
Abstract
Humans infected by Toxoplasma gondii express no specific symptoms but manifest higher incidence of many diseases, disorders and differences in personality and behavior. The aim of this study was to compare the political beliefs and values of Toxoplasma-infected and Toxoplasma-free participants. We measured beliefs and values of 2315 responders via an online survey (477 Toxoplasma-infected) using the Political Beliefs and Values Inventory (PI34). This study showed Toxoplasma-infected and Toxoplasma-free participants of our cross-sectional study differed in three of four factors of PI34, scoring higher in Tribalism and lower in Cultural liberalism and Anti-Authoritarianism. We found sex differences in political beliefs associated with Toxoplasma infection. Infected women scored higher in tribalism and lower in cultural liberalism, compared with the Toxoplasma-free control group, while infected men scored higher in economic equity. These results fit with sexual differences in behavior and attitude observed after toxoplasmosis infection. Controlling for the effect of worse physical health and mental health had little impact, suggesting that impaired health did not cause these changes. Rather than adaptation to prevalence of parasites, as suggested by parasite-stress theory, the differences might be side-effects of long-term mild inflammatory reaction. However, to get clear picture of the mild inflammation effects, more research focused on different infectious diseases is needed.
Keywords
Introduction
Toxoplasma gondii, the parasitic protozoon of cats, infects about one-third of the human population in both developed and developing countries (Tenter et al., 2000). Infected humans express no specific symptoms of the life-long infection, however, they differ from non-infected subjects by a higher incidence of many diseases and disorders (Flegr & Escudero, 2016; Flegr, Klapilová, et al., 2014; Flegr, Prandota, et al., 2014) and also by specific changes in personality (Flegr, 2013; Khademvatan et al., 2013; Lindová et al., 2012) and behavior (Fekadu et al., 2010; Houdek, 2017). These behavioral differences are mostly considered to be products or by-products of the manipulative activity of Toxoplasma aimed to increase the chance of transmitting from the infected intermediate host, which can be any warm-blooded animal, to its definitive host, a cat (Webster, 2007). However, Toxoplasma infected animals, including humans, express many signs of the activated immune system. They have increased levels of some proinflammatory cytokines, especially IL-6 (Kaňková et al., 2010). It is known that inflammation, and independently also resulting stress have very strong impacts on various motivational, emotional, and behavioral processes, for recent reviews, see, e.g., Moieni & Eisenberger, 2018; Lasselin et al., 2018; Gassen & Hill, 2019. It was suggested (Lindova et al., 2010; Martynowicz et al., 2019; Tedford & McConkey, 2017) that a large part of the observed toxoplasmosis-associated changes are not the products of the manipulative activity of Toxoplasma but a result of mild chronic stress associated with long-term parasitic infection and resulting health problems. It is known that many toxoplasmosis-associated changes go in opposite directions in the infected men and women (Lindová et al., 2006), and also that men and women cope with stress in diametrically opposed ways (Matud, 2004; Tamres et al., 2016). The stress-coping hypothesis suggests that many toxoplasmosis-associated changes, e.g., higher extroversion in infected women and lower in men, or lower suspiciousness of infected women and higher in suspiciousness of infected men (all in comparison to non-infected peers) can be interpreted as gender-dependent stress coping reaction.
Additionally, the immune response to chronic stress due to parasite infection may elicit a different immune response in the two sexes and lead to different behavioral changes. The research focused on the role of cytokines in the inflammatory process of the CNS showed the presence of a difference between males and females (Bernardi et al., 2020; Lefèvre et al., 2012). The increment of cytokines during toxoplasmosis infection can affect the dopaminergic function (Felger & Miller, 2012) and provoke the behavioral change (Kamerkar & Davis, 2012). Indeed, many of the behavioral changes associated with toxoplasmosis are correlated with the dopaminergic system in humans and in rats (Flegr, 2007; Skallová et al., 2006). Therefore, the behavioral differences observed in infected men and women can be a consequence of differences in the immune system, related to the production of cytokines and the function of the dopaminergic system.
