
Abstract
The restructuring of the psychotherapist training in Germany has increased the demand for university-based teaching strategies that effectively support the development of practical psychotherapeutic competencies. This exploratory study applies the concept of professional vision, established in teacher training, to psychotherapy education. It investigates differences in perceptions of therapeutic processes in two therapy videos between students and psychotherapists in training, who were combined into one group (n = 60) based on a manipulation check on self-rated experience in trauma treatment, and experienced supervisors (n = 30). Using a mixed-methods design, we combined quantitative ratings of relevant therapeutic processes (therapeutic relationship, competence, and affect) with qualitative analyses of verbal data, focusing on the components of knowledge-based reasoning (description, explanation, and prediction) as part of professional vision. Qualitative results indicated that supervisors were more advanced in describing and explaining as well as in predicting therapeutic processes, although these differences were not consistent across all domains examined. Quantitative analyses revealed only limited differences in the ratings between the groups. Practical implications for the design of instructional formats are derived and considerations for future research in this area are discussed. This study provides initial evidence for applying the concept of professional vision to psychotherapeutic education.
Introduction
The training of psychotherapists in Germany has recently been restructured (Der Bundestag, 2019). Before the reform, students had to complete a bachelor's and master's degree in psychology (including some courses in clinical psychology), followed by 3 to 5 years of postgraduate training outside the university to become a psychological psychotherapist. Practical psychotherapeutic skills were mainly acquired in the postgraduate training under supervision, whereas the focus of the university course was mainly theoretical and content-related (Wilhelm et al., 2020). Due to the new licensing requirements for psychotherapists, many universities have now implemented a direct master's program in psychotherapy after a polyvalent bachelor's degree in psychology. This means that the former postgraduate psychotherapeutic training is now integrated into university-based master's programs within established psychology departments (Alpers & Hengen, 2021). It concludes with a licensing examination, and if passed, students are authorized to treat clinical patients. Subsequent postgraduate training is still required, but the right to practice is granted directly. Consequently, practical skills must be tested in the licensure exams at the end of the master’s program. Therefore, the implementation of new teaching formats with practical clinical components in university psychology programs is needed to enable students to develop psychotherapeutic skills and to apply their theoretical knowledge in practice.
In this context, the question arises how psychotherapeutic competencies are developed and how this development can be didactically supported in university teaching. This exploratory study draws on the established concept of professional vision (PV) from educational psychology and teacher research (van Es & Sherin, 2002, 2008) and applies it to the context of psychotherapy training, examining it across different levels of training. The study may contribute to the support of university teachers in promoting the development of therapeutic competence in psychology students in university teaching.
Theoretical Background
Models of Therapeutic Competence
The concept of therapeutic competence is a relatively new one (Wampold et al., 2018), but it is a central topic in psychotherapy research (Caspar et al., 2021). Although there are several definitions and models of therapeutic competence, a universally accepted standard is still lacking (Koddebusch & Hermann, 2018). The German Federal Chamber of Psychotherapists (Bundespsychotherapeutenkammer, 2008) divides therapeutic competence into professional-conceptual skills (e.g., knowledge of models of mental disorders and treatment options), personal skills (e.g., ability to self-reflect and empathy), and relational skills. This last group of skills includes not only the ability to establish and maintain a stable therapeutic relationship but also the ability to differentiate between one's own and another's affect: Therapists must be able to perceive emotions and provide patients with access to their emotions for therapeutic change (Holl et al., 2020). At the same time, it is important for therapists to be able to regulate their own emotions (Caspar et al., 2021). Overall, the importance of the ability to establish a good therapeutic relationship has long been known and generally accepted (Caspar et al., 2021). Patients find it particularly important for therapists to show empathy and appreciation (Orlinsky et al., 1994).
Sharpless and Barber (2009) outline five stages of competence development, from novice to expert. Weck (2013) describes which psychologists fit each group. In stage 1, novice, the focus is on learning and applying rules. Psychology students are typically at this stage. In stage 2, advanced beginners, previous experience in treating patients can be applied to new therapy situations but it still requires intensive reflection and supervision. Therapists in the initial phase of their training often fall into this stage. In stage 3, competence, therapists can identify core symptoms and tailor treatment to patients’ needs. It is often seen in students in advanced psychotherapy training. Stage 4, proficiency, involves the use of a more intuitive approach that requires fewer cognitive resources. It is reached at the end of the therapeutic training or in further clinical work after the training. Finally, in stage 5, expertise, therapists take appropriate therapeutic actions without consciously following rules, relying on years of practical experience. In line with this model, Caspar (2017) emphasizes that psychotherapeutic training should aim to develop intuitive and differentiated information processing skills.
However, a clear operationalization and reliance on empirical evidence for the described competencies is often lacking, and qualitative aspects of how these competencies are acquired remain largely unaddressed (Koddebusch & Hermann, 2018), leaving open the question of how best to support the acquisition of psychotherapeutic competencies from a didactic perspective in psychology education. To address this conceptual and empirical gap, this study transfers the concept of PV, well-established in the field of teacher education, to the field of psychotherapeutic competence development. In doing so, this study is used as a starting point to explore PV in this area.
