
Abstract
Complex health and welfare organisations struggle to align resources and integrate services for mental health patients. In Western Norway, 16 leaders across four local public organisations participated in this action research study. Providing services for joint service users, they were mandated to make necessary changes towards resource alignment and service integration. The purpose of this study was to learn how these leader experienced the process and outcomes of participating in the four year action research project aiming at transforming practices by implementing a portfolio of social innovation initiatives. More than 300 people, including service users, frontline workers and leaders were involved in the social innovation initiatives, including two service design projects and a network for leaders for collective governance across organisations. Data for this study were co-created in reflexive dialogues in a focus group interview and a whole-day evaluation workshop for leaders in the network. Through reflexive thematic analysis this study found that participants experienced transformations in services, power relations, relational awareness of interdependency, organisational culture, and capability for self-steering in a `systemic whole`. We conclude that combining social innovation and action research enabled local contextualising of problems and solutions, contributing to co-creation of integrated, safer services and resource alignment in the Health Community.
Keywords
Introduction
In the mental health sector, problems are often described not only as complex and wicked but also as malign, as some services cause additional harm to service users (Samuriwo & Hannigan, 2020). According to Norway’s auditor general (2021), poor collaboration, inadequate coordination and insufficient services across multiple sectors and organisational levels pose significant risks to patient safety in mental health care. Fragmented responsibilities and lack of awareness of different providers’ mandates and contexts make resource alignment and coherent service delivery difficult (Vik, 2018).
Traditional strategies for improving health services have emphasised person-centred integrated care and standardising efficient care pathways (Porter, 2010; Rohwer et al., 2023). Even if care pathways have proven successful in integration of services concerning somatic illnesses, this has not been successful yet in the mental health care context. The concept of mental health is complex (Patel et al., 2018), and attempts to implement care pathways have been experienced as top-down implementations of illegitimate solutions with low context fit (Tørseth & Ådnanes, 2022), failing to align resources and integrate services. In other European contexts, Finch et al. (2023) identified a disconnect between policy rhetoric and implementation of integrated services. This gap has been attributed to poor policy context fit, lack of institutional trust, insufficient evaluation of past interventions and fear of failure, inhibiting innovative approaches necessary for effective service delivery (Finch et al., 2023). Consequently, local health and welfare organisations face significant challenges in providing integrated services.
In the study presented in this article, leaders from local health and welfare service providers in Western Norway collaborated to address this challenge. These leaders and their organisations’ efforts aligned with national policies in the national hospital plan (Meld. St 7, 2019), calling for innovation to address the unmet need of their joint service users, local mental health patients. The term Health Communities was introduced in the national hospital plan to describe expected collaboration between municipalities and hospitals as equal partners in creating safe, efficient and integrated services. We refer to the four organisations in this study as a Health Community due to their interdependent services aimed at joint users. They continuously seek to transform their services, focussing on safety, integration and resource alignment.
Social innovation offers a promising path for transforming practices and systems, and it is defined in many ways. This article aligns with Avelino et al.’s (2019, p. 197) definition of social innovation as ‘change in social relations, involving new ways of doing, organising, knowing and framing’. A relational approach to welfare may help ensure that social innovation leads to equitable outcomes and genuinely improves well-being. This approach focuses on human relationships, social justice and individual capabilities in creating public value (Heimburg & Ness, 2021). Thus, social innovation processes continue to target common, socially desirable goals. In healthcare, these goals include social justice, patient and actor empowerment, integrated services for users and sustainability through resource alignment among service-providing organisations. Services include indoor/outdoor medical and psychological treatment, economical or practical support for housing, workforce inclusion for individuals with disabilities and social benefits, among others. Achieving integration requires a deep understanding of services and providing them in different organisations’ contexts.
Social practices need to change to facilitate transformations towards desirable policy goals or missions (Edler et al., 2024), and transformative social innovation can be viewed as a contingent process through which social innovation contributes to transformative change in specific contexts (Avelino et al., 2019). In a local Health Community context, social innovation can lead to new social practices across levels and sectors, aiming to be transformed towards policy goals of integrated, safe services and resource alignment by processes that put citizens’ needs at the centre of innovation, in which actors participate as equals (Meld. St 7, 2019). Joint service design projects (Yang & Sung, 2016) and governance networks can provide relational spaces and arenas in which actors can mobilise and cocreate new knowledge about problems they face, and cocreate new solutions and practices. When the framing of problems and actions to solve challenges changes, and new routines on how this is handled within organisations’ mundane activities become a reality, we can describe the changes as institutionalised (Scott, 2014). When changes in a Health Community become institutionalised and structurally significant, such as shifts in culture or organisation of service provision across different actors, we view them as transformed, and the process towards this as transformational.
