
Abstract
A surgical luminaire containing two types of phosphor-converted LEDs was employed to illuminate a large midline incision in a 90 kg pig. The PC-LEDs were proportionally blended to create four spectra defined by their approximate correlated colour temperatures: 3000, 4000, 4500 and 5100 K. Sixteen surgeons evaluated the colour appearance of internal anatomy under each spectrum. All four spectra were rated as highly effective. There was no significant difference between the 4000, 4500 and 5100 K spectra. The 3000 K spectrum was rated as less effective, though this does not mean it was ineffective. The spectrum by participant interaction was significant where it could be estimated, suggesting that surgeons may develop individual opinions about which spectra are most effective. While the surgeons moderately agreed that the colour of internal anatomy was altered by the different spectra, they were undecided whether the differences would increase the risk of surgical error or influence surgical decisions. They were also largely undecided whether they would select different spectra during a single procedure, for different procedures, or for different anatomy. Overall, the linear mixing for variable CCT employed in this experiment did not provide obvious utility for surgeons making visual evaluations.
1. Introduction
During many surgical procedures, it is necessary for surgeons to evaluate subtle differences in the visual appearance of internal anatomy. The quality of light provided by surgical luminaires may play a role in providing the visual information necessary for accurate visual diagnosis. Light emitting diodes (LEDs) are overtaking conventional sources – such as xenon, halogen and metal halide – because of their increased efficiency, long lifetime and reduced heat at the surgical site. Their availability in a wide range of spectral power distributions (SPDs) permits the development of spectrally tunable surgical luminaires, where an array of LEDs with distinct SPDs can be mixed to produce a variety of spectra from a single luminaire.
The spectrum of light from a surgical luminaire affects colour contrast and discrimination. Appropriately, engineered spectra have the potential to facilitate visual observations, including the diagnosis of tissue abnormalities. Optimised spectra have been shown to enhance colour difference between tissues of specific clinical interest with well-defined spectral reflectance distributions (SRDs).1–3 Others have optimised spectra for endoscopy,4–8 an imaging technology application that does not necessarily require white light. It is only recently, likely prompted by technological advances in LEDs, that the spectral composition of LED general surgical luminaires has received interest.
One method of adjusting the spectrum of a surgical luminaire is by varying correlated colour temperature (CCT). At its simplest, this is achieved by the linear combination of two types of white phosphor-converted LEDs (PC-LEDs) with individual CCTs near the extremes of the desired CCT range. For this work, a prototype surgical luminaire employing this technique was created, and an experiment was performed to assess surgeons’ (1) perceived ability to effectively evaluate the colour appearance of internal anatomy under a range of CCTs, and (2) interest in utilising a variable CCT surgical luminaire should it be available.
2. Methods
Spectral characteristics
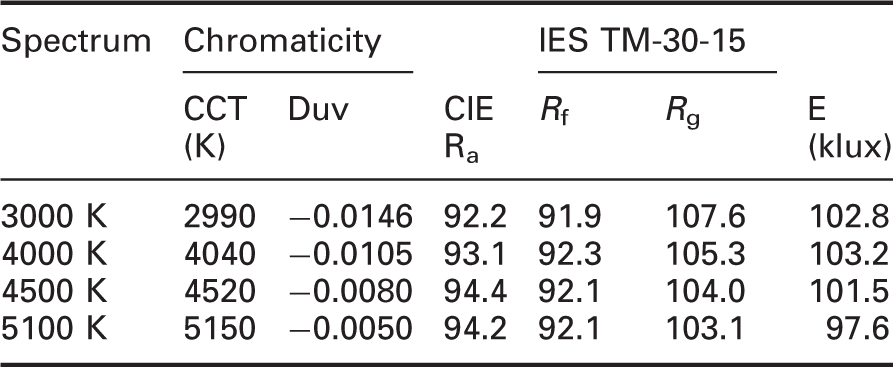
Note: Exact chromaticity defined by CCT and Duv is provided. Duv quantifies deviation above or below the black body locus, with negative values indicating chromaticity below the black body locus. 11 The lower CCTs exhibit lower Duv values, suggesting a relatively increased magenta tint. CIE Ra is a measure of colour fidelity, 10 with a value ≥ 85 required by IEC 60601-2-41. 9 IES TM-30-1512,13 provides an improved measure of fidelity (Rf), a measure of relative gamut size (Rg), and graphics and other supplemental quantities not discussed here. TM-30-15 was developed to address two problems: (1) CIE Ra has flaws that are especially apparent for sources with narrow spectral features, including some LEDs, and (2) colour quality cannot be quantified with any single measure.13,14 All experimental spectra exhibited excellent colour rendering with CIE Ra above 90, IES TM-30-15 Rf above 90, and Rg above 100. Mean illuminance (E) at the surgical site was 101.3 klux, which is typical of open surgery; each condition deviated by less than 4% from the mean. All measurements were taken just above the surgical site.
CCT: correlated colour temperature; CIE Ra: Commission Internationale de l’Eclairage general colour rendering index.
Ethics approval for the experimental design was provided by The Pennsylvania State University Institutional Review Board (study # 00006476). Ethics approval for use of the pig was provided by Case Western Reserve University (CWRU) Institutional Animal Care and Use Committee (protocol # 2014-0048).
2.1 Procedures and participants
The experiment was conducted in a single session at the CWRU Animate Skills Laboratory. A 90 kg sedated adult pig received a large midline incision, exposing the five organs of interest shown in Figure 1: bladder vasculature, colon, omentum, liver and the xyphoid process. CWRU medical staff was present throughout the experiment to monitor the status of the pig, hydrate the abdominal cavity and drain the bladder. These efforts helped limit changes in the visual appearance of internal anatomy during the approximately 9 hours of the experiment.