Professional Vision
The concept of PV was introduced by Goodwin (1994) and refers to findings that actions and events are perceived and interpreted differently by members of different professions. (Van Es and Sherin, 2002, 2008) applied PV to the context of teacher education. There, it is seen as a prerequisite for successful teaching practice (Sherin, 2007). PV refers to the teacher's ability to notice and interpret learning-relevant events in the course of teaching based on their theoretical knowledge. They describe two components: noticing and knowledge-based reasoning. Noticing involves perceiving important situations in the classroom that are essential for effective teaching from the teacher's professional perspective (Seidel & Stürmer, 2014). Knowledge-based reasoning involves processing the identified situations in a knowledge-driven manner (e.g., by incorporating theories and prior knowledge). Seidel and Stürmer (2014) propose three basic components of knowledge-based reasoning: description (i.e., the ability to identify and distinguish relevant events without making evaluative judgments), explanation (i.e., linking classroom events to broader instructional knowledge and categorizing them) and prediction (i.e., the ability to anticipate the outcomes of observed classroom events). PV overlaps with skills commonly emphasized in psychotherapy training, such as clinical reasoning and case conceptualization, but differs in focus and function. Clinical reasoning involves integrating various forms of knowledge to make diagnostic and treatment decisions (Yazdani & Hoseini Abardeh., 2019). Case conceptualization refers to organizing and synthesizing client information into a working model that guides individualized interventions in psychotherapy (Eells, 2015; Sperry & Sperry, 2020). Both emphasize analytical, hypothesis-driven reasoning. In contrast, PV centers on the perceptual and interpretive processes that enable practitioners to notice and make sense of relevant cues in complex situations (Goodwin, 1994; van Es & Sherin, 2002).
Previous research has often used videotaped classroom situations to examine the components of PV (e.g., Gold & Holodynski, 2017; Seidel & Stürmer, 2014). Few studies have examined noticing using eye-tracking, while more studies have examined the components of knowledge-based reasoning using video analysis and interviews (Grub et al., 2020). Empirical studies confirm differences in PV between novices and experienced in-service teachers: while novice teachers can describe classroom situations, their ability to accurately explain and predict the consequences and outcomes of these situations is not as advanced as that of experienced in-service teachers (Schäfer & Seidel, 2015). Analyses of verbal data suggest that novice teachers tend to describe teaching situations in simplistic and superficial terms, whereas experienced teachers use their conceptual knowledge more effectively to contextualize, elaborate, and interpret such situations (Stürmer et al., 2015). Meschede (2013) concludes from comparative studies that experts can perceive teaching more professionally than novices due to their more pronounced knowledge structure. As professional vision can be seen as the basis for adaptive teaching practices (Jürgens, 2021), it should be developed during the initial teacher training (Stürmer et al., 2015). Therefore, university courses have been developed and it has been shown that PV can be promoted through video training (Gold et al., 2013).
Transferred to the context of psychotherapeutic competence development, videotaped psychotherapy clips could be used to study PV in groups with different levels of expertise in psychotherapy, assuming that differences in the components of PV could also be observed here.
The Current Study and Research Questions
Recent reforms in psychotherapist training in Germany highlight the need for practice-oriented training in the teaching of psychology to support effectively the development of psychotherapeutic competencies. Our study employs a quasi-experimental design with videotaped therapy clips to examine differences in the perception between psychology students, psychotherapists in training (PiTs), and supervisors on two levels: qualitative analyses of verbal data, focusing on the components of knowledge-based reasoning as part of PV, and additional quantitative ratings of important therapeutic processes in psychotherapy.
Transferring the concept of PV, more specifically knowledge-based reasoning, to the context of therapeutic competence development, we were interested in the following: RQ1: Are there differences between groups with different levels of training (students, PiTs, supervisors) in the extent of description, explanation and prediction as part of knowledge-based regarding relevant therapeutic processes when watching videotaped psychotherapeutic sessions?
As described in the stage model (Sharpless & Barber, 2009; Weck, 2013), therapists with different levels of competence behave differently in therapy situations. While the qualitative verbal data were conceptually aligned with the concept of PV, the quantitative ratings served as an exploratory supplement to assess whether the different groups evaluate relevant aspects of therapeutic processes in videotaped therapy sessions differently. Since, to our knowledge, no study has examined differences in the ratings of psychotherapeutic processes between different groups of psychotherapy training, we formulated this exploratory research question: RQ 2: Are there differences between groups with different levels of training in the quantitative ratings of relevant therapeutic processes (e.g., therapeutic competence, therapeutic relationship, affective states of patients and therapists) in videotaped psychotherapeutic sessions?
Methods
Sample
The sample consisted of N = 90 participants (77 female, 13 male) with three subsamples:
n = 30 master's students in psychology; we classified this sample group as novices (stage 1; Sharpless & Barber, 2009). n = 30 PiTs with at least 6 months of training in cognitive behavioral therapy. (M = 2 years of professional experience treating patients, S = 8 months); corresponding to stage 2 (advanced beginners) to stage 3 (competence; Sharpless & Barber, 2009). n = 30 supervisors, that is, licensed cognitive behavioral psychotherapists with at least 5 years of professional experience, working as supervisors in a postgraduate training institute (M = 19.5 years, S = 8.67 years); corresponding to stage 5 (experts; Sharpless & Barber, 2009).
Inclusion criteria for participation were sufficient knowledge of German, written consent to participate and to maintain confidentiality. Participants received monetary compensation. Students received 15€, PiTs 75€ and supervisors 150€. The amounts varied between groups, as PiTs and especially supervisors seemed to require higher financial compensation for their loss of earnings due to their participation in the study. We recruited participants via flyers and emails to mailing lists and extended professional networks. We collected data between July 2022 and May 2023.