A scoping review of social innovation in healthcare found that empirical evidence mainly provided practical insights on implementing social innovation in health systems, particularly regarding increasing patient participation in healthcare and healthcare innovation (van Niekerk et al., 2021). However, none of the studies addressed the issue of service transformation. Hence, the scoping review concluded that empirical studies have not yet demonstrated service transformation within the healthcare context. This article examines whether social innovation initiatives in a Health Community for mental health contribute to transformative change in the specific context.
Transformational social innovation can be achieved effectively through action research (AR) involving collaborative inquiry and practical solutions to drive systemic change and enhance social well-being. AR is recommended to foster transformation at both organisational levels (Yang & Sung, 2016) and to address societal grand challenges (Bradbury et al., 2019; Edler et al., 2024). By combining scientific rigour with efforts to facilitate organisational change through the participative process, AR can create valuable arenas for new social relations across organisations and levels. Typical AR projects involve iterative development of problem solutions through learning activities, such as planning, experimentation, reflection, evaluation and adjustment (Wittmayer & Schäpke, 2014). Hence, AR can ensure that the solutions developed are contextually relevant and sustainable. Through collective sensemaking about framing the problem, what changes are needed and how to implement them can provide actionable insights for prefigurative change towards shared goals for the future (Wittmayer et al., 2019), to which all actors can contribute. Therefore, we argue that AR is well-suited to support social innovation processes in the Health Community context.
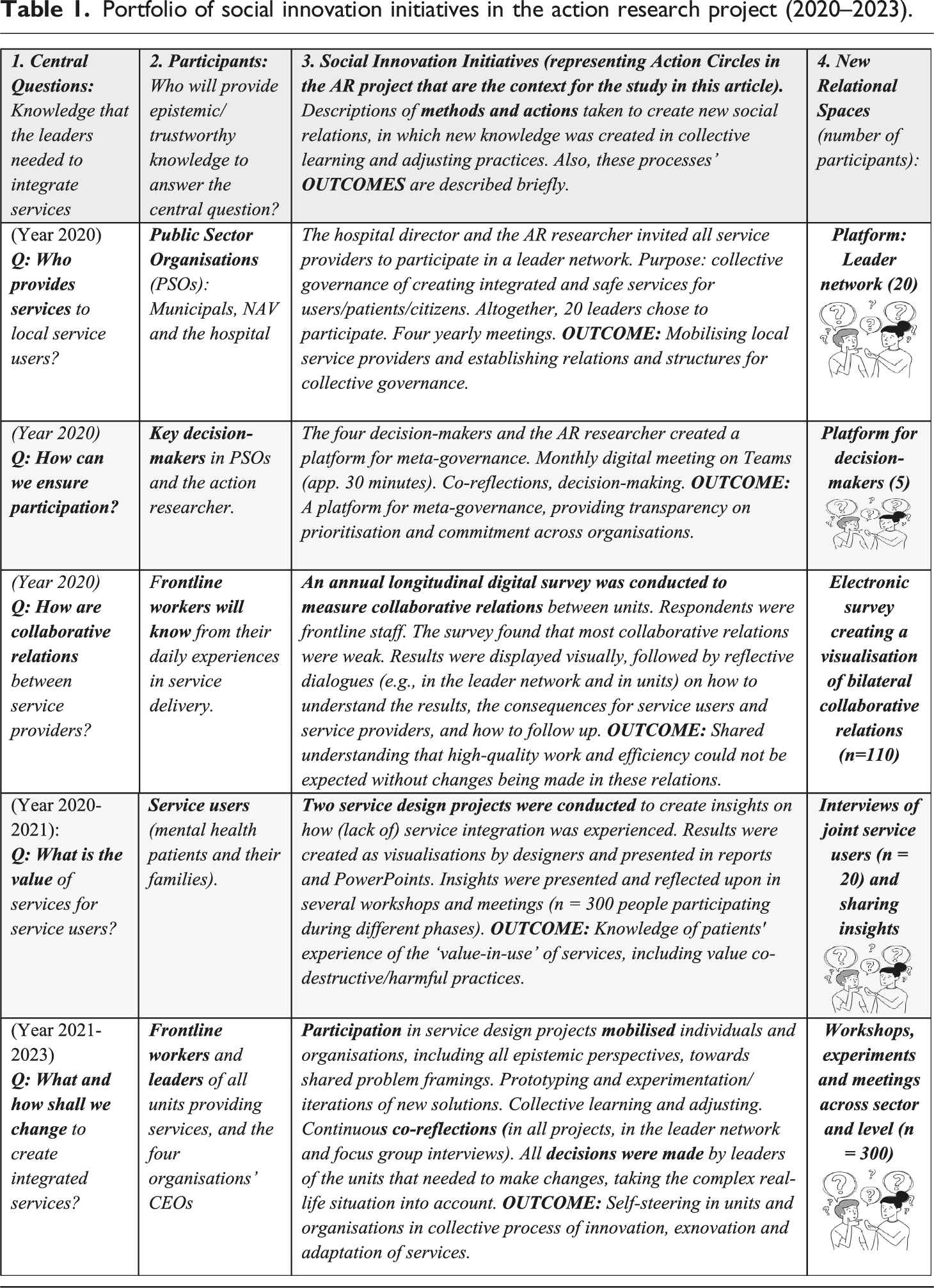
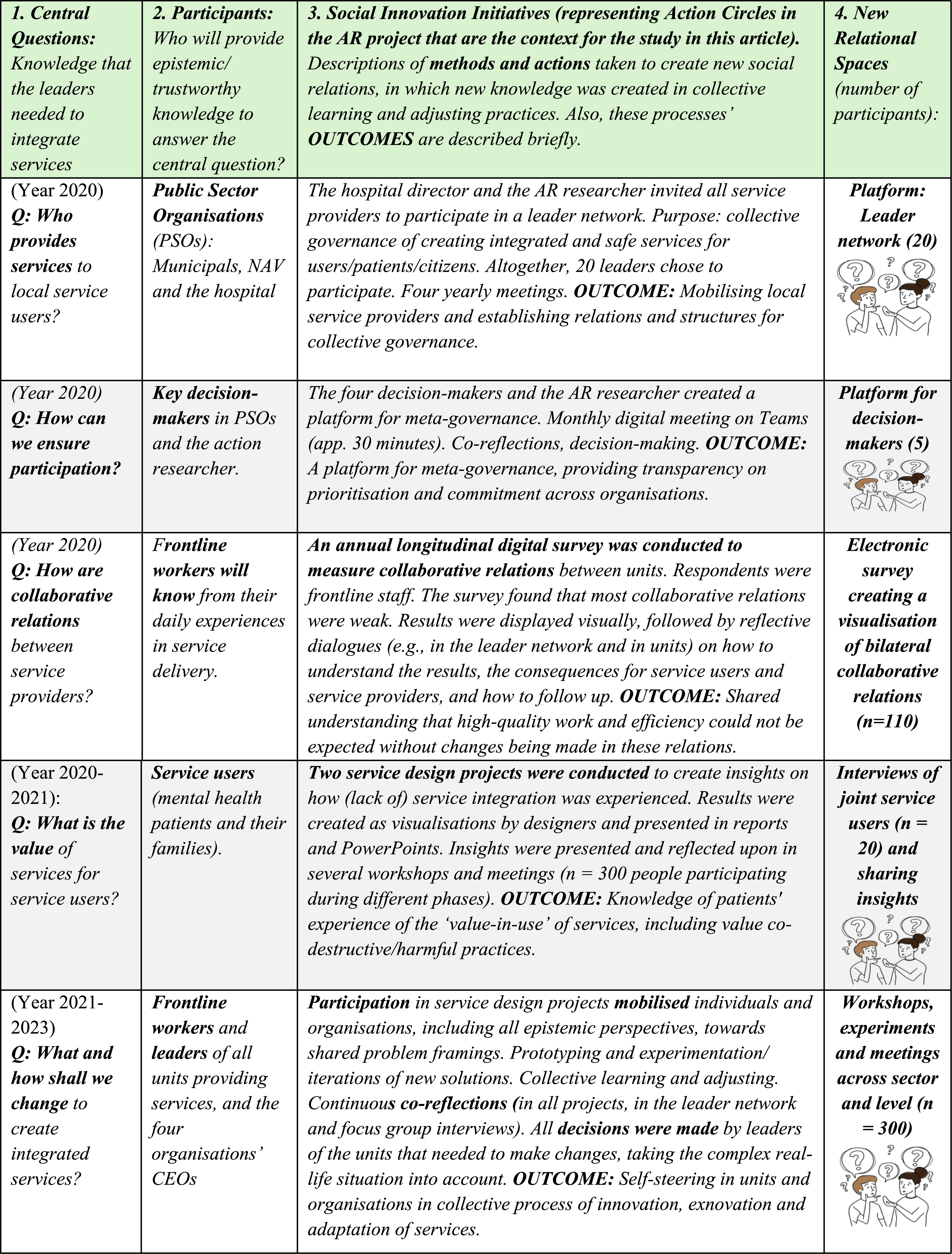
Portfolio of social innovation initiatives in the action research project (2020–2023).
This study aimed to understand how leaders experienced the process and outcomes of participating in an AR project implementing social innovation initiatives to target transformative change in service delivery in the context of a Health Community. This exploration leaves open the question of whether social innovation implemented with AR processes yield transformational outcomes. The specific research question (RQ) was: How do leaders experience the process and outcomes of participating in a portfolio of social innovation initiatives aimed at integrating health and welfare services?