The pig was situated on a surgical table with a sliding top; surgeons were instructed to move the table horizontally to place organs of interest under the most concentrated light. This allowed the surgical luminaire to remain stationary and at the same vertical distance throughout the experiment, limiting variation in illuminance and shadowing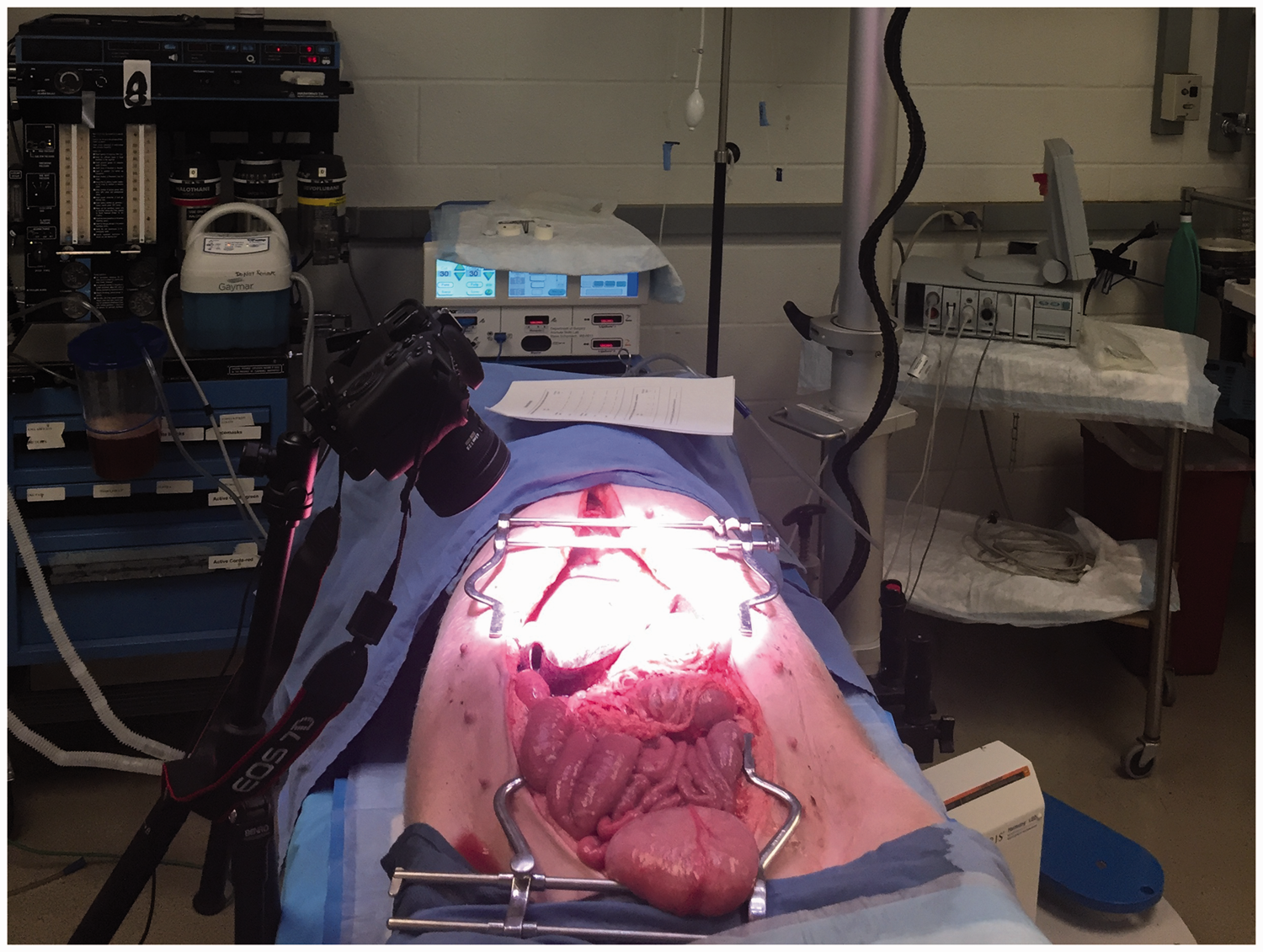
Participants included 12 male and 4 female surgeons, all practicing in the Cleveland, Ohio area and affiliated with Case Western Reserve University and the Cleveland Clinic. Surgical experience ranged from 3 to 38 years (avg. 15 years), with 11 surgical specialties represented (bariatric, cardiac, cardiothoracic, colorectal, general, laparoscopy, oncology, orthopedic, pediatric, thoracic, transplant). Participants were 28 to 73 years old (avg. 46 years) with height from 1.5 to 1.9 m (avg. 1.75 m). Eleven surgeons wore glasses or contacts. All surgeons passed a six-plate Ishihara test for colour vision abnormalities. 15
Upon arrival, participating surgeons reviewed an informed consent document and provided verbal consent. Surgeons were asked to evaluate the pig’s internal anatomy by orally responding to survey questions posed by an experimenter. Each session was completed with a demographic survey. The entire process took about 30 minutes per participant.
