
Abstract
Adequate illumination plays an important part in providing a healthy environment for nursing home patients with dementia. With increasing awareness of non-visual responses to light, new approaches to quantifying illuminance have emerged. In the present study, we assessed the illuminance in nursing home dementia units in terms of melanopic equivalent daylight illuminance, a metric which aims to quantify the non-visual physiological effects of light by weighing irradiance according to non-visual photoreception. It is among the most comprehensive studies of light conditions conducted in dementia units in terms of melanopic equivalent daylight illuminance to date, and the first to elucidate seasonal differences in melanopic illumination. Light conditions were assessed in all 15 nursing homes with dedicated long-term dementia units in Bergen municipality (60.39°N), Norway, during summer and winter. Results indicated that seasonal differences and gaze direction had some impact on melanopic equivalent daylight illuminance, but most measurements still fell below even conservative recommendations across seasons. The findings indicate a need for additional light sources that can compensate for limited natural daylight in dementia units. The ubiquity of insufficient melanopic equivalent daylight illuminance in dementia units suggests a role for lighting interventions in future research seeking to improve entrainment, sleep and mental health of dementia unit residents.
1. Introduction
Exposure to light has important regulatory functions, affecting numerous aspects of human health and behavior, such as sleep–wake behavior, cognitive performance and mood. 1 Illumination is therefore an important aspect of the indoor environment, particularly for people who spend most or all of their day indoors, such as patients in dementia units. Many of the non-visual effects elicited by light are linked to circadian rhythms; behavioral and physiological cycles of approximately 24 hours that help us anticipate and adapt to the changing demands of our environment. In mammals, circadian rhythms are adjusted (‘entrained’) daily by external stimuli, especially daylight.2,3
The retina contains a specialized type of non-visual cell, the intrinsically photoreceptive retinal ganglion cell (ipRGC) that projects directly to the hypothalamic suprachiasmatic nuclei, the master clock, 4 as well as other targets, eliciting circadian entrainment as well as acute effects on mood and alertness1,5,6 in response to retinal illuminance. The ipRGCs receive input from rods and cones, but also have the ability to detect light independently via the light sensitive photopigment melanopsin.7–9 Collectively, the effects of light that are independent of the visual perception of our environment (image formation) are referred to as non-visual, or non-image forming, responses.1,10
Maximal non-visual responses, such as melatonin suppression, increase in core body temperature and alertness, are elicited by short wavelength light (about 460–490 nm).11–15 Other factors such as the timing, illuminance and duration of the light stimulus will also determine the response. 16 In addition, the response partly depends on light exposure history of the individual. 2 Research suggests that an adequate day–night light contrast is necessary to establish a well-adjusted circadian rhythm (i.e., ensuring sleep at night and wakefulness during daytime). Low illuminance during the day may result in sensitization to the disruptive effects of light at night, whereas high levels of daytime illuminance may protect against this.2,17,18
Ageing leads to changes in eye physiology, such as reduced lens transmission and decreased pupil size. By the age of 45 years, circadian photoreception is half that of a 10-year old, and at 95 years it is 10 times lower. 19 Paradoxically, studies have found that older individuals, particularly nursing home patients, are exposed to far less bright light than younger people.20,21 For nursing home patients, poor lighting has been associated with an increased risk of falls,20,22 which is a common cause of severe and sometimes fatal injury. 23 Furthermore, circadian disruption is implicated in a wide range of health outcomes, including mental disorders and sleep problems.24–26 Sleep problems are common among nursing home residents 27 and people suffering from dementia, 28 and have been linked to increased morbidity and mortality, cognitive decline 29 and additional symptoms such as agitation, hallucinations, depressed mood and disturbed appetite.30,31 Studies have found that exposure to bright light can improve sleep and entrainment of circadian rhythms, 32 as well as ameliorate aggressive behavior and depression33–35 in people with dementia, suggesting that dementia patients are exposed to inadequate levels of illuminance.
Standards for indoor illumination are often intended to ensure visual function and comfort, and vary in terms of the task to be performed and the population. They also typically refer to horizontally measured illuminance on surfaces, whereas the eye is most frequently vertically oriented, and thus receives less direct illumination from overhead light sources. 36 Furthermore, lighting standards are normally expressed as photopic illuminance (irradiance weighted according to perceived brightness for a standard human observer, with a peak in sensitivity at 555 nm) and do not account for the fact that non-visual responses to light are most sensitive to shorter wavelengths (∼480 nm). 15 Although determining the most suitable approach to measuring the non-visual impact of light is a subject of ongoing debate and research, illuminance quantified according to its impact on melanopsin has been shown to be a better predictor than photopic illuminance of non-visual responses such as melatonin suppression 37 and alertness. 38 This quantification has been adopted by the International Commission on Illumination (CIE) in the form of the SI-compliant metric ‘melanopic equivalent daylight (D65) illuminance’ (melanopic equivalent daylight illuminance, EDI), based on previous work by Lucas et al. 39 and Enezi et al. 40 A reanalysis of 19 laboratory studies 41 showed that melatonin suppression, circadian resetting and alerting responses could be accurately predicted by melanopic EDI, supporting its utility as a basis for guidelines. Notably, other metrics have been proposed, such as Circadian Stimulus (CS), which is based on nocturnal melatonin suppression in response to light.15,42
Although the importance of non-visual responses is increasingly acknowledged by international authorities on illumination, research has still not reached consensus with regards to developing standards/recommendations to account for these responses.43–45 Standards, such as those provided by the CIE and the Illuminating Engineering Society of North America (IES) provide recommendations regarding lighting for older people in terms of photopic illuminance of a horizontal surface, reflecting requirements for visual performance.45,46 For these purposes, 200–1000 lx are considered adequate.45,46 The WELL Building Institute recommends 240 equivalent melanopic lx (EML, equivalent to about 217 melanopic EDI).10,43 A previous version of this recommendation was also used as a threshold in a 2018 field study of melanopic illuminance in nursing homes. 47 In addition, the Underwriters Laboratory (UL) 42 gives recommendations in terms of CS. While not directly comparable to the EML, the suggested CS of 0.3 is achieved with an EML of 240 for a variety of common light sources, including daylight. 42 The UL guideline states that 500 lx (photopic) should be sufficient to achieve this CS in 90% of commercially available light sources.
