
Abstract
Background
Psychology coursework may include opportunities to reduce mental illness stigma attitudes among college students. However, some strategies are known to backfire, and little is known about how these attitudes evolve during psychology coursework.
Objective
The purpose of this study was to examine whether psychology students’ mental illness stigma attitudes change over the course of a semester.
Method
This research examined changes in mental illness stigma across four undergraduate psychology courses: Introductory Psychology, Abnormal Psychology, Basic Helping Skills, and Internship. Students (N = 400) completed two mental illness stigma measures at the beginning and end of the semester.
Results
Regardless of course, students showed slightly decreased anxiety-related stigma regarding individuals with mental illness and lower social distancing attitudes toward individuals with schizophrenia, as well as increased perceptions of the treatability of mental illness, over the course of the semester.
Conclusion
The findings suggest limited stigma reduction through the psychology curriculum.
Teaching Implications
Greater emphasis on systematic efforts for stigma reduction across the psychology curriculum is warranted and instructors may want to consider developing gender-related stigma reduction methods.
Mental illness stigmatization is a problem internationally (Krendle & Pescosolido, 2020; Taskin et al., 2003), including in the United States (U.S.; Link et al., 1999). This stigma consists of negative attitudes and behaviors toward those with mental illness (Link & Phelan, 2001), such as perceptions that those with mental illness are dangerous, criminal, unintelligent, untreatable, at fault for their condition, unproductive, and/or lazy (e.g., Parcesepe & Cabassa, 2013). Stigma may manifest in interpersonal anxiety towards those with a mental illness (Day et al., 2007) and social distancing behaviors (e.g., Nordt et al., 2006), with those on the receiving end experiencing lowered self-esteem, quality of life, and discrimination (e.g., housing, employment; Corrigan et al., 2003), as well as a decreased propensity to seek help due to a fear of stigma (Downs & Eisenberg, 2012).
Unfortunately, mental health professionals, on average, endorse stereotypes toward individuals with mental illness at a level comparable to the public (Nordt et al., 2006) and client perceptions of this stigma may have particularly harmful impacts including exacerbation of mental illness–related problems (Mak et al., 2007). Stigma attitudes held by mental health professionals likely develop long before these individuals enter the field and have been documented in the literature among college students (e.g., Lipson et al., 2019).
Considering that one in five psychology majors will progress to a career in the human service field (United States Department of Labor, Bureau of Labor Statistics, 2017), endorsement of mental illness stigma is particularly concerning among this group. In fact, the American Psychological Association has indicated specific learning objectives for undergraduate psychology students regarding sensitivity to diverse groups (Goal 3; APA, 2013). Thus, it is critical that the psychology curriculum seeks to reduce mental illness stigma. Reduced stigma attitudes not only benefit future clinicians, but also prepare students to be socially aware citizens in their communities.
One might, therefore, wonder how much students change their mental illness stigma attitudes in psychology courses. Although researchers have examined specific pedagogical components (e.g., lectures, assignments, contact interventions and service learning; Barney et al., 2017; Kosyluk et al., 2016; LaCaille, et al., 2019; Matteo & You, 2012) and programs (Maslowski et al., 2019) designed to reduce stigma, psychology curriculum more broadly appears to have been neglected. Extant Abnormal Psychology studies with an “instruction-as-usual” condition have been discouraging, suggesting little change might be expected without targeted interventions (e.g., Ferrari, 2016; Strassle, 2018). However, outside of an experimental design, most psychology instructors might incorporate some degree of stigma-relevant instruction, therefore the question of the expected natural stigma change over time among psychology students remains.
One might, therefore, wonder how much students change their mental illness stigma when taking psychology courses. Although researchers have examined specific pedagogical components, including assignments (Barney et al., 2017; Kosyluk et al., 2016; LaCaille et al., 2019; Matteo & You, 2012) and programs (Maslowski et al., 2019) designed to reduce misconceptions and stigma, psychology curriculum more broadly appears to have been neglected. A few studies in Abnormal Psychology courses with an “instruction-as-usual” condition have been discouraging, suggesting little change might be expected without targeted interventions (e.g., Ferrari, 2016; Strassle, 2018). However, outside of an experimental design, psychology instructors might incorporate some degree of stigma-relevant instruction, so the question of the expected natural stigma reduction among psychology students remains.