Among the traits affected by toxoplasmosis are also such that could affect the political beliefs of infected subjects. For example, infected men have lower superego strength, i.e., the tendency to disregard the rules of society, while the opposite tendency was observed in infected women (Flegr, 2007). Both infected men and women have lower conscientiousness (Lindová et al., 2012), lower generosity (Lindova et al., 2010) and have lower novelty-seeking (Flegr et al., 2003; Skallová et al., 2005). Men express lower and women higher altruism in the dictatorship game (Lindova et al., 2010). Infected subjects express higher entrepreneurship activity and have a higher tendency for risky behavior (Johnson et al., 2018), which might explain a higher risk of traffic accidents in the infected subjects (Flegr et al., 2002; Kocazeybek et al., 2009). Toxoplasma-infected women have also higher aggression (Cook et al., 2015) and self-aggression (Mathai et al., 2016; Postolache et al., 2021).
Although certain effects of infection by a parasitic disease on political views ought to be expected based on the research summarized above, to our knowledge, no relation of toxoplasmosis (or other parasitic diseases) and political beliefs and values has been reported to date. Moreover, studies focused on possible causal connection between infectious diseases (except for toxoplasmosis) and changes in personality profiles are also few and far between, and focused mainly on diseases causing profound changes in brain, e.g. AIDS (Meehan & Brush, 2016) or neurocysticercosis (El-Kady et al., 2021).
Regarding the connection between parasite stress and political views, there exists extensive literature describing changes in traits that differ with varied geographical parasite stress levels. All published studies, however, are population-based studies, searching for the difference between populations exposed to different intensity of the parasite stress. While it is possible to consider our data in the context of this parasite-stress theory and it will be done so in the Discussion, this study primarily focuses on association between Toxoplasma status and political beliefs on an individual level. For this purpose, we measured political beliefs and values of 2315 respondents of an internet survey (477 Toxoplasma-infected) using the Political Beliefs and Values Inventory (PI34). To test the hypothesis that the observed changes in three of the factor (Tribalism, Cultural Liberalism, and Anti-authoritarianism), but not the fourth (Economic Equity), are related to stress-coping strategies of men and women, we ran the analyses separately for each sex and to find out whether the observed differences are mediated by impaired health of the infected subjects we also analysed a complex model controlling not only for age, sex, size of place of residence, and level of education but also for physical health and mental health.
Results
The final data set of 2315 respondents, consisted of 467 men (mean age 35.54, s.d. 12.8) and 1848 women (mean age 35.95, s.d. 11.5); the difference in age was not significant (t = −0.69, df. = 2313, p = .493). In men, 90 men (mean age 35.54, s.d. 12.9) were infected with Toxoplasma and 377 (mean age 35.53, s.d. 12.4) were Toxoplasma-free; again, the difference in age was not significant (t = −0.69, df. = 2313, p = .493). In contrast, the difference in age between 518 Toxoplasma-infected women (mean age 38.39, s.d. 12.8) and 1330 Toxoplasma-free women (mean age 35.01, s.d. 11.2) was highly significant (t = −5.72, df. = 1846, p < .0001). Prevalence of toxoplasmosis was lower in men (19.27%) than in women (28.03%) (Chi2 = 14.8, p = .0001). Prevalence of toxoplasmosis decreased with size of place of residence from 32.9% in smallest villages to 20.9% in the cities over 500,000 inhabitants (Partial Tau controlled for age and sex = −0.070, p < .0001). No association was observed between toxoplasmosis and education (Partial Tau controlled for age and sex = −0.013, p = .368), however, the absence of the association in the whole population was caused by the existence of positive association between toxoplasmosis and achieved level of education in men (Partial Tau controlled for age and sex = 0.083, p = .007) and negative association between the toxoplasmosis and achieved level of education in women (partial Tau controlled for age and sex = −0.037, p = .017).