Most previous studies on nursing home illumination have reported threshold values in terms of photopic illumination,20,24,48,49 ranging from 750 to 2000 lx. Consequently, we will relate current results to the melanopic EDI threshold of 217 lx (240 EML) 10 and to two photopic illumination thresholds; 300 lx reflecting the lower end of the CIE recommendation for older people, and 500 lx as it is estimated to satisfy a CS of 0.3 in the majority of cases. 42
Among the few existing studies evaluating nursing home illuminance in terms of non-visual requirements,24,48 most have still reported results in the form of photopic illuminance. One exception is a recent study by Konis, 47 which found that daylit spaces in dementia care facilities offered substantial benefits in terms of higher equivalent melanopic illuminance, with gaze direction and proximity to windows making a significant difference. These findings were measured on clear mornings in Southern California, representing conditions that are not comparable to typical environments further away from the equator, for instance in Northern Europe. Furthermore, seating arrangements and activities are not necessarily situated in ways that prioritize light exposure.
Consequently, we wanted to investigate melanopic EDI in Norwegian dementia units as it is likely to be experienced by a resident on a typical day and at a representative position relative to windows. We also wanted to evaluate seasonal variations, and the capacity of installed electric light independently to produce illuminance above recommended thresholds. Specifically, we aimed to: (i) assess the contribution of seasonal variation (measurement occasion) and physical orientation (window/non-window) to the illuminance in nursing homes; (ii) assess the amount of illumination provided by electric light sources in the absence of natural light, and thus the capacity of the current electric lights to compensate during the darkest winter months; and (iii) compare measured illuminance with recommended thresholds for indoor lighting.
2. Method
2.1 Setting
Managers at all public nursing homes in Bergen municipality were asked whether they had a dedicated dementia unit for long-term care. All those who answered affirmatively (n = 15) also agreed to allow us to measure illuminance at their facilities, and the units in question were consequently included in the present study. As most nursing homes in Norway are public, and typically situated in both old and new institutional buildings, the 15 units arguably yielded a representative sample. In the eight cases where the nursing home had multiple dementia units, one was selected using random assignment in SPSS. 50 The assessments were restricted to the living room. Although the measured illuminance may not be equal to that of the patients’ bedrooms, bathrooms and hallways, we selected the living room as it is the space most frequently occupied by the patients during daylight hours. Furthermore, bedroom illumination may be subject to high variation due to placement of private furnishings such as lamps and curtains, as well as patient preferences.
2.2 Procedure
Illuminance was measured using the GL Spectis 1.0 T Flicker spectrometer by GL optic. The spectrometer has a spectral range of 340–780 nm, and a frequency range of 0.1 Hz–12.5 kHz. The software used for the corresponding spectral analysis was GL Spectrosoft. Effective illuminances for each of the photopigments, including melanopic illuminance, were calculated according to the α-opic illuminance model using the irradiance toolbox developed by Lucas et al. 39 Melanopic illuminances were converted to melanopic EDI using a factor of 0.9058. Although a spectral correction function based on the age of the observer has been proposed, 43 we opted to report results without this correction, as the age range of patients in dementia units varies considerably.
Measurements were conducted on three occasions: daytime winter, daytime summer and after astronomical darkness. Daytime illuminance was recorded in February 2017 and in August 2018, between 10:00 and 14:00 to stay well within the limits of daylight in winter, and to capture the times at which most patients would be awake and present in the living room according to nursing home schedules. In addition, measurements of indoor illuminance were recorded during winter, after astronomical darkness, i.e. after 18:00 hours at local coordinates 60.393° N 5.3242° E. Daytime measurements were carried out on cloudy days (defined as sky visibly covered by clouds, as confirmed by the weather service) to ensure consistency between the measurements across nursing homes. If dimmers were used, the light was turned to full capacity in order to assess the potential of the electric lights for providing adequate illumination. Although vertical measurements are the focus of the present study, horizontal measurements were also conducted in order to allow for comparisons with previous research and standards which have been reported for this measurement angle. For each nursing home, and on each occasion, measures were taken at seven different positions, amounting to a total of 315 data points.