Method
In this section we detail the research design and spesific context of our study.
Research context, procedures and participants
This study was conducted at the conclusion of a four-year longitudinal AR project (2020–2023), ‘Leading for Innovation and Collaboration in a Health Community for Mental Health, Aiming to Increase the Value of the Services for the Service Users’. The project aimed to create integrated health and welfare services for joint service users across their units and organisations, defining themselves as a Health Community. Service users were local mental health patients. The 20 participating leaders represented 20 different units within the four local public health and welfare organisations: two municipalities, a mental health hospital and the Norwegian Labour and Welfare Administration (NAV), hence they represented the service providers. For further description of the context, see Senneseth and Berg (2025, p. 72).
To answer the aforementioned research question, qualitative data were generated through evaluations of and reflections on the entire four-year process among the participants. All participants in the leader network were invited to participate in this study and were recruited because they were key decision-makers or frontline leaders from the local service providers. Representing the central public health and welfare system, they had a mandate to make necessary changes proposed by national policies. Altogether, 16 of the 20 invited leaders participated in this study. Before presenting the data and analysis, we further outline the research context by describing the AR project.
The action research project
The ‘actions’ in the AR project were pragmatically chosen collaboratively by the action researcher and the participating leaders by examining the best methods available to address participants’ real-life questions and challenges. These initiatives/actions aligned with the social innovation definition presented above as change in social relations, involving new ways of doing, organising, knowing and framing (Avelino et al., 2019) Thus, these actions are characterised as social innovation initiatives in this article, as presented in Table 1. These actions are not, per se, the data for this study, but are essential to understanding this study’s context and answering the research question.
The portfolio of social innovation initiatives implemented in the AR project enabled the use of various methods new to the context (see Table 1), conducted abductively (Gehman et al., 2018) and systematically integrating emerging knowledge needs with innovative approaches. Networks and temporal organisations (Lundin & Söderholm, 1995), such as service design projects (Patrício et al., 2020), enabled flexible collaboration and learning with opportunities for collective action described as central for transformations, such as realigning normative, institutional and cultural elements; exploring knowledge complementarities and facilitating collective sense-making (Vink & Koskela-Huotari, 2022).
Table 1 was designed to aid reader comprehension (Cloutier & Ravasi, 2021) of the research context by describing the portfolio of social innovation initiatives implemented. Each row describes a social innovation initiative based on four central dimensions in the columns. The first column describes the question the leaders asked and the required knowledge creation. The second column describes the participants, who were recruited strategically to provide epistemically humble (Skelton et al., 2024) and trustworthy knowledge to answer or handle the question in the first column. The third column contains descriptions of the actions taken to generate knowledge and these actions’ outcomes. The fourth column describes the new relational spaces created for collaborative learning and/or governance purposes in each specific social innovation project or process.
Data and analysis
Reflexivity is vital in AR projects, and systemic reflexivity is pivotal in creating transformative capabilities (Moore et al., 2018; Wittmayer et al., 2019). In this study, we zoom in on two such co-reflexive processes at a particular moment in the larger AR project through the participating leader’s evaluations and co-reflections after four years of a process implementing social innovation initiatives together. The specific data developed for this article were generated in two contexts: First, a one-and-a-half-hour focus group interview (Hummelvoll, 2008) was conducted with the four key decision-makers representing the four organisations. Second, a one-day evaluation meeting was conducted in the leader network, providing 4 hours of recorded reflections and discussions. Altogether, 16 leaders, decision-makers and frontline leaders from different units within the four organisations participated in the meeting. The focus group interview and evaluation meeting were audio-recorded and transcribed verbatim. In addition to generating data to answer this article’s research question, these methods created arenas for co-reflection and learning between the participants and a foundation for decisions concerning further collective actions, which are central ingredients in the iterations of AR processes.
Through reflexive thematic analysis (Braun & Clarke, 2022) of the focus group interview and evaluation meeting transcripts, we identified five key themes of processes and outcomes described by the leaders. Initially, the first author became familiarised with the data by reading and listening to the interviews, aiming to grasp the essence of the leaders’ descriptions and stories. During this phase, words, sentences and ideas for potential themes were noted. Next, the first author reread the transcripts to delve deeper into how the leaders described their experiences, focussing on new social relations’ specific contributions and processes concerning new ways of doing, organising, framing and knowing; and descriptions of transformations. Post-it notes then were used to create main theme groups, presented in this article’s findings section. Throughout the analytical process, the themes were discussed continuously with the second author.