Toxoplasma-infected women expressed worse mental and physical health, and Toxoplasma-infected men worse physical health than their Toxoplasma-free peers (Figure 1). MANCOVA computed with the physical and mental health problems as the dependent variables, toxoplasmosis, sex, and sex-toxoplasmosis interaction as the factors, and age and size of place of living as covariates showed significant effects of age (F2,1843 = 70.02, p < <0.0001, partial eta2 = 0.07) and toxoplasmosis (F2,1843 = 7.34, p = .0007, partial eta2 = 0.008). Results of corresponding ANCOVA analyses computed separately for physical and mental health problems and men, women, and men and women together are shown in Table 1.

Association of toxoplasmosis and sex on health. Note. The vertical bars show 95% C.I., the mean values computed for covariates (age and size of place of living) at their means.
the Associations Between Physical and Mental Health and Toxoplasmosis.
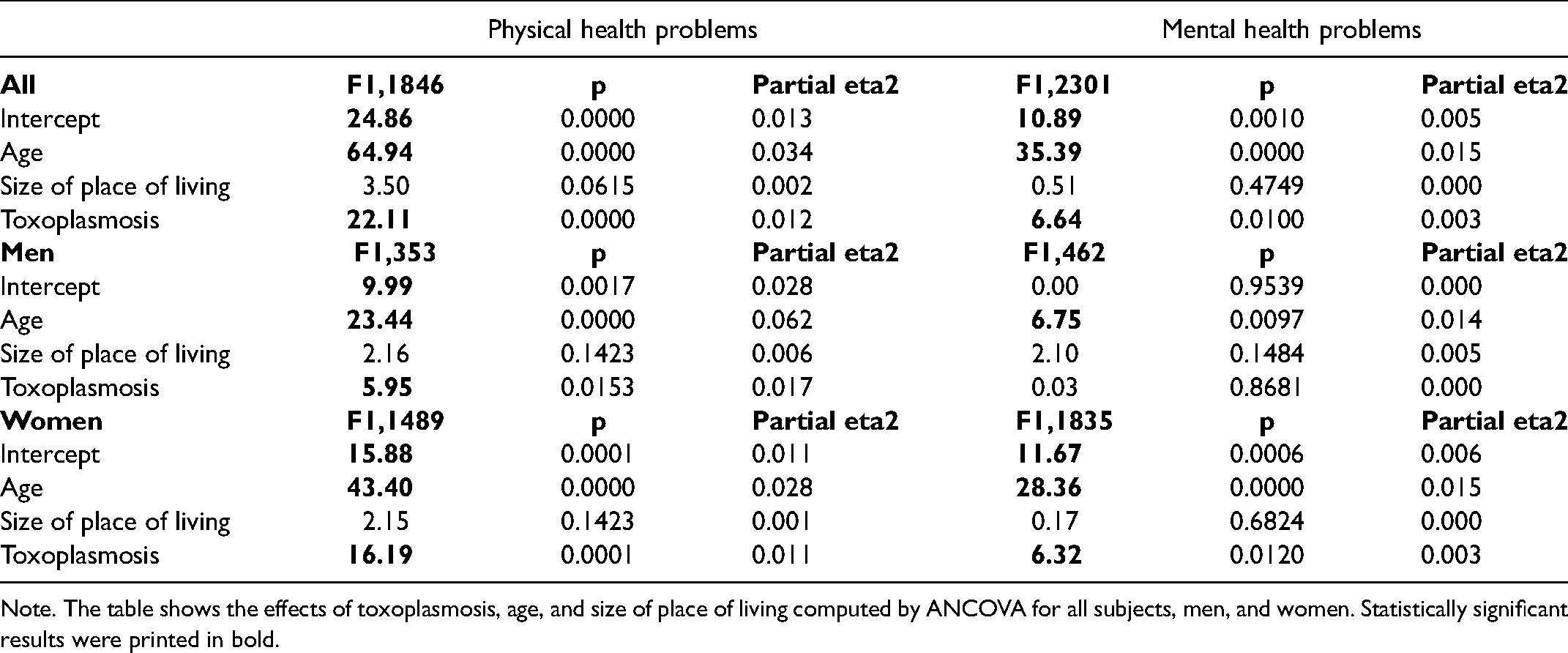
Note. The table shows the effects of toxoplasmosis, age, and size of place of living computed by ANCOVA for all subjects, men, and women. Statistically significant results were printed in bold.