Study Design and Procedure
We used a mixed-methods approach with a between-subjects design (training level). One of three trained investigators conducted the study individually with each participant, which lasted approximately 90 minutes. We informed them that they would view two 10-minute therapy video clips, each divided into two parts, featuring sessions with patients who had experienced interpersonal trauma. Participants were randomly assigned beforehand to view one of the two videos first. Patient anonymity was maintained, and all participants confirmed that they did not know the patients in the videos. We provided them written background information on the context of the therapy video (e.g., type of trauma and previous interventions). They watched the first part of the first video and we offered them to take notes. Afterwards, the experimenter asked them to describe their perceptions freely, recorded the verbalizations and took notes on a prepared protocol form. We showed the second part of the first video and repeated the procedure. After watching both parts of the first video, participants answered additional questions in a semistructured interview. Next, participants completed online questionnaires assessing the therapeutic relationship (Helping Alliance Questionnaire; Bassler et al., 1995), emotional intensity of patient and therapist (Positive and Negative Affect Scale [PANAS], Krohne et al., 1996), and therapeutic competence (Cognitive Therapy Scale [CTS], Weck et al., 2010). The entire procedure was repeated for the second video, featuring a different patient–therapist dyad. Finally, participants provided demographic information (gender, professional experience). They also rated their experience in providing trauma-related treatment on a 5-point Likert scale. We used this as a manipulation check to assess whether the groups differed beyond their formal affiliation, possibly resulting in a group merge for further analyses.
Material and Measurements
Video Clips
The video clips used in this study were recorded for supervision purposes as part of the research project “C-Metta: Cognitive Techniques and Metta Meditations to Reduce Trauma-Related Feelings of Guilt and Shame” (Müller-Engelmann et al., 2024). C-METTA is a 6-session intervention that combines cognitive techniques and Metta meditation (for a more detailed description, see Müller-Engelmann et al., 2024). We selected video clips of trauma therapy sessions because trauma treatment requires specific therapeutic competencies (American Psychological Association, 2015).
The main author preselected possible video clips from four patient-therapist dyads out of 17 available video therapy sessions and discussed them with one of the co-authors. We selected the clips because we perceived the competence within the clips to be neither clearly positive nor clearly negative, following Seago's (2003) recommendation that “the most useful video clips were based in situations where there was some elements of confusion” (p. 267). While we perceived the therapy situation in video 1 (V1) to be more exploratory in nature, we found the therapy situation in video 2 (V2) to be very structured in procedure. V1 is from session 1 and 9 min long, V2 is from session 5 and 12 min long. Therapists and patients wore face masks as C-Metta took place during the COVID-19 pandemic.
Helping Alliance Questionnaire
The HAQ (Bassler et al., 1995) measures the quality of the therapeutic relationship. It can be completed by patients and therapists. Agreement with 11 statements is measured on a six-point Likert scale (1 = strongly disagree, 6 = strongly agree). For the present study, we reformulated the items so that the respondents rated the therapeutic relationship between patient and therapist (e.g., I have the impression that the therapist understands the patient).The reliability proved to be excellent for both videos (Supplemental Appendix 1).
Cognitive Therapy Scale
We used the CTS (Weck et al., 2010) to assess therapeutic competencies. This scale assesses different therapeutic competencies (e.g., clarity of communication, focusing on key cognitions and behaviors) using 14 items on a seven-point scale (0 = poor, 6 = excellent). We excluded three items (agenda, revising homework, and homework assignment), because they could not be assessed on the basis of the video clips and computed a total score of the included items. The internal consistency was excellent for both videos (Supplemental Appendix 1). Furthermore, we added two global items, one assessing the overall therapeutic competence, one assessing the treatment difficulty, again on a seven-point scale.
Positive and Negative Affect Schedule
The German version of the PANAS (Krohne et al., 1996) measures positive (PA) and negative affective states (NA) with 20 adjectives (e.g., interested, upset). Participants were asked to rate the intensity of the therapist's and patient's affective states at the time of the video using a five-point scale (1 = not at all, 5 = extremely). The internal consistency of the NA scale (therapist) was questionable for V1—in all other comparisons, the internal consistency was acceptable, high, or excellent (Supplemental Appendix 1).
Think-Aloud and Semistructured Interview
After each video clip, we asked participants to describe their perceptions freely and recorded their verbalizations. We were interested in whether the participants commented on the following seven areas, which are considered important factors in psychotherapy and analogous to the quantitative scales above: the therapeutic relationship, the affective states of the patient and the therapist, the therapeutic competencies in general, and in particular, the structuredness, the clarity of communication, and the appreciation of the patient. On the record sheet, we indicated in each case whether they described the construct (i.e., they named the construct, e.g., the therapeutic relationship was good), whether they explained the description (i.e., whether they said how they noticed that the therapeutic relationship was good, e.g., the patient opened up to the therapist), and whether they made a prediction about the construct (i.e., how they thought the therapeutic relationship would be in future sessions). In the following interview, we repeated what we had noted for each construct and asked if they wanted to add anything. If they had not said anything about the specific construct, we asked them to describe it, explain it, and make a prediction about it.