A summary of the experimental survey and the means and standard deviations of the responses from the surgeons
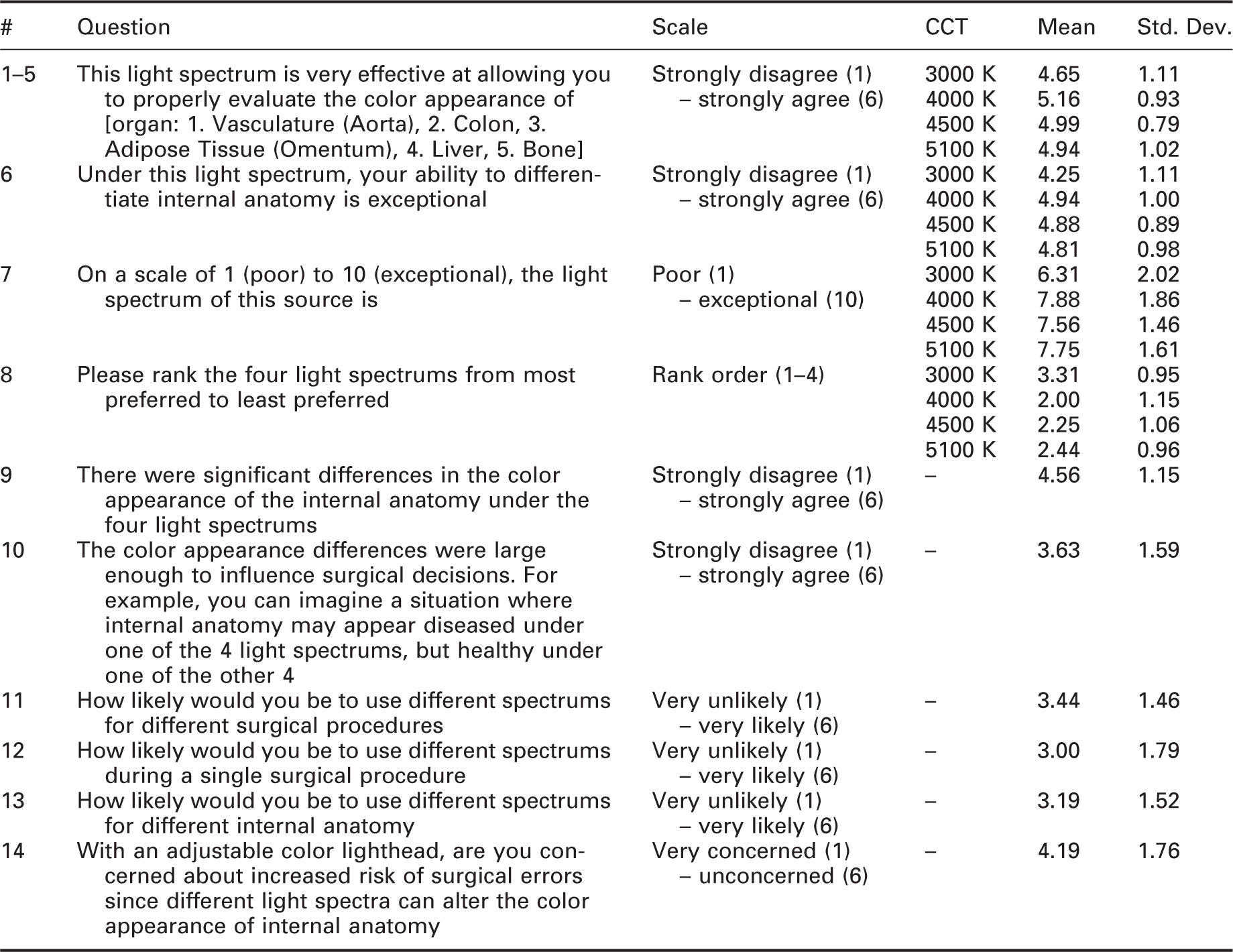
Note: The first section of the survey, composed of questions 1–7, was repeated for each experimental spectrum. The second section, composed of questions 8–14, was given only once for each surgeon.
CCT: correlated colour temperature
2.2 Independent and dependent variables
SPDs were measured using a PR-655 SpectraScan spectroradiometer (Photo Research Inc., Cary, NC, USA) with a 1° field of view aimed at a diffuse reflectance standard (SRT-MS-100, ρ = 99%) (Labsphere North America, North Sutton, NH, USA) mounted on a tripod and positioned just above the midline incision. SRDs were measured by aiming the PR-655 at a portion of each of the five organs that did not contain a veiling reflection. Illuminance measurements were taken using a Minolta T-10 illuminance meter (Konica Minolta, Ramsey, NJ, USA) positioned just above the surgical site. All measurements were taken in the central beam of the surgical luminaire.
In order to simulate an actual surgical environment, overhead fluorescent lighting remained on during the experiment. The effect on chromaticity and colour rendering was immaterial as the fluorescent lamps provided approximately 0.5% of the illuminance at the surgical site. The SPDs reported in Figure 2 include small spikes at 544 and 616 nm, which represent contributions from the overhead fluorescent lamps.
The four experimental spectra comprised spectra from warm and cool white PC-LEDs with small contributions from the overhead fluorescent lighting. These measurements were taken at the end of the experiment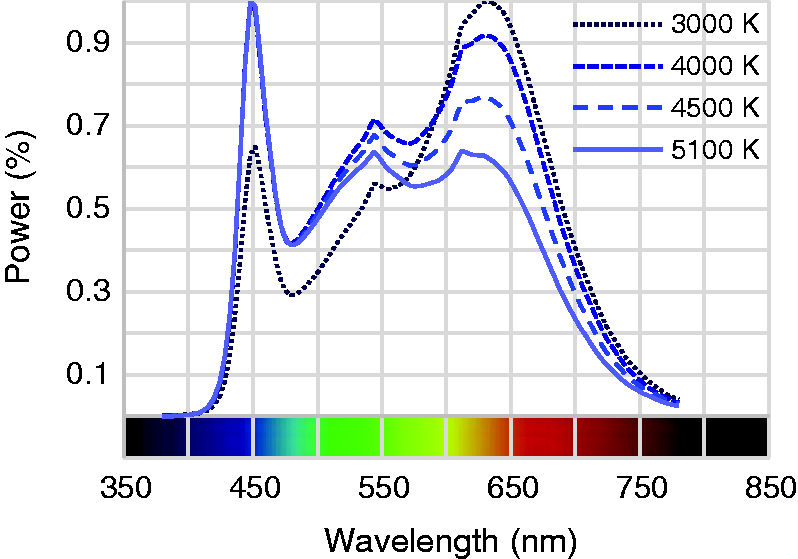
Reflected power distributions were measured from each of the organs at the beginning (morning) and end (evening) of the experiment. SRDs for the organs of experimental interest reported in Figure 3 were produced by dividing the lighting condition out of the measured reflected power distributions. The colour appearance of organs changed from morning to evening and measuring the same location was not possible. Due to this, the morning and evening SRDs should be considered independent measurements of different conditions of similar anatomy.
