
Abstract
This article explores very young children’s food preferences, perceptions and influencing factors using a mix of visual and game-based methods that empowered children to meaningfully participate in research in a variety of ways. Eighteen workshops were conducted in 10 preschools involving a total of 64 children aged 3–5 years. Inductive thematic analysis using NVivo software was performed. Results show that very young children’s food preferences and perceptions are influenced by: familiarity with foods and parental modelling, sensory appeal of food, satiety and hunger, internal and external cues to eat, perceptions of healthiness of food and a preference for a variety of food. This research found a relationship between food and emotions in children as young as 3 years of age and this should be considered when developing interventions for very young children. The findings from this research can be used to develop targeted interventions for promoting healthy eating habits, positive relationships with food and better nutrition in 3–5-year-old children.
Introduction
Early childhood is a critical period for growth and development, and dietary habits formed at this age may persist in later years (Birch et al., 2007; Pesch et al., 2020). Nurturing healthy eating among children has the potential to promote their immediate and long-term health and well-being.
Food acceptance by children is influenced by many innate preferences and aversions (Fildes et al., 2014; Holley et al., 2020; van Den Brand et al., 2023) but also by a range of family, social and environmental factors. Early care settings provide an opportunity to positively influence food habits through education and food provision and are particularly important for children from socio-economically disadvantaged families (Jones-Taylor, 2015; Liu et al., 2016). Indeed, interventions to improve dietary habits among 3–5-year-old children are plentiful (Matwiejczyk et al., 2018; Wolfenden et al., 2020), showing young children can accept and learn to prefer novel or disliked foods with regular and repeated exposure combined with positive feeding practices (Anzman-Frasca et al., 2012). However, to facilitate better acceptance of healthy foods by young children and aid in creating effective nutrition education programmes for promoting healthy eating behaviours, it’s essential to gain a deeper understanding of children’s perceptions of food and their food environment.
By age 5, children possess enough personal experience to have basic knowledge about food, for example, they can distinguish between edible and inedible substances (DeJesus et al., 2018) and understand that food affects the body and is essential for growth and health (Tatlow-Golden et al., 2013; Wiseman et al., 2018). They can recall factual information and correctly categorise food items based on their taxonomy (fruits and vegetables; DeJesus et al., 2018; Rioux et al., 2018) and nutritional value (healthy or unhealthy; Harrison et al., 2016; Tatlow-Golden et al., 2013), and express preferences based on their likes and dislikes (Lafraire et al., 2016).
However, previous studies primarily used quantitative research methods to measure children’s food and nutrition knowledge or task-oriented approaches, such as meal construction tasks involving images of food or food models. Findings from these quantitative studies demonstrate that 3–5-year-old children can organise their mental representations of food through cognitive processes and explain their understanding (Dial and Musher-Eizenman, 2019; Freedman et al., 2021; Harrison et al., 2016; Holub and Musher-Eizenman, 2010; Nguyen, 2020). The increasing acknowledgement of 3–5-year-old children’s agency to impact their own health habits (Sun et al., 2023) has highlighted the need for a better understanding of their views on why they make health-related decisions, including food choices. Gaining a child-centered perspective may help identify often-overlooked environmental influences that shape their food choices. To date, there has been limited qualitative research exploring young children’s understanding of food, food preferences, and food behaviours, as well as the contextual factors that may impact these aspects. This study aims to address existing gaps in literature.
Furthermore, most studies involved children aged 5 and older, and there are fewer high-quality studies involving children aged 4 and younger (Sun et al., 2023) because it was believed that very young children, especially 3-year-olds, do not have sufficient cognitive and communicative skills to take part in qualitative research (Nilsson et al., 2015; Sun et al., 2023; Swauger et al., 2017). Therefore, involving very young children in research requires careful, age-appropriate methods to gain insight into how they view food, make dietary choices, and experience their food environment. Sun et al.’s (2023) systematic review demonstrates progress in listening to children but argues that more needs to be done to promote children’s agency and in the assent process during research with very young children. They recommend that seeking assent from children should not be a one-off event, but rather it should be practiced as a ’process consent’ (Heath et al., 2007: 409).
