driving within the mesopic range and, given that the range of recommended road surface luminances in the standard is between 0.3 cd/m2 and 2 cd/m2, 7 one of the main applications of mesopic photometry is public lighting. 1 At mesopic light levels, with luminance limits established by the Commission Internationale de l’Eclairage (CIE) of 0.005 cd/m2 and 5 cd/m2, both rods and cones contribute to the processing of visual information. 1 In the upper mesopic range, that is 1 cd/m2, no lamp effect was found when comparing HPS and MH lamps on off-axis vision. However, as we approach the lower limit of the mesopic range, that is, 0.01 cd/m2, luminance thresholds were lower for MH lamp. It is also important to mention that at this luminance level visibility is relatively improved in off-axis vision compared to foveal vision, an important change because the main task of the driver is to obtain enough information from the visual field to cope with the environment.8–10
Visual tasks related to driving include detection, reaction and discrimination, among others.1,8 Firstly, it is essential to detect unexpected pedestrians or potential hazards in a background, both with a certain luminance, resulting in a contrast value. 11 Secondly, the reaction to these hazards is critical in terms of driver and pedestrian safety and also proves to be a consistent index relating driving performance and the number of collisions. 12 For this reason, contrast threshold (CT) and visual reaction time (RT) are considered reliable and representative indexes of visual performance during night driving and are therefore assessed in this work. 13 These visual tasks have been evaluated under conditions of mesopic illumination and off-axis vision provided by lamps that differ in their spectrum, such as HPS and MH lamps, especially in young subjects. In the case of CT, MH lamp provides better off-axis detection at low background luminances and low contrast stimuli.14,15 From a more applied perspective, Uttley et al. 16 found that in young and old subjects with normal ocular media, simulated obstacle detection improved for lamps with a higher S/P ratio and an illuminance value of 0.2 lx (low mesopic range). As far as RT is concerned, experiments both in the laboratory and in more natural viewing conditions show that RT is shorter when using the MH lamp compared to the HPS lamp. Lewis 10 came to this conclusion using a two-channel Maxwellian view optical system as used in this work. Akashi et al. 17 obtained the same result by performing an experiment in more realistic conditions (outdoor parking), at night-time. The same spectrum effect on RT has also been obtained using LED light sources that differ in their spectra, with faster responses as the S/P ratio increases. 18
Currently, old people constitute a significant and growing percentage of drivers.19,20 However, aging poses a number of problems recognized by older drivers, 20 which lead them to limit their activity. 21 This limitation is accentuated by the presence of cataracts, 22 as drivers report greater difficulty in overall driving performance, especially in detecting and avoiding obstacles at night and with incoming headlights.19,23,24 Nonetheless, the review of Subzwari et al. 19 shows a strong association between cataract surgery and a reduction in the difficulties experienced by old drivers at night, including the detection and avoidance of obstacles. Regarding the type of implanted intraocular lens (IOL), there is an ongoing controversy about the choice of blue light-filtering intraocular lenses (BIOLs) based on their effect on photoprotection and photoreception. Short-wavelength blocking has proved neither to affect photopic and mesopic visual acuity and contrast sensitivity 25 nor to cause disruption in photopic colour vision. 26 In mesopic conditions, although some studies report a reduction in colour vision in the blue region of the spectrum, 27 this effect is much less than that produced by a normal-aged lens. 28 Considering the existing information on the effect of BIOLs on photoprotection and photoreception, the quality of evidence guiding the selection of IOLs based on their effect on visual performance is quite deficient. Particularly under mesopic illumination conditions, where short-wavelength photoreception becomes relevant for peripheral tasks applicable to night driving, visual performance is more likely to be negatively affected by the transmission properties of a BIOL.
In addition, no literature has been found on the effect of different street lamps on the visual performance of cataract and pseudophakic subjects implanted with IOLs of different transmittance. On the contrary, in young subjects, either in field studies or in laboratories, both CT and RT seem to benefit from the greater short-wavelength content of MH lamp, compared to HPS lamp.9,13,16,17 Thus, the aim of this experiment is to analyse the effect of blue light-filtering IOLs, by comparison to non-blue light-filtering IOLs (NBIOLs), and common street lamps on visual performance, evaluating CT and RT, under mesopic lighting levels and off-axis vision.
2. Method
2.1 Patients
Written informed consent was obtained from all test participants. The study followed the tenets of the Declaration of Helsinki and procedures were approved by the Clinical Research Ethics Committee of the Eastern Area of Valladolid.
In this prospective comparative study, 30 participants with no history of ocular disease underwent a complete ophthalmological examination, including long-distance refraction, colour test assessment and examination of anterior and posterior segments with slit lamp and fully dilated fundoscopy, respectively. Patients were divided into four groups. Group 1: 10 young subjects (24 ± 2.6) (0.0 ± 0.06 logMAR − minimum angle of resolution) who were considered as the baseline group. Group 2: 20 old subjects (69.2 ± 9.3) (0.37 ± 0.16 logMAR) diagnosed with age-related surgical cataracts constituted the cataract group. Groups 3 and 4: the same subjects from group 2 after cataract surgery, 10 patients implanted with a blue light-filtering IOL constituted the BIOL group (67.8 ± 8.9) (0.14 ± 0.09 logMAR) (group 3) and 10 implanted with a non-blue light-filtering IOL constituted the NBIOL group (71 ± 10.2) (0.13 ± 0.1 logMAR) (group 4). Exclusion criteria were known colour-vision defects, the use of medication that could affect colour vision, the presence of diabetes, ocular pathology other than cataract and intraoperative complications.