The measured spectral reflectance distributions (SRDs) in the morning (left) and evening (right). The reported SRDs are truncated above 720 nm, and the morning vasculature SRD was additionally truncated below 390 nm to eliminate measurement errors.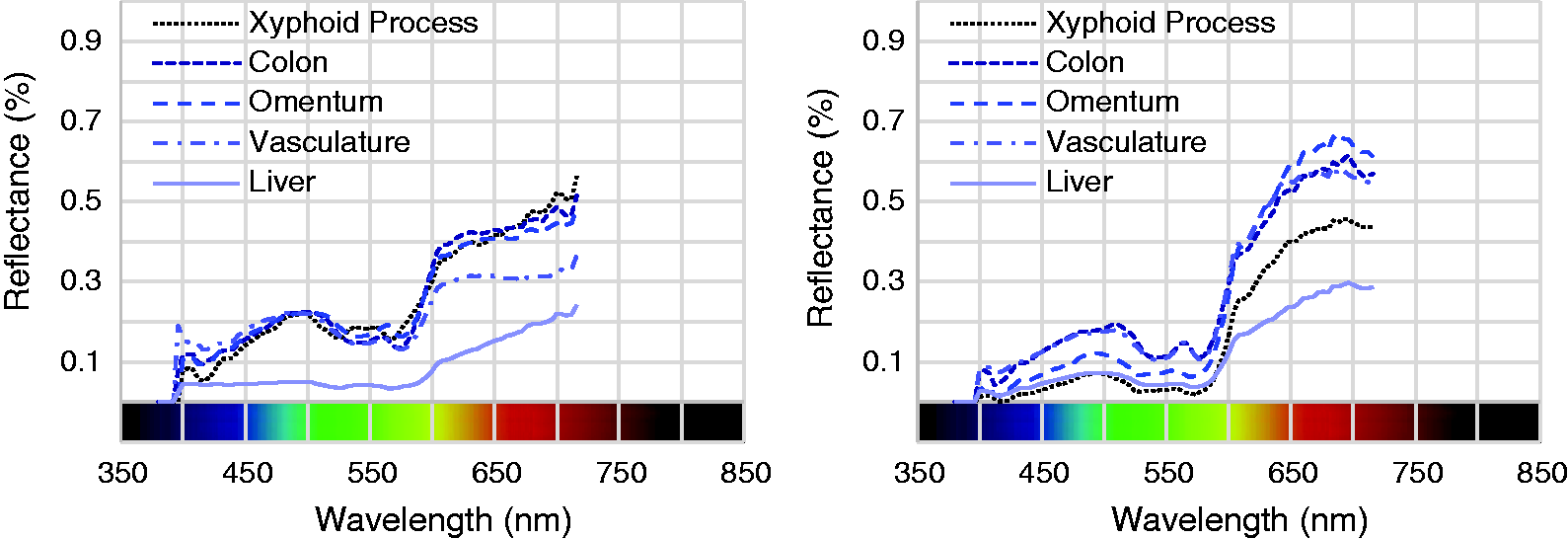
3. Results
Statistical analysis was performed in Minitab 17.1 (Minitab Inc., State College, PA, USA). Surgeons’ evaluations of the colour appearance of the five organs under the four spectra were analysed using a full factorial ANOVA. Spectrum and organ were treated as fixed factors and surgeon was treated as a random factor (because we are interested in all surgeons rather than these surgeons). Organ (p = 0.55) and its interactions were not statistically significant. Spectrum alone was not statistically significant (p = 0.20). The spectrum by surgeon interaction illustrated in Figure 4 was significant (p < 0.001), suggesting that spectrum mattered for at least some surgeons’ evaluations of organs’ colour appearance.
95% confidence intervals for each surgeon by spectrum combination are aggregated from the evaluations of the five organs. Surgeons are ordered from left to right from lowest to highest mean rating across all four spectra. The upper limit of the confidence intervals is truncated to the maximum rating of six. Despite the statistical significance of the surgeon by spectrum interaction, a clear trend is not apparent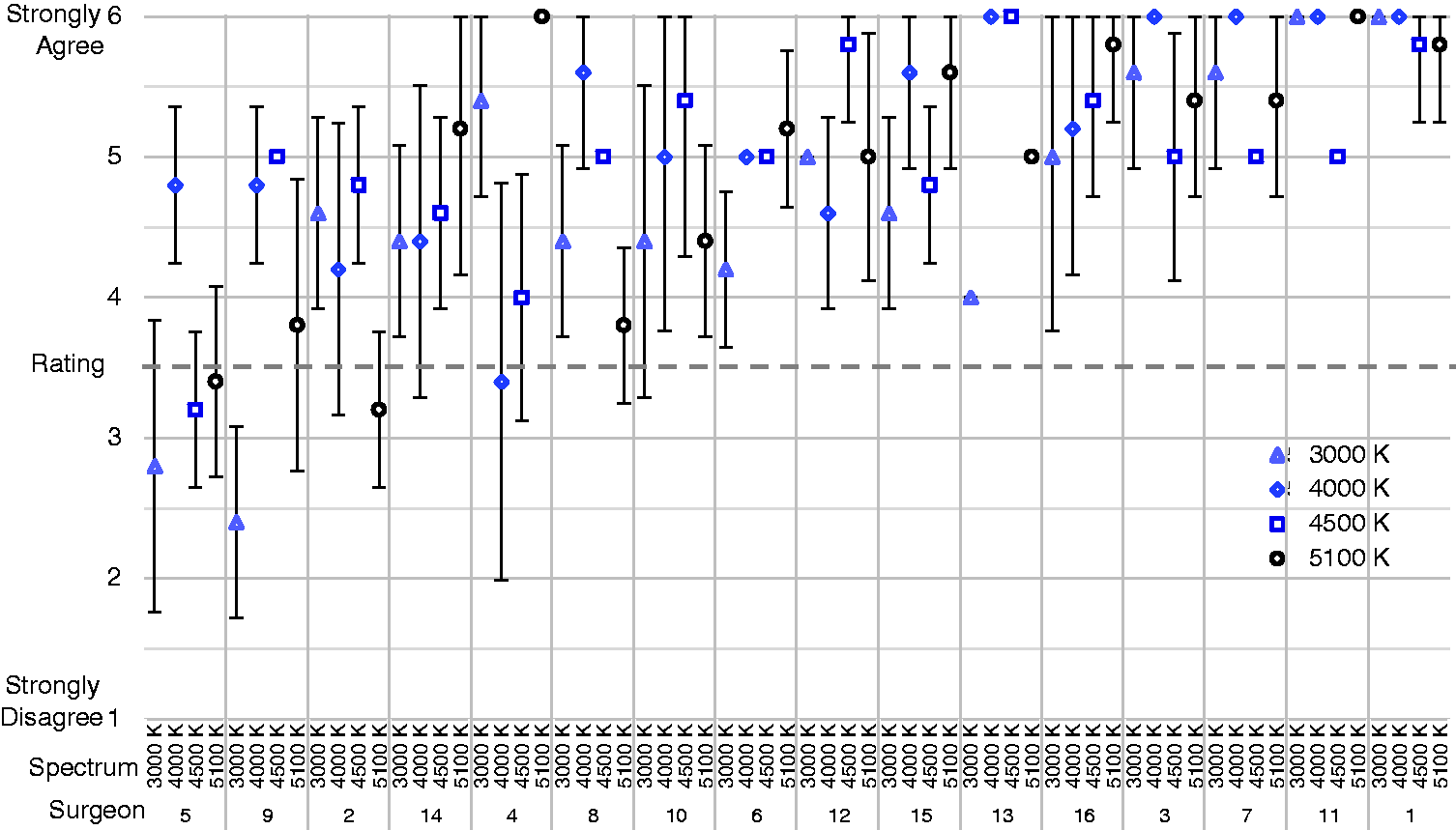