Although Abnormal Psychology might naturally attend to the topic of stigma, stigma-reduction efforts are likely relevant to a variety of other psychology coursework. Psychology internships, for example, often offer opportunities to interact with individuals with mental illness. This interpersonal contact may reduce stigma attitudes (Yamaguchi et al., 2013), though experiences with someone who does not conform to stereotypes of individuals experiencing mental illness (e.g., they are perceived as non-dangerous, live independently) risks confirming or solidifying preexisting negative attitudes about mental illness, as these individuals may be perceived as non-representative or atypical of individuals with mental illness (i.e., the boomerang/backfire effect; Kundra & Oleson, 1997; Lewandowsky et al., 2012). A brief service-learning activity in an Abnormal Psychology course appeared to reduce implicit and self-reported biases (Barney et al., 2017; Strassle, 2018); however, no studies to date appear to have assessed stigma reduction over the course of completing an undergraduate psychology internship.
Additionally, undergraduate psychology students might change stigma attitudes while learning microcounseling skills. Stigma involves a kind of distancing in which students might view those with mental illness as “other” or different from themselves (Ottati et al., 2005), whereas empathy might be seen as the reverse. Indeed, empathy is linked with a decreased desire for social distance (Phelan & Basow, 2007). Furthermore, skill-based courses such as Basic Helping Skills involving role-play practice not only appear to improve empathic communication (Reich et al., 2021), but also students’ self-efficacy regarding communication skills (Hill et al., 2014; Jackson et al., 2014), which could also translate into stigma reduction. However, studies have yet to directly assess whether stigma reduces because of skills-based training courses.
The aim of this study was to test whether the null “instruction-as-usual condition” findings for mental illness stigma (e.g., Ferrari, 2016; Strassle, 2018) would replicate under naturalistic (non-experimental) conditions. Specifically, we examined psychology students’ mental illness stigma at the start and end of the semester and explored differences between stigma change in four courses: Introductory Psychology, Abnormal Psychology, Basic Helping Skills, and Internship.
Method
Participants
Between 2017 and 2019, 568 undergraduate students at a mid-sized public university in the midwestern United States participated. Students were excluded if they did not complete both surveys (n = 130) or were simultaneously enrolled in more than one of the courses in the study (n = 38). In the final sample (N = 400; 71% female), ages ranged from 18 to 62 (M = 22.10, SD = 7.27). Students were enrolled in: Introductory Psychology (n = 91), Abnormal Psychology (n = 121), Basic Helping Skills (n = 119), and Internship (n = 69). Introductory Psychology students were significantly younger (M = 18.44, SD = 1.00) than students in the other courses (Abnormal Psychology M = 26.68, SD = 11.52; Basic Helping Skills M = 20.87, SD = 2.03; Internship M = 20.97, SD = 2.65), F (3, 395) = 24.41, p < .001, η2 = .15.
Courses
Introductory Psychology
Introductory Psychology was open to all majors and provided a foundational introduction to the field of psychology, including a brief overview of mental disorders and therapy. One face-to-face section (n = 157) of this course was invited to participate. Misconceptions about mental illness were briefly mentioned in select lectures, such as overrepresentation of paranoid schizophrenia in the media and prevalence rates for mental disorders including lifetime depression.
Abnormal Psychology
The Abnormal Psychology course was an upper-division course which required Introductory Psychology as a prerequisite. The introduction to the study of abnormal behavior and psychopathology was based on the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013), including etiology and treatment. All five sections (ns = 28–31) were taught entirely online by the same instructor. Students viewed several videos of individuals discussing their mental illness, completed assignments regarding case studies (for diagnostic comparisons), and were taught about evidence-informed treatments. Additionally, students evaluated a popular film in terms of common misrepresentations (e.g., people with mental illnesses are violent, cannot recover). Another assignment involved reading refutational texts, developing a myth debunking poster, and critiquing others’ posters.