Considering the language and cognitive abilities of very young children, along with the ethical and methodological considerations involved in working with this age group, this study aimed to explore children’s food preferences and perceptions of (healthy and less-healthy) foods. To achieve this, a combination of age-appropriate methods was used, guided by a participatory approach (Montreuil et al., 2021).
The objectives of the research were to employ multiple creative and engaging methods with 3–5-year-old children to explore: (1) their food preferences; (2) children’s perception of (healthy) food; (3) factors that influence young children’s food preferences and perceptions.
Methods
Study design and participants
In this qualitative study, purposive sampling was used to achieve a mix of socioeconomic backgrounds, and 18 community (predominantly state-funded) and private (paid-by-families) preschools located in disadvantaged areas in the West of Ireland were invited to participate. Both community and private childcare facilities operate the government-funded Early Childhood Care and Education scheme that provides two free-of-charge years of preschool service for all children of preschool age (3–5-year-olds), therefore, children from families with a mix of socioeconomic backgrounds attend private preschool settings located in disadvantaged areas. The inclusion criteria were healthy preschool children aged 3–5 years attending community and private preschools in disadvantaged areas. Children with dietary restrictions and aversions were excluded from the study.
Recruitment and consent
Preschool managers were invited to take part by letter, follow-up phone calls and visits to their centres. After consent from preschool managers was obtained, recruitment letters to parents with active consent forms were distributed by preschool teachers, and consent forms were collected by teachers. Parents were informed that children without parental consent will not feel left out and can still participate in the activities, however their responses will not be included in the project’s data. Respecting children’s rights and competencies as social agents (Montreuil et al., 2021), their assent to participate was obtained by explaining information about the study and what to expect as a research participant using age-appropriate language. Children were informed that they could withdraw from the activities at any stage and were free to ask questions at any time. Throughout all interactions with children, the researcher was cognisant of the power imbalance and their ethical responsibilities to child participants (Swauger et al., 2017). Open dialogue was maintained, and children were encouraged to clarify what they said, understood/misunderstood, and/or recorded (Sun, 2023). Recognising that gaining assent should not be a one-off event but an ongoing process (Sun et al., 2023), the researcher observed throughout the workshops both the verbal and nonverbal cues children use to communicate their assent or dissent (Mayasari, 2022; Sun et al., 2023; Taylor, 2014). The participants’ anonymity was ensured by assigning participant numbers. Full ethical approval was granted by the Research Ethics Committee of the institution where the researchers work.
Research tools and instruments
The choice of research tools was informed by a review of creative, visual, narrative, and participatory research methods that have been used with young children to elicit their understanding of health, well-being, their environment and food knowledge (Clark and Moss, 2011; Granö and Turunen, 2022; Harrison et al., 2016; Holub and Musher-Eizenman, 2010; Nguyen et al., 2011; Pascal and Bertram, 2021; Tatlow-Golden et al., 2013). Central to all creative and participatory research methods is consideration of the multiple voices of children who express their views in different ways as promoted by Reggio Emilia’s approach (Edwards et al., 1998). This approach provides children in early stages of language development with a variety of verbal and nonverbal possibilities to describe their environment and what matters to them. Considering the multiple voices of children, children’s cognitive and language abilities and the goal to include all children who wanted to participate, a mix of visual (stories and drawings) and game-based activities (meal-creation game), complemented with discussions – were chosen for use during the children’s workshops rather than a single instrument. Careful selection of these tools aimed to provide each child with different opportunities to express, demonstrate, or illustrate their food-related experiences and preferences in ways that were familiar and easy for them.
