
Abstract
A number of initiatives are aimed at reducing mental illness stigma, yet stigma remains a problem in the general population. A focus on stigma reduction with students is particularly relevant, as students often hold negative attitudes toward mental illness, have regular contact with persons experiencing mental health difficulties, and because stigma influences students’ own help-seeking attitudes and behaviors. The psychology classroom presents an ideal opportunity to address stigma, since many courses include mental health-related topics and are taken by large numbers of students from diverse fields. This paper undertook a review of the published literature to determine the extent that knowledge and/or contact-based strategies to address stigma were implemented in the psychology classroom; successful interventions are described and contextualized within the larger stigma reduction literature. Recommendations for instructors who are interested in integrating an anti-stigma approach in their classroom include (1) consider a social contact-based approach, (2) look locally for resources, (3) be familiar with optimal conditions for contact, and (4) evaluate your outcomes.
Mental illness stigma is often conceptualized as negative thoughts, emotions, and behaviors directed at and experienced by people with a mental illness (Corrigan, 2000; Corrigan & Lee, 2013; Link & Phelan, 2001). There is a wealth of scholarly literature demonstrating the negative stereotypes and inaccurate beliefs society holds regarding people with mental illness. The most pervasive belief is that people with mental illness are dangerous or violent; other common beliefs include the following: they are to blame for their illness, have a poor prognosis, and are unproductive and unpredictable (Angermeyer & Dietrich, 2006; Boysen & Vogel, 2008; Corrigan, Markowitz, Watson, Rowan, & Kubiak, 2003). Negative emotional reactions (prejudice) are also common and are typically that of anger, fear, irritation, anxiety, and uneasiness (Corrigan et al., 2003; Link, Yang, Phelan, & Collins, 2004). Discrimination generally consists of social distancing, such as withholding help or opportunities, coercive treatment, and avoidance of contact (Corrigan et al., 2003; Corrigan & Shapiro, 2010).
The psychology classroom is a particularly relevant setting for stigma reduction, not because psychology students stigmatize more or less than the general population, but because mental health topics are salient to most psychology course curricula and there is an opportunity to reach large numbers of students from diverse disciplines and programs. Stigma reduction is relevant for the college/university student as students report levels of stigma that are similar to those reported by the general population, students frequently interact with persons with a mental illness, and because stigma reduction also improves help-seeking for one’s own mental health difficulties. The purpose of this article is to describe two evidence-based strategies for stigma reduction (knowledge and contact), examine the research that has used these approaches in the classroom, and provide recommendations for psychology instructors who wish to implement an anti-stigma approach in their teaching.
Why Focus on Mental Illness Stigma?
Thornicroft (2006) has suggested that people with mental illness may be the last minority group against whom it is socially acceptable to stigmatize, discriminate, and exclude. There is a large body of literature demonstrating stigma’s negative outcomes, including lowered self-esteem and quality of life, loss of opportunity across major life domains, and direct interference with treatment-seeking and adherence (e.g., Corrigan, 2000, 2004; Corrigan, Druss, & Perlick, 2014; Corrigan, Watson, & Barr, 2006; Wahl, 1999). Due to stigma’s significant impacts, a number of national and international initiatives are aimed at reducing mental illness stigma. Readers are likely to be aware of a national campaign against mental illness stigma in their home country, such as Opening Minds (Canada; www.mentalhealthcommission.ca), Stigmabusters (USA; www.nami.org), Time to Change (United Kingdom; www.time-to-change.org.uk), See Me (Scotland; www.seemescotland.org), Say No To Stigma (Australia; www.sane.org), and Like Minds, Like Mine (New Zealand; www.likeminds.org.nz). Other campaigns focus on reducing stigma associated with a particular disorder, such as schizophrenia (e.g., the World Psychiatric Association’s Open the Doors initiative; www.openthedoors.com). Regional and local initiatives tend to focus on specific target groups, such as elementary, secondary school, and college/university students (e.g., Bulanda, Bruhn, Byro-Johnson, & Zentmyer, 2014; Kendra, Cattaneo, & Mohr, 2012; O’Mara et al., 2014; Pitre, Stewart, Adams, Bedard, & Landry, 2007).