Coding of Audiotapes
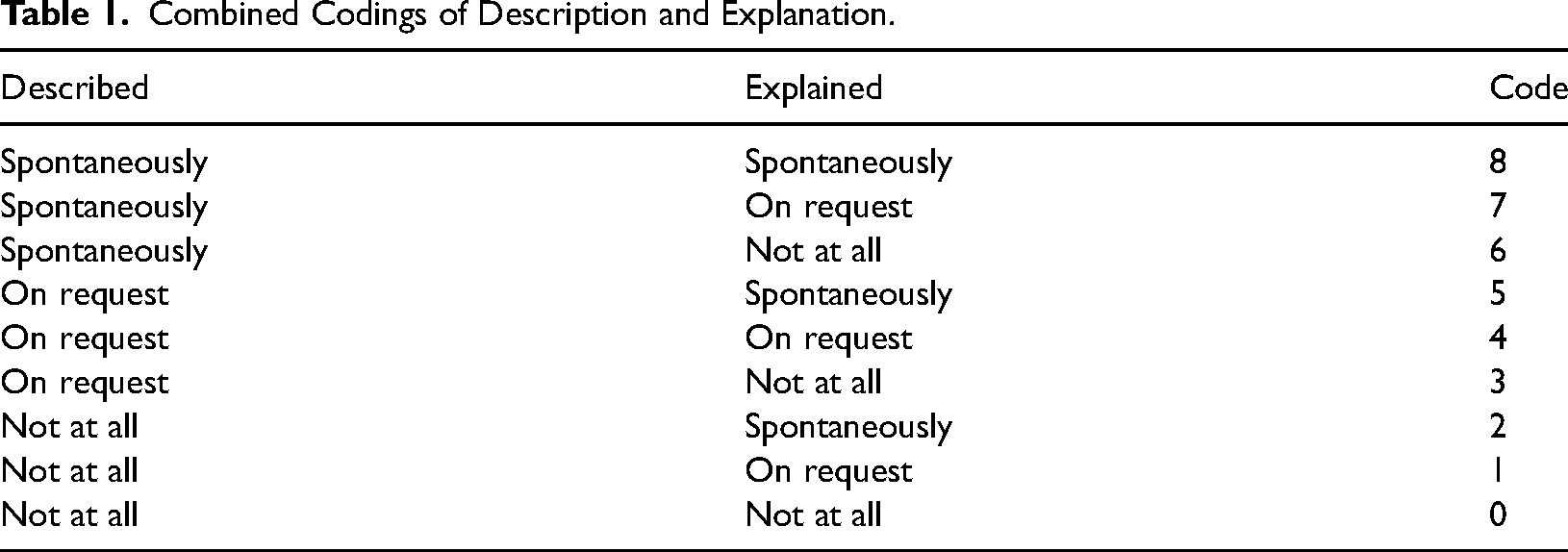
We developed a coding manual to assess whether the three components of knowledge-based reasoning—description, explanation, and prediction—were addressed by participants spontaneously (i.e., during the think-aloud process), on request (i.e., in the interview), or not at all for each of the seven areas. As we discovered during the coding process that the results are more meaningful when we combine the codings of describing and explaining, we performed a combined rating of these components, resulting in the following possible codes (Table 1).
Combined Codings of Description and Explanation.
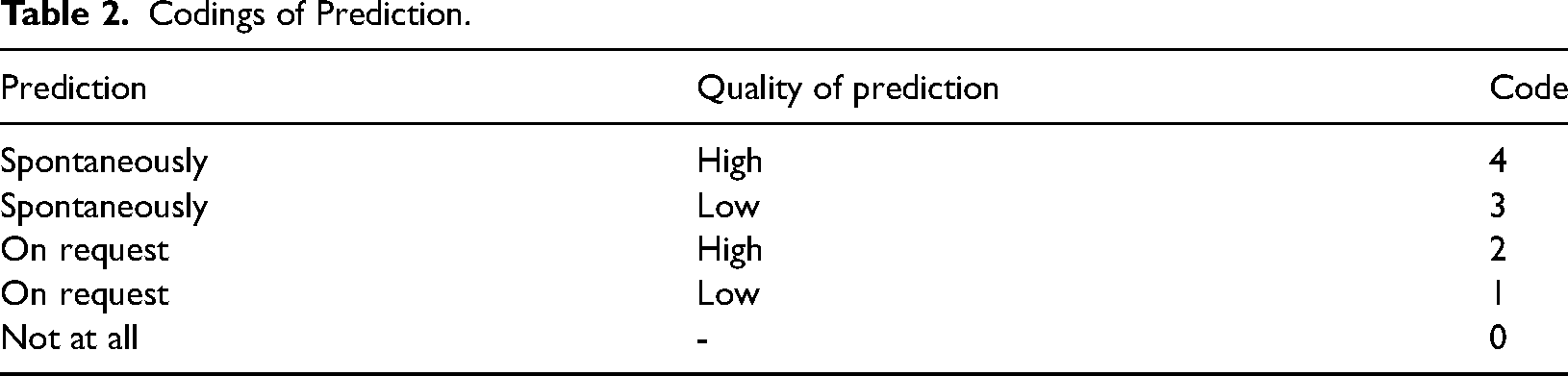
For the codings of the prediction component, we rated whether they made a prediction spontaneously or on request and whether the quality of the prediction was high or low. For example, if a participant simply stated that competencies will remain the same without further elaboration, we coded it as low quality. However, if additional justification was provided or the prediction was presented in a more nuanced way, we coded it as high quality. This resulted in five possible codings (Table 2).
Codings of Prediction.
In one case, the recording of V1 (student 8) failed, so the verbal data in this case were unusable. Errors in the study's execution led to some missing values across all verbal codes, particularly among supervisors and students in the predictions. The affected codes were excluded from the analysis, which resulted in slightly reduced group sizes for individual comparisons (see Supplemental Appendix 2). While this led to minor variation in group sizes for some comparisons, the overall rate of missing data remained low (3.8%) and did not systematically affect the interpretation of results.The main author and two student assistants coded the interviews. To assess the interrater reliability, all raters coded nine interviews and two raters coded an additional nine interviews, resulting in significant consistency for three raters (Fleiss’ Kappa = .70) and excellent consistency for two raters (Cohen's Kappa = .85).