Figure 1 shows the seven points of measurement at each occasion (three horizontal and four vertical measurements). The horizontal (task area) measurements were taken 0.5 m from the place receiving the most natural light (i.e. the wall with the most windows), 0.5 m from the rear wall and at the midpoint between these. Measurements from the middle and back of the room were averaged to generate one composite non-window assessment, in order to approximate average light exposure in most orientations that were not directly window facing. Measurement points in the dementia unit living rooms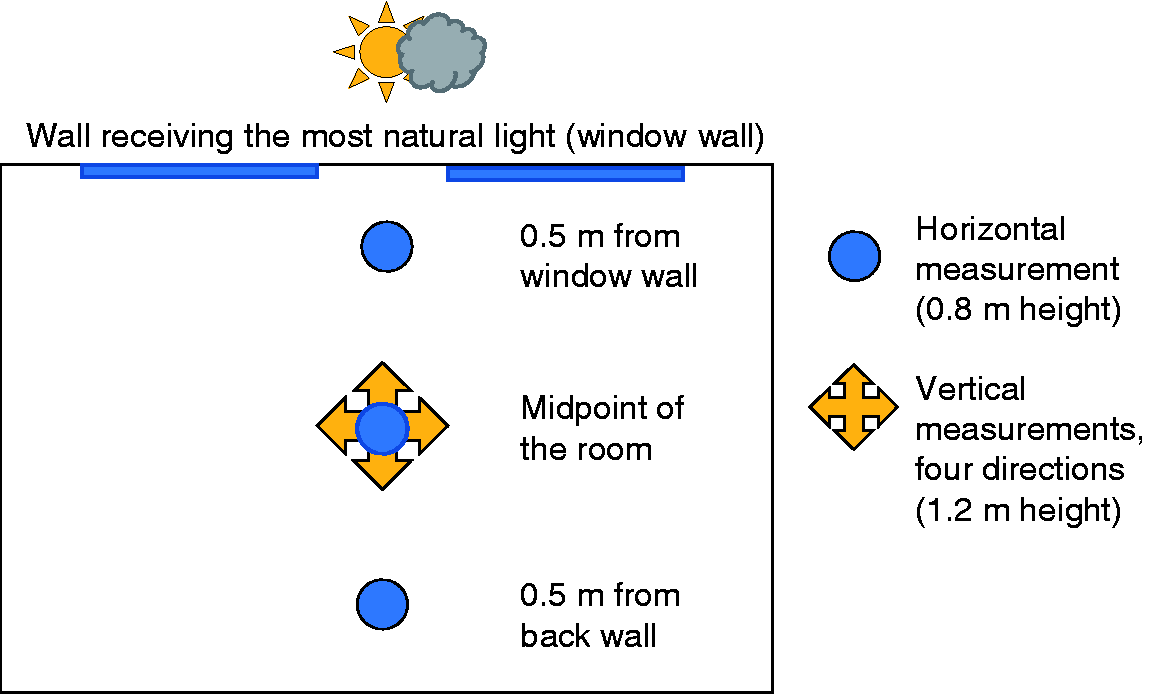
Vertical (corneal) illuminances were measured at the midpoint of the room (equidistant to all corners), in four measurement directions: facing the window, as well as three other directions at 90° steps relative to the window facing measure. The three non-window facing directions were averaged to create one inward facing variable. The height of the vertical measurement was chosen to approximate corneal illuminance of a seated resident (1.2 m above the floor), and horizontal measurements were taken at the typical height of reading or other visual tasks (0.8 m above the floor).
2.3 Data analysis
Statistical analyses were conducted using the statistical software R, 51 with vertically measured melanopic EDI as the dependent variable.
To assess the impact of season and gaze direction on vertical (corneal) illuminance, a multilevel regression model was fitted using lme4, 52 with random intercepts for each nursing home (N = 15) to account for repeated measures at the same locations. The final model was fitted using restricted maximum likelihood (REML) estimation. Two highly influential points were identified and removed based on a criteria of Cooks D above 1 and/or studentized residuals above 2. 53 Due to a highly non-normal error distribution, the dependent variable (melanopic EDI) was log-transformed. It was also standardized to have a mean of 0 and a standard deviation of 1, for the ease of interpretation.