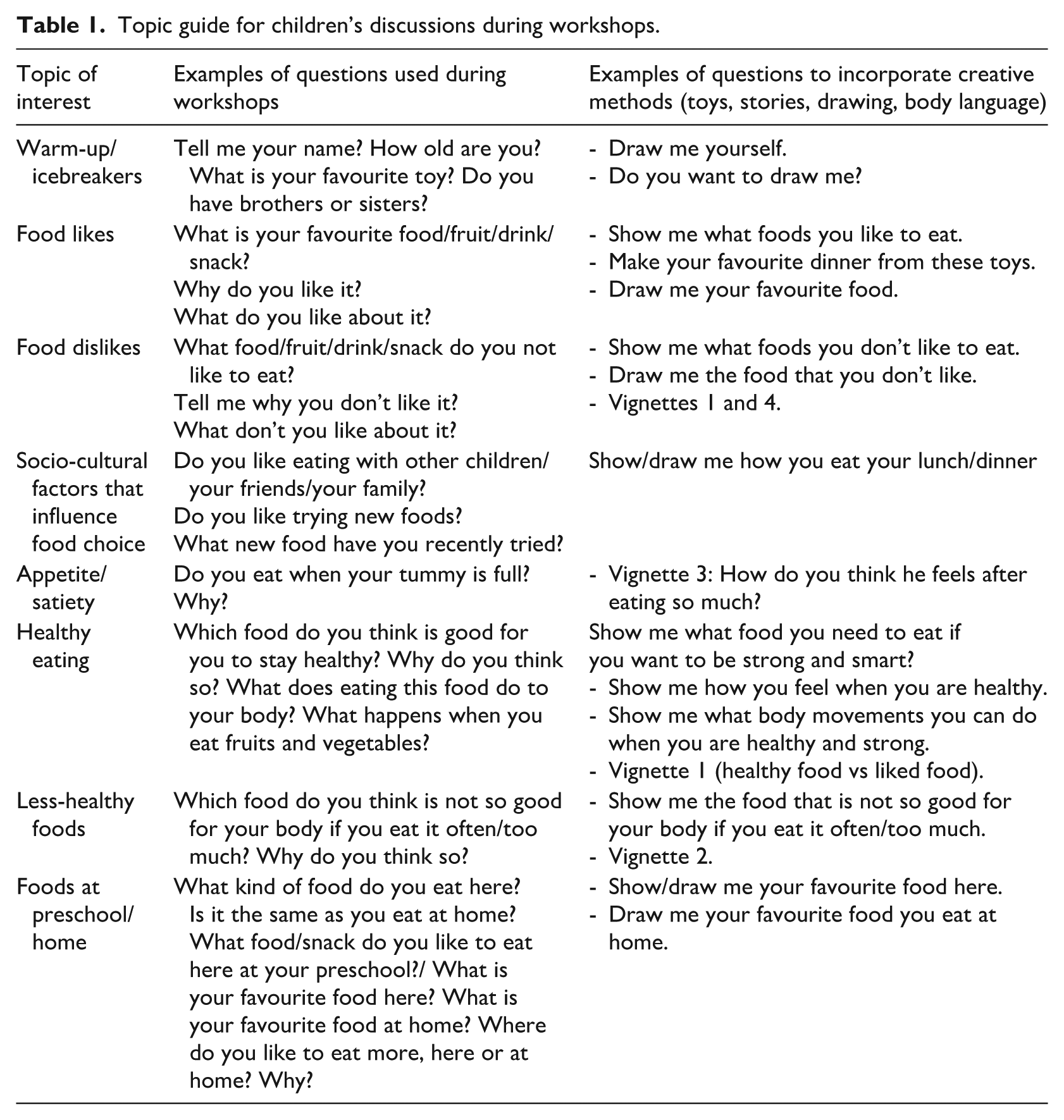
Researchers developed an age-appropriate semi-structured topic guide (Table 1) with open-ended questions about 3–5-year-old children’s perceptions of food. The topic guide was pilot tested with a group of five preschool children. All children understood and answered the questions verbally in varied ways, and therefore only minor changes were made.
Topic guide for children’s discussions during workshops.
Children’s workshops
Children’s workshops were conducted in each preschool with one or more small groups of two to five children. Children with parental consent were seated at the same table in a quiet area on-site. After explaining the study and obtaining children’s assent, the researcher discussed their friendships and families to build rapport. Then the researcher asked children if they would like to play a game with food toys and ‘make’ their favourite dinner. After the game-based activity with toys, the researcher invited children to discuss different scenarios using vignettes. Vignettes are short stories, often with accompanying pictures, about hypothetical characters in specified circumstances. Participants are invited to respond to elicit participants’ perceptions, beliefs and attitudes about the topic in the vignette (Palaiologou, 2017). In this study, the children were shown four pictures, and the accompanying short stories were read aloud by the researcher. The vignettes described different child characters, their food preferences and their behaviours in various situations such as ‘healthy eating’, ‘less-healthy eating’, ‘moderation when eating’, and ‘how children feel when eating food they dislike’ (Figure 1).