Similar to the general population, college and university students are known to hold negative attitudes about mental illness (e.g., Kendra et al., 2012). This stigma exists despite the fact that students have frequent exposure to persons with mental illness either through their own personal experience of mental health difficulties, a family member/friend/coworker, or through depictions of persons with a mental illness in the media. Mental health difficulties are as common amongst college/university students as their same-age (non-student) peers (Blanco et al., 2008) and some research suggests that they are increasing in number and severity (Hunt & Eisenberg, 2010). The first onset of mental health difficulties often occurs during early adulthood, a time when many people are pursuing higher education and other training opportunities (Mcgivern, Pellerita, & Mowbray, 2003). For example, a nationally representative sample of US college/university students found that approximately half of students had experienced a diagnosable mental disorder in the prior 12 months (Blanco et al., 2008). Mood and anxiety disorders, alcohol use, disordered eating, and personality disorders are most common amongst students (Blanco et al., 2008; Zivin, Eisenberg, Gollust. & Golberstein, 2009). These numbers increase when the broader concept of “psychological distress” is measured; estimates of psychological distress ranged from 30% in a sample of Canadian undergraduate students (n = 7800; Adlaf, Gliksman, Demers, & Newton-Taylor, 2001) to 83.9% in an Australian sample (n = 6,479; Stallman, 2010). A significant number of college/university students therefore have personal experience with a mental health difficulty and/or psychological distress.
Beyond the possibility of personal experience with a mental health difficulty, students are also likely to know or interact with persons with mental illness. For example, 96.4% of abnormal psychology students (n = 56) at a small American university reported knowing at least one person with a psychiatric disorder; the average number of relationships with a person with a psychiatric disorder was 5.09 (SD = 2.53; Connor-Greene, 2001). In a different sample of American community college students, 35% had a family friend with a mental illness, 28% had a relative with a mental illness, and 24% worked with a person with mental illness (Corrigan, Green, Lundin, Kubiak, & Penn, 2001). Exposure to mental illness is, of course, most common through film and media; 95% of this sample had been exposed to film depictions of mental illness and 68% had been exposed to more objective documentaries about mental illness (Corrigan et al., 2001). Students are therefore familiar with media depictions of mental illness (at the very least), and inaccurate and negative media and entertainment portrayals of persons with mental illness are linked to the development and perpetuation of public stigma (Arboleda-Flórez & Stuart, 2012; Canadian Mental Health Association, 2011). This student exposure to mental illness – either through personal experience of a mental health difficulty, interaction with someone with a mental illness, and/or media exposure – makes stigma reduction a relevant topic due to the negative personal and societal consequences previously described, as well as stigma’s consequences for help-seeking.
Stigma influences attitudes toward treatment and help-seeking behavior; stigma reduction may therefore lead to increased treatment-seeking amongst students, a group who typically under-utilize mental health supports. Despite the prevalence of mental health difficulties, on average less than one third of students who experience mental health difficulties seek treatment (Blanco et al., 2008; Gallagher & Taylor-Webmaster, 2014; Stallman, 2010), and overall young adults are less likely to seek mental health services compared to other adults (Kessler et al., 2001). These findings are of concern, as lack of appropriate treatment may have lasting implications, particularly for the first onset of a mental health difficulty (Eisenberg, Downs, Golberstein, & Zivin, 2009). Stigma is strongly connected to students’ help-seeking attitudes and intent (Bathje & Pryor, 2011; Martin, 2010); self-stigma (also referred to as internalized stigma and personal stigma) in particular has a negative association with help-seeking (Eisenberg et al., 2009; Lannin, Vogel, Brenner, & Tucker, 2015; Tucker et al., 2013). Addressing mental illness stigma may therefore positively impact on student help-seeking.