Factor analysis performed on data from the Political Inventory revealed four factors with an eigenvalue higher than 1.0. According to loading of these factors by particular questions of the inventory (Table 2), it was possible to identify these factors as Tribalism (11.5% of variability), Economic equity preference (7.8% of variability), Cultural liberalism (5.1% of variability), and Anti-authoritarianism (3.0% of variability). We computed values of these four variables for each respondent as scores in particular factors.
Loadings of Four Factors Identified by Factor Analysis of 34 Questions of the Political Inventory.

To disclose the effect of Toxoplasma infection on political beliefs, we computed the associations of the toxoplasmosis with Tribalism, economic equity preference, Cultural liberalism, and Anti-authoritarianism using partial Kendall correlation controlled to age, sex, and size of place of residence. The results showed that being Toxoplasma-infected correlated positively with Tribalism and negatively with Cultural liberalism, and Anti-authoritarianism, see Table 3. All three associations retain statistical significance after the correction for multiple tests. Table 3 also shows the results of the same analyses performed separately for men and women. The most conspicuous sexual differences were the absence of the positive association of toxoplasmosis with Tribalism in men – here the partial Tau was even negative, −0.014, p = .760 in men vs. 0.040, p = .009 in women, and the presence of the positive association with the preference for economic equity in men 0.064, p = .040 but not in women Tau = 0.010, p = .526, see Figure 2.

The violin plots show the means and the distribution computed as the kernel probability density for male and female, toxoplasma-infected and toxoplasma-free participants of the study.
Correlation of Political Beliefs with Toxoplasmosis and Potential Confounding Variables.

Note. The left half of the table shows partial Kendall Tau controlled for age, sex, size of place of residence, and the right half Tau controlled for age, sex, size of place of residence, physical health, mental health, and achieved education level. A variable that was used as the dependent variable) was removed from the list of covariates to be controlled for. Statistically significant results were printed in bold.
Toxoplasmosis had a strong association with human health and the size of the place of residence. At the same time, political beliefs had a strong association with health, size of place of residence, and achieved level of education (Table 3, left part). It could be therefore speculated that the association between toxoplasmosis and health is just the side effects of the associations of toxoplasmosis with these confounding variables. To test this possibility, we repeated the partial Kendall analyses, this time controlled not only for sex, age, and size of place of residence but also for physical and mental health and achieved level of education. The results were nearly identical as those obtained with the simpler model (Table 3, right part). Therefore, the effect of toxoplasmosis on political beliefs was not mediated by the effect of toxoplasmosis on health or education.
Discussion
The present study showed that Toxoplasma-infected and Toxoplasma-free participants of our cross-sectional study differed in three of four factors measured with Political inventory, namely scored higher in Tribalism and lower in Cultural liberalism and Anti-authoritarianism. These results are in line with previous broad research, showing that individuals in parasite affected areas are more likely to be conservative and authoritarian (Murray et al., 2013).
Furthermore, we observed sex differences in the studied factors associated with the Toxoplasma infection. Indeed, Toxoplasma-infected men scored higher in Economic Equity, showing a preference for a more equal and less competitive society, while women infected with toxoplasmosis scored higher in tribalism and lower in cultural liberalism. These associations were not reduced when the effect of worse physical health and mental health were controlled, suggesting that impaired health of infected subjects is not the cause of changes in political beliefs. The same conclusion was also supported by the fact that the changes go in the same direction in men and women, because stress coping-associated behavioral and personality changes mostly go in different directions in men and women.