Because surgeon (p < 0.001) and the surgeon by spectrum interaction were statistically significant, demographic correlations were investigated. Gender, age and height exhibited no statistical significance. Surgical specialty (p < 0.001) and the surgical specialty by spectrum interaction (p = 0.03) were statistically significant. The observation order plot revealed no ordering bias, suggesting evaluations did not significantly change over the course of the day, which indirectly suggests that changes in organ appearance throughout the experiment were not large enough to influence evaluations.
Hedge’s g effect sizes for spectrum (Q6)
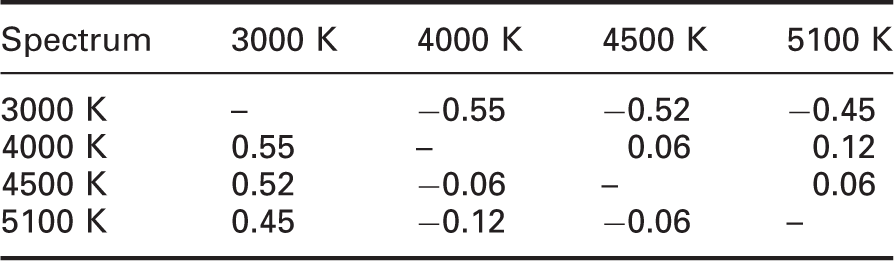
Note: Moderate effect sizes exist between 3000 K and all other spectra. In context with the Tukey intervals, this suggests that 3000 K was rated as less effective than the other spectra, and there was no difference in ratings of effectiveness between the other spectra.
Hedge’s g effect sizes for spectrum (Q7)
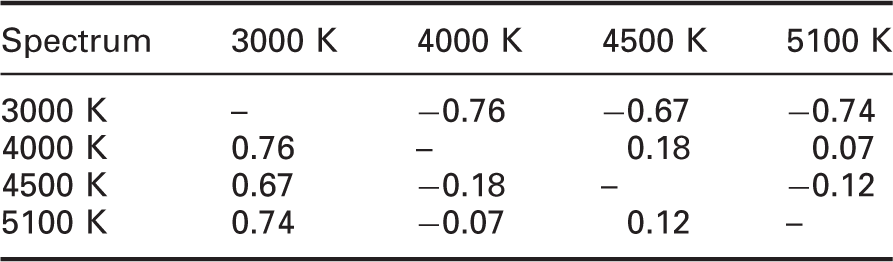
Note: Results are similar to Table 3, though the effect sizes between 3000 K and all other spectra are marginally larger.