Results
Manipulation Check
To test for differences between the groups regarding the self-rated experience with treating trauma-related disorders, a one-way analysis of variance (ANOVA) was conducted. Results indicated a significant effect, F(2, 87) = 46.03, p < .001, η²p = .51. Tukey post hoc analysis revealed significant differences (p < .001) between supervisors and students (1.57, 95% CI [1.07, 2.06]) and between supervisors and PiTs (1.83, 95% CI [1.34, 2.33]), with supervisors reporting significantly higher experience. No significant differences were found between students and PiTs, p = .40 (.27, 95% CI [−.23, .76]). These results suggest that supervisors differ from students and PiTs not only in their formal affiliation, but also in their self-rated experience with treating trauma-related disorders. However, differences between PiTs and students were not empirically supported, indicating similar self-rated experiences. Descriptive statistics of the variables confirmed the similarity between these groups (Supplemental Appendix 3). Consequently, we merged students and PiTs into one group for further analyses, resulting in a combined group of students and PiTs (n = 60), alongside supervisors (n = 30).
RQ1
First, we created two frequency plots with the relative frequencies of the different codings of describe and explain and predict within both groups across the areas of interest in both videos to map descriptive differences. Figure 1 shows that supervisors achieved the highest knowledge-based reasoning score, that is, they spontaneously described and explained the areas of interest across all areas in V1 and V2, in 41% of their codes, compared to 33% for students and PiTs. Supervisors also had fewer instances where areas of interest were neither described nor explained than students and PiTs (2% vs. 6%).
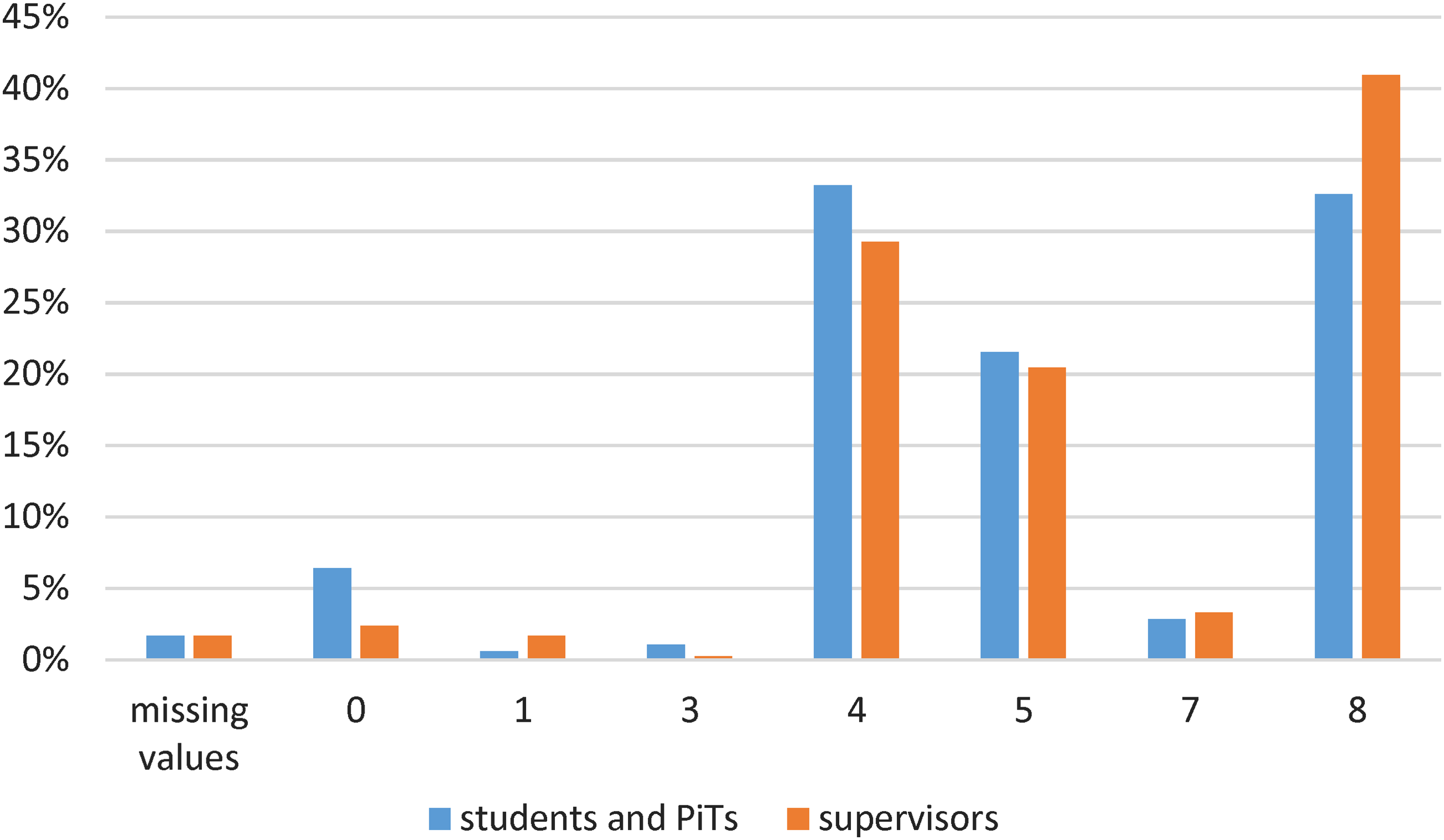
Relative frequencies of the different codes within each group for describe and explain across all variables, for videos 1 and 2. 0 = Not described and explained, 1 = not described, explained on request, 3 = not described, explained on request, 4=described and explained on request, 5 = described on request, explained spontaneously, 7 = described spontaneously, explained on request, and 8 = spontaneously described and explained. Note that code 2 and code 6 were not assigned.