For the reasons just described, stigma reduction is an important and relevant topic for the general university/college student. This realization has led to the development of national and local anti-stigma initiatives aimed at college and university students. Active Minds, for example, is a well-known mental health advocacy organization with more than 400 university chapters across North America; its focus is on peer-led suicide and mental health awareness amongst students (www.activeminds.org). Colleges/universities often have additional local, grass-roots anti-stigma initiatives led by the campus health centre, student services, student union, and/or special interest groups.
The psychology classroom provides another context in which to challenge mental illness stigma. Mental health topics are relevant to most psychology course curricula: mental health and psychopathology are topics included in many psychology courses (e.g., introductory psychology, abnormal psychology, health psychology, developmental psychology) and, thus, a focus on stigma is a natural fit with these course components. Introductory psychology, in particular, is taken by large numbers of students from all fields and disciplines, providing a broad and captive audience for an anti-stigma intervention (Mann & Himelein, 2008). Due to the potential to reach large numbers of people with a non-intrusive stigma intervention, “teaching psychopathology without concern for stigma is a missed opportunity we cannot afford” (Mann & Himelein, 2008, p. 549).
There is, however, evidence to suggest that traditional psychology teaching methods may actually serve to increase stigma. Traditional teaching of psychopathology emphasizes memorization and intellectual learning through methods such as didactic lectures, textbook readings, and clinical accounts of mental illness (Kendra et al., 2012). Although textbooks often include case descriptions and examples, most case examples are written from a detached and/or professional perspective, lacking personal viewpoints and information about the impact of mental illness on the person, his/her family, and the community (Banyard, 2000). Furthermore, the teaching of psychopathology (as in introductory and abnormal psychology) often focuses on symptoms, diagnoses, and the medical model, which tend to encourage labeling and categorization (Mann & Himelein, 2008). In fact, there is a growing literature to examine the impact of biomedical explanations of mental illness on stigma (e.g., describing mental illness as a “brain disease” that is treated by medication), finding that such approaches at the very least are ineffective and at worst serve to increase stigma (e.g., Angermeyer, Holzinger, Carta, & Schomerus, 2011; Read, Haslam, Sayce, & Davies, 2006; Walker & Read, 2002).
In the wider literature examining attitude change, two evidence-based anti-stigma strategies have emerged: knowledge and contact. Knowledge-based strategies (also referred to as education-based strategies) are founded on the premise that increased knowledge about mental illness leads to decreased stigma; such strategies seek to provide accurate information about mental illness and address myths and misperceptions (Corrigan, River, et al., 2001; Mann & Himelein, 2008). Contact-based strategies involve interactions with a person with lived experience (PLE; Corrigan, River, et al., 2001). Research comparing both approaches has consistently shown that contact results in greater stigma reduction; it is associated with larger effect sizes and longer maintenance of gains compared to knowledge-based interventions (Corrigan, Morris, Michaels, Rafacz, & Rüsch, 2012; Corrigan, River, et al., 2001; Pinfold, Thornicroft, Huxley, & Farmer, 2005).
Review of Classroom Strategies for Addressing Mental Illness Stigma
The goal of this review was to determine the extent that knowledge and/or contact-based strategies to address stigma have been implemented in the psychology classroom, and to describe the strategies used. A second goal was to contextualize these interventions within the larger anti-stigma literature.
Inclusion Criteria
Published peer-review literature was included in the review. The types of articles included consisted of classroom-based (teaching/course-based) interventions and teaching strategies targeting mental illness stigma and attitudes (either generally, or for a particular disorder or set of disorders) for college/university students. Although there is a larger literature examining anti-stigma interventions amongst college/university students, with many studies utilizing psychology students for participants, the focus of this review is on classroom implementations. Thus, studies using non-classroom-based interventions/strategies were excluded from this review (for a recent systematic review and critical appraisal of this related literature, see Yamaguchi et al., 2013). Also excluded were studies that utilized a group/classroom format but not as part of a course.