Basic Helping Skills
Basic Helping Skills was an upper-division psychology elective available to majors and non-majors. Students were trained in microcounseling skills, such as empathic listening, and were introduced to theories and research pertaining to behavior change and therapy. The course emphasized the practice of microcounseling skills in small groups. Students from six sections (ns = 16–30) were invited to participate, all taught by the same instructor.
Although students watched videos of therapy, mental health diagnosis was rarely discussed, as helping skills rather than client characteristics were the focus. However, students were assigned to read a short fact sheet provided by the National Alliance on Mental Illness (NAMI) dispelling common myths about mental illness (Powell, 2015). Help-seeking stigma was discussed, via a book chapter and one lecture, both as a barrier to treatment as well as an attitude which the helper must overcome within themselves to be effective. During lectures, the instructor deliberately shared a brief relevant observation from personal therapy experience to help destigmatize help-seeking. In all sections, at least one student made spontaneous and unsolicited disclosures of past personal histories in response. Students were also exposed to skills training relevant to “dangerous” mental health scenarios such as de-escalation and suicide prevention strategies.
Internship
The Internship course was an upper-division course for psychology majors in which students completed a minimum of 9 hours per week at a community placement. Students from eight sections (n = 10–14) led by four different instructors were invited to participate. The 69 students who volunteered for the study interned at the following types of sites: child/adolescent treatment programs (28.2%), family therapy and domestic violence shelters (12.7%), organizational psychology, human resources, or employment programs (12.7%), adult mental health and chemical dependency programs (11.3%), academic counseling services (9.9%), and after-school programs (1.4%). During a weekly 1-hour faculty-led group supervision, interns discussed their experiences. Students completed weekly reflection journals and a final paper and presentation about their field experiences. Exposure to mental illness was coded through a discussion by two primary faculties who rated placements as involving “exposure” or “minimal exposure.” Most students (n = 49, 71%) had some direct exposure to individuals with mental illness through their internship. In addition, students at other internship sites would have heard about their peers’ experiences during the weekly group supervision meeting, which sometimes emphasized the discussion of experiences that were challenging or unusual. Perspective-taking and discussions exploring systemic contributions to issues of violence, substance abuse, and mental illness were common. However, there were no assignments directly targeting mental illness stigma.
Measures
Mental Illness Stigma
The Mental Illness Stigma Scale (Day et al., 2007) is a 28-item questionnaire that includes seven subscales to assess attitudes toward people with mental illness. Items are rated on a scale from 1 (completely disagree) to 7 (completely agree). Higher scores on four subscales (interpersonal anxiety, relationship disruption, poor hygiene, visibility) indicate greater stigma, whereas higher scores on three subscales (treatability, professional efficacy, recovery) indicate less stigma (α = .71–.90).
Social Distancing
Participants read vignettes (adapted from Link et al., 1999) about two hypothetical individuals with a mental illness: depression and schizophrenia. Each vignette was followed by six questions about one’s willingness to socialize with the individual. Items were taken from a social distance scale developed by Chung et al. (2001) but adapted for use with college students (Mann & Himelein, 2004). Items were rated on a scale from 1 = definitely willing to 5 = definitely unwilling, with higher total scores reflecting a greater tendency to social distance (α = .81 for both vignettes).
Help-Seeking Stigma
Help-seeking stigma was not initially considered by the authors at the outset of data collection; however, as it was documented within the literature as a primary barrier to help-seeking (Downs & Eisenberg, 2012), it was added as a variable of interest later in the data collection phase. Data on help-seeking stigma, measured using the 10-item Self-Stigma of Seeking Help scale (Vogel et al., 2006), was collected from 40% of participants (n = 160): Introductory Psychology (n = 91); Abnormal Psychology (n = 21); Basic Helping Skills (n = 32); Internship (n = 16). Items were rated on a 5-point scale from 1 = strongly disagree to 5 = strongly agree, with higher total scores indicating greater stigma (α = .84).