All patients were operated on by the same surgeon using a standard procedure and topical anaesthesia. The one-piece foldable Acrysof IQ SN60WF and Acrysof SA60AT posterior chamber IOLs were randomly selected for implantation (Alcon Laboratories, Inc., Fort Worth, TX), both have identical materials and dimensions, except for the aspherical design and the covalently bounded yellow chromophores of the SN60WF IOL. Their spectral transmissions were measured immersed in a balanced salt solution in our spectroscopy laboratory (OMA2 detector camera) and are shown in Figure 1, with the SN60WF IOL transmitting on average 55% more radiation for the short-wavelength range (440–500 nm) of the spectrum.
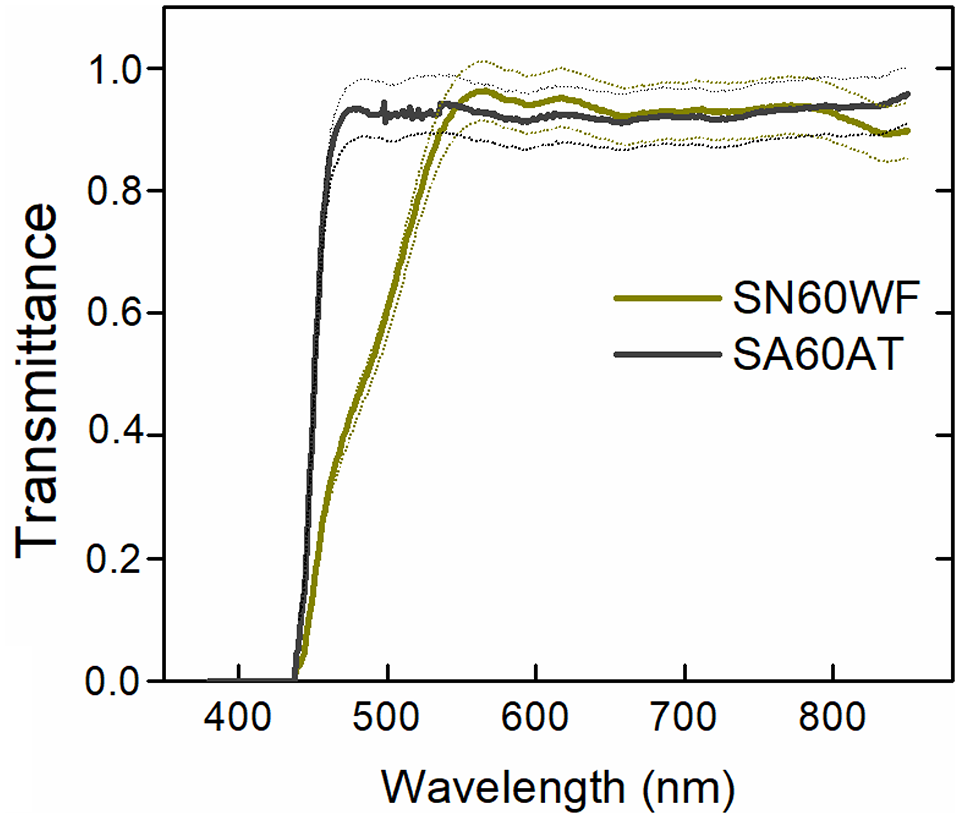
Spectral transmittance of Acrysof IQ SN60WF and Acrysof SA60AT IOLs for wavelengths 375–800 nm. Dotted lines represent corresponding standard deviation
2.2 Method
A custom-made computerized two-channel Maxwellian view optical system was used as experimental set-up and is represented in Figure 2, although described in more detail in previous work. 29 Maxwellian vision ensures all the light coming from the light source reaches the retina. The image of the light source has a diameter of 2.5 mm in the entrance pupil of the observer. The concentric background and probe beams, coming from the same lamp, reached the subject’s pupil, subtending 10° and 2°, respectively. These underlying sizes of both beams are obtained by the appropriate placement of lenses (L) and diaphragms (D). Neutral density filters (F) and shutters (S) enable the control of the luminance and exposure times of both beams, respectively. In the probe beam there is a mirror (MP) which produces a 90° reflection of the beam, three motorized discs with neutral density filters (FP1.0, FP0.5, FP0.1), two lenses (LP160, LP200), two shutters (SP1, SP2), two diaphragms (DP1, DP2) and a beam splitter (BSB). For the background beam, there are three discs with neutral density filters (FB2.0, FB0.5, FB0.1), two diaphragms (DB1, DB2), two lenses (LB160, LB200), a mirror (MB) that produces a 90° reflection of the beam and a beam splitter (BSB) which overlaps the background and probe beams. In addition, there are two beams corresponding to the CCD camera and the eccentric fixation test beams.