Figure 2 shows that none of the subjects made spontaneous predictions across areas of interest in both videos. Supervisors made high-quality predictions more frequently on request (54% of their codes) than students and PiTs (47%). Students and PiTs made no predictions at all in 1.67% of the cases, compared to 0.7% for supervisors.
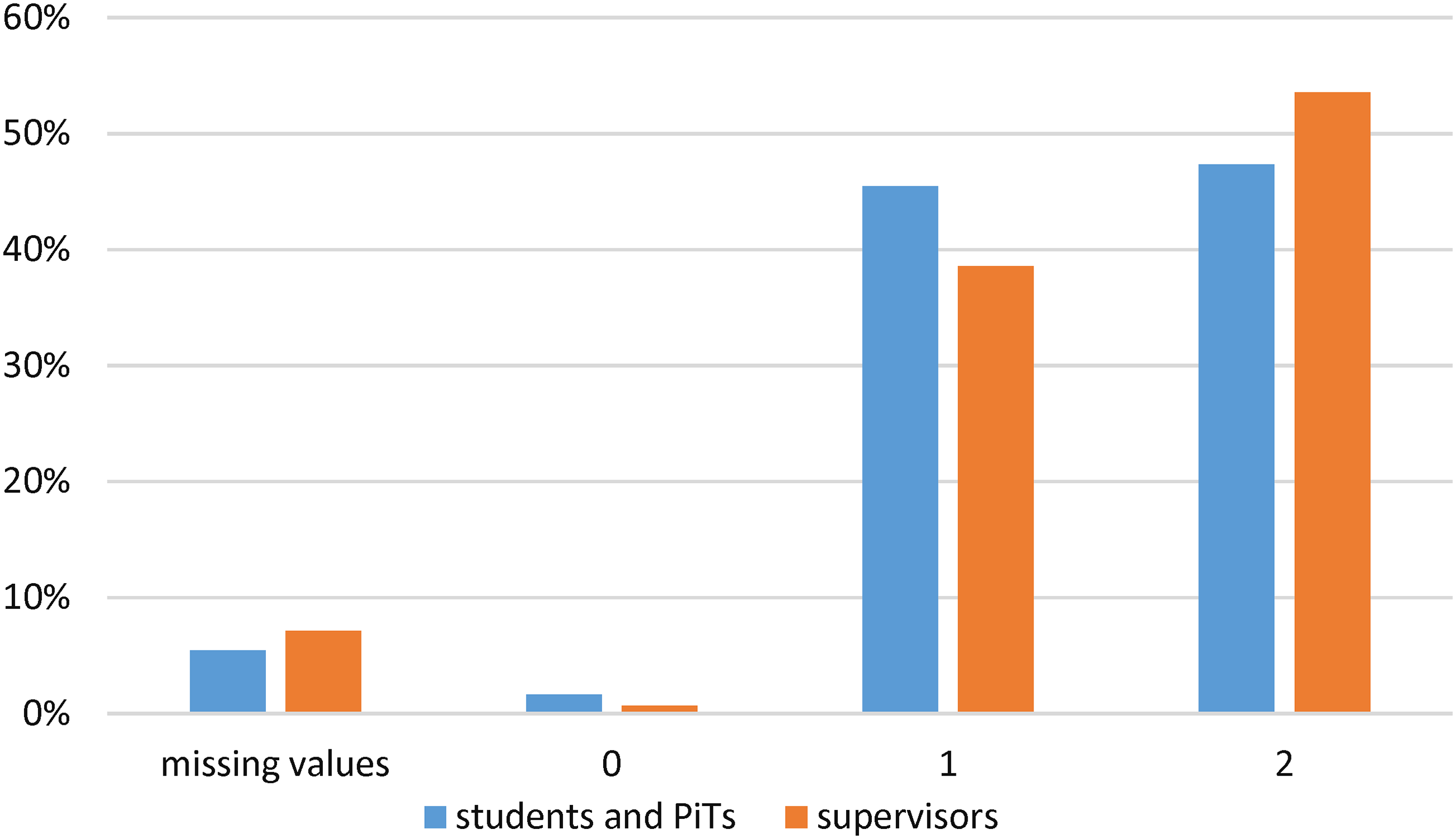
Relative frequencies of the different codes within each group for prediction across all variables, for videos 1 and 2. 0 = No prediction made, 1 = prediction on request, low quality, 2 = prediction on request, high quality. Note that code 3 and 4 were not assigned.
To statistically address RQ1, we conducted Mann-Whitney-U-tests based on the ordinal-scaled codings for description and explanation and for prediction for each of the seven areas of interest (therapeutic relationship, emotions of patient and therapist, therapeutic competencies in general, and especially the structuredness, clarity of communication, and appreciation of the patient). Because we presented two different videos as independent examples, we did not treat them as a within-subjects factor in the analyses. Instead, we conducted separate analyses for each video, as the clips differed in content, dyads, and therapeutic focus. To account for the exploratory nature of the study and to minimize the risk of type II errors, we did not apply Bonferroni correction for multiple testing (Armstrong, 2014 ). Two-tailed p-values are reported. Full results, including group sizes and test statistics for each comparison, are provided in Supplemental Appendix 2.