Reflections on the action researcher’s role
Action researchers can adopt various roles (Wittmayer & Schäpke, 2014). During the four years of the AR project, the first author became deeply embedded in the case. What can be described as deep knowledge and thick descriptions of the context were obtained by coordinating the portfolio of social innovations, conducting surveys, longitudinally participating in and/or facilitating various formal meetings and participatory processes, conducting informal conversations and multistage focus group interviews, and serving as the project leader in one of the service design projects described in Table 1. The various encounters allowed the action researcher to assume the role of a change agent, engaging as a transformative action researcher (Horlings et al., 2020). As a PhD student in innovation, the first author functioned as a knowledge broker between the `outsider position’ from the academic realm and an ‘insider perspective` from the real-life field of innovation and as an experienced health professional (psychologist).
However, deep involvement can blur awareness of one’s power dynamics; thus, precautions were taken during organisational research with close collaborators, for example, communicating when data were collected for citation purposes to avoid participants feeling monitored. Transparency was another key ethical consideration, with most knowledge cocreated in groups and written reports readily accessible to participants. This way, we also avoided delays typical of traditional research, and the participants could utilise the knowledge immediately.
Conducting AR is described as risking entanglement in ‘dilemmas of power inequalities and complex relational dynamics’ (Bartels & Friedman, 2022, p. 101). As an action researcher, the first author reflected on own stance regarding power dynamics and values embracing equality and justice. This allowed continuous awareness and discussions with participants concerning the process, procedures and what is experienced as equal partners. This helped us develop literacy and consciousness concerning the blind spots existing concerning just participation. Thus, listening to all participants actively and humbly was an aim, including awareness of power balances between the researcher and participants and between participating actors. Furthermore, one’s biases and experiences can influence understanding and interpretations of participants’ stories. Thus, the second author’s critical view has been important, both in the research process and in the analysis and writing of this article.
Research ethics
The Norwegian Centre for Research (NSD, now renamed Sikt. Project number: 464812) approved this study, and we adhered to ethical guidelines throughout. Participation in interviews and surveys was voluntary, with written informed consent obtained from all participants. To maintain anonymity, participants are referred to below as leaders without linking them to their specific organisations, unless it is particularly important for explaining findings (e.g., concerning power relations).
Findings
This study examined how leaders perceived the processes and outcomes of participating in social innovation initiatives designed to integrate health and welfare services across organisations. In this section, we describe and discuss the findings concerning the main themes from the data analysis. Through thematic analysis, we identified five themes: (1) Transforming power relations from ‘master and servant’ to ‘equal partners’; (2) Transforming relational ignorance into relational awareness; (3) Transforming capability to self-steer Own Unit in a systemic whole; (4) Transforming the organisational culture from ‘us’ and ‘them’ to ‘we’ and 5) Transforming services and harmful practices. The processes and outcomes were described as co-evolving and nonlinear and, thus, must not be interpreted as ‘stages’, but rather as fuzzy ingredients towards change and transformation.
Transforming power relations from ‘master and servant’ to ‘equal partners’
The leaders described how new ways of collaborating in projects and cogoverning in networks and projects transformed their relationships, including changes in their actions and behaviours, which led to transformations in power dynamics between the hospital and municipalities’ representatives over the four-year period. Previously, municipal representatives had viewed hospital representatives as domineering. Municipal leaders described earlier meetings as arenas in which ‘the hospital was just telling the municipality how it should be’ without room for dialogue. Thus, collaboration ‘was not experienced as being on equal footing’. Their past experiences with asymmetrical power relations aligned with a well-known phenomenon described in research from the Norwegian health context (Vik, 2018). A shift towards a partnership on equal footing was experienced during the past four years, initiated by a new hospital director’s behaviour. A municipal leader described how the new way of ‘doing’ collaboration was based on dialogues and exploration of the problem at hand together: We began discussing the challenges related to collaboration. No one had predetermined decisions about those challenges; we explored them together. This approach was entirely new compared to how the hospital had handled things before.
The new hospital director described a strategic decision to move away from conducting decision-making on behalf of other organisations: ‘I was determined that this had to change. It was a strategic choice. I do not get involved in (what) is not my business’. Self-steering of each organisation’s participation in joint initiatives and decisions concerning whether to make changes in own organisations were established as the new norm for collaboration: ‘This is how we do it now’, one municipal leader said. As the new approach evolved into new routine practices between actors over time, it indicated an institutional change (Scott, 2014) representing a shift in power relations between parties.
Power can be used to exercise ‘power over’ others or to share ‘power with’ others (Avelino, 2021). In this study, we found that the hospital director initially held a dominant position and had power to make changes. The director then shifted towards equal participation among self-steered actors. It is not the organisation, but rather individuals within an organisation and the organisational culture that act. Therefore, how individuals within organisations with dominant power positions choose to exercise their power can impact maintenance or transformation of relationships and power dynamics between actors significantly. This finding demonstrates that one leader can be pivotal in transforming power positions between organisations of hospitals and municipalities by changing their actions.