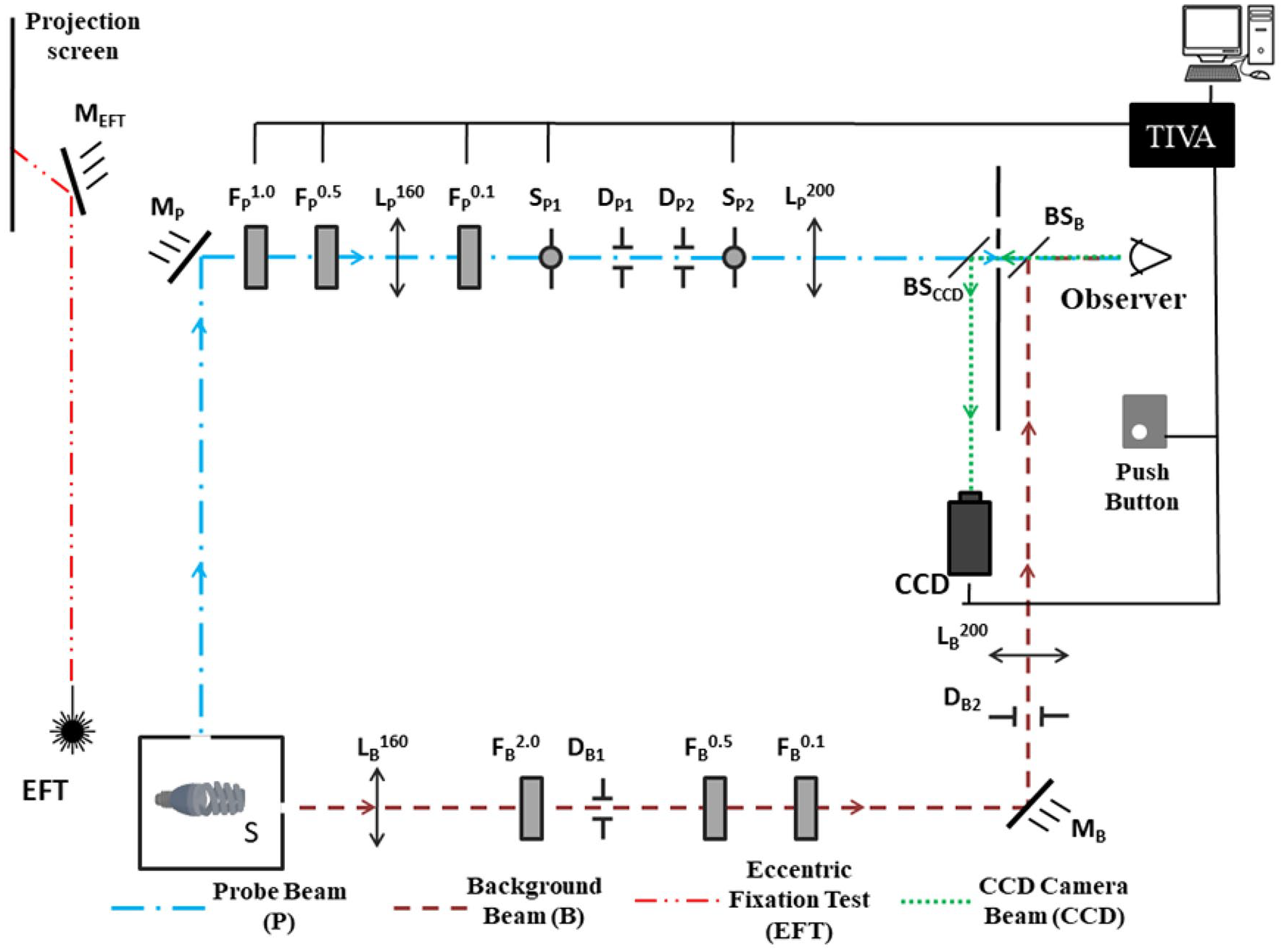
Scheme of the experimental set-up. The subscripts P and B refer to the elements in the probe and background beams, respectively. The CCD subscript refers to the elements in the CCD camera beam. The subscript EFT refers to the elements in the eccentric fixation test beam. The numerical superscripts of the filters refer to the optical density steps and those of the lenses refer to the focal length
Considering these sizes, the spatial frequency associated with the stimulus is approximately 0.5 cycles per degree (cpd), with no possible influence of high-frequency harmonics on contrast sensitivity given the low luminance level employed and the poor retinal resolution at that light level.30,31 The fixation of the subject was maintained at a single, dim and infinity-located single point of fixation, during the light adaptation time and psychophysical measurements. The point allowed the presentation of the stimulus at 10° of temporal eccentricity, an eccentricity recommended by the CIE for the evaluation of visual performance during driving. 8 Overall, this experimental design simulates the appearance of roadside obstacles, with the background simulating the overall light provided by the street lamp, The stimulus simulates the presence of an obstacle illuminated by the same lamp and the fixation point (10º) simulates the fixation of the driver on the road. During measurements, the head of the subject was fixed to the experimental set-up by bitting on a bite bar made of dental compound.
The light sources consisted of two common street lamps: HPS and MH lamps. The absolute irradiance spectral power distribution of both lamps was obtained by placing the lamp 50 cm from the entrance slit of a spectrometer, and the results showed that MH lamp has a higher emission in the short-wavelength region, compared to HPS lamp. 32 From the spectral power distribution, the S/P ratios were calculated. The S/P ratios of HPS and MH lamps were 0.49 and 1.17, respectively. The emision of MH lamp in the short-wavelength range (440-500 nm) was 76% higher than that of HPS lamp.
