
Abstract
An ecological approach to social perception states that impressions of faces have functional value in that they guide adaptive behavior ensuring people's survival. For example, people may avoid others whose faces appear sick to avoid an illness representing a survival threat. We broadened the ecological approach in the current work by examining whether merely thinking about what illnesses on faces look like (i.e., how sickness on faces is represented) holds functional value in guiding behavior to ensure survival. Using an example of a real illness threat as proof of concept, we showed that people self-reported performing more adaptive health behaviors in response to COVID-19 if they had sicker representations of COVID-19 on faces (Experiment 1a). These sicker representations of COVID-19 on faces explained, in part, a positive relation between perceptions of COVID-19 as threatening and people's self-reported adaptive health behaviors. We then replicated these patterns when experimentally manipulating illness threat (Experiment 1b). We found that people expected more adaptive health behaviors and had sicker representations of illness on faces in response to illness threats that were more relative to less threatening. These findings suggest that mentally representing sickness on faces is enough to guide people's behaviors in response to illness threats.
The COVID-19 pandemic has presented an enormous public health challenge for the United States and the world. Slowing the spread of the illness requires people's engagement in behaviors aimed to protect them and vulnerable groups. As such, the Centers for Disease Control (CDC) advocates the increased practice of adaptive health behaviors such as hand-washing, social distancing, and self-quarantining, among others (CDC, 2021). Because these behaviors have been key to slowing the spread of COVID-19 (CDC, 2020), of interest is the identification of factors relating to people's increased adherence to them (e.g., Mortensen et al., 2010; Sharot, 2011; Witte & Allen, 2000). Although many factors likely contribute to engagement in adaptive health behaviors (for a review, see Lunn et al., 2020), the current investigation focused on face perception. An ecological approach to face perception suggests that trait impressions from faces are highly functional because they provide cues to ensure survival (Zebrowitz & Montepare, 2006). The adaptive value of identifying sick faces, for example, may prepare people to respond to cues potentially marking sickness (Zebrowitz et al., 2003). Whether such aspects of face perception relate to engagement in adaptive health behaviors, however, is understudied. Here, we examined how representing sickness in faces related to self-reported engagement in adaptive health behaviors at the onset of the COVID-19 pandemic (Experiment 1a) and anticipated engagement in response to hypothetical illnesses (Experiments 1b).
People engage in adaptive health behaviors (e.g., wearing masks) to protect against disease-causing organisms. Much work on understanding adherence to adaptive health behaviors has focused on the behavioral immune system (Schaller, 2011). The behavioral immune system is a theorized motivational system causing people to avoid disease-causing organisms in the service of ensuring their survival (Schaller, 2011; Schaller & Park, 2011). One function of the behavioral immune system is that it enables people to avoid infected individuals (van Leeuwen & Petersen, 2018). For example, people avoid others whose facial characteristics suggest the presence of infectious diseases (Ryan et al., 2012).
Research on the behavioral immune system has largely been conducted using experimental manipulations of people's vulnerability to infectious diseases (for a review, see Schaller, 2011). People rate themselves lower on extroversion, for example, when illness threats are more salient (Mortensen et al., 2010), suggesting that illness threats elicit self-protective avoidance responses. The behavioral immune system has implications for a largely distinct literature on trait impressions of faces (see, e.g., Ryan et al., 2012). Trait impressions of faces are also self-protective in that they relate to motivations to approach what looks safe and to avoid what looks threatening (e.g., Slepian et al., 2017). Such work is characteristic of an ecological approach to social perception oft-discussed in the social cognition literature, which asserts that face impressions are rooted in motivations to thrive within one's environment (McArthur & Baron, 1983).
The ecological approach asserts that faces provide adaptive cues about potential social interactions (McArthur & Baron, 1983). For example, whereas angry faces elicit avoidance responses among perceivers (Marsh et al., 2005), babyish faces elicit approach responses (Berry & McArthur, 1986). Although this approach may often assume impression accuracy, face impressions often do not predict target behaviors (e.g., Rule et al., 2013). Thus, the ecological approach proposes that being attuned to facial cues produces biased face impressions through overgeneralization (Zebrowitz & Montepare, 2006). Overgeneralization effects emerge when facial cues shown to accurately characterize, for example, low unhealthiness, are also perceived in people whose facial characteristics simply resemble being unhealthy (Zebrowitz et al., 2003). Using face impressions to adjust behaviors in self-protective and evolutionarily adaptive ways is consistent with both an ecological approach to social perception and the behavioral immune system. Recognizing and avoiding sickness is important for survival, suggesting that perceiving sickness in faces is functionally adaptive in that it will help people avoid disease-causing organisms. Supporting this idea, impressions of normal adult faces’ unhealthiness are predicted by their similarity to faces of actually unhealthy people (Zebrowitz et al., 2003). Further, impressions of faces as unhealthy positively relate to people's discomfort with contact with those targets (Bressan, 2021; van Leeuwen & Petersen, 2018). Notably, this work has largely examined responses to actual faces. While key to identifying how sickness-related facial cues affect self-protective adaptive health behaviors, people also think about faces when they are not responding to a specific person. That is, they have images in their minds of others (i.e., they mentally represent faces of people) who have distinct trait attributes (e.g., Dotsch et al., 2008). Whether these mental images hold functional value to affect adaptive health behaviors is unclear.