3. Results
3.1 Descriptive statistics
Illuminance in 15 dementia unit living rooms, by measurement angle, occasion, and orientation relative to windows
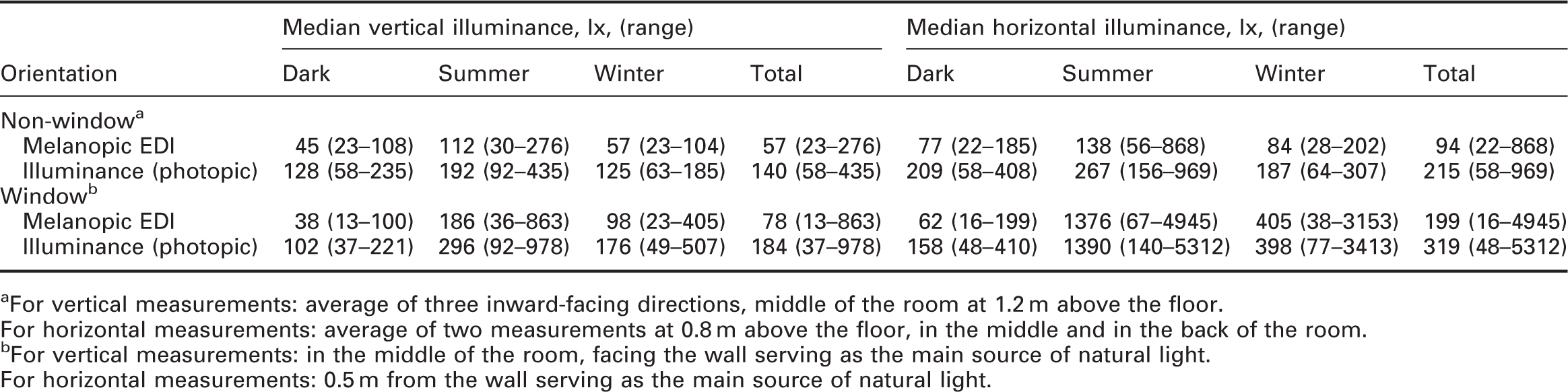
aFor vertical measurements: average of three inward-facing directions, middle of the room at 1.2 m above the floor.
For horizontal measurements: average of two measurements at 0.8 m above the floor, in the middle and in the back of the room.
bFor vertical measurements: in the middle of the room, facing the wall serving as the main source of natural light.
For horizontal measurements: 0.5 m from the wall serving as the main source of natural light.
Vertical (corneal) melanopic EDI in the middle of the room facing inward ranged from 23 to 108 (median = 45) after astronomical darkness, 30–276 in summer (median = 112), and 23–104 (median = 57) in winter. The mean correlated color temperature of the composite vertical measurements (all directions) was 3212 K in winter, 3761 K in summer, and 2737 K after astronomical darkness. Figure 2 shows example spectrometer outputs from the data collection, illustrating the differences in light composition between natural daylight and indoor measurements. They show irradiances at each wavelength (y-axis on different scales to enable visibility of the indoor measurement). Typical