Description and Explanation
In V1, a Mann-Whitney-U-test indicated a significant difference in description and explanation of competence between supervisors (MRank = 55.50) and students and PiTs (MRank = 39.67), U = 570, Z = −3.38, p < .001, r = .36. Furthermore, there was a marginally significant difference in clarity of communication in V1 between supervisors (MRank = 49.45) and the other group (MRank = 41.28), U = 683, Z = −1.94, p = .05, r = .21, and a significant difference in clarity of communication in V2, U = 566.50, Z = −2.92, p = .003, r = .31, again with higher mean ranks for supervisors (MRank = 55.62) than for students and PiTs (MRank = 39.60). Additionally, a significant difference in therapeutic relationship in V2 was found between supervisors (MRank = 52.50) and students and PiTs (MRank = 42.15), U = 699, Z = −2.07, p = .04, r = .22. No significant differences in description and explanation were found for the other areas of interest.
Prediction
In V1, Mann-Whitney-U-tests indicated significant differences between supervisors (MRank = 50.79) and students and PiTs (MRank = 40.60) in predicting the therapist's own emotion management, U = 644, Z = −2.42, p = .02, r = .26. Similarly, significant differences were found in predicting how the therapist would manage the patient's emotions in V1, with supervisors showing higher mean ranks (MRank = 49.89) than students and PiTs (MRank = 41.20), U = 661, Z = −2.136, p = .03, r = .23. Furthermore, in V1, there were marginal differences between supervisors (MRank = 48.67) and students and PiTs (MRank = 40.73) in predicting the therapeutic relationship, U = 685, Z = −1.66, p = .097, r = .18. Marginal differences were found for predicting clarity of communication in V1, U = 567, Z = −1.85, p = .06, r = .21, with higher mean ranks for supervisors (MRank =46.69) than for the other group (MRank = 38.31). No further significant differences in prediction were found in V1 or V2.
RQ 2: Quantitative Ratings
We conducted separate t-tests for independent samples for V1 and V2 with the following dependent variables: total score of HAQ, total score of CTS, treatment difficulty, assessment of overall competence, PA and NA of patient and therapist affects (PANAS). For the same reasons mentioned above, we did not apply a Bonferroni correction.
The results indicated a significant difference in V2 in the rating of negative affect of the patient, t(88) = 2.01, p = .047, d = .45. Supervisors reported a lower mean score (M = 1.72, SD = .50) than students and PiTs (M = 1.96, SD = .53). Additionally, a significant difference in V2 was found for the rating of treatment difficulty, t(88) = 2.41, p = .018, d = .54, indicating that students and PiTs (M = 3.62, SD = 1.26) perceived the treatment as more difficult than supervisors (M = 2.93, SD = 1.29). No further significant differences were found for HAQ, CTS, and PANAS.
Discussion
This mixed-method study aimed to investigate differences in the perception of psychotherapy video clips and to transfer the concept of PV, more specifically knowledge-based reasoning, to the field of psychotherapy competence development to gain insights for teaching in psychology. To the best of our knowledge, no previous study has applied PV to this area and studied it across different levels.
First, the manipulation check confirmed that supervisors reported significantly more experience in trauma treatment than students and PiTs. However, no differences were found between students and PiTs, despite their different formal affiliations. After carefully weighing the advantages and disadvantages, we merged students and PiTs into one group for subsequent analyses, simplifying the comparisons between less experienced participants and experienced supervisors. One possible explanation for the similar self-assessment of experience could be that students overestimate their experience due to their existing theoretical knowledge. Vollmer et al. (2013) provide support for this, showing that while PiTs outperform students in practical tasks (e.g., case conceptualization and treatment planning), both groups have comparable levels of theoretical knowledge.
Second, analyses of the think-aloud process and subsequent interviews allowed us to test for group differences in knowledge-based reasoning about relevant therapeutic processes (RQ1). On a descriptive level, we found a superiority of supervisors on the overall scoring for description and explanation, while the combined group of students and PiTs showed more instances where areas of interest were neither described nor explained, indicating a gap in their observational and interpretive skills. However, inferential statistics confirmed significant differences at the level of individual ratings for description and explanation for only some areas: therapeutic competence (V1), therapeutic relationship (V2), clarity of communication (V2, marginal in V1), with supervisors outperforming the other group. Regarding the prediction component, supervisors showed a descriptive trend toward better predictive reasoning overall. Significant inferential differences in prediction were found in V1 for predicting how the therapist would manage both her own emotions and her patient's emotions. Additionally, marginal differences emerged for the prediction of the therapeutic relationship and the clarity of communication, again in V1. In all cases supervisors outperformed students and PiTs. Overall, these results suggest differences in the components of knowledge-based reasoning between supervisors and the group of less experienced students and PiTs, with a consistent advantage of supervisors. However, this is not the case for all of the areas of interest examined in this study, and effect sizes were small to medium for description and explanation and small for prediction. Accordingly, the findings should be interpreted with caution and regarded as tentative rather than conclusive. Notably, no spontaneous predictions were made across any of the groups. This may reflect a difference in task interpretation rather than a lack of predictive ability as the task instructions emphasized perception of the video clip rather than the anticipation of future events. Under different conditions, larger effect sizes or clearer group differences in the prediction domain might have emerged.
Our findings are consistent with the knowledge encapsulation model by Boshuizen and Schmidt (1992), which suggests that experts integrate theoretical and practical knowledge into intuitive schemas that allow for faster, more efficient processing of complex information. Novices, by contrast, rely more on explicit theoretical reasoning, making their observations slower and less sophisticated. This model helps to explain why supervisors in this study demonstrated a more advanced level of reasoning than students and PiTs, possibly because the latter relied primarily on theoretical knowledge. Furthermore, our results align with the stage model of therapist development (Sharpless & Barber, 2009), which describe how the perception and processing of therapeutic situations become more intuitive and integrated with increasing experience. From this perspective, PV may reflect this developmental progression and help to explain the observed group differences.