Search Strategy
PsychINFO (2000–2016, English language) was searched in May 2015 and updated in July 2016, using the keywords (stigma* OR attitude) AND (mental OR schizophreni* OR psychiatri*) AND (college* OR universit*) AND (student*) AND (educat* OR train* OR program* OR interven*) AND (class*) AND (psychol*) NOT (school*) Hand searches (2000–2016) of the journals Psychology Learning and Teaching and Teaching of Psychology were conducted, along with checking of reference lists from relevant reviews (Holzinger, Dietrich, Heitmann, & Angermeyer, 2008; Yamaguchi et al., 2013) and reference lists of included articles.
Selection Process
A total of 140 abstracts were generated with the search terms. An additional 16 abstracts were identified through hand searches and checking reference lists. After examining titles and abstracts against the inclusion criteria, a total of 27 abstracts were retained; any abstracts that offered a potential match to the criteria were retained at this stage. Complete articles of all 27 abstracts were then obtained to fully assess whether they met inclusion criteria. At the conclusion of this process, seven articles met the inclusion criteria and were subject to inclusion in this review.
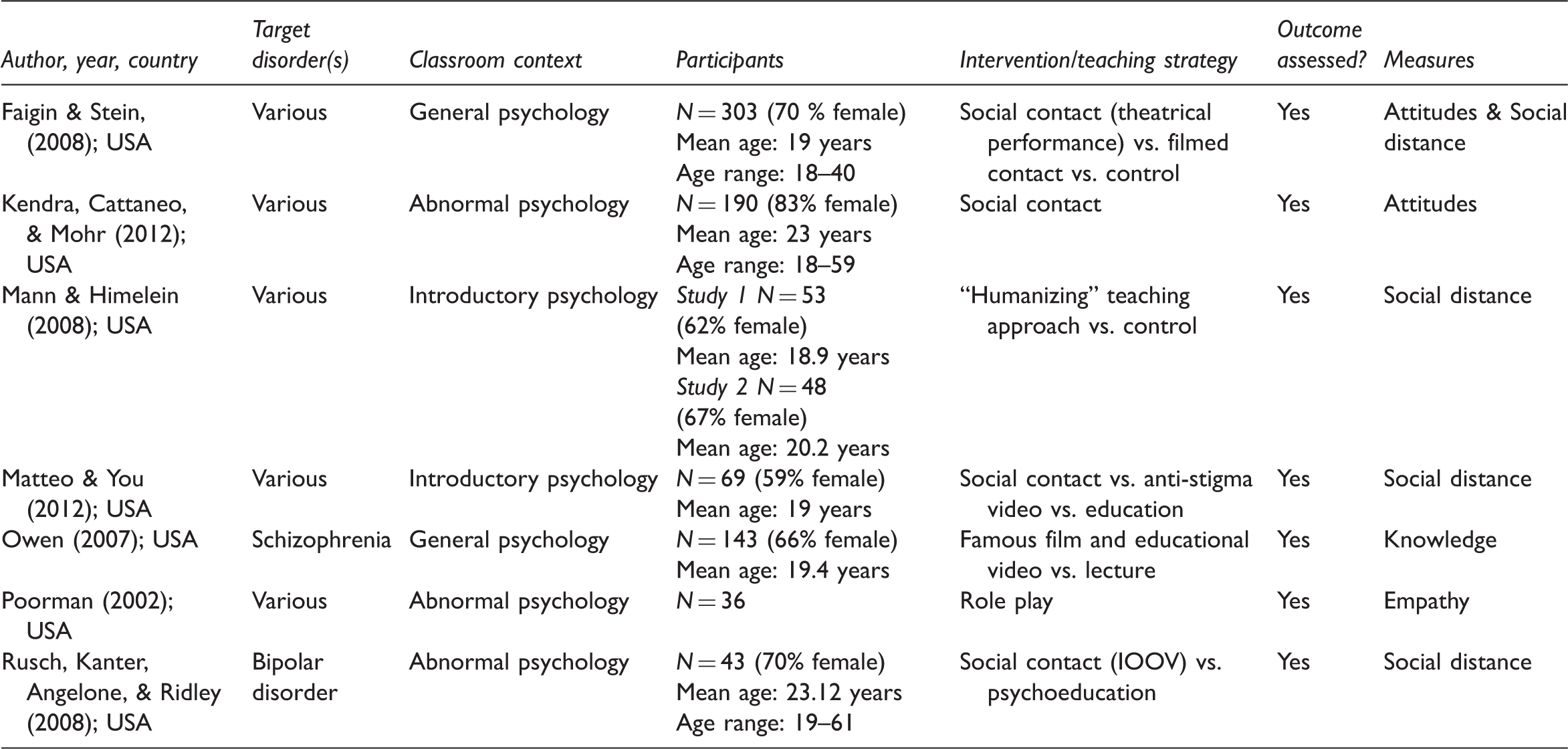
A data extraction form was used to record details about the country of origin, target disorder(s), classroom context, intervention/teaching strategy, participants, whether outcomes were assessed, and type of measure(s) used. Although a critical appraisal of published research studies is beyond the scope of this article, relevant study characteristics (e.g., sample size, outcome measures) were extracted and described when relevant.
Description of Included Articles
Characteristics of included studies.
Social Contact in the Classroom
The definition of social contact used in this review was any live interaction between people with mental health problem(s) and students in a classroom context. For example, Rusch and colleagues (2008) used a variation of the National Alliance on Mental Illness’s (NAMI’s) In Our Own Voice (IOOV) presentation in an abnormal psychology course. Two trained NAMI presenters, both with bipolar disorder, spoke for approximately 25 minutes each to one course section, describing his/her childhood, depressive and manic episodes, hospitalizations, interpersonal experiences, and successes with employment, volunteer work, and advocacy. A different abnormal psychology section served as a comparison group, and received a typical lecture about bipolar disorder. Participants in the IOOV section reported decreased social distance compared to the comparison group (Rusch et al., 2008).