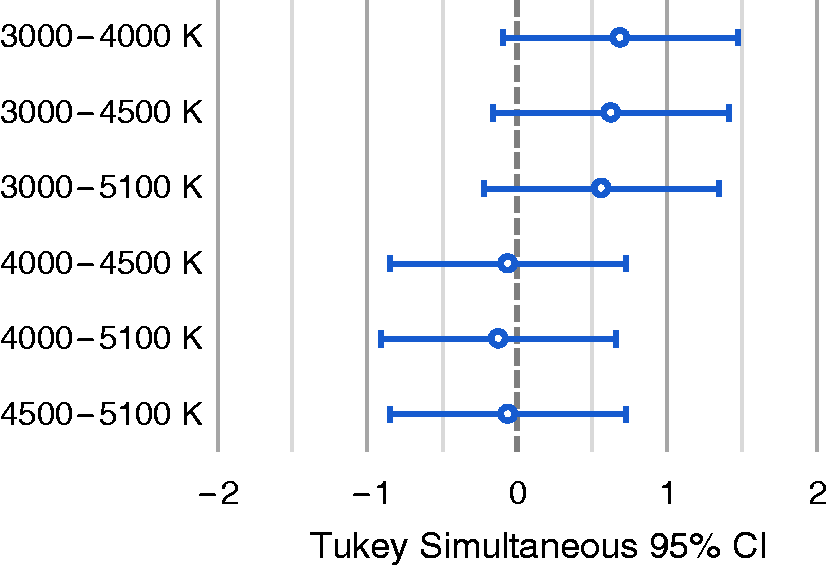
Tukey intervals for spectrum pairs (Q6). At the 95% confidence level, no significant differences exist between experimental spectra; at the 75% confidence level, 3000 K splits off from the other spectra. There were no differences in surgeons’ ratings of effectiveness between any of the other spectra
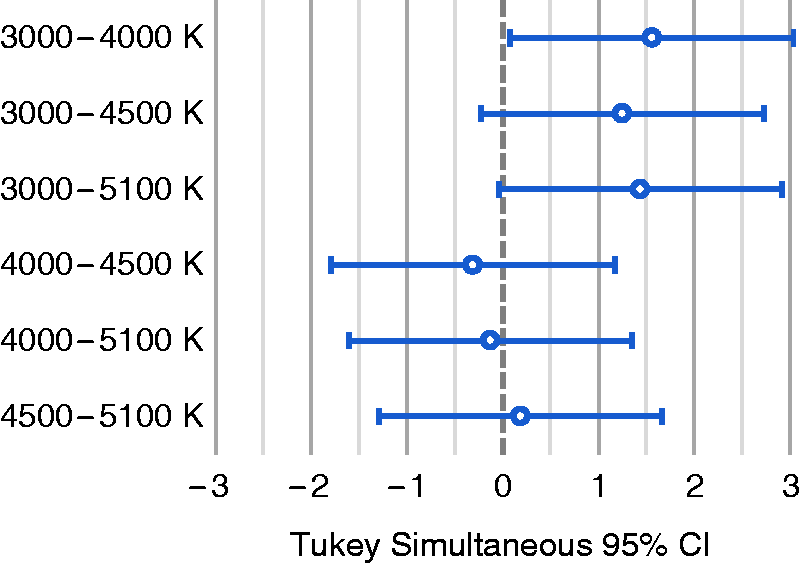
Tukey intervals for spectrum pairs (Q7). At the 95% confidence level, the only significant difference lies between 3000 K and 4000 K; at the 85% confidence level, 3000 K splits off from the other spectra. There were no differences in surgeons’ ratings of effectiveness between any of the other spectra
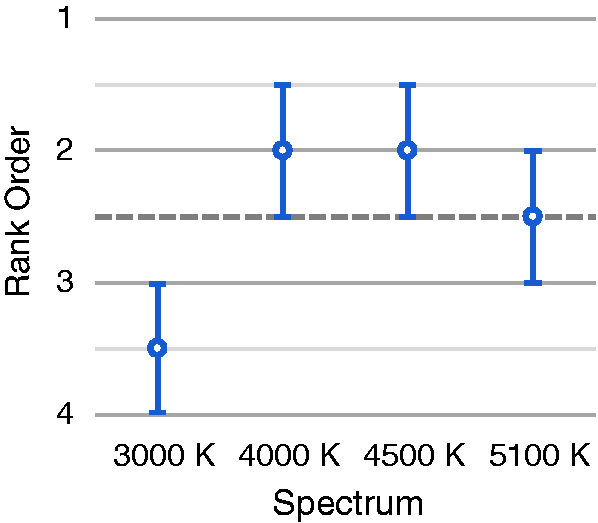
Spectrum rank order (Q8). Ordinal rank order data are inappropriate for analysis of variance because it violates the assumption of independence. The Wilcoxon rank sum test was employed to test for significant difference from the group mean of 2.5. 3000 K was less preferred while the other spectra exhibited no significant differences
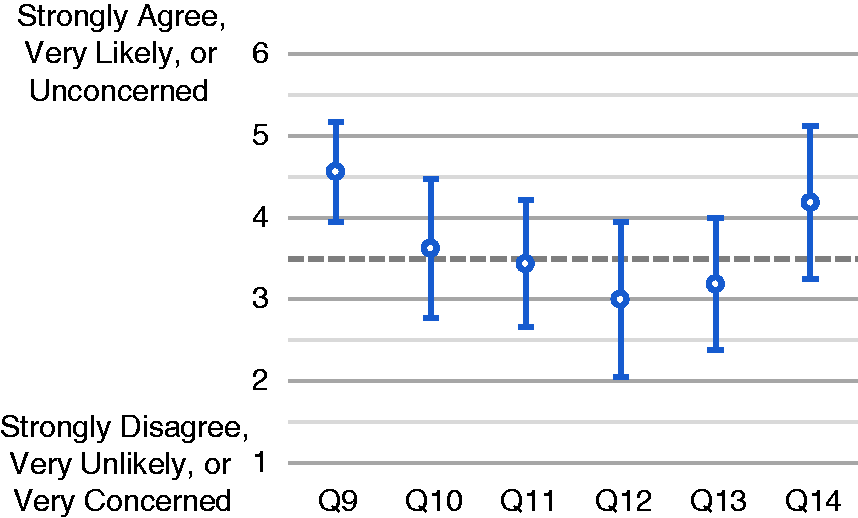
General questions (Q9–14). The dashed line at an average score of 3.5 indicates the midpoint of the scale. Though the semantic scales are only defined at their endpoints (see Table 2), the midpoint of the scale is assumed to represent ‘undecided’. Only question 9 is significantly different from undecided, though the means for questions 12 and 14 are more than half a point different from undecided
ΔEab colour difference
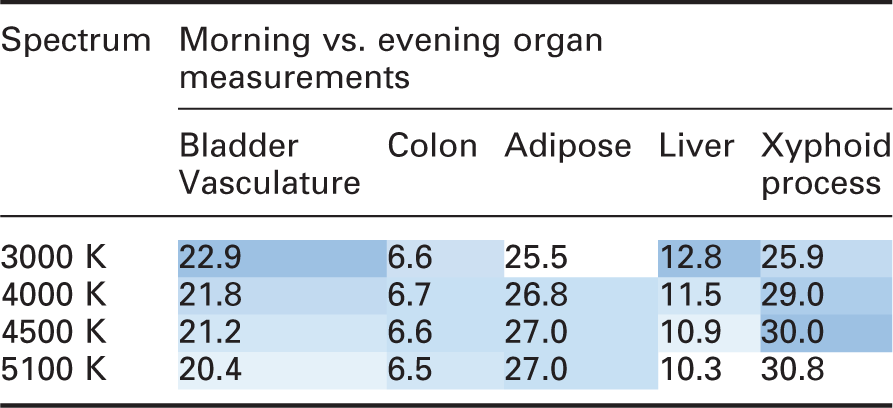
Note: Magnitudes of individual colour differences are not the subject of investigation. Shading is used to assist with the comparison of spectra and the evaluation of trends. The difference in ΔEab between experimental spectra ranged from 0.2 (unnoticeable) for colon to 2.5 (just noticeable) for bladder vasculature and liver – with the exception of the xyphoid process under the 3000 K spectrum, which was a poor performing outlier. Spectra were not ordered the same for each pair of spectral reflectance distributions.