It was suggested by Lindová et al, (2006, 2012) that these associations might be the results of a mild chronic stress caused by the toxoplasmosis infection instead of the result of the toxoplasmosis itself. The presence of a chronic stress not only explain the presence of behavioral and political differences with the non-infected control group, but also the presence of sex differences in these behavior and ideologies as different responses to chronic stress in the two sexes, involving differences in the immune system response and in the coping strategies used. Many of the behavioral changes observed in toxoplasmosis infected people correlate with the function of dopamine in the brain and they may have more broad implications, including political ideologies. In line with our results, previous studies (Flegr et al., 2003, Skallová et al., 2005) showed that infected subjects scored lower in novelty seeking, a factor that contributes to a conservative and political opinion (Carney et al., 2008). Indeed, in our sample the infection was associated with higher tribalism and lower cultural liberalism, specifically in women. While we expected differences in the political ideologies of infected men and women, we did not expect a higher score in economic equity in infected men. Typically, men affected with toxoplasmosis showed higher risk propensity and higher entrepreneurial activities (Johnson et al., 2018) more compatible with a competitive type of economy. The association of toxoplasmosis and the preference for an egalitarian economy in men needs to be better explored in future works.
Several studies have found that societies that are more affected by infectious pathogens also exhibit higher levels of conservative political attitudes such as xenophobia and traditionalism (Bennett & Nikolaev, 2020; Murray et al., 2013; Nikolaev & Salahodjaev, 2017; Thornhill et al., 2009). Similar results have also been found in our study performed on the individual level. The hypothesis that has been proposed is that the attitudes exhibited are connected to pathogen avoidance behaviors aimed at minimizing contact with outsiders (intergroup effect) (Aarøe et al., 2017) who may be carrying new pathogens as well as the maintenance of social traditions that may serve to help protect against pathogens (intragroup effect) (Fincher & Thornhill, 2012), with evidence from a recent cross-national study favoring the intragroup effect (Tybur et al., 2016). Significantly, however, both the effects – and the intragroup effect in particular – seem potentially open to the interpretation that they are generalized responses to stress, rather than to a pathogen (Brown et al., 2016; Currie & MacE, 2012; Hruschka & Henrich, 2013; Ma, 2020).
While the present study examines differences found in association between a parasitic infection and political values in context of increased stress at individual level, the results can be seen as an alternative to the parasite stress theory (Fincher et al., 2008; Thornhill & Fincher, p. 2014) for the following two main reasons: Parasite-stress theory aims to be the ultimate evolutionary explanation of changes in traits that differ with varied geographical parasite stress levels, yet this study focuses directly on the difference between actual infected and non-infected subjects in one small region, where the intensity of the parasite stress is mostly constant (and low). Second reason is that it has been shown that primarily non-zoonotic diseases have a relation to human personality and societal values (Thornhill et al., 2010). However, toxoplasmosis is primarily a zoonotic disease with very specific and limited spread between people – the only intrapersonal route of infection was suggested from male to female or between two male partners through sexual transmission (Flegr, Klapilová, et al., 2014; Flegr, Prandota, et al., 2014; Hlaváčová et al., 2021; Kaňková et al., 2020).
This being said, there might be a possible connection between the present study and the parasite-stress theory after all. An extensive body of research confirms association between infectious (and in most cases parasitic) diseases and changes in personality profile of animals from molluscs (Seaman & Briffa, 2015) and minnows (Kekäläinen et al., 2013) to migratory birds (Marinov et al., 2017) and mammals (Boyer et al., 2010) including men (Webster, 2001). There are also well studied associations between personality traits and political views, e.g. (Furnham & Fenton-O’Creevy, 2018; Harell et al., 2021; Verhulst et al., 2010; Wang, 2016). While the direction of causality needs to be studied further (Bakker et al., 2021) and while the human-centred field of parasite induced changes in personality traits is regrettably understudied and quite complex (Friedman, 2008), we might expect at least some effect of infectious diseases on political attitudes caused by shifts of personality traits. A possibility thus exists, that at least part of the reported difference in political attitudes in countries with different parasitic disease burdens is not caused by parasite-avoidance but results from a significant part of the population being infected with one or multiple pathogens. This hypothesis is supported by studies that linked a change in personality traits with clear connection to political attitudes (e.g., conservatism) with chronic diseases, although not the infectious ones (Mendelsohn et al., 1995; Sutin et al., 2013). On the other hand, some results suggest stronger prediction of personality traits by historical prevalence of diseases rather than by the current situation, suggesting parasite-avoidance as a factor with greater importance in personality shifts (Schaller & Murray, 2008).