Procedure
Students in courses taught by instructors who opted in during the study period completed a consent form. Instructors asked students to complete the online questionnaires within the first week of the semester (pretest) and within the final 2 weeks of the semester (post-test). An attention check question was passed by all participants. The assessments were considered part of the course expectations and were awarded a small number of points (approximately 2–3% of their course grade) for completion. Students could request an alternative assignment; however, none did so. The university’s Institutional Review Board approved the use of the de-identified dataset for this study.
Statistical Approach
Changes in stigma for each of the outcome measures (Mental Illness Stigma, Social Distancing, and Help-Seeking) were assessed via 4 (course) × 2 (time) mixed factorial ANOVAs. With this analysis, the interaction indicates whether patterns of attitude change over time varied depending on course. In the absence of a significant interaction, the main effect of change over time was interpreted. The effect size partial eta square (ηp2) is reported and can be interpreted as .01 = small effect, .06 = medium effect, and .14 = large effect (Cohen, 1988). The simple effects of significant interactions are reported as paired sample (pre-post) t-tests with Cohen’s d effect sizes, which can be interpreted as 0.2 = small effect, 0.5 = medium effect, and 0.8 = large effect.
Results
Descriptive and Two-Way ANOVA Statistics for Mental Illness Stigma.
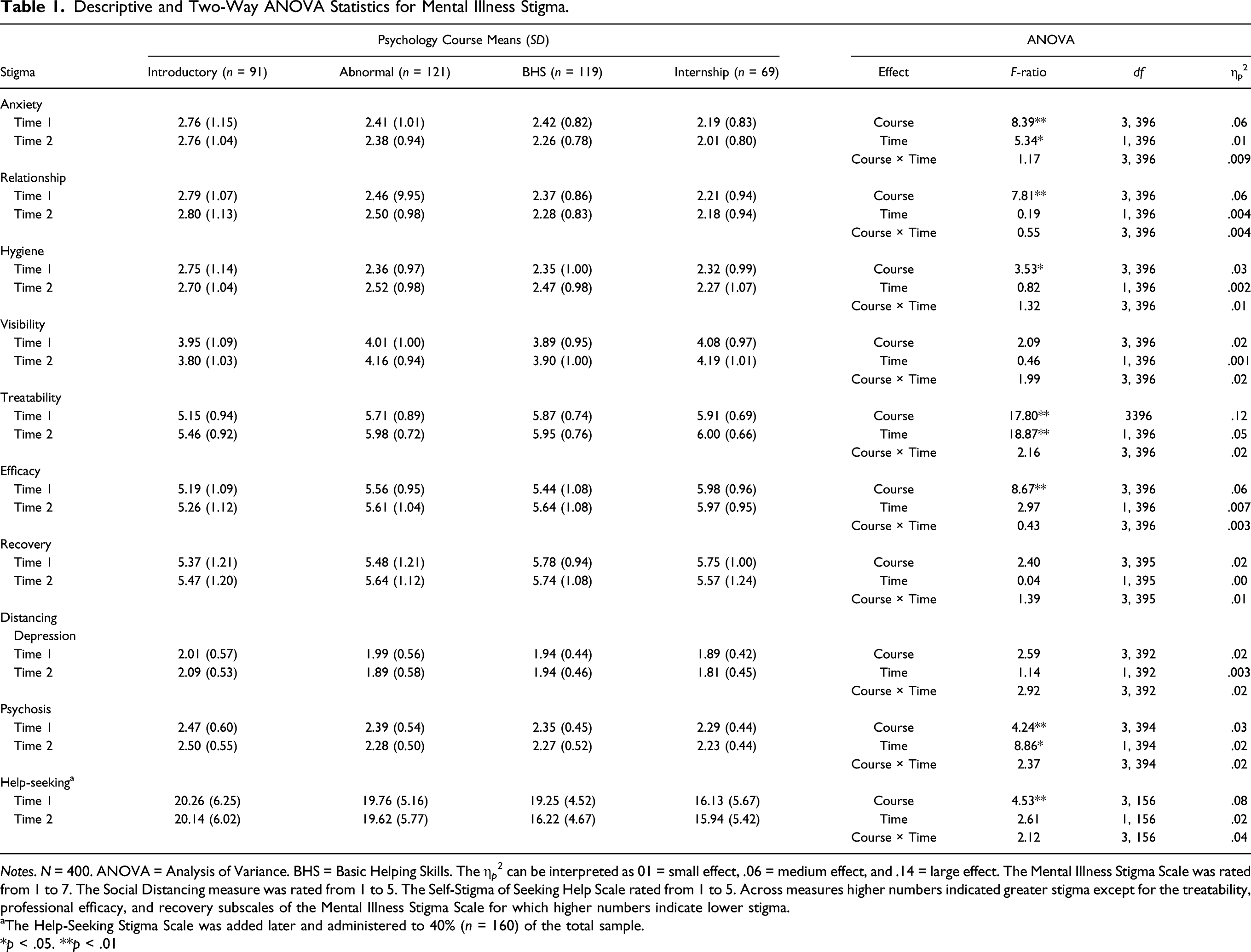
Notes. N = 400. ANOVA = Analysis of Variance. BHS = Basic Helping Skills. The η p 2 can be interpreted as 01 = small effect, .06 = medium effect, and .14 = large effect. The Mental Illness Stigma Scale was rated from 1 to 7. The Social Distancing measure was rated from 1 to 5. The Self-Stigma of Seeking Help Scale rated from 1 to 5. Across measures higher numbers indicated greater stigma except for the treatability, professional efficacy, and recovery subscales of the Mental Illness Stigma Scale for which higher numbers indicate lower stigma.
aThe Help-Seeking Stigma Scale was added later and administered to 40% (n = 160) of the total sample.
*p < .05. **p < .01
There were significant main effects for course types for anxiety, relationship, hygiene, treatability, professional efficacy, social distancing from schizophrenia, and help-seeking stigma. In all but one case, post hoc analyses revealed statistically significant differences such that the Introductory Psychology course had more stigmatized attitudes overall than the other three courses (all ps < .05). For helping-seeking stigma, Introductory Psychology students reported significantly more stigma than Basic Helping Skills and Internship students (ps < .05) but were not significantly greater than Abnormal Psychology students (p = .64). Notably, help-seeking stigma data was only available for a smaller subsample of the participants (n = 160). Internship students reported more professional efficacy for working with individuals with mental illness compared to the other courses (all ps < .05).