spectral power distributions for (left) outside during winter on a cloudy day (4997 lx, 6908) and (right) inside dementia unit living room (25 lx, 2745 K), both in February. This shows irradiance (mW/m2) at different wavelengths (nm). Shorter wavelengths (∼480 nm) are more effective at eliciting non-visual responses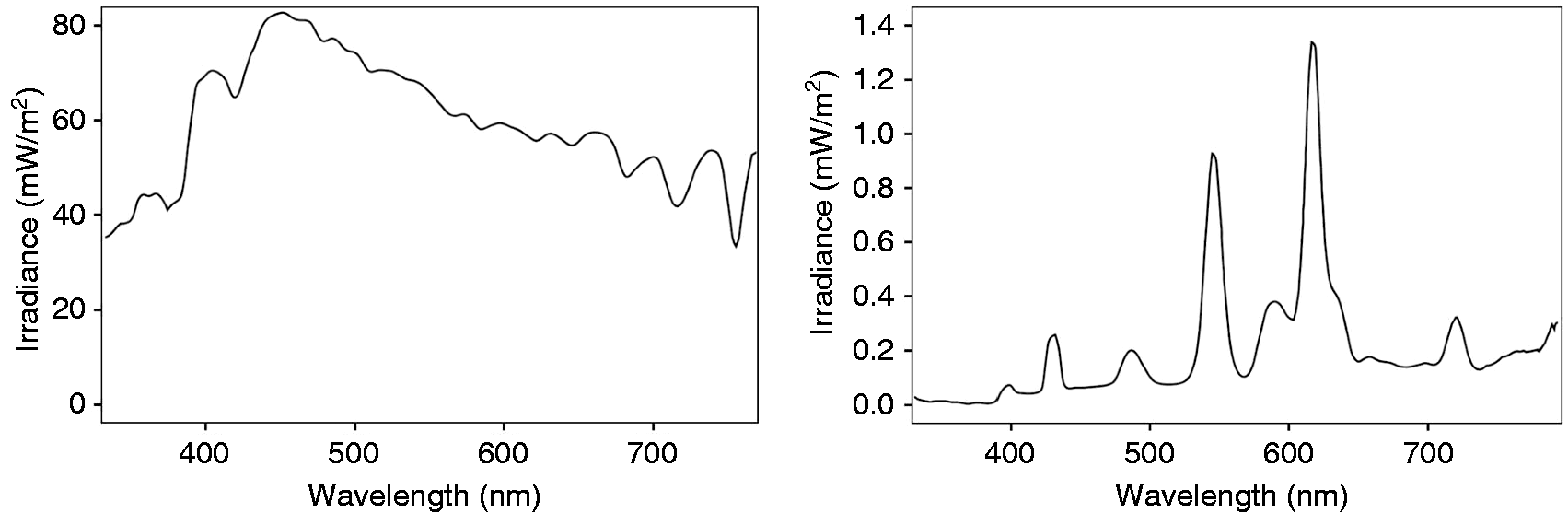
3.2 Multilevel regression – seasonal variation and gaze direction
Multilevel regression model testing the effect of occasion (season) and gaze direction on illuminance at eye level
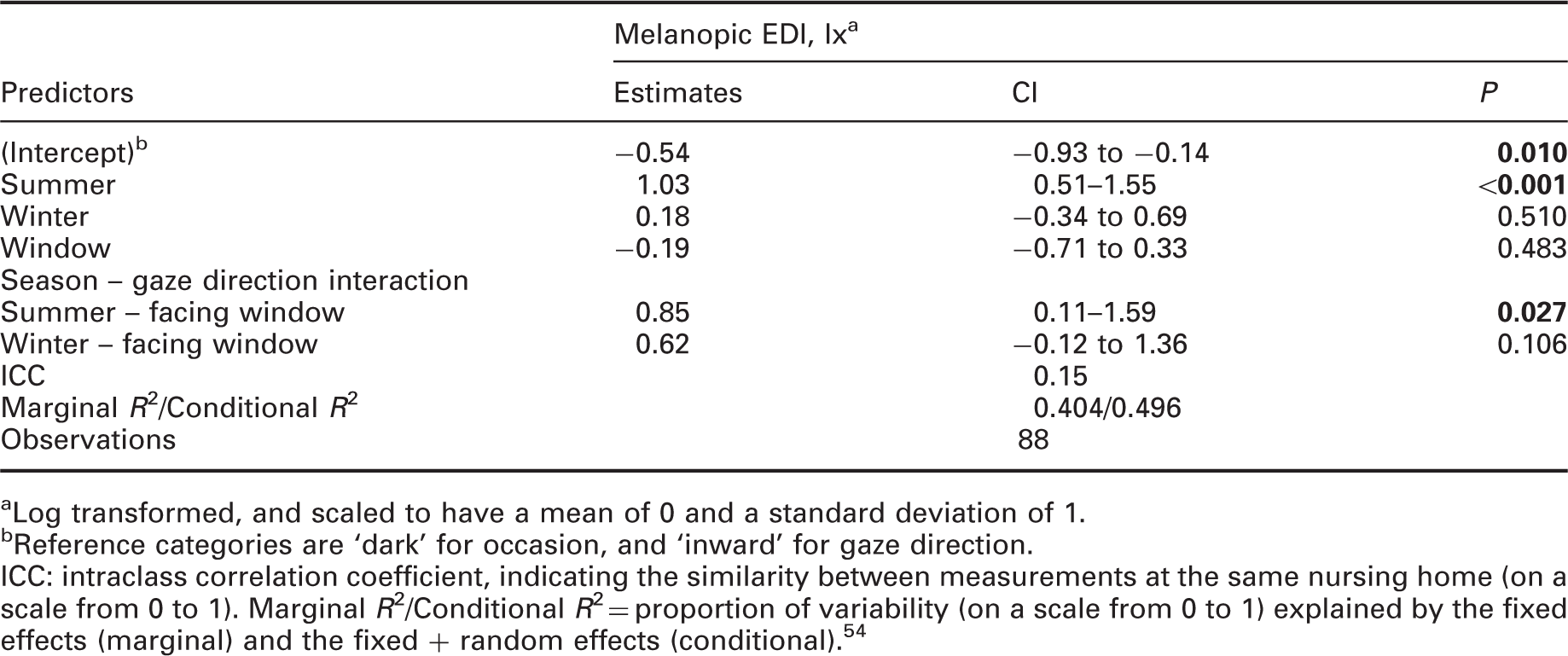
aLog transformed, and scaled to have a mean of 0 and a standard deviation of 1.
bReference categories are ‘dark’ for occasion, and ‘inward’ for gaze direction.
ICC: intraclass correlation coefficient, indicating the similarity between measurements at the same nursing home (on a scale from 0 to 1). Marginal R2/Conditional R2 = proportion of variability (on a scale from 0 to 1) explained by the fixed effects (marginal) and the fixed + random effects (conditional). 54
The reference categories in the multilevel regression model were ‘dark’ (night time, electric illuminance only) for occasion, and ‘inward’ (not facing a window) for gaze direction. For the inward facing measurements, melanopic EDI during daytime in summer (median = 112) was significantly higher than the dark (median = 45) condition (B = 1.03, CI = 0.51–1.55). Melanopic EDI during daytime in winter (median = 57) was not significantly higher than the dark (median = 45) condition (B = 0.18, CI = −0.34 to 0.69). Thus, for inward facing measurements, the day–night difference was only significant during summer. The season × gaze direction interaction was significant for measurements taken during summer, at which point the median melanopic EDI was 74 lx higher for window facing (median = 186) compared to non-window facing (median = 112) measurements (B = 0.85, CI = 0.11–1.59). The corresponding difference of 41 lx in winter was non-significant. Figure 3 shows a box plot of melanopic illuminance at different occasions and gaze directions. Influence of gaze direction and occasion on illuminance (in melanopic EDI)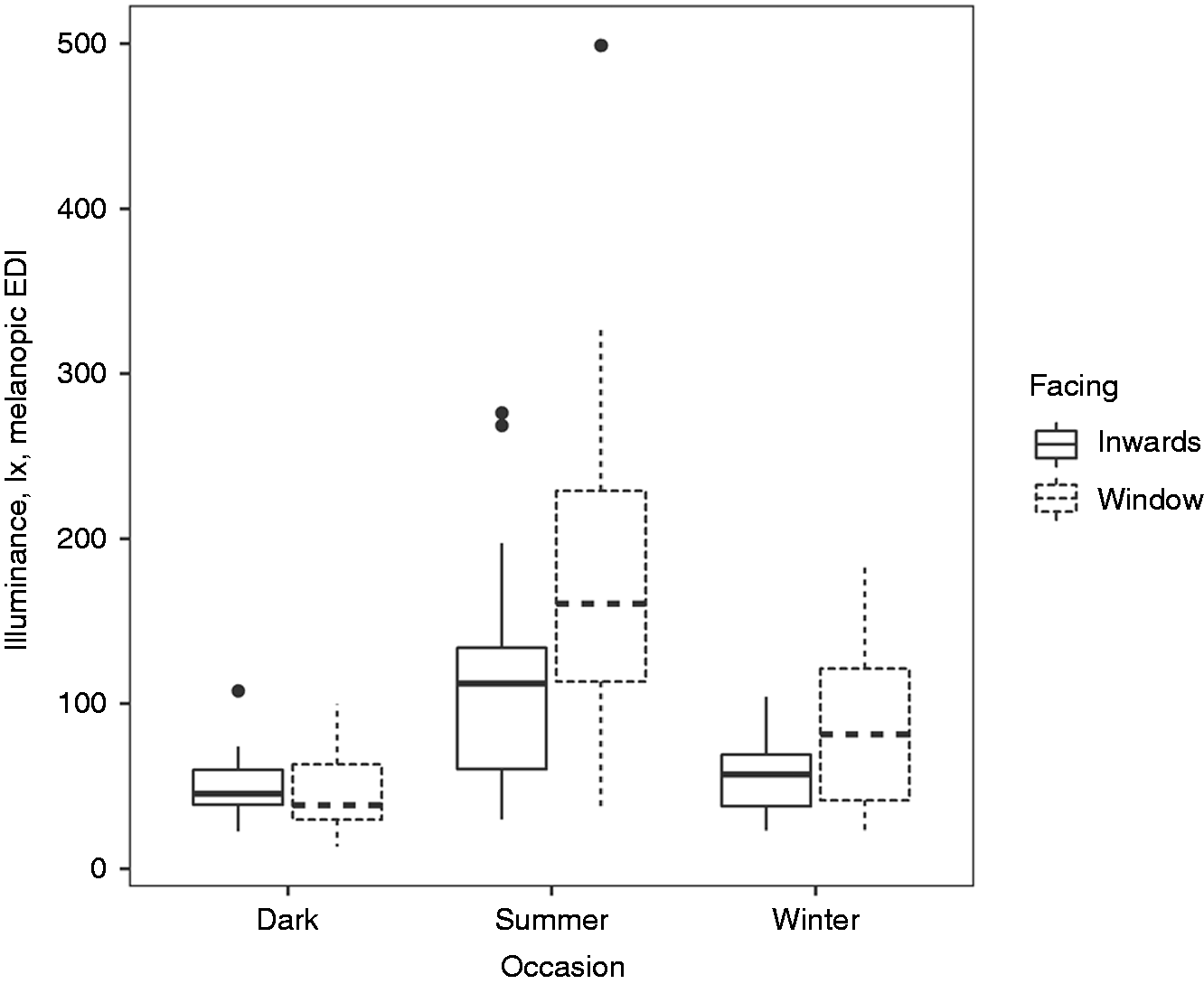
The intraclass correlation coefficient (ICC) is interpreted as the proportion of the variance that can be attributed to group-level variance, on a scale ranging from 0 (no similarity between scores from the same nursing home) to 1 (all variance accounted for by differences between nursing homes). 55 The ICC of .15 indicates that only 15% of the unexplained variance was due to differences between nursing homes.