Since the available body of literature discussing possible causal relationships between infectious diseases and political beliefs and values is very sparse, this direction of research might provide interesting and important insight into the changing political climate in certain countries. Studies focused on a wider range of infectious diseases besides toxoplasmosis and severe debilitating illnesses such as neurocysticercosis or AIDS would be especially valuable.
The present study showed a 19% prevalence of toxoplasmosis in men and 28% in women. The most recent Czech epidemiological study performed between 2014–2015 (Flegr, 2017) showed the prevalence of 25% in men and 36% in women aged 30–39 years. It is known, however, that prevalence of toxoplasmosis decreases relatively quickly in most developed countries, including the Czech Republic. For example, a large epidemiological study performed on Czech male soldiers 20 years ago found a prevalence of 35% for the age strata 30–35 years (Kolbekova et al., 2007). It is, therefore, possible that the observed seroprevalence reflects the actual situation in the Czech general population.
Limitations
The main limitation of the present study was the fact that the participants of the study were self-selected. Their subpopulation probably represents a specific (more altruistic and more curious) segment of the Czech population, rather than a random sample of the Czech internet population. In addition, people with impairments or severe diseases as well as those from the lowest socioeconomic strata were unable to participate. It is not therefore clear to which extent the results can be generalized to the general Czech (or the World) population.
Another limitation of the study is the moderate number of Toxoplasma-infected men (90). The reason of imbalanced sex ratio was the fact that women are often tested for toxoplasmosis during pregnancy and therefore a larger fraction of women than men know their toxoplasmosis status. Due to the lower number of men, the associations of toxoplasmosis with Cultural liberalism and Anti-authoritarianism were not significant in men, despite being stronger in men than in the more numerous (518) women.
Since this study dealt with the effect of pathogen-caused stress, there is a possible interference of the global COVID-19 pandemics. However, only 6% of the respondents participated in the period between April 2020 when the first infection in Czechia was observed, and the end of data collection in April 2021.
In the present study, we calculated aggregate indices of physical and mental health and used these indices in our statistical models. In future studies, it will be valuable to analyse the effects of individual health-related variables to disentangle the complex relationships between toxoplasmosis, mental and physical health, psychological traits and political beliefs. Such research could also answer important questions related to the causal direction of the observed correlations.
The associations found in the present study are based on correlations and we cannot infer the direction of causality. It cannot be ruled out that the explanation of the effect is in the opposite direction, that e.g., higher tribalism itself, by an unknown mechanism, increases the chance of being infected by Toxoplasma gondii. Like nearly all past studies, also this one was cross-sectional in nature. It is very difficult to study the relationship between Toxoplasma infection and personality using a longitudinal design. The frequency of the Toxoplasma infection in adulthood is low, and thousands of participants should be recruited to find several dozens of subjects who will acquire the infection during the study. Until such a study is performed, any conclusion about the causality behind the correlation between the infection and human personality must be based only on analogies with animal models (Skallová et al., 2006; Hodková et al., 2007) or on the existence of a correlation between length of infection and observed personality trait changes (Flegr et al., 1996, 2000) and must be therefore considered only provisional.
Further research is also needed to better clarify the extension and the implication of the associations we found between toxoplasmosis infection and political ideologies, and to clarify the role of sex differences.
Material and Methods
Subjects
The questionnaire was distributed via the internet as an online Qualtrics survey. Participants were invited to partake in the study using a social media-based snowball method (Kankova et al., 2015). Potential volunteers, mostly members of the “Lab bunnies” community, an 18,000-member group of Czech and Slovak nationals willing to take part in evolutionary psychology experiments, were invited to participate in an anonymous study about “mystical thinking, superstitions, prejudices, religion and the relation between various environmental factors and health and wellbeing.” The online questionnaire was also promoted in various types of electronic and printed media and TV. Toxoplasmosis and political belief were not explicitly mentioned in the information provided to potential participants in order not to affect the participants’ responses; this procedure was approved by the IRB, see below. They were, however, informed about that the data anonymously collected in the research will be health- and beliefs-related and gave their informed consent with participation in the experiment. Responders were not monetarily compensated for their participation in this study; nevertheless, after finishing the approximately 80 min questionnaire, they were provided with information about the results of related studies and their own results of several tests that were part of the questionnaire.