Other educators, however, have developed their own contact-based interventions. For example, students in an introductory psychology course generated questions they would ask a person with lived experience of mental illness (PLE), and in a subsequent 90-minute class met three community-dwelling PLEs. Each PLE provided some brief context about themself and then met with small groups of students for 15 minutes to interact and answer questions. Students in this condition showed a decreased desire for social distance compared to students in education-only and video-only conditions (Matteo & You, 2012). Faigin and Stein (2008) utilized a theatrical performance to decrease stigma amongst students in a general psychology course. A live performance by non-professional actors with a history of severe mental illness depicted a fictional mutual support group session (themes included the impact of stigma on the group members, social and treatment challenges of living with a serious mental illness, and the possibility of recovery). The 70-minute performance took place during a regularly scheduled class, and a previously recorded video of the play was shown to a different section for comparison purposes. Compared to a third section of students who did not receive any intervention, students in the live and filmed play conditions reported greater willingness to engage in future contact with a person with a mental illness and improved attitudes toward people with a mental illness (Faigin & Stein, 2008).
The final article that utilized social contact had students in two sections of an abnormal psychology course engage in 15-minute unscripted student presentations about personal or family member difficulties with a mental illness (e.g., schizophrenia, eating disorders, depression, alcohol dependence); these presentations were scheduled throughout the course to correspond with the lecture topics (Kendra et al., 2012). There were no differences in attitudes about mental illness between these sections and three other abnormal psychology sections who did not receive this form of social contact.