Mental Illness Exposure at Internship Sites
As indicated by a series of independent samples t-tests, only one of the stigma measures at the post-test differed significantly depending on amount of exposure to mental illness at the students’ internship sites. Students who had moderate-high mental illness contact viewed mental illness as significantly more treatable (M = 6.11, SD = 0.66) than students at no-low contact sites (M = 5.75, SD = 0.59), t (67) = 2.11, p = .04, a medium effect d = 0.57. Removing students at no-low contact internship sites from the primary analyses did not substantially alter the findings.
Discussion
In previous research examining mental illness stigma in Abnormal Psychology courses (e.g., Ferrari, 2016; Strassle, 2018), “instruction-as-usual” control conditions have suggested little change. The purpose of this study was to test whether the null “instruction-as-usual condition” findings would replicate under naturalistic conditions. Changes in mental illness stigma were examined from the start to the end of the semester among students enrolled in one of four psychology courses: Introductory Psychology, Abnormal Psychology, Basic Helping Skills, and Internship. Regardless of course type, findings revealed that at the end of the semester participants were slightly less anxious about interacting with someone with a mental illness, more willing to socially interact with someone with schizophrenia, and viewed mental illness as more treatable relative to their endorsements at the start of the semester. Altogether, these findings suggest some limited stigma reduction is achievable through a psychology curriculum. The results also generally fit with existing literature of other populations, which suggests that people who have a greater acquired knowledge of mental illness are less likely to report discrimination and stigmatizing beliefs and engage in social distancing behaviors (Dipaula et al., 2011; Maslowski et al., 2019). In addition, only a single statistical comparison (i.e., Introductory Psychology students’ social distancing for schizophrenia), out of all comparisons analyzed in this study, showed an increase in stigma attitudes. Otherwise, data did not suggest that exposure to mental illness course content or exposure to clinical populations was associated with increased stigma over time in these courses.