At the beginning of the survey, the participants were given the following information and were asked to provide their informed consent to participate in the study by pressing a special button: “The study is anonymous and obtained data will be used exclusively for scientific purposes. Your cooperation in the project is voluntary and you can terminate it at any time by closing this web page. You can also skip any uncomfortable questions; however, complete data is most valuable. If you agree to participate in the research press the “Next” button”. Only the subjects who provided their informed consent (95.2% of the visitors of the web page) were allowed to participate in the study. Between 27th May 2016 and 24th April 2021, 14,902 responders took part in the study.
All methods were performed in accordance with the relevant guidelines and regulations. The project, including the method of obtaining electronic informed consent to participate in this anonymous study from all participants, was approved by the IRB anonymized.
Questionnaire
The electronic survey consisted of several parts that concerned various unrelated projects on evolutionary psychology and psychiatry. In the present study, we inspected and analysed only the data from the Political Inventory (see below), Toxoplasma seropositivity. Regarding toxoplasmosis, participants were asked whether they were laboratory tested for toxoplasmosis, what was the result of the laboratory test, and what was the reason for their test. Only participants who were tested due to pregnancy (62% of female participants), health reasons (28% male and 20% female participant), or as part of other research (60% male and 35% female participants) and were, therefore, informed about their toxoplasmosis status by a medical or research professional were included in the study. In the Czech Republic, IgG ELISA is always used in clinical diagnostic, however, in our research, the participants were tested with both ELISA and complement fixation test, therefore a certain fraction of participants were tested with both tests. To control for potential confounding variables, the responders were also asked about their sex, age, education (ordinal scale 1–8: 1– elementary, 8 – Ph.D.), and the size of the communities where they currently live (ordinal variable urbanization: 0 – less than 1000 inhabitants, 1: 1–5 thousand inhabitants, 2: 5–50 thousand inhabitants, 3: 50–100 thousand inhabitants, 4: 100–500 thousand inhabitants, 5: more than 500 thousand inhabitants).
In the anamnestic part of the questionnaire, the participants were also asked to respond to a set of questions concerning their physical health and mental health. They were asked how many different prescription drugs they were taking currently, how many different non-prescription drugs they were taking currently (“how many different herbs, food supplements, multivitamins, superfoods, etc. do you currently take per day”), how many times they visited their primary care doctor in past 365 days (“not for prevention”), how many times they used antibiotics in the past 365 days, and how many different medical specialists they visited (not for prevention) in the past five years. The physical health problems score was calculated as a mean of Z-scores of the last five variables. The responders were also requested to rate how much they suffer from anxieties, phobias, depression, mania, obsessions, auditory hallucinations, and visual hallucinations using a 0–100 scale. We also counted the number of diagnosed and the number of undiagnosed mental health disorders that the responders checked on a list of 25 mental health disorders and epilepsy. The mental health problems score was calculated as a mean of Z-scores of these 9 variables.
Political beliefs and values of the responders were measured with the Political Inventory (PI34). This instrument consisted of 34 questions (see English translation in appendix) in randomized order. The respondents rated the strength of agreement with statements on a scale of 1–5 (1 – strongly disagree, 2 – rather disagree, 3 – neither agree nor disagree, 4 – rather agree, 5 – strongly agree). The ratings were inversed for questions marked with r. Tribalism is calculated as the arithmetic means of responses to questions 8, 9, 15, 16r, 17r, 18, 19, 21, 24, 25, 30, 32, 34; Economic equity as the arithmetic mean of responses to questions 1, 4, 6, 11r, 20, 26, 27r; Cultural liberalism as the arithmetic mean of responses to questions 2, 7, 14, 21r, 23r; and Anti-authoritarianism as the arithmetic mean of responses to questions 3, 12r, 13, 22, 24r, 29, 33. Rather than examining actual partisanship related to established political parties or established ideologies, we assembled the Political Inventory based on contemporary public discourse in the Czech society as a culturally specific questionnaire was needed. Selection of topics for PI34 was inspired mainly by 10 Items in the ideological Consistency Scale by PEW based on the using set of questions since 1994 (Dimock et al., 2014) and the 12-item political and social conservatism scale (Everett, 2013).