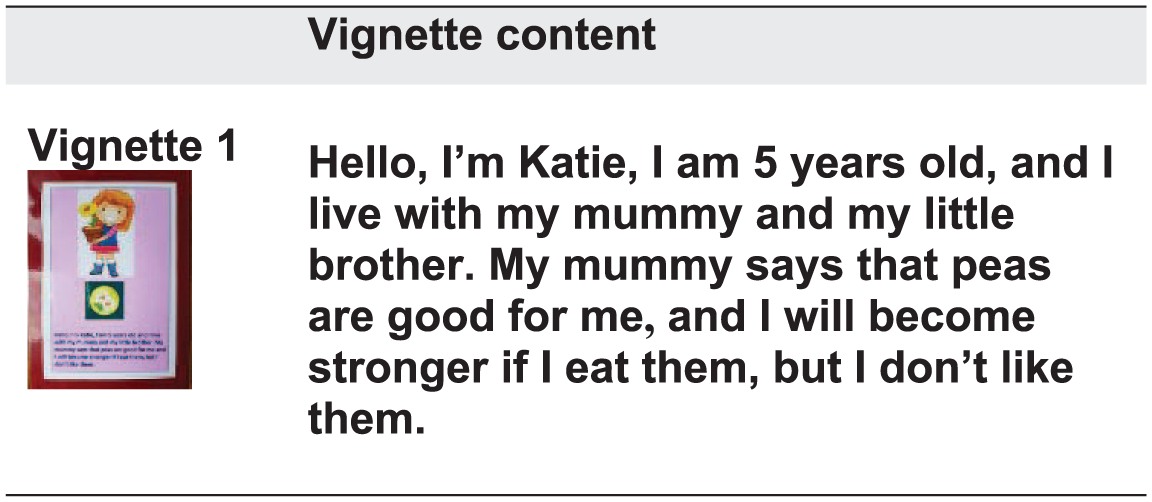
Example of a vignette used in the study.
In this study, ‘healthy’ food was defined as food that can be eaten often, and ‘less-healthy’ food as food that can be eaten sometimes. The researcher was aware that the language used to describe food can shape children’s attitudes and beliefs and has a powerful influence on children’s relationship with food (Scaglioni et al., 2018). Therefore, when talking about food with children, the researcher used neutral language, avoiding reference to food as ‘good’ or ‘bad’ or categorising food as ‘junk food’ or ‘unhealthy’.
At the end of the workshop, the researcher invited children to draw and explain pictures of their food likes and dislikes. The topic guide (Table 1) was used throughout all three activities to ensure children were asked similar questions whilst still allowing the conversation to be spontaneous and personalised to gain an understanding of a child’s perspective. The researcher took notes immediately after the activity with each child and after each workshop.
Analysis
Three types of data (toys, vignettes, and drawings) together with field notes of discussions and researcher reflections were collected, audio-recorded and transcribed verbatim. Inductive thematic analysis was conducted (Braun and Clarke, 2013). First, transcripts were read multiple times, and initial thoughts and ideas were documented. Next, data collected from three research methods were integrated and analysed using NVivoPro11, which involved coding and categorising followed by identification of sub-themes. The sub-themes were compared for convergences (similar insights or evidence) and divergences (differing perspectives or findings). Further, the themes were agreed followed by refinement and naming themes, and direct quotes from participants were used for narrative descriptions of findings. The researchers discussed and debated the codes, sub-themes, themes and representative quotes at weekly meetings. Methodological triangulation of qualitative methods (toys, stories, and drawings) provided diverse perspectives on children’s food preferences and perceptions, enhancing data validity by reducing potential biases from using a single method (Patton, 1999). To increase the credibility of findings, the researchers had regular debriefing meetings to enhance the understanding of data, analysis process and interpretation of findings. On-going reflexive notes were kept about the study’s progress reflecting researchers’ views, thoughts, insights, interpretations and decisions about research tool development, data collection, analysis, coding process, and the researchers’ perceptions about the study’s themes that emerged during the research process.