2.3 Procedure
CT and RT were obtained in off-axis vision (10° temporal eccentricity), for probe exposure times of 40 and 500 ms, respectively, and for a background luminance of 0.01 cd/m2 (2.5 × 10−2 photopic trolands (Td)) provided by HPS and MH lamps. CT was determined by the method of limits and the subject was instructed to respond whether the stimulus was detected or not, providing a ‘yes/no’ answer, after a warning tone sounded 1 second before the presentation of the stimulus. To obtain the individual luminance value used for the CT calculation, the range of luminances employed consisted of six runs (three descending, three ascending), each one with eight different luminances (0.1 steps of logarithmic units), equivalent to a total of 48 tests for each CT data obtained. In the case of RT task, individual data were collected for a Weber contrast of 0.2 (3 × 10−2 photopic Td) repeated 20 times. The subject was instructed to press the response button as soon as the stimulus was detected. The presentation of the stimulus varied from one trial to another over a randomized time period of 3 to 7 seconds, to prevent from subject conditioning and to increase the reliability of the procedure. RT values above 2000 ms and below 150 ms were automatically eliminated and the measurement was repeated. 33 Values outside this range are uncommon and usually due to loss of attention or blinking. 34 The same protocols and procedures were followed for each visual task for all the four groups. The minimum waiting time after cataract surgery for psychophysical tests was 45 days, always after a complete normal postoperative ophthalmological examination. All subjects, including the emmetropic and the users of contact lenses, were compensated with the same type of ophthalmic lenses to avoid transmission differences in the results due to this factor. 35 The right eye was always selected for the measurements, while the left one was occluded. CT and RT measurements were taken together on two different days, 1 day for each lamp, to minimize the effect of fatigue. The order of the lamps was randomized to reduce the learning effect and the participants were instructed and trained to familiarize with the measurement procedure. Prior to each set of measurements, the subject was dark-adapted for 30 minutes (1.25 × 10−5 scotopic Td). Immediately afterwards, the tested temporal area of the retina was exposed to the corresponding background luminance for 3 minutes to light adaptation.
2.4 Statistical analysis
The statistical analysis was performed using SPSS statistical software (version 19.0, IBM Corp., Armonk, NY, USA). Several t-tests were performed for the data as a function of two factors, the type of lamp (HPS and MH) and transmittance of the ocular media (baseline, cataract, BIOL and NBIOL groups). The significance level was set at α = 0.05. The analyses were used to compare the differences between the CT and RT variables for the different conditions analysed. Due to the fact that multiple comparisons are tested, the given α-value of 0.05 may not be appropriate for each individual comparison but for the set of all comparisons, so to avoid false positives, the Bonferroni correction was performed, the simplest and most conservative approach to adjust p-values. All the reported results have been already corrected. The