Statistics
The raw data file contained the records of 14,902 participants, some of them, however, did not complete the final parts of the questionnaire with the political inventory. We filtered out all subjects younger than 18 and older than 90 years. We also filtered out all records with suspicious data, e.g., those from subjects reporting too low (< 130 cm) or high (> 215 cm) body height and too high number of reported diagnosed or undiagnosed mental health disorders (>10). This data set was used for computing physical health problem scores, mental health score (see above), and for factor analyses. In the main analyses, we used the factors (scores) computed with the Maximum likelihood factors extraction method after varimax rotation, however, the results were very robust; a nearly identical structure of factors was obtained with another method of factor extraction and other methods of factor rotation. In fact, all four factors (plus four other factors) were identified even by the principal component analysis.
For analysing the association between toxoplasmosis and political beliefs we used a core data set consisting of 2315 responders who had been tested for toxoplasmosis in the past and were able to provide us with the information about the results of their laboratory test. About 39% of participants were tested in our laboratory during other scientific studies, 29% during pregnancy, 22% because of their health problems, and 10% for other reasons, e.g., curiosity, blood donation, their partner's pregnancy, etc. Some output variables had asymmetric distribution; therefore, we performed all focal analyses with a partial Kendall test that is not sensitive to such irregularity in data. The correction for multiple tests was performed with the Benjamini-Hochberg procedure with a False Discovery Rate set to 0.1 (Benjamini & Hochberg, 1995). Partial Kendall tests were performed in R 3.3.1 (R Core Team, 2018) using the package ppcor (Kim, 2015). All other tests, factor analyses, and PCA analyses were performed with the statistical package Statistica v. 10.0.
Conclusions
Beside worse mental health in Toxoplasma-infected women and worse physical health of Toxoplasma-infected participants of both sexes, our study showed sex-dependent differences in Tribalism, Cultural liberalism, and Anti-authoritarianism between Toxoplasma-positive and Toxoplasma-negative subjects. Specifically, we have found positive association of toxoplasmosis and Tribalism in women but not in men, and a positive association of toxoplasmosis and preference for social equity in men but not in women, in both sexes, there were also negative associations with Cultural liberalism and Anti-Authoritarianism. While our results are in agreement with the parasite-stress theory that predicts higher Authoritarianism and Conservatism in areas with higher prevalence of parasitic diseases, the results cannot be interpreted simply in the framework of this theory, i.e., as a result of enhanced behavioral immunity (parasite avoidance). Rather, the direct effect of long-term mild stress caused by an inflammatory reaction to the presence of a parasite may be at play, shifting hosts’ personalities and thus also their political attitudes. Considering the substantial lack of literature discussing effects of mild infectious diseases on personality traits of infected individuals as well as effects of being infected by a parasite on political beliefs and values, further research should be encouraged.
Footnotes
Author Contribution
Conceptualization RK, LP, JF; methodology RK, LP, SB, KTK, JF; data curation JF; statistical analysis JF; writing - original draft and reviewing and editing RK, LP, SB, KTK, JF. All authors have read and agreed to the published version of the manuscript.
Data Availability
Dataset available on Figshare.com https://figshare.com/s/fb78539b38e11db6f73f
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Grantová Agentura České Republiky, (grant number 21-31059S).
Institutional Review Board Statement
This study was approved by the IRB of the Faculty of Science, Charles University (Komise pro práci s lidmi a lidským materiálem Přírodovědecké Fakulty Univerzity Karlovy)—No. 2015/07
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.