However, avoidance of exercising power dominance is not enough to create transformation. To create the dynamics of exercising ‘power with’, all relevant actors’ in the Health Community had to be included, come forward, and take on responsibility for own service provision and make necessary changes. For example, by acknowledging how they contributed to harmful practices and changing these practices. The changes in the actors’ mundane practices described actions that we understand as changes in how the actors conduct services for service users, and how they do collaboration between the organisations, aligning with descriptions of new ways of ‘doing’ collaboration as part of a social innovation process, in which the outcome was a transformation in the power balance between the actors. The social innovation portfolio conducted with AR processes provided a transparent and systematic method to include and enable this participation, and allowed the actors to participate on their own terms, aligning with descriptions of epistemic and procedural justice (Skelton et al., 2024). Hence, the awareness and sensitivity to these central AR principles contributed to the transformation from asymmetric to equal partners.
Transforming relational ignorance into relational awareness
Participation in the new relational spaces provided by the social innovation initiatives and the processes of dialogues, cocreation of joint experimentation/iteration of new services, and co-reflections for learning permitted participants to get to know each other and the situated contexts in new ways. What had been relational ignorance between the actors – that is, lack of knowledge about who the other service providers were, which services they provided for the joint service users, and interdependencies and dynamics between the actors – shifted towards relational awareness. This new knowledge and awareness enabled the actors to understand the Health Community’s `parts’ and ‘whole’. As one leader explained it: ‘The way we sat together, from different organisations, was more important than what we did’. As they learned about the many service providers involved, each other’s roles and the variety of services provided, they realised they had been ignorant about each other. One leader burst out to another participant, ‘I did not know you, and I didn’t even know your unit existed!’ By focussing solely on their domains, they had been ignorant of the other actors and their joint responsibilities across organisational borders. One leader stated: ‘The focus was “this is my (domain and)” responsibility’. Through social innovation initiatives, participants identified relational, structural and institutional barriers. They also revealed the blind spots on how their organisation might hinder others’ efforts to serve joint service users: ‘It was constructive; we examined the pain threshold for collaboration and became aware of our sphere of interaction’, one leader stated.
Service users’ needs and experiences while encountering services were described as meaningful and legitimate focal points for all actors, with one leader describing this as the core mandate: ‘The service users’ experience concerns the core of our mandate and task’. This way, systemic awareness developed concerning how the services provided as ‘parts’ and as a ‘whole’ affected service users. This concerned that most actors did not know what services the others provided; thus, when they referred service users to other units/organisations, they created wrong impressions about what the service user could expect from other service providers. This destroyed service users’ trust in the health and welfare system and caused frustration between actors, and everybody felt they wasted time and energy sorting out misunderstandings. Further, new insight concerning how ‘revolving door’ patients were harmed in encounters with different service providers was identified; such as being treated disrespectfully or not getting access to the services they needed when they needed them. This way, practices that caused lack of service integration and resource alignment were identified concretely. This included the high costs, both economically and in human suffering, of either providing harmful services or faulty due to negligence. This new cocreated insight transformed the framing of existing practices from legitimate to illegitimate in a systemic perspective of the health community as a whole, even if practices in each silo organisation were according to policy and routines.
The leaders from all organisations described how these projects enhanced the understanding that all epistemic perspectives were needed to comprehend the ‘value-in-use’ (Vink et al., 2021) for service users to enable the organisation’s ability to align resources. Furthermore, as the understanding that fidelity to sectoral policies did not guarantee safety and value for service users in a systemic perspective, a new narrative emerged; that services delivered according to routines could still contribute to harm to the service users.
These descriptions align with how contextualising and recontextualising (Meier & Dopson, 2019) can foster awareness of the systemic perspective (Senge, 2006) through dialogues and reflexive practices. This, in turn, enhances the mentalisation capacity (Fonagy et al., 2011) of all actors regarding the situated and evolving context as they experience it. We understand these processes as continuous sensemaking (Patrício et al., 2019), enabling participants to flexible move the understanding between the silos and the systemic whole (Hajjar et al., 2024), thus seeing ‘the parts’ and ‘the whole’ together.
We view sensitivity to ensuring participation in these reflexive processes as contributions to the emergence of a collective consciousness (Kinder et al., 2021) towards understanding and taking collective responsibility for services provided (or not), including taking on responsibility for own actions contributing to value co-destructive practices (Järvi et al., 2018) in need for dismantling or exnovation (Hartley & Knell, 2022).
Transforming capability to self-steer own unit in a systemic whole
The empowering shifts in power dynamics and relational awareness of the systemic whole elicited a capability to take on the responsibility to make changes in own units where they were mandated. Thus, new ways of organising between the actors emerged based on self-steering and self-organising changes in own unit towards what they understood was best for the systemic ‘whole’ of the Health Community and their joint service users.