Student’s t-distribution is used to compare whether the mean values of a variable in two groups are equal, i.e., once we know that there are differences in at least one pair of groups, the post-hoc t-test analyses in which pairs those differences are. Thus, the statistics provided below include the t-values, which are related to Student’s t distribution. Additionally, the effect size for each significant comparison described in the results section was evaluated by means of Hedges’ g statistic and the Pearson’s r correlation coefficient, 36 the former being an effect size statistic appropriate for small samples, 37 and the latter as a way of showing the strength of the relationship between the different levels of the factors.
3. Results
Considering the two lamps and the four groups of subjects, 4800 stimuli were presented for the CT measurement and 2000 stimuli for the RT measurement. According to Sawilowsky, 38 considering the number of participants for each group and the values obtained in CT and RT for each condition, 19 out of the 23 statistically significant comparisons were found to provide large size effects (Hedges’ g values greater than or equal to 0.8), very large size effects (greater than or equal to 1.2) or huge size effects (greater than or equal to 2.0), while only 4 of the 23 comparisons provide medium size effects (values between 0.5 and 0.8). Pearson’s r correlation coefficients provide the same results.
3.1 Contrast threshold
CT was analysed for the four groups of participants at a background luminance of 0.01 cd/m2 provided by HPS and MH lamps. Figure 3 shows the results obtained for the different experimental conditions.
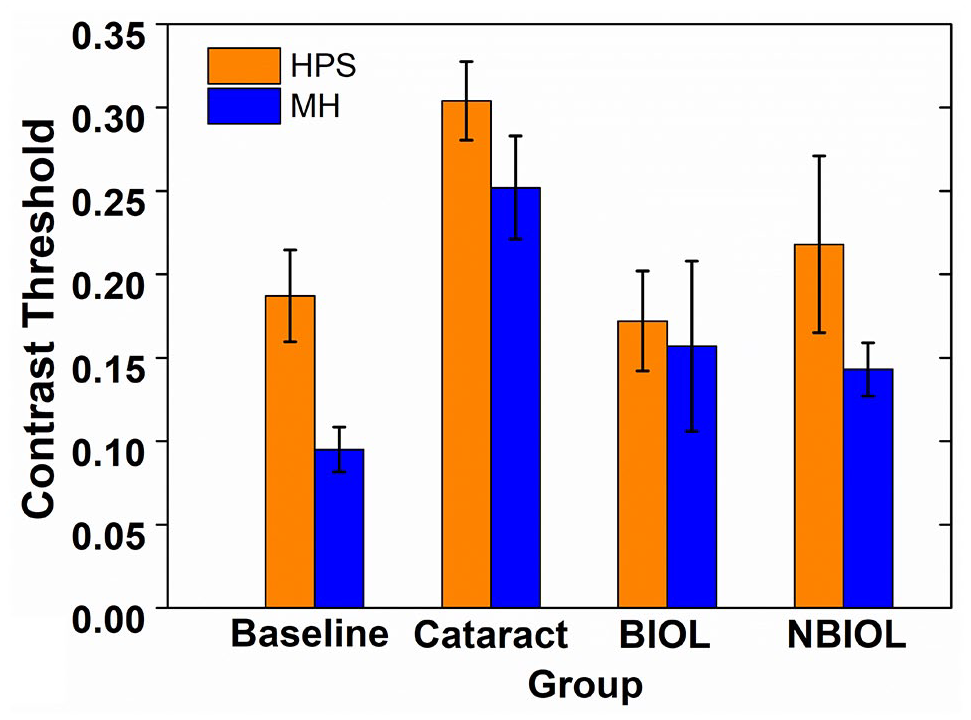
Mean CT for both lamps (HPS and MH) as a function of the group of subjects (baseline, cataract, BIOL and NBIOL groups) at a background luminance of 0.01 cd/m2. Error bars define the 95% confidence interval
3.1.1 Lamp effect
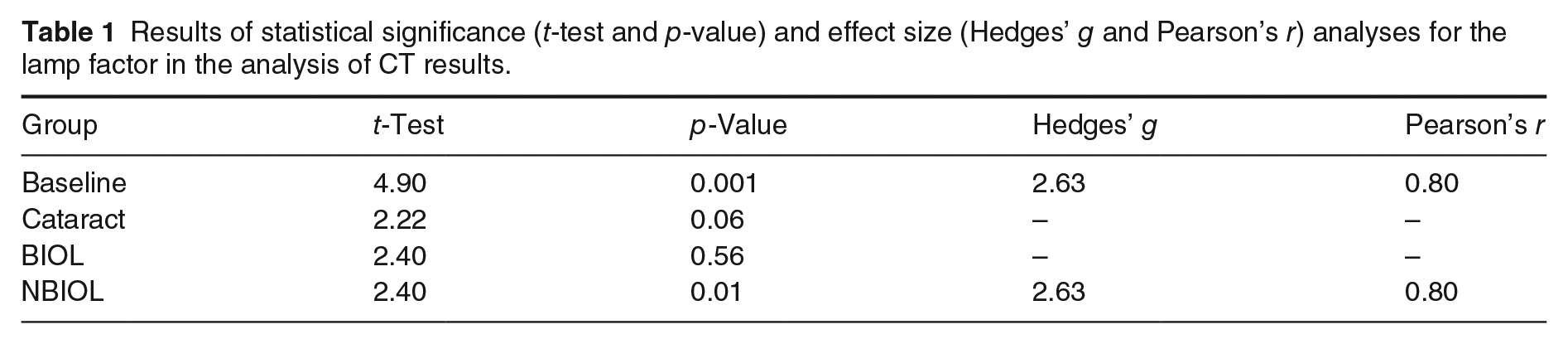
In the baseline group, CT is significantly lower for MH. On the other hand, in the cataract group there is no lamp effect. After surgery, CTs in the BIOL are similar between lamps. In contrast to the NBIOL group, where CT of HPS lamp is significantly higher compared to MH lamp. The statistical results for the effect of the lamp factor on CT are shown in Table 1.
Results of statistical significance (t-test and p-value) and effect size (Hedges’ g and Pearson’s r) analyses for the lamp factor in the analysis of CT results.
3.1.2 Transmittance effect
The comparison between the baseline and cataract groups reveals significantly higher CT for the last group and for both lamps. In the case of the pseudophakic groups, CT has significantly improved after surgery for HPS and MH lamps. On the other hand, when comparing the results between the BIOL and NBIOL groups for each lamp separately, the results are similar regardless of the lamp.
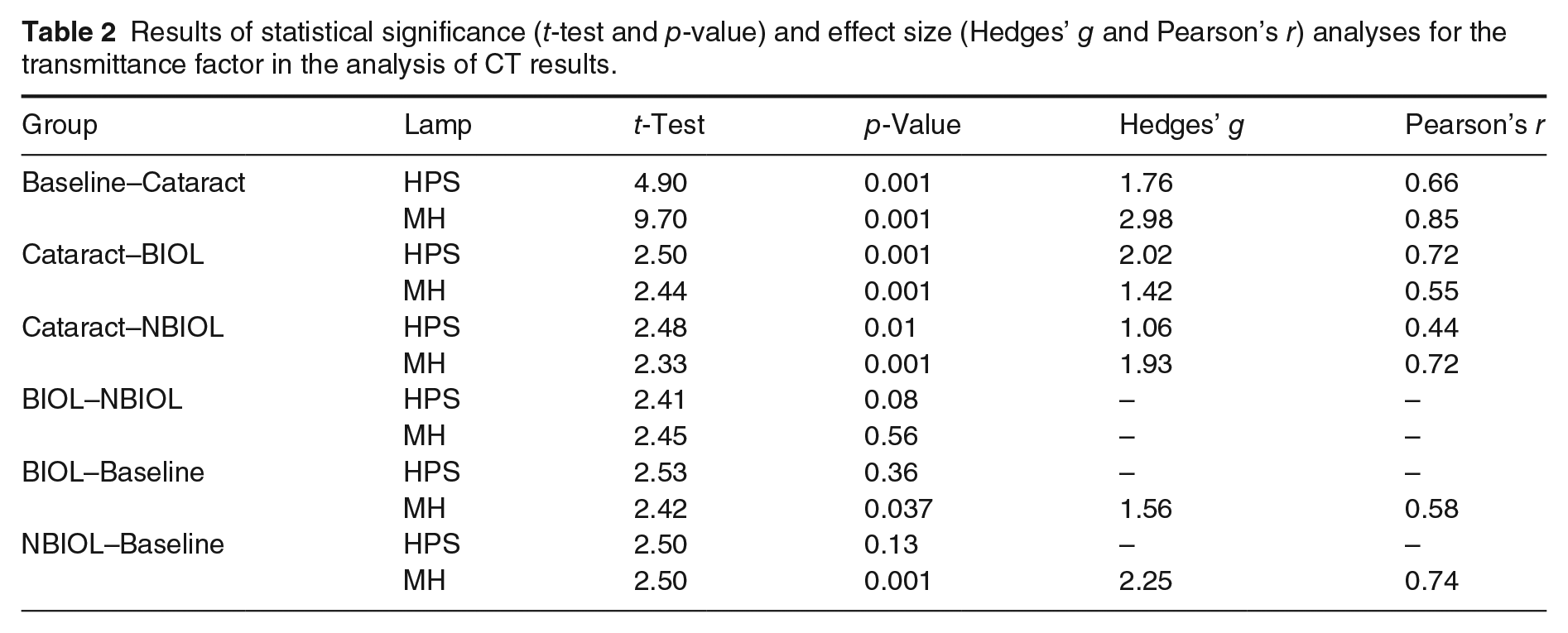
Finally, the comparison between the pseudophakic and baseline groups provides different results depending on the lamp. For HPS lamp, CT results are similar. However, for the MH lamp, CT results for the BIOL and NBIOL groups are significantly greater compared to those of the baseline group. The statistical results for the effect of the transmittance factor on CT are shown in Table 2.