It is notable that unique patterns of change were not readily apparent for particular courses. Although students completing an internship reported greater professional efficacy of working with individuals with mental illnesses, their stigma reduction was like students in other classes. This finding contradicts contact theory that suggests personal contact approaches reduce negative attitudes and social distancing toward individuals with mental illnesses (Yamaguchi et al., 2013), but is consistent with the finding that mental health professionals endorse mental illness stereotypes too, despite frequent contact as a nature of their work (Nordt et al., 2006).
Notably, students in our program reported relatively low levels of mental illness stigma attitudes in general, even at the start of their college careers. Moreover, although mean baseline scores on the Mental Illness Stigma Scale appear generally in line with what has been collected in previous research (Day et al., 2007), mean baseline scores for social distancing and help-seeking were much lower than what has been documented in research that has employed the Social Distancing Scale (Mann & Himelein, 2004, 2008) and Self-Stigma of Seeking Help Scale (Ferrari, 2016). These findings might be explained by recent data collected in a large national sample of university students between 2007 and 2017 that suggests a decline in mental illness stigma among college students (Lipson et al., 2019).
Increases in rates of mental illness among college students (Duffy et al., 2019; Twenge et al., 2019) might suggest that students more frequently encounter peer and personal contact examples, which may naturally aid in stigma reduction. If so, it would call into question whether findings regarding the stigma among mental health professionals (e.g., Nordt et al., 2006) have undergone a generational shift or if such attitudes are established later during professional development. Ultimately however, there does not appear to be literature that indicates a generational shift in views has occurred for mental health professionals, although it has been documented in more recent research that stigma attitudes remain prominent among mental health professionals (Hansson et al., 2013).
Several limitations of the current study should be noted. Although previous researchers have observed stigma reduction with comparably low baseline scores (Day et al., 2007), it remains possible that low levels of student-reported stigma in general within this sample might have limited the opportunity for meaningful improvement to be observed. It would be beneficial for future research to investigate whether such statistically significant reductions in student stigma levels over time show practically meaningful significance, potentially via longitudinal methods to track stigma levels after completion of coursework. Notably, the help-seeking stigma measure was added later during data collection and as a result the smaller sample might not generalize as well. Due to the naturalistic approach of this study, comparisons of courses cannot be distinguished from any course-related features such as instructors and their teaching styles, delivery format (e.g., asynchronous online, face-to-face), and explicit course content and methods. The changes observed within each course may also be attributable to methodological confounds including testing effects or the passage of time between testing periods. Impression management may also have influenced responses, particularly with students receiving course credit for participation.
Other possible confounds include several student characteristics. Specifically, the differences in stigma reduction between Introductory Psychology students and students in other courses may be attributable to the significant age difference observed between the groups, namely that introductory students were significantly younger and may have taken less psychology coursework. Additionally, although participants across courses were primarily female, analyses indicated a larger number of males in Introductory and Abnormal psychology classrooms than would be expected by chance, and so a study with more balanced gender identity representations across the sample may yield different and more generalizable outcomes. For a more thorough discussion on gender effects, see our supplemental analyses and discussion are available on Open Science Framework (Jamieson, 2021).
It is worth noting that mental illness stigma reduction was not a specific learning objective within the psychology curriculum nor explicitly advanced as such in any of the specific courses examined in this study. However, given the popularity of the topic of mental disorders among students, its prominent place within clinical psychology, and the limited findings in the current study of stigma reduction with teaching as usual, we believe more systematic coverage of mental illness stigma would be a valuable step forward. At the same time, as new stigma-reduction strategies are introduced to the classroom, we recommend instructors evaluate learning and stigma outcomes to avoid backfire effects (Lewandowsky et al., 2012).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.