3.3 Comparisons with thresholds and standards
Number of nursing homes, out of 15, achieving specified illuminance levels measured vertically a
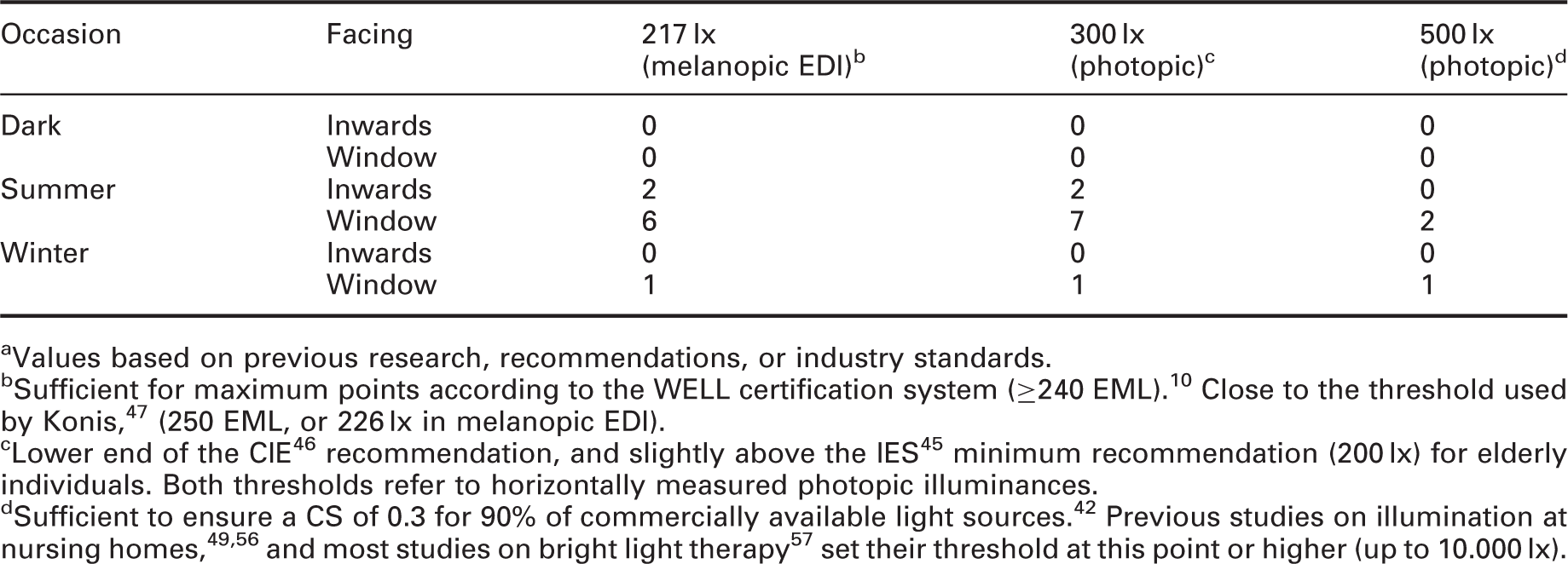
aValues based on previous research, recommendations, or industry standards.
bSufficient for maximum points according to the WELL certification system (≥240 EML). 10 Close to the threshold used by Konis, 47 (250 EML, or 226 lx in melanopic EDI).
Of the inward-facing measurements, only 2 out of 15 nursing homes exceeded 217 melanopic EDI during summer, and none during winter. Of the window-facing measurements, six reached 217 melanopic EDI in summer, and one in winter. Only window-facing measurements reached the photopic illuminance threshold of 500 lx; two of these in summer and one in winter. Higher thresholds were not included in the table, as only one measurement (during summer, facing the window) reached 750 lx. After astronomical darkness, none of the measures reached even the lowest thresholds, suggesting that none of the installed electrical lights could independently provide illumination above these thresholds without the presence of natural light from windows.
Across all occasions, the median horizontal (task area) photopic illuminances in the middle and back of the room were below 300 lx. However, in the window zone it exceeded this in daytime both during summer and winter (see Table 1).
4 Discussion
Melanopic illuminance at eye level in nursing home dementia units was partly dependent on seasonal variations and gaze direction, although differences were small. The electrical lights were not capable of independently providing sufficient melanopic illumination in the absence of natural light, and the absence of day–night differences in winter suggests that very little natural light reaches the inside environment even during the day. Almost all measurements, regardless of direction and measurement occasion, were below even conservative industrial standards and thresholds recommended for eliciting non-visual responses to light, also during summer.
Measurements during winter were lower than corresponding summer measurements, and facing the window in the center of the room increased melanopic illuminance significantly only during summer. The absence of a significant day–night contrast in melanopic illuminance during winter suggests that the amount of natural light available in central room positions during winter is negligible, highlighting the need for electric lights capable of independently producing sufficient melanopic illuminance. Current electric lights only produced a median of 45 melanopic EDI, or 128 lx (photopic) when turned to their maximum capacity in the absence of daylight (after astronomical darkness), which is about 172 melanopic EDI below the recommendation of the WELL Building Standard, 10 or 172 and 72 lx (photopic) below the minimum horizontal illuminances recommended by CIE 46 and IES 45 respectively. The lack of day–night contrast observed in melanopic EDI during winter is suggestive of an absence of a reliable time signal for circadian entrainment.
4.1 Comparisons to standards and predetermined thresholds
Only two inward-facing measurements reached 217 melanopic EDI (Table 3), none of these during winter. None of the measurements conducted after astronomical darkness reached any of the recommended thresholds. Even the highest median vertical illuminance achieved (186 melanopic EDI or 296 lx), directly facing the window during summer, barely exceeds the lowest recommended thresholds.10,45,46 Thus, even when windows are present, the amount of light that actually reaches the inside environment for a resident seated in the middle of the room on an overcast day is too low. This was consistent across all locations, with only about 15% of the unexplained variation attributable to random differences between nursing homes (e.g. room size, the number of windows, location and orientation of the building, choice of indoor light fixtures, etc.). Based on our findings, it is therefore reasonable to conclude that nursing home patients do not receive light cues sufficient for entrainment of circadian rhythms regardless of gaze direction, especially in winter.
Of the horizontal measurements, window adjacent measurements during summer and winter were the only two conditions in which median light levels exceeded the minimum recommendation of 300 lx for horizontal photopic illuminance. 46 It is therefore likely that the illuminance available to perform visual tasks is also too low if seated in the back or the middle of the room, and at times when daylight is limited.