Results of statistical significance (t-test and p-value) and effect size (Hedges’ g and Pearson’s r) analyses for the transmittance factor in the analysis of CT results.
3.2 Visual RT
RT was analysed for the four groups of subjects at a background luminance of 0.01 cd/m2 provided by HPS and MH lamps. Figure 4 shows the results obtained for the different experimental conditions.
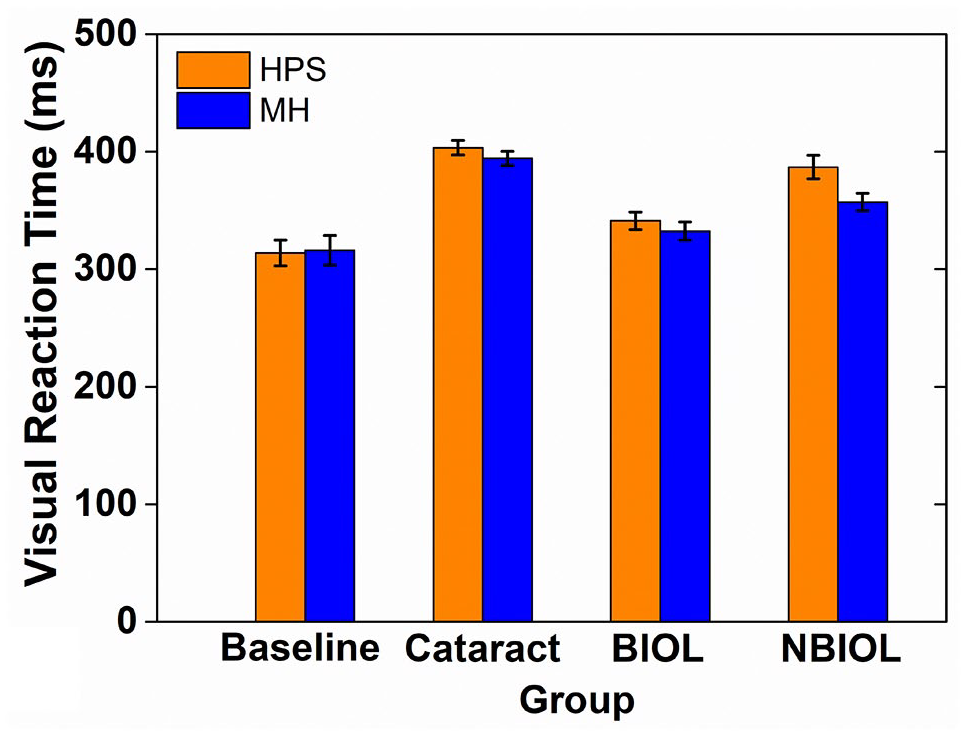
Mean RT for both lamps (HPS and MH) as a function of the group of subjects (baseline, cataract, BIOL and NBIOL groups) at a background luminance of 0.01 cd/m2. Error bars define the 95% confidence interval
3.2.1 Lamp effect
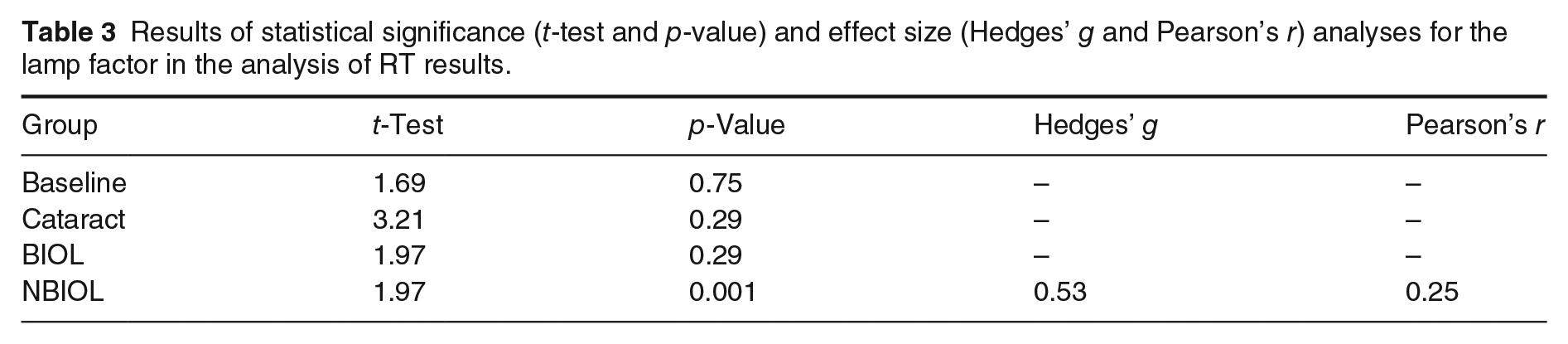
No lamp effect is obtained in either the baseline group or the cataract group. In the case of the pseudophakic groups, for the BIOL group, the mean RT is comparable between lamps. For the NBIOL group, the mean RT is lower for MH lamp compared to HPS lamp. The statistical results for the effect of the lamp factor on RT are shown in Table 3.