It was crucial for leaders to make strategic decisions about who they wanted to include for participation in the different processes. The leaders needed to ensure that the participants had maximum fitness for the purpose. Sometimes, this could be a person’s professional background. Other times, it could be a person’s collaborative skills, local ‘know-how’ or an informal leadership position that was desirable. Being able to select their participants during all phases of the social innovation initiatives fostered a great sense of ownership: ‘It was new for us to select who we wanted, and this gave us stronger ownership’. This self-steering principle was experienced as a flexible, expedient and respectful approach, enabling actors to address their challenges. The approach also honoured each organisation’s capabilities when external pressures on organisations during the COVID-19 pandemic constantly shifted and impacted organisations differently over time. As one leader noted: It’s a respectful way of collaborating because we have different laws, policies and organisational contexts. None of us have stable economic situations, and we all face changing challenges.
All the leaders emphasised the importance of stable platforms for collaboration and governance, enabling them and their organisations to comprehend the complex situated landscape. This understanding allowed them to decide how and when to engage.
Collaborating with external organisations also legitimised internal changes. One leader explained how external perspectives helped increase self-awareness of own organisations impact on others, and to dismantle silo barriers in own organisations: ‘It is about enhancing our self-awareness, understanding how we actually work and taking a step back to dismantle these walls we have built around ourselves’. That was also the case when it came to handling their own contributions to the harmful practices identified. The new understanding called for a transformation of own practices, but these had to be aligned with the other actors’ practices. Making changes within one single ‘part’ of the silo systems would not provide sufficient change. They recognised that they all needed to act and handle failures if the `whole` of the services in the Health Community should be integrated and provide value for service users.
We understood the leader’s descriptions of the processes as central features of AR involving a multi-learning environment with joint planning, experimentation and reflexivity to steer practice towards the aim (Patrício et al., 2019; Wittmayer et al., 2019). The outcome was increased capability for all actors to participate in improving services for their joint users through collective governance (Kinder et al., 2021; Senneseth & Berg, 2025).
Transforming the organisational culture from ‘us’ and ‘them’ to ‘we’
The combination of joint projects and the self-steering and self-organising norm within the systemic whole transformed the organisational and collaborative culture. The participants described the changes as ongoing through various encounters in networks and projects, rather than any single project. One leader emphasised that the organisational change in culture occurred between meetings: ‘The portfolio focusses on what we do outside of the meetings; the meetings are about building a shared understanding, developing a common knowledge base and discussing our challenges’.
The leaders reflected on their past tendency to speak negatively about other organisations to service users. ‘It’s a shame, but that’s what we did’, one leader admitted, expressing regret. She described how she now felt genuine pain when hearing negative remarks about collaborators: ‘It really hurts’, she said, placing her hand over her heart. This shift in perspective stemmed from a growing familiarity with other organisations and their challenges. ‘I know that you do…and we do the best we can’, she acknowledged, emphasising that understanding others’ efforts transformed her view and enhanced empathy. Earlier, they had narratives about each other as competitors, fighting over resources and suspecting that others would trick them into delivering services. Now they understood that all actors were short of resources and faced similar pressures. ‘We now understand that the pressure is on all of us, and we understand what it means for each of us’. While acknowledging that transformations take time, one leader expressed hope by observing changes in their frontline staff: ‘It is so obvious that they now have a different understanding and attitude (…) beneficial for our joint service users’.
Participants from all organisations described transformations as a shift from an organisational culture of ‘us and them’ to a ‘we’ culture, acknowledging that no single solution or quick fix exists. A ‘we’ culture is crucial for systemic understanding and collective actions (Kinder et al., 2021; Senge, 2006). The new culture for handling value failure together was developed collectively, breaking with earlier blaming and scapegoating by trying to find ‘the fault’ and ‘the guilty’. Leaders took on collective responsibility for the failure, anticipating that increased demand for changes would be impossible to handle alone in the silos for the future. We understand this as transformation in the narrative on governing to meet future challenges (Wittmayer et al., 2019) towards collective actions and collective goals. The leaders further understood the need for personal engagement to develop their roles (Senneseth & Berg, 2025) and services to exercise ‘power with’ each other (Avelino, 2021) for the future and to conduct collective leadership (Kinder et al., 2021).
Transforming services and harmful practices
The findings indicate that the actors transformed the services they collectively identified as harmful and expensive, thereby realigning practices towards service integration and safety for service users and resource alignment between the organisations. The harmful practices concerned how service providers mislead service users by creating wrong impressions about what they could expect from another service provider, and concerning ‘revolving door’ patients as they were harmed in the encounters with several service providers.