Results
Ten preschools took part including full-daycare (n = 4) and part-time/sessional care preschools (n = 6). Seventy-one children with parental consent were recruited, however, seven children did not participate due to absence or sleep on data collection days. Therefore, 64 children participated in the study. Participants ranged in age from 3-years-2-months to 5-years-8-months, and 95% of participants were 4-year-olds and younger: 32 three-year-olds, 29 four-year-olds and 3 five-year-olds; 6% African, 16% Asian/Pacific Islander, and 78% White-Caucasian. The sample consisted of 42 girls and 22 boys.
Children’s food preferences
Children’s food preferences were collected through multiple methods, and counts of food preferences provided an overview of specific food preferences. Children’s food preferences consisted mostly of meats, fruits, vegetables, bread/grains, sweets, chips and pizza. Chicken was the children’s most popular food, followed by sausage, strawberry, carrot, and fish. In general, the number of foods that children liked was greater than the foods they disliked.
Results of thematic analysis of workshops
Six themes were identified that describe and explain children’s food perceptions and preferences: (1) Sensory appeal of food; (2) Emotions associated with food; (3) Family and social influences; (4) Healthy food is ‘good for you!’; (5) Internal and external cues to eat; (6) Variety and exposure to food.
Sensory appeal of food
The sensory aspect of food played a dominant role in how children described food and explained their preferences. All children described senses relating to taste, smell, sight, sound and touch. While playing, children were ‘eating’, smelling, and even biting the ‘food’. Taste was the most frequent sensory aspect described and was characterised as ‘yummy’, ‘yummy for my tummy’, ‘I like how it tastes’, ‘delicious’, or ‘yucky’, ‘don’t like its taste’. Other sensory aspects of food, such as touch and sound, were also described (‘crunchy’, ‘juicy’, ‘gooey’, ‘fizzy’ and ‘squishy’). Some children gave importance to the colour of food when explaining their food likes: “[I like it] because it’s red, it’s red in colour” [tomatoes] Boy-4-year-old; ‘because it’s brown’ [chicken] Boy-3yo; “it’s green [lettuce] Boy-3yo, ‘. . .because it’s purple and because it’s green’ [grapes] Boy-4yo; ‘because it has green in it and I don’t like green colour’ [broccoli] Girl-4yo.
Emotions associated with food
Children’s feelings and emotions associated with eating certain foods were very evident. Emotions such as feeling good, happy, sad, or proud were articulated by children: ‘[I like] strawberry - it feels good when eating it’ Boy-3yo; ‘Sometimes I eat it, when I eat it, I smile’. [lettuce] Girl-4yo; ‘Fish, it’s a big fish. Once my Daddy caught a big fish, and it was delicious!’ Boy-4yo. ‘Fish fingers, because they have fish in them, makes you happy’ Girl-4yo.
Family and social influences
During discussions and through their drawings many children referred to their family, predominately their parents, who had a major influence on their food preferences. For example, when discussing why children liked a certain food they said: ‘Because my mum said eat my egg’ [egg] Girl-4yo; ‘Because my Mummy and Daddy give me’ [sandwich] Girl-4yo; and food they disliked: ‘My Mummy drinks a lot and got sick’ [Coke] Boy-4yo., ‘Because they are made of pig and my Mummy said “No”’ [sausages] Girl-4yo; ‘Because I don’t like it because my Mummy doesn’t cook it’ [fish] Boy-3yo. Children’s food preferences were influenced by their familiarity with certain foods from daily experiences.: ‘[I like it] because I always eat it’ [egg] Boy-4yo; ‘Because I put it on my chips’ [ketchup] Girl-4yo. Children also demonstrated the food/cooking practices they observed or participated in at home.
Foods eaten by children when dining outside the home were described and fast-food outlets were predominantly mentioned (‘[I like it] because they are in xxx, there are chips and sausages there’ Girl-3yo). Children described popular fast-food establishments in Ireland, illustrating that food brands and outlets are familiar to preschool children.
Healthy food is ‘good for you!’