Results of statistical significance (t-test and p-value) and effect size (Hedges’ g and Pearson’s r) analyses for the lamp factor in the analysis of RT results.
3.2.2 Transmittance effect
The presence of cataract is responsible for higher RT values in the cataract group compared to the baseline group, as can be seen in Figure 4. On the other hand, surgery significantly improves RT in both pseudophakic groups.
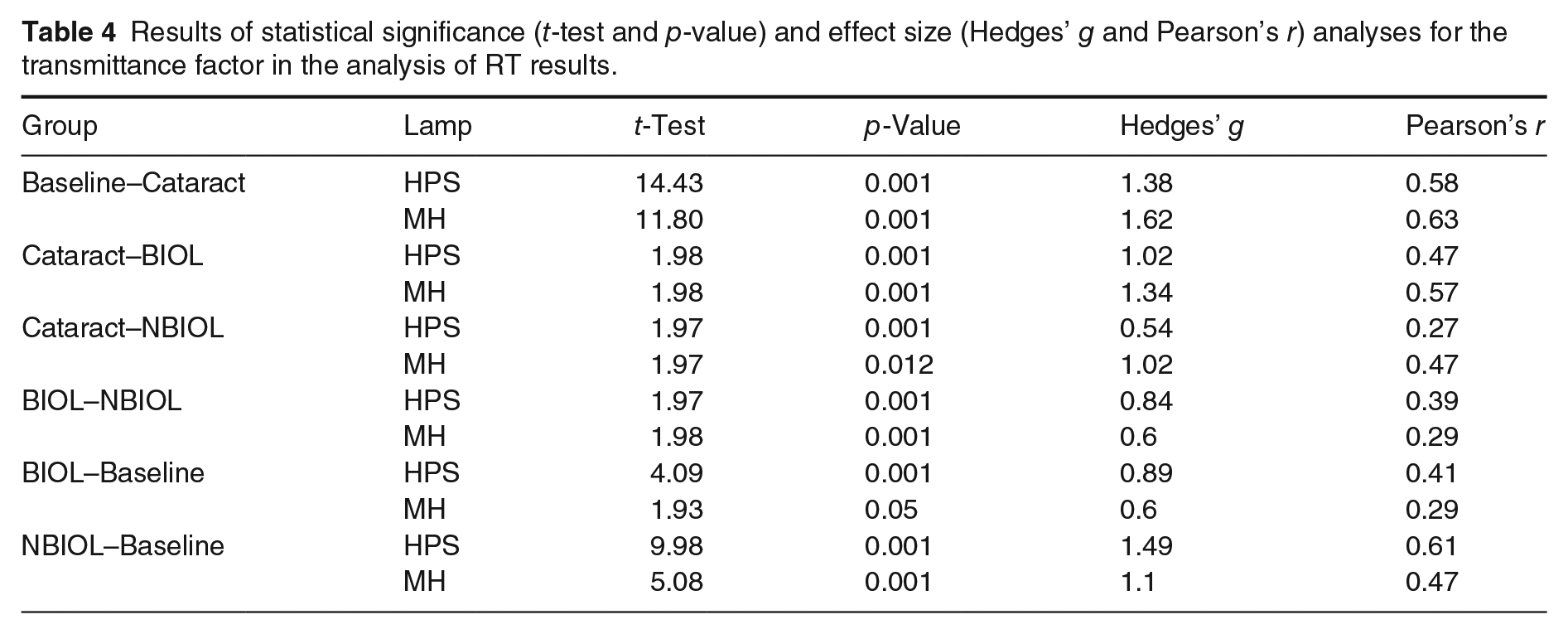
When RT is compared between both pseudophakic groups, RT is found to be significantly lower for the BIOL group, and for both lamps. Finally, the results for both groups of IOLs do not resemble those of the baseline group neither for HPS lamp nor for MH lamp. The statistical results for the effect of the transmittance factor on RT are shown in Table 4.
Results of statistical significance (t-test and p-value) and effect size (Hedges’ g and Pearson’s r) analyses for the transmittance factor in the analysis of RT results.
4. Discussion
This work provides new insight into the effect on two driving-related tasks, CT and RT, of the interaction between the spectral power distribution of common street lamps and the transmittance properties of different IOLs. At mesopic levels, the blocking effect of blue light-filtering IOL on light transmission would be more evident under MH lamp, as mesopic sensitivity is more dependent on short wavelengths. 39 However, no detrimental effect of the yellow filter on the results is found for any of the visual tasks analysed, under those experimental conditions representing night driving, including different street lamps.