The new understanding called for a transformation of each actor’s own practice, which needed to be aligned with all other actors’ practices. Making changes within one single ‘part’ of the silo systems would not provide sufficient change. As one leader noted, ‘We just cannot do that anymore’. The leaders recognised they all needed to act and handle failures where they were mandated, if the `whole` of the services were to be integrated and provide value for service users. Hence, the focus shifted away from pressuring others to change, towards taking on responsibility to improve one’s own practices, aiming to secure patient safety for service users. This aligns with descriptions of a psychologically safe environment (Edmondson & Lei, 2014) between the actors, creating institutional trust (Finch et al., 2023) and a fundament for addressing value co-destructive practices and iterating new solutions (Hartley & Knell, 2022) together.
Due to the detailed picture of the (lack of) alignment of resources and service integration, and its consequences for service users, each actor could see both the parts and the whole of the Health Community, framing the problem as shared, yet acknowledging their own contributions. Recognising their contributions to the problem and learning about others’ willingness to make changes empowered each actor to alter their practices and service delivery. However, they had not yet reached a state of providing no harm to service users. ‘That is what we are trying to experiment with now’. Hence, the actors had to endure the uncertainty about whether the new solutions would create safe services for the users.
Closing discussion
This study finds that the participants in the social innovation initiatives in the AR project yielded transformations in the context of a Health Community; in services, power relations, relational awareness of interdependency, organisational culture, and capability for self-steering in a systemic whole. This study suggests that to transform the wicked and even malign practices known to exist in the mental health care context (Riksrevisjonen, 2021; Samuriwo & Hannigan, 2020), the actors providing services must engage and participate, and so must service users, as suggested in relational welfare approaches (Heimburg & Ness, 2021).
The existing maps and agreements on collaboration in service provision made on a decontextualised macro-level did not represent the terrain in which the service provisions were practised. Thus, it was difficult for leaders of local services to use the oversimplified maps to navigate change within or across sectors and levels.
This study provides an alternative. The social innovation initiatives functioned as boundary objects (Meier, 2015), where the participants could develop relations where they cocreated a new understanding of the shared challenges they faced and worked together towards a desired future state (Wittmayer et al., 2019) in multiple processes of becoming aligned and provide safe, integrated services. The cocreation of new services was experimented with, iterated and updated continuously through participatory reflective learning processes (Vink & Koskela-Huotari, 2022) between equal partners. This empowered actors with the capability for self-steering and self-organisation within an emerging collective consciousness (Kinder et al., 2021) and awareness of the interdependent relationships within the Health Community.
The future sustainability of these transformations will depend on maintenance and involvement from all participants, and whether policymakers and the backbone public organisations support the local initiative or destroy them with top-down implementation of `new solutions` entailing practices with low contextual fit.
Combining social innovation and AR, this study increases the understanding of what a bottom-up approach can contribute. Creating new relationships between interdependent health and welfare system actors with sensitivity to AR principles supporting development of social spaces with participation for epistemic justice (Skelton et al., 2024), mobilised new ways of knowing about the problem and solutions from the different perspectives of service users, frontline workers and leaders. Thus, (lack of) alignment of resources and service integration was revealed by demonstrating actionable insight from value-in-use perspectives (Vink et al., 2021) from different participants, sectors and levels.
We conclude that local contextualising of problems and solutions can empower service providers to transform practice (Patrício et al., 2020). Thus, combining social innovation with action research can empower local actors to succeed with the central aims for Health Communities (Meld. St 7, 2019); to create integrated, safe services by putting patients’ needs at the centre for innovation between equal partners.
This study’s limitations and implications
This study presents knowledge based on a longitudinal case in a specific context, in which local transformations of relationships, practices and narratives have given participants a game-changing understanding of the local health and welfare system to which they belong and cocreate the future. Empirical cases like this are of limited value concerning generalisations, however, they can inspire visionary changes for leaders, managers, politicians, organisations, researchers, service users and citizens. They can also contribute new knowledge to the broader question of empowering local actors to co-govern the transformation of services across siloed organisations in the health and welfare sectors, aiming for resource alignment and integrated, valuable and safe services for patients and society.
To understand whether the changes described in this article will elicit resource alignment and more integrated, safe and valuable services for users in the longer term, the case should be followed up with a longitudinal investigation of outcomes for service users, both qualitatively and quantitatively.
Furthermore, it should also be examined whether taking a systemic perspective and implementing social innovation initiatives with AR can help transform services for other vulnerable groups addressed in Health Communities, namely young patients, frail elderly and people with chronic diseases.
Footnotes
Acknowledgement
The authors gratefully acknowledge the editors and reviewers for their constructive and detailed critiques on earlier submissions, which facilitated a valuable learning process and significantly improved the quality of our work.
Author note
Both authors confirm their authorship and that it is both the author's work.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.