Higher illuminance than what is reported here will naturally occur on days of more direct sunlight, or if sitting very close to a window looking out. For most nursing home patients, however, especially in the Northern hemisphere during winter, it is likely that the vast majority are exposed to even lower levels of corneal illuminance, for instance due to sitting far back in the room, short day lengths (mid-winter), daytime napping, eye placement lower than 1.2 m or gazing in a downward direction. During the darkest period of the year (December/January), the period of daylight lasts only for about 6 hours (09:45–15:45) at the local coordinates (60.393°N 5.3242°E). Furthermore, we utilized conservative thresholds, not accounting for eye disease, degenerative conditions affecting neural signaling, or very advanced age, which may impact illuminance requirements. In any standard that is not adjusted for age, the illuminance will probably have to be at least doubled for elderly individuals to account for age related loss of retinal sensitivity 19 and reduced responsivity to short wavelength light. 58
It should be noted that the thresholds used for comparison in the present study are merely of suggestive nature. While there are a number of studies suggesting that high illuminances and shorter wavelength light are more effective at stimulating non-visual responses, 59 there is no consensus concerning the amount or composition of light that is an appropriate minimum for nursing homes. The efficacy of light in stimulating non-visual responses depends on multiple factors, including timing and duration of the light stimulus, 16 as well as previous light exposure history and individual differences. 17 Setting appropriate standards for nursing homes will require knowledge about the effects of absolute and relative illuminance, timing and light composition, in terms of both acute and delayed responses. The levels of adjustment needed for ageing individuals and patients suffering from dementia in terms of non-visual responses also need to be empirically validated, in light of ample evidence that photoreception becomes significantly reduced as we age. 19
Adapting a consistent standard for measuring and reporting light is a necessary step in this process, as previous studies on ambient light conditions and research on light therapy seldom report how light was measured (e.g. vertical or horizontal), and have mostly resorted to reporting photopic illuminance. 39 In the present study, we opted for melanopic EDI as a way to account for the wavelength sensitivity of the non-visual responses; however, effective illuminances for other photopigments are reported in supplementary materials (Table S1).
The clinical impacts of insufficient illumination in nursing homes are potentially many and severe. The low light levels described in this paper may impair the ability to perform visual tasks, reduce mobility and increase the risk of falls and injuries.22,23 Conversely, improved lighting conditions may produce improvements in terms of circadian entrainment, sleep, mood and behavioral symptoms.34,60,61
4.2 Strengths, limitations and suggestions for future research
A strength of the present study is that time of day, weather and placement of measurements were standardized across all nursing homes. Measurements were repeated to investigate the effects of seasonal variation. Furthermore, we considered both the photopic and the melanopic aspects of light, as well as various standards, when assessing the adequacy of the indoor illuminance. We measured illuminance at every nursing home with a long-term dementia unit in Bergen municipality, thus ensuring a broad sample across building years, placements and structural variation.
We did not, however, assess the illuminance under different weather conditions, such as direct sunlight. The generalization of the findings to geographical locations with far more sunlight is thus uncertain. Neither did we investigate light at night in the patients’ bedrooms, as it is likely subject to a large amount of individual variation in preferences and habits. However, based on previous research we know that low exposure to illumination during the day can have a sensitizing effect on responses to illumination at night,2,17,18 possibly causing circadian disruption. Furthermore, worn dosimeters allow for more personalized estimates of the illuminance experienced by wearers over time 62 and would be a useful supplement to the present findings about the living environment. Due to the cost as well as potential demands on staff involved in ensuring proper wear and minimizing discomfort, we did not utilize dosimetry in the current study. Important visual aspects of light, such as glare and flicker, were not evaluated in the present study, but should also be considered when designing the nursing home light environment. 45 Increases of illuminance that cause more glare may result in a significant reduction of visual acuity and comfort, particularly for people who have glaucomas. 63 More research is needed to appraise the implications of the light conditions on multiple health factors and well-being among residents at nursing home dementia units. Specifically, future research on light conditions in nursing homes should aim to link the light conditions to circadian rhythm parameters of the resident. The present study suggests there is little natural variation in light levels between nursing homes, seasons or physical orientation/gaze direction. This calls for experimental designs with light fixtures capable of providing a wider range of illuminances. Furthermore, investigations of the ways in which ageing and associated conditions may affect non-visual responses to light would enable us to better estimate the thresholds necessary to ensure circadian entrainment, mental health and well-being.
5. Conclusion
Despite the lack of a definite standard for melanopic illumination, the present study shows that illuminances in dementia unit living rooms are below even the most conservative recommended thresholds, with respect to both visual and non-visual requirements. There was no significant difference between day and night-time measurements in the contribution from natural daylight to indoor illuminance in winter, even when directly facing a window. It is therefore concluded that, overall, there is a need for improved indoor lighting in nursing home dementia units, especially during winter. Given the ubiquity of insufficient illumination, optimization of illumination in the nursing home setting has the potential to better entrain the circadian rhythm and improve sleep and mental health of residents.
Footnotes
Acknowledgements
We would like to thank Bergen municipality and the participating nursing homes for allowing us the opportunity to conduct measurements at their facilities.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Eirin Kolberg and Eirunn Thun received their PhD and postdoc grants from the University of Bergen, while Gunnhild Johnsen Hjetland received her PhD grant from the Research Council of Norway and the City of Bergen.