4.1 Contrast threshold
In the baseline group, CT is lower for MH than for HPS lamp because its higher short-wavelength content strongly activates the blue light-sensitive photoreceptors, rods and S-cones, a finding already reported in the literature.14–16,32 On the other hand, cataract causes the formation of a veil overlaid on the retina 40 that reduces the contrast of the retinal image, resulting in increased CT. In addition, two factors should be considered. Firstly, the wavelength dependence of the opacity and the resulting scattering has an additional negative effect on retinal image for MH lamp due to its higher short-wavelength content. 41 Secondly, the density and sensitivity of rods decrease with age,42,43 which, although less noticeable in off-axis vision, have been corroborated from a psychophysical point of view. As for the cones, their density and sensitivity remain more stable with age for the eccentricity used in this work. 44 This leads to a greater worsening in detection for MH than for HPS lamp, compared to the baseline group, giving similar results between lamps. Cataract surgery is responsible for the decrease in CT for both pseudophakic groups regardless of the type of lamp due to increased light transmission and reduced scattering, which enhances the quality of the retinal image. 19 The expected spectral transmittance after surgery resembles that of the baseline group. In the case of the BIOL group, CT is not influenced by the type of lamp. This could be due to the reduced short-wavelength transmission through the yellow filter, a similar effect to that produced by a cataract, but without the decrease in light transmission caused by the opacity. With regard to the NBIOL group, CT is lower for MH lamp than for HPS lamp due to a greater excitation of rods and S-cones. A difference already found in the literature when comparing traditional street lamps that differ in their S/P ratio. 45 For the lowest of the illuminances studied (0.2 lx), they found that obstacle detection in elderly subjects improves as the S/P ratio increases. However, of particular relevance is the comparison of the results of the pseudophakic groups for each lamp separately, finding no differences on CT. Hence, although theoretically a higher CT should be expected in the BIOL group for MH lamp, given the presence of a yellow filter, it does not seem to have such an effect. One possible explanation could be the geometry, an aspheric IOL improves mesopic contrast sensitivity at low spatial frequencies by inducing negative spherical aberration and thus reducing the total spherical aberration compared to a spherical IOL. 46 This reduction of aberrations in the BIOL group over the NBIOL group could explain the absence of differences.
Finally, the relationship between CT for the pseudophakic groups and the baseline group is justified. Results for HPS are similar among the three groups of subjects, this can be justified from two points of view. Firstly, Crassini et al. 47 find that contrast sensitivity is similar for young and healthy old subjects at low spatial frequencies similar to our test (0.5 cpd). Secondly, the reduced effect of aging on the density and sensitivity of L- and M-cones would help to justify this result. 43 On the other hand, for MH lamp CT is higher for the pseudophakic groups than for the baseline group, probably due to the yellow filter (BIOL group), the IOL design (NBIOL group) and rod aging. As at the low light levels such as the one used in this work, an old subject requires more short-wavelength light photons to reach the CT value of a young subject.48,49
4.2 Visual RT
No lamp effect is found in the baseline group. Perhaps the repeated presentation of a single supra-threshold contrast is easier to perform in young subjects than the random presentation of values closed to the threshold region, which may reduce the influence of external factors such as the type of lamp. This finding is contrary to the literature, perhaps because Lewis 10 assesses recognition RT, a different task to the one studied in this work. Meanwhile, Akashi et al. use a more temporal retinal eccentricity in their measurements (15º and 23º), so that the rod density is higher. In addition, the S/P ratios of their lamps (HPS: 0.62; MH: 1.53) are 27% more different from each other than those used in this work (HPS: 0.49; MH: 1.17). Finally, the argument concerning the weight of the visual component in RT when using close-to-threshold contrasts justifies to a large extent the differences found with respect to the work of Vicente et al. 18 using LEDs. On the other hand, the increase in RT observed in the cataract group, in comparison to the baseline group, and the absence of lamp effect are explained by the above-mentioned changes in the light transmission produced by cataract. In addition, the use of a supra-threshold contrast favours the prevalence of the non-visual component of RT over the visual one, reducing the influence of external factors such as the type of lamp. 10 Likewise, changes in light transmission and reduced scattering largely explain the improvement in RT after surgery. 48 In the BIOL group, no effect of the type of street lamp was found, justified by the predominance of the motor component. This argument is equally valid for the NBIOL group, which, despite having obtained a lower RT for MH lamp, the difference is less than 30 ms and the result could be considered clinically irrelevant. When comparing the pseudophakic groups, although significantly lower RTs are obtained for the BIOL group compared to the NBIOL group, the greatest difference between the two groups is 46 ms for HPS lamp. The greater inter-variability of old subjects when performing psychophysical tests, 50 together with the variability of RT as a visual task, 46 could contribute to explain the difference.
Finally, the comparison of the RT results of pseudophakic groups with those of the baseline group evidences the existence of an age-related slowdown in central sensorimotor processing that affects the non-visual component of RT. 51
4.3 Limitations
In order to assess the impact of the findings on daily life, the question arises as to how far the results could be extrapolated to real-life conditions. The Maxwellian view setting presented two major differences compared to natural viewing conditions: monocular vision and a difference between the effective and real pupil at mesopic illumination levels. Firstly, no evidence was found for the relationship between binocularity and the effect of spectral power distribution. Secondly, the image of the light source in the plane of the subject’s pupil was a 2.5-mm diameter circle. This being the rough size of a typical senile miosis of an old subject, but not the case for a young subject, with an expected pupil diameter of 7 mm, approximately. The influence of pupil size on contrast sensitivity can be ignored at such low spatial frequencies. 52 However, in terms of retinal illuminance, this change in pupil size would produce an increase in retinal illuminance by a factor of about 8 (7/2.5) 2 . For the baseline group this means a reduction of the measured CT for the HPS lamp and less meaningful for the MH lamp. In either case, it is important to point out that, although the experiment was conducted in a laboratory, which allowed a precise control of the experimental conditions, our results coincide with those previously obtained by other authors under natural viewing conditions. 16 In this work, Uttley et al. 16 find an influence of S/P ratio on obstacle detection under different mesopic luminance conditions.
5. Conclusions
In night-driving conditions, the lower short-wavelength transmission of IOLs with a yellow filter, in comparison to those without yellow filter, does not have a negative effect on two driving-related tasks under the illumination provided by lamps of different spectrum. The presence of age-related cataracts worsens the performance of both measured tasks, especially under the MH lamp due to its higher short-wavelength content. Cataract surgery and IOL implantation enable old subjects to visually perform more efficiently, regardless of the type of lamp and IOL implanted.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.