4. Discussion
The surgeons did not differentiate the effectiveness of the 4000, 4500 and 5100 K spectra. This was not unexpected; the spectra all have similar colour rendering with a maximum IES Rf difference of 0.2, maximum IES Rg difference of 2.2 and resulted in a maximum difference in ΔEab of 1.8 for the five internal organs evaluated in this experiment. Figure 9 illustrates the surgeons’ perception of their ability to effectively evaluate organ colour appearance under each of the spectra in terms of their responses to questions 1–5.
Spectrum scores (Q1–5). The 95% confidence interval for each spectrum is averaged across surgeon and organ. While the Q1–5 data are properly understood in terms of the spectrum by surgeon interaction, these results indicate that all spectra were ranked as highly effective. Though other analyses suggest that 3000 K was least effective, that does not mean that it was ineffective. The dashed line at an average score of 3.5 indicates the midpoint of the scale. Though the semantic scales were only defined at their endpoints (see Table 2), the midpoint of the scale is assumed to represent ‘undecided’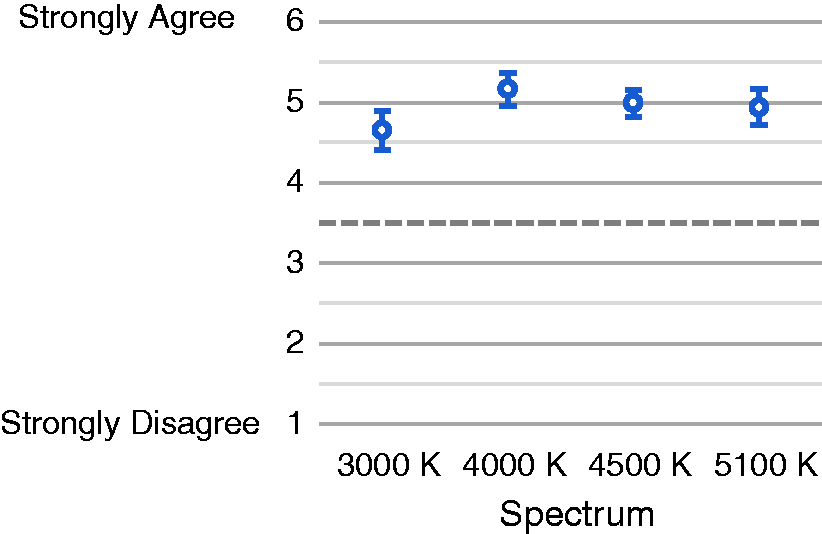
The 3000 K spectrum as measured during the experiment does not adhere to the IEC standard for chromaticity or CCT. 9 Two surgeons made unprompted comments on a pinkish tint of the spectrum, which is supported by its low CCT and negative Duv. The slight tint of the 3000 K spectrum may have been the reason that the surgeons’ rated this condition as the least effective.
The 5100 K spectrum produced about 5% less illuminance than the other experimental spectra. Two surgeons made unprompted comments indicating the 5100 K spectrum was comparatively dimmer, suggesting that this difference was perceptible to at least some of the participants. At the high illuminance present during the experiment, this deviation did not appear to influence ratings of spectrum effectiveness; the survey analysis demonstrated that 5100 K was not significantly less effective than the 4000 K or 4500 K spectra.
As summarised in Figure 8, the surgeons moderately agreed that the colour appearance of internal anatomy was altered by the different spectra. They were undecided as to whether the differences were large enough to affect surgical decisions and undecided leaning toward slightly unconcerned that varying the spectrum could increase the risk of surgical error. The surgeons were undecided whether they would select different spectra for different surgical procedures and whether they would select different spectra for viewing different internal anatomy. They were undecided leaning toward slightly disagree as to whether they would utilise different spectra during a single surgical procedure.