The finding that three out of these four articles reported improved attitudes and reduced social distance fits within the larger stigma literature, which asserts that social contact is a more powerful change agent compared to knowledge/education alone (Corrigan, River, et al., 2001; Corrigan et al., 2012; Pinfold et al., 2005). In fact, a systematic review of anti-stigma interventions tested using college and university students confirmed that contact-based approaches are most effective (Yamaguchi et al., 2013). There are several reasons described by Kendra and colleagues (2012) as to why their social contact intervention did not influence attitudes as expected, focusing in large part on the use of unscripted student presentations. While unscripted presentations have the benefit of providing an authentic first-person perspective, they may not incorporate the types of information that are typically associated with attitude change (e.g., Corrigan & Penn, 1999). The fact that not all forms of social contact are equally effective is evident in the literature examining health professionals’ attitudes about mental illness: although this group holds much knowledge about mental illness and has a significant amount of contact with persons with lived experience, medical and mental health professionals endorse stigma at rates equal to or greater than the general public (Lauber, Nordt, Braunschweig, & Rössler, 2006; Nordt, Rössler, & Lauber, 2006; Ross & Goldner, 2009; Thornicroft, 2006).
Educators wishing to use a social contact approach in their classroom should therefore be familiar with the conditions under which social contact reduces stigma. Contact-based strategies are centered on the premise that such interaction can reduce prejudice toward that group (the contact hypothesis, Allport, 1954; Pettigrew, 1998); contact theory specifies that attitude change will occur when four key conditions are present: equal group status, common goals, intergroup cooperation, and authority support (most studies, however, find positive effects of contact even if these conditions are not met; Pettigrew, 1998). Additional conditions for optimal contact include positive expectations, appreciation of similarities and differences, and the perception that the person with mental illness is typical of the group (in other words, the person mildly or moderately conforms to the stereotype; Corrigan & Penn, 1999).
Video-Based Social Contact in the Classroom
Video-based social contact was defined as classroom use of videos depicting people with mental health problems talking about their personal experiences (consistent with the definition provided by Yamaguchi et al., 2013). One included study used video-based social contact as the primary intervention (Owen, 2007) and one other study used this approach for a comparison group (Faigin & Stein, 2008). Owen (2007) constructed a 36-minute video illustrating eight myths and corresponding (correcting) facts about schizophrenia. The “myth” video clips were taken from famous films, while the “fact” video clips were taken from documentaries and/or training videos. Students who viewed the video as well as students in a comparison group (traditional lecture) demonstrated increased knowledge about schizophrenia; in other words the video did not result in greater change versus the traditional lecture (Owen, 2007). In contrast, Faigin and Stein (2008; who utilized the previously described live theatrical performance) found that students in a film condition experienced the same improvement in attitudes and social distance as students in the live social contact condition; change in both groups was significant beyond a no-intervention group.
To help contextualize these findings, there is a small experimental literature that has compared live social contact with video-based social contact. A recent meta-analysis found that both live and video-based social contact had a significant effect on stigma, but live social contact was associated with a greater overall impact and attitude change (Corrigan et al., 2012). One challenge related to this area of research, and thus the conclusiveness of any findings, is that there is great diversity in videos used in the classroom. Video-based social contact can take many forms including (but not limited to) first-person narratives, documentaries, media reports, and feature films. It is in fact quite popular to use feature films to demonstrate course concepts (Green, 2011), and numerous websites and text book supplements provide reviews of popular films that can be used as demonstrations. However, the stigma-related impact of these films is rarely evaluated in the classroom context and educators should keep in mind that the entertainment industry is frequently identified as having a negative influence on mental health-related attitudes and opinions (Canadian Mental Health Association, 2011). Filmed contact is, however, appealing to educators due to its low cost, ease of access, and dissemination potential (for example, it can be used in a face-to-face course as well as in online teaching).