In general, children were more willing to talk about food they considered ‘healthy’ than ‘less-healthy’ food, and the number of foods children thought were ‘healthy’ was greater than the foods they considered ‘less-healthy’. Children associated ‘healthy’ foods with ‘nice food’ and ‘goodness’. Healthy food was described as something that makes them ‘big’ and ‘strong’, ‘is good for you’, and ‘makes you grow’. Fruits and vegetables were commonly labelled as ‘healthy’ foods, while fewer children identified sweetened drinks and chips as ‘less healthy’. Their food dislikes were categorised as ‘less-healthy’ foods and were mostly associated with ‘not growing’, being ‘small’, and becoming ‘weaker’ or ‘sick’. However, although the majority of children had some idea about ‘healthy’ or ‘less-healthy’ foods, they could not elaborate further on how these foods affect health. Some children described the food as ‘bad’, ‘. . .because you won’t grow’ [white bread], and could suggest its healthier alternative, ‘It should be brown’ Girl-4yo. Others described it as ‘bad’ without giving a reason, ‘Popcorn bad. . . .But they are yummy!’ Boy-5yo. Children learned about healthy eating mostly from their parents with some influence evident from their preschool ‘Because my Mummy said I’ll be big’ [egg] Girl-3yo; ‘Because my Mum said [it is healthy]’ [strawberry] Girl-3yo; ‘My teacher told me they are nice’ [tomatoes] Boy-4yo).
Internal and external cues to eat
Children described feelings of hunger and fullness and how such feelings explain why some children did not eat their vegetables. For example, when discussing the vignette in which a ‘girl’ does not like the taste of peas, but her mother says she will get stronger if she eats them, children explained that the girl might ‘dislike’ peas, not because of the taste, but because ‘she is not hungry enough to eat it’ (Boy-3yo). However, other children described how they finish all their food, and this makes them stronger. Children’s conversations disclosed the ‘Eat all your food/clean your plate’ narrative: ‘I finish all my food’ Girl-4yo; ‘I eat all my lunch and I grow stronger’ Boy-3yo. Children gave these answers with a sense of pride.
Variety and exposure to foods
Children were excited to see such a variety of ‘foods’ in front of them and choose any ‘food’ they liked, ‘I like this. . . and this! . . .yummy! . . . and this!’ Children played with the ‘food’ and demonstrated their knowledge of preparing it in different ways, for example, ‘sandwich man’, ‘I can have it in different ways’ [egg] Girl-4yo. Children’s preference for variety was evident: ‘I like different [foods]’ Boy-5yo, ‘get sick of burgers and chips’ Boy-3yo. Children explained that repeated exposure and boredom (‘maybe he eats it every day’ Boy-3yo) may prevent from liking certain foods (e.g. broccoli). Similarly, children shared their experiences of trying new foods: ‘I kind of like them. I didn’t like eggs but now like them’ Girl-5yo.
Discussion
This study aimed to gain an understanding of 3–5-year-old children’s food preferences, perceptions of (healthy) food and influencing factors using research methods appropriate for this age group. The use of multiple methods provided each child with various opportunities to talk, demonstrate, or illustrate their food experiences and preferences. This child-led approach was based on fun and familiar activities and thus minimised the power relationship between the adult researcher and the child. Through respect for children’s opinions and perspectives, this research empowered even the youngest children to actively engage and input to the research process. The findings presented six main themes that give insight into children’s food preferences and perceptions.
The data illustrate several important factors that influence children’s food preferences and food choices. Consistent with previous research (Dazeley and Houston-Price, 2015) on young children’s engagement with food, this study showed that sensory appeal plays a major role in determining children’s food preferences. Children have a natural tendency to prefer sweet or salty energy-rich foods (Birch and Fisher, 1995), and this was reflected in children’s responses. Children described both taste and non-taste qualities of food in line with other work reporting that appearance, taste and texture were the most important reasons for the lack of children’s fruit and vegetable consumption (Zeinstra et al., 2010). Alternatively, it was reported that playing with food and feeling the texture of food with hands increases preschool-aged children’s acceptance of food with the same texture (Nederkoorn et al., 2018; Roberts et al., 2022). As Matheson et al. (2002) described, 5-year-old children classify food primarily based on its concrete, easily observed physical characteristics, including colour or shape, rather than more abstract criteria such as food groups. This study’s findings support this work while extending this assumption to 3–4-year-old children, and that the development of interventions to increase knowledge and experience of foods should include listening, seeing, touching and smelling food in addition to tasting it (Alsulami and Goodell, 2021). Thus, since liking various taste and non-taste attributes of food predicts young children’s food choices, emphasising the ‘nice’ taste/colour/sound, etc. of healthy foods and providing children with healthy foods they like could be efficient strategies to promote healthy eating habits in children.