Surgeon comment summary
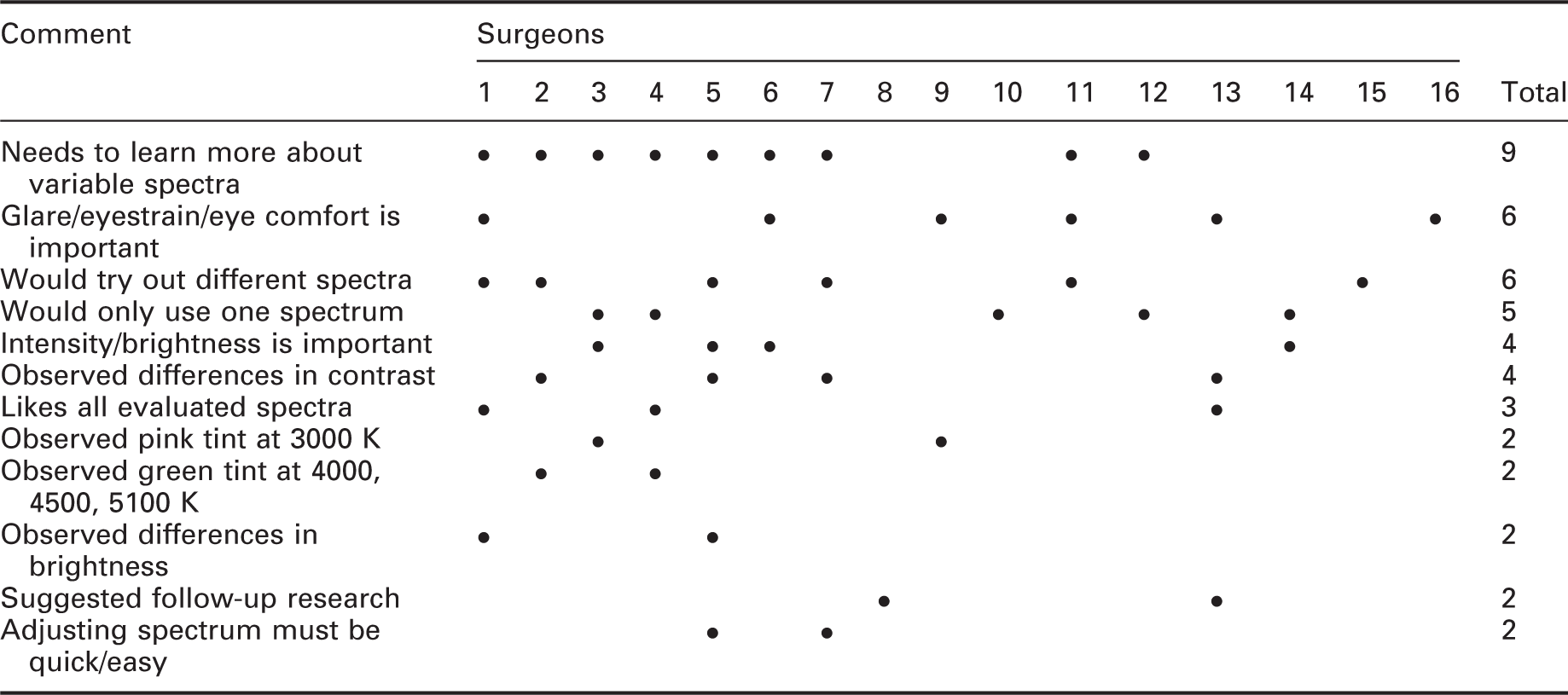
Note: Comments are grouped into the tabled summaries. Among surgeons indicating a need to learn more about variable spectra, seven indicated they wanted to learn from personal experience and two indicated they were interested in recommendations. Comments not summarised here generally pertained to spectrum preference or specific organs and surgical practices.
Many surgeons are likely unaware of the effect of chromatic adaptation on colour perception when substantially changing a luminaire’s chromaticity. The only surgical specialties where one spectrum was clearly rated as more effective included only a single surgeon, indicating that this result is not generalisable utilising only this data set. Considered together with surgeons’ comments during the experiment, and existing research on task-specific spectra,1,3,20 the relationship between light spectrum and surgical specialty may warrant further study. In any case, the small and unbalanced sample of this study makes demographic-based conclusions tenuous and premature.
The trends in ΔEab performance suggest that specific colour differences may be enhanced by different CCTs. Basu et al. 4 found that lower CCTs enhanced contrast between melanin and hemoglobin when diagnosing skin cancer. Wang et al. 3 found that CCTs in the range of 4000 to 5000 K were optimal for maximising colour difference in the oral cavity. For the experiment presented in this paper, the effects of CCT cannot be isolated from Duv since they were not separately controlled in this study. Royer et al. 21 found that the CCT by Duv interaction was significant for predicting colour preference. In their study, the effect of Duv on colour preference was negligible at 4300 K, but was important at 2700 K, where a source with negative Duv was less preferred than a source on the blackbody locus. This is consistent with our findings: all four conditions that we studied had negative Duv (see Table 1), but the lowest CCT condition (3000 K) was judged to be less effective than the conditions at 4000, 4500 and 5100 K.
Engineering optimised spectra requires a thoughtfully constructed objective function. Maximising colour difference, which will improve colour discrimination, is a key objective, though minimising hue distortion is likely an important secondary objective. 22 Constraining the objective function to meet IEC 60601-2-41 requirements will constrain the spectrum to nominally white light. Once candidate spectra have been identified, their utility should be confirmed by further studies. While task-specific optimisation necessitates trade-offs, this could be addressed by a multi-channel LED array capable of a variety of task-optimised and high-fidelity settings.
5. Conclusions
All four experimental spectra were rated as highly effective by the participating surgeons, and by CIE Ra, IES Rf and IES Rg scores, though the 3000 K spectrum fell just outside of IEC compliance. No statistically significant differences existed between the 4000, 4500 and 5100 K spectra. The 3000 K spectrum was ranked as least effective, though this does not mean it was ineffective. The spectrum by surgeon interaction was significant in all models where it could be estimated, suggesting that surgeons may develop opinions about which spectra are most effective for the tissues that they prioritise. There is some evidence that surgeons with different specialties had distinct ratings of effectiveness, but the sample is too small to draw confident conclusions.
The trends in ΔEab performance support the concept of task-optimised spectra, but surgeons’ evaluations coupled with the magnitude of differences in ΔEab performance suggest that the experimental spectra had only a small influence on the evaluations of effectiveness. The linear mixing for variable CCT employed in this experiment did not provide obvious utility for surgeons making visual evaluations.
Spectral optimisation based on empirical research, guided by colorimetric predictions, could provide clear recommendations for settings that would be expected to enhance colour discrimination for particular tissues or conditions. Surgeons may be reluctant to utilise spectral tuning features until they are able to develop familiarity with the available spectra.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The prototype luminaire employed in this study is the proprietary design of STERIS Corporation. The participating surgeons were compensated by STERIS Corporation. STERIS Corporation reviewed the experimental protocols that were developed by The Pennsylvania State University. Representatives of STERIS Corporation were observers during data collection. STERIS Corporation had no role in the collection, management, analysis and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The experiment involving the prototype luminaire was funded by STERIS Corporation through a sponsored research agreement with The Pennsylvania State University.
Acknowledgement
The Animate Skills Laboratory at the Case Western Reserve University prepared the pig and provided medical oversight.