Experiential Teaching Methods
The final two articles that were included in this review had interventions that focused on teaching pedagogy (Mann & Himelein, 2008) and role play in the classroom (Poorman, 2002). Mann and Himelein (2008) empirically evaluated outcomes associated with these approaches by assigning two introductory psychology classes to receive either traditional teaching methods (a focus on symptoms and diagnosis, case examples written from a clinician perspective, viewing of a third-person perspective video, and a diagnostic writing assignment) or humanizing teaching methods (inclusion of first-person narratives, a video depicting first-hand perspectives, and a writing assignment designed to foster empathy) for a two-week abnormal psychology module. Students who were exposed to the traditional teaching method held unchanged attitudes, while students who were exposed to the humanizing approach demonstrated a reduction in stigma. These findings were independently replicated in two subsequent introductory psychology classes (Mann & Himelein, 2008). Poorman (2002) had students in an abnormal psychology course write a fictional biography of a person with a mental illness; students were then asked to role play their character in one of three settings, while the other students in the class interacted with the character and “assessed” and “diagnosed” the character. Empathy scores following the exercises indicated a decrease in emotional distance between students and people with a mental illness (Poorman, 2002).
Experiential teaching methods such as these are often used in the classroom in an effort to reduce stigma. These approaches emphasize experiential learning and attempt to increase the personal relevance of course material through methods such as reading first-person accounts of mental illness, fostering empathy, and engaging students in meaningful discussion. Experiential approaches are also capable of addressing several factors associated with stigma reduction. Corrigan and Penn (1999) described four important factors associated with stigma reduction in knowledge-based programs, namely personal information about the patient, addressing myths directly, increasing empathy, and including an opportunity for discussion. Although not included in this review (because the focus was not on reducing mental illness stigma), Banyard (2000) and Norcross, Sommer, and Clifford (2001) provided many examples of how first-person perspectives can be integrated into abnormal psychology courses.
Simulation is another experiential learning approach that has been used with the goal of increasing students’ perspective of the experience of mental illness and fostering empathy. A common in-class paradigm is to simulate auditory and visual hallucinations as may be experienced during psychosis (e.g., through an audio recording and/or video). Although this review did not include any such articles (none met the classroom-based inclusion criterion), this simulation exercise is mentioned here as it is a popular in-class demonstration. Viewed from a stigma reduction lens there is dubious evidence to support this approach. A systematic review examining 10 studies found that simulated hallucinations consistently increase desire for social distance from people with schizophrenia (Ando, Clement, Barley, & Thornicroft, 2011). This learning approach is thus not recommended.
Discussion
This paper has sought to determine the extent that knowledge and/or contact-based strategies to reduce mental illness stigma are implemented in the psychology classroom, and to contextualize these strategies within the larger anti-stigma literature. Seven such articles were identified, with four focused on a social contact approach, one focused on video-based social contact, and two focused on experiential teaching methods. All anti-stigma approaches took place in general/introductory or abnormal psychology courses. The studies included in this review fit within the larger anti-stigma literature, which supports the use of knowledge and contact in reducing mental illness stigma.
The following recommendations, based on this review and the larger stigma reduction literature, are offered for instructors who wish to incorporate an anti-stigma approach in the psychology classroom.