Another theme evident from the data is emotions associated with food. Research on preschool children’s food-related emotions has mainly focused on emotional eating, such as over- or under-eating in response to negative emotions and its association with parental feeding practices (Powell et al., 2017). Very limited research about food-elicited emotions, particularly using a qualitative approach, has been conducted with preschool children to date (Alsulami and Goodell, 2021). The present study produced novel findings showing a relationship between food and emotions, both positive and negative, in children as young as 3 years. Alsulami and Goodell’s (2021) work with 4–5-year-old children found that children based their food-related emotions on past eating experiences and suggests that children learn to prefer foods associated with positive contexts and dislike foods presented with negative ones. The present study adds to the literature and demonstrates this among 3-year-olds. Clearly, social and emotional atmosphere during eating is important in children’s food-related decisions and should be considered when developing interventions for very young children. Our work supports the call for more research on food-related emotions in preschool-aged children.
An important aspect of associative learning during very young children’s food experiences is seen through family and social influences. Higgs and Thomas (2016) argue that social influences on eating are powerful and pervasive. The present study highlights the central role of parents in the acquisition of eating habits of preschool children, which conforms with other studies (Gibson et al., 2020; Strzelecka et al., 2022). Familiarity with food was another factor influencing children’s food preferences. This finding is supported by preschool children’s food acceptance studies, indicating that repeated opportunities to taste unfamiliar foods result in increased liking and consumption (Aldridge et al., 2009). According to Cooke (2007), children like what they know, and they eat what they like; thus, children’s experiences with food strongly influence their preferences and intake. Therefore, caregivers play a critical role in determining which kinds of foods will become familiar to their children. Indeed, children who, from an early age, have plentiful opportunities to sample a variety of healthy foods appear to have healthier diets throughout childhood (De Cosmi et al., 2017).
Children’s understanding of ‘healthy’ and ‘less-healthy’ foods was limited, especially in the youngest children; however, most children could show a rudimentary understanding of this concept. In line with previous research on young children’s knowledge about healthy and unhealthy foods (Nguyen et al., 2011; Tatlow-Golden et al., 2013), this study found that 3–5-year-old children were better able to identify ‘healthy’ foods compared to ‘less-healthy’ foods. Conversations with children, particularly discussions of the vignettes, provided insight into what types of foods children consider healthy and unhealthy. Like existing work (Holub and Musher-Eizenman, 2010; Tatlow-Golden et al., 2013), children associated ‘healthy’ and ‘less-healthy’ foods with their personal preferences. For example, many children stated that food was ‘healthy’ because they liked it or ‘less healthy’ because they did not. Similarly, in a study by Sigman-Grant et al. (2014), when children were presented with health-related statements (e.g. ‘A healthy food is good for you’), most children associated the term ‘good for you’ with taste rather than health, suggesting lack of reasoning behind their food choices. In support of work by Tatlow-Golden et al. (2013), our findings that 3-year-olds were less able than 4-year-olds to express whether food was healthy or unhealthy corroborate their assumption that understanding of health and nutrition concepts starts to develop by the age of 4 years. Research shows that by age 4 years, children appropriately apply the evaluative categories of healthy and unhealthy foods to a variety of foods (Lafraire et al., 2016). By the same age, children can generalise or extend information learned about one food, particularly its potential impact on the human body, to another food of the same evaluative category. This is an important ability and may be related to children’s own health and well-being as they make decisions about what foods to eat. Furthermore, when health is presented in a strategic, intentional language using simple concepts, combined with repetitive activities that promote familiarisation and associative and observational learning, this provides a concrete understanding of the relationship between health and food and helps children use their knowledge about health and guide their food choices (Birch and Anzman, 2010). These findings, suggesting that children begin to show signs of understanding the reasoning behind these food classifications by age 4 years, may be used to develop age-appropriate nutrition education programmes.