Third, we were interested in analyzing possible group differences in the quantitative ratings of psychotherapeutic processes. We found significant differences only for the rating of negative affect of the patient and for the treatment difficulty in V2, indicating that students and PiTs perceived the patients’ negative affect and the treatment difficulty as higher than supervisors. This may reflect supervisors’ greater treatment experience, which could reduce their perception of difficulty and negative affect in challenging situations. The lack of further significant differences suggests that the different groups rated the processes similarly overall. This could mean that the different groups of training share a basic understanding of observable therapeutic processes. In contrast, the qualitative analyses, which targeted professional vision (RQ1), revealed clearer group differences. This suggests that open-ended tasks may be more sensitive to capturing expertise-related differences in perception and reasoning than standardized rating formats.
Limitations and Future Research Directions
The generalizability of the findings is limited by the selection of the specific video sequences and by the focus on trauma therapy. Future research could include video clips from different therapeutic contexts, such as depression treatment, to increase the generalizability. Also, the video quality was reduced because the therapist and the patient wore masks, potentially making it more difficult to identify relevant processes. Although this affected all groups, it may have biased the results. Moreover, as we merged students and PiTs into one group in this study, future studies should investigate possible differences in greater detail to better understand them and to promote the competence development in a targeted manner. A qualitative content analysis of the study's transcripts could be a useful addition, as well as longitudinal studies and the use of eye-tracking techniques.
Also, verbal data alone may not fully reflect how knowledge is applied in practice (Gegenfurtner et al., 2020), especially in complex contexts such as psychotherapy. Furthermore, we did not have clear anchor points for determining what constitutes a “good” response, as no prior expert study was conducted. While we identified whether certain aspects of therapy were mentioned, we assessed quality only for prediction, not for describing and explaining, due to the study's exploratory nature, the relatively large sample for qualitative data analysis, and the range of variables collected. Consequently, potential quality differences at a more detailed content level could not be identified. Future research could benefit from a pilot phase involving expert raters to define benchmark responses for high-quality reasoning. This would support a more standardized assessment of verbal data and allow for more granular analysis within specific competence domains. Additionally, we did not apply a Bonferroni correction for multiple testing, as we aimed to reduce the risk of type II errors in this exploratry design. Hovever, this decision potentially increases the risk of type I errors. Therefore, results must be interpreted with caution, and effect sizes should be considered to evaluate their practical significance Future studies could address this by applying corrections or focusing on fewer variables. Additionally, no spontaneous predictions were made, possible due to task instructions. Refining the task framing could help to elicit more explicit predictive reasoning. Examining whether participants suggest improvements (Kersting et al., 2010) or alternative actions (Gold et al., 2016) could also be promising.
Implications for University Teaching
The results of this exploratory study provide preliminary evidence that the concept of PV can be applied to psychotherapy training. Based on our findings and instructional approaches established in teacher education, we suggest teaching strategies for university educators to promote PV in psychology students. In that field, video-based formats combining structured observation, guided reflection, and group discussion have been shown to foster key components of PV (e.g., Blomberg et al., 2013; Bonaiuti et al., 2020; Scholten & Orschulik 2022).Video-based case studies may similarly help psychology students practice key components of PV, such as describing observed therapeutic processes, identifying relevant indicators (e.g., signs of a good therapeutic relationship), and evaluating potential barriers to or outcomes of therapy. Faculty could design structured assignments with prompts or scaffolding tools to systematically guide students through these steps. Additionally, students could use the components of PV to provide feedback to one another during therapeutic role-play exercises. Collaborative formats, such as supervised analysis of therapy videos, could further enhance learning by providing opportunities for students to observe advanced thinking modeled by experienced supervisors and to receive targeted feedback. To further explore and refine these approaches, universities could develop and test pilot teaching formats specifically designed to promote PV. These programs could incorporate the teaching practices described here. Systematic evaluation of such courses is critical to assess their impact on students’ development of PV and to identify areas for improvement so that university teacehrs can better prepare students for the complexities of clinical practice and bridge the gap between theoretical knowledge and applied psychotherapeutic competencies.
Supplemental Material
sj-docx-1-plj-10.1177_14757257251372807 - Supplemental material for Professional Vision in Psychotherapy: An Exploratory Study
Supplemental material, sj-docx-1-plj-10.1177_14757257251372807 for Professional Vision in Psychotherapy: An Exploratory Study by Nicola Alina Maier, Meike Müller-Engelmann and Miriam Hansen in Psychology Learning & Teaching
Supplemental Material
sj-docx-2-plj-10.1177_14757257251372807 - Supplemental material for Professional Vision in Psychotherapy: An Exploratory Study
Supplemental material, sj-docx-2-plj-10.1177_14757257251372807 for Professional Vision in Psychotherapy: An Exploratory Study by Nicola Alina Maier, Meike Müller-Engelmann and Miriam Hansen in Psychology Learning & Teaching
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
The ethics application was approved by the Ethics Committee of Faculty 5 (Psychology and Sports Science) of the Goethe University Frankfurt (processing number: 2021-37). The patients and therapists in the videos signed a consent form to allow the videos to be shown to the subjects as part of the study. The subjects signed a consent form and agreed to keep information about the content and people in the therapy videos confidential and not to disclose it to third parties.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.