Consider using a social contact-based approach. Three of the four included articles that focused on a “live” social contact-based approach reported statistically significant improvement in students’ attitudes, social distance, knowledge, and/or empathy following the intervention. Laboratory and community-based research with college/university students and members of the general population consistently show greater improvement in attitudes and reduced social distance for interventions that use live interaction between participants and persons with a mental illness compared to knowledge-based interventions (Corrigan, River et al., 2001; Corrigan et al., 2012; Pinfold et al., 2005). Video-based social contact can also be a useful strategy, and has the added benefits of relative ease of access and dissemination. Look locally for resources. Although all of the articles included in this review described a unique anti-stigma intervention/approach developed or modified by the authors (even the NAMI IOOV presentation was modified for the classroom setting; Rusch et al., 2008), instructors are likely to find excellent established resources that they can integrate into their classroom. The Mental Health Commission of Canada has a large list of evaluated stigma interventions on its website (www.mentalhealthcommission.ca), many targeting college/university students. National anti-stigma initiatives and mental health advocacy organizations often have anti-stigma resources freely available for use. For example, a local branch of the Canadian Mental Health Association has a grass-roots developed anti-stigma presentation, consisting of live social contact, video-based social contact, and knowledge/education, which has been integrated into the author’s abnormal psychology course. Another good example is the NAMI IOOV program, which consists of a 90-minute presentation by two trained speakers (persons with lived experience) and a video depicting first-hand experiences with mental illness. The speakers share their personal story of recovery with the audience and focus on themes of recovery and hope (Brennan & McGrew, 2013). IOOV has been shown to reduce stigma in undergraduate students (Corrigan et al., 2010; Rusch et al., 2008; Wood & Wahl, 2006) and is widely available in the USA through NAMI. Be familiar with optimal conditions for reducing stigma. If instructors choose to create their own anti-stigma intervention, it is recommended that they first familiarize themselves with intervention factors that enhance outcomes. A large meta-analysis found strong support for contact-based strategies, but studies demonstrated larger effect sizes when more optimal conditions for contact were met (Pettigrew & Tropp, 2006). Equal group status, common goals, intergroup cooperation, and authority support are important considerations for social contact-based strategies (Pettigrew, 1998). It is also recommended that instructors provide personal information about cases (consider using first-person narratives), address myths, foster empathy, and include discussion (Corrigan & Penn, 1999). Corrigan and Penn (1999) provide an excellent description of how factors such as equal status, cooperative interaction, and institutional support impact affect outcomes for contact-based interventions. Evaluate your outcomes. It is evident from this review that strategies to address stigma in the psychology classroom vary widely; evaluation of outcomes thus becomes very important, as a well-intentioned intervention does not necessarily lead to stigma reduction. Instructors would therefore do well to ensure their interventions are achieving the desired goals by evaluating outcomes. Social distance measures (including measures of intended behavior) and attitude-based measures were most commonly used by articles included in this review. They have the advantage of being relatively brief, adaptable to a specific mental illness or a more general concept, and there are a number that are empirically supported (for an excellent review of anti-stigma measures and concepts, see Link et al., 2004). Evaluation would also help inform the wider literature supporting knowledge and contact-based approaches to stigma reduction. This review only identified seven articles that have applied/examined these strategies in the university classroom – the vast majority of the research examining knowledge and contact-based strategies with students has used laboratory-based designs. Although this type of research is important to our understanding of the effects of an intervention and the relative contribution of each component, there is also a need to evaluate outcomes in vivo; that is, in the classroom.
The findings of this review should be considered with the following limitations in mind. Only one person (the author) conducted the literature search, article screening and selection, and data abstraction, which may have resulted in errors being made. Only one database (PsychINFO) was searched and articles were limited to the English language. Although hand searches of two journals with an international readership were conducted, only US-based articles/studies were identified in this review and the findings are therefore based on this culture and system of learning. There is a growing literature examining mental illness stigma in other countries and cultural groups, as well as cultural aspects of stigma (e.g., Abdullah & Brown, 2011; Ciftci, Jones, & Corrigan, 2013; Coker, 2005; Ng, 1997) and the recommendations stemming from this literature review may not be relevant to these contexts.
Conclusions
Overall, there is evidence that knowledge and contact-based strategies are effective anti-stigma approaches within the psychology classroom. Contact-based strategies are the most powerful and it is recommended that instructors examine ways to incorporate social contact into psychology courses. For some readers this article will affirm current teaching methods and strategies; for others this article may provoke further reflection about how they teach about mental illness and the need to consider stigma when doing so. Overall the psychology classroom can be viewed as another setting in which to reduce mental illness stigma.
Footnotes
Acknowledgement
This article is based on a paper presented at the 2015 Vancouver International Conference on the Teaching of Psychology, Vancouver, Canada.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.