Another important finding in this study was that 3–5-year-old children demonstrated their capability to recognise internal and external cues to eat. However, some children demonstrated a willingness to eat food beyond their satiety level as they perceived that ‘eating all food on the plate’ was praiseworthy. This is noteworthy because children can be offered large quantities of food, which, as evidence suggests (Norton et al., 2015; Reale et al., 2019), they can and will eat, overriding their satiety cues. The present study’s findings align with evidence that although young children are highly capable of self-regulation of their energy intake, the extent to which they exercise this ability is determined by environmental conditions (Hughes and Frazier-Wood, 2016; McCrickerd, 2018). In addition, when children are forced to eat foods usually perceived as ‘good for them’, this can produce dislikes for these very foods (Boots et al., 2019; Roberts et al., 2022). Similarly, if food is presented as instrumental to being healthy, that is, ‘makes you strong’, this negatively impacts its consumption as children assume that food that offers instrumental benefits would be less tasty (Maimaran and Fishbach, 2014). Therefore, this study suggests that serving appropriate amounts of food to young children and letting them eat until they are satisfied are important messages for preschool staff and parents. In addition, placing ‘value’ on food (e.g. good vs bad foods) can be counterproductive, and a shift in focus to discussing food in the context of its origin, impact on the planet, and health would be preferable. Interventions promoting healthful eating among 3–5-year-old children should consider the role of appetite, feelings of satiety and hunger and encourage children’s self-regulation of food intake. Haines et al. (2019) argue that structure and autonomy support are important feeding practices in early years and are associated with better outcomes for children’s eating habits than more coercive practices, for example, food restriction and pressure to eat. In this context, feeding strategies that are responsive to hunger and satiety, encourage children’s attention towards these cues, and support their self-regulation, should be promoted.
Finally, children clearly expressed their preference for variety in the foods they eat. This contrasts with much of the existing research that 3–5-year-old children are ‘fussy’ and ‘picky’ eaters, and the majority of them do not tend to try new foods at this age (Patel et al., 2020). However, currently, there is little evidence on whether 3–5-year-old children hold food variety-seeking preferences (Ahl and Dunham, 2020). Ahl and Dunham (2020) in their quantitative study observed a variety-seeking food behaviour in 5- and 6-year-olds, but not 3- and 4-year-olds and explained it by the fact that younger children were not asked to reason this behaviour. The present study employed a qualitative approach and found that the youngest children (aged 3–4 years) undoubtedly prefer a variety of foods while expressing boredom from repeatedly consuming the same food. This finding is encouraging since food variety contributes to children’s nutritional diversity and adequacy of the diet (Steyn et al., 2006). In addition, a higher dietary variety among young children is linked with a higher general enjoyment and interest in food (Vilela et al., 2018). However, as this study is exploratory and its generalisability is limited, larger-scale studies are needed to investigate food variety-seeking behaviours of 3–5-year-old children and the ways to support them. A limitation of this study is that the food toys may not accurately represent the cultures of children from ethnic minorities. However, offering these children different ways to express their food preferences, such as through drawings and open discussions about food, could have helped address this limitation.
Implications for research and practice
The study adds to the literature on 3–5-year-old children’s preferences and perceptions of food and healthy eating by applying a mix of creative methods that empowered children to actively participate in research and express themselves freely in a variety of ways. The child-led and familiar activities minimised the power dynamics between the researcher and the child and produced meaningful data.
The findings of this study highlighted diverse influences on children’s food preferences, including familiarity with foods and parental modelling. The sensory appeal of food, a variety of food and the role of appetite, satiety, and hunger, and encouraging children’s attention towards these cues in supporting their self-regulation deserve greater recognition and application in interventions designed to promote healthy eating and positive relationships with food among 3–5-year-old children. The study produced novel data showing that a relationship between food and emotions is evident in children as young as 3 years of age. As social and emotional atmosphere during eating is important in children’s food-related decisions, this should be considered when developing interventions for very young children. The development of interventions to increase 3–5-year-old children’s knowledge and experience of foods should include non-taste experiences in addition to tasting a variety of foods. Overall, this study suggests that nutrition education programmes should build on children’s everyday experiences, promote consumption of a variety of foods and positive emotions associated with food, use hands-on learning to facilitate acceptance of new and varied foods, and encourage children’s self-regulation of food to meaningfully shape their food behaviour. Thus, efforts to improve food standards alone in early care settings will not be sufficient to promote healthy food choices without consideration of the diverse influences on food preferences identified in this study. Additionally, given the significant role of parents in shaping children’s food perceptions, good communication between early care settings and parents can inform families’ food choices and, in turn, facilitate children’s acceptance of healthy foods.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Hardiman Research Scholarship, University of Galway
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.