That representing attitudes and beliefs in mental images of faces holds consequences for people's behaviors indirectly supports the possibility that mentally representing sickness on faces relates to adaptive health behaviors. In one study (Brown-Iannuzzi et al., 2017), people mentally represented negative traits in welfare recipient faces. Suggesting consequences of these representations, people were less likely to support giving welfare benefits to a person depicted by a welfare recipient relative to a non-welfare recipient face representation. These findings support the possibility that mentally representing sickness on faces may have functional value in guiding adaptive health behaviors. Since these behaviors are self-protective, such a pattern would support work showing that attitudes and behaviors toward people exhibiting disease-associated are a biproduct of the behavioral immune system (Crandall & Moriarty, 1995; Kurzban & Leary, 2001). The current work provides proof of concept of this possibility over two experiments.
Experiment 1a
Given variability in risk perceptions of COVID-19 worldwide (Dryhurst et al., 2020) and divergent messaging about COVID-19 within the United States (Niemi et al., 2021), we first examined whether mentally representing sickness related to COVID-19 on faces at the onset of the pandemic related to people's adaptive health behaviors in response to it. We used reverse correlation to quantify sickness representations of COVID-19 on faces. Reverse correlation estimates representations of traits on faces without explicit endorsement by generating images of how people visualize traits (for details, see Dotsch & Todorov, 2012). Such paradigms are popular in social cognition research because they capture how people visualize traits while prohibiting social desirability from affecting responses (e.g., Petsko et al., 2020).
First, we sought to identify a positive relation between representing sickness related to COVID-19 on faces and adaptive health behaviors in response to it (Hypothesis 1). Second, we sought to characterize this relation's specificity. One possibility was that specifically representing COVID-19 on faces as sicker would relate to reporting more adaptive health behaviors in response to it. If true, the expected relation should emerge when people represent COVID-19 on faces as sicker, but not another illness (Hypothesis 2a). Another possibility was that more general representations of sickness would relate to adaptive health behaviors in response to COVID-19. Indeed, such behaviors can more generally prevent illness spread (Xun et al., 2021). If true, the expected relation should generalize to representing sickness due to another illness (Hypothesis 2b). To this end, people were randomly assigned to generate representations of COVID-19 or the common cold on faces.
Third, we explored whether attitudes toward COVID-19 related to adaptive health behaviors in response to it through representing sickness related to COVID-19 on faces with, which would provide more evidence that representing sickness in faces has functional value. Because threat-related responses are consistent with perspectives (McArthur & Baron, 1983; Slepian et al., 2017; Zebrowitz & Montepare, 2006) suggesting that face impressions guide survival, we reasoned that perceiving COVID-19 as threatening relative to other illnesses may relate to sicker representations of faces with the illness. We expected that sicker representations of COVID-19 on faces may explain, in part, a positive relation between perceiving COVID-19 as threatening and performing more adaptive health behaviors in response to it (Hypothesis 3).
Method
Participants
A power analysis (G*Power; Faul et al., 2007) using f = .15 and alpha = .05 targeted 77 participants for 80% power to detect a significant regression model to determine if mental representations of sickness, the represented illness, or their interaction positively related to adaptive health behaviors. One-hundred fifty people from MTurk participated on March 18, 2020. We oversampled to account for expected online participant loss. We excluded 14 people for responses suggesting that they were “bots,” two for indicating that they had not heard of COVID-19, one who did not respond to 65% of items in the main task (see below), and one for submitting a code to MTurk twice. These exclusions yielded a sample of 132 participants (Mage = 38.94, SD = 12.38, Myears of education = 15.64, SD = 1.87; 69 female). The University of North Carolina at Greensboro IRB approved all experiments. All participants provided informed consent. Data analyzed for all experiments can be found at https://osf.io/2qthf/?view_only=8ba476e1dc354b229bba8a5b7c4bbe36.
Estimating Mental Representations of Sickness
The reverse correlation paradigm is a data-driven approach quantifying how people visualize faces in their minds (i.e., how they mentally represent them) over two phases. Mental representations widely vary in how they reflect different traits (e.g., Dotsch & Todorov, 2012), making them well-suited to determine how mentally representing sickness in faces relates to the range of adaptive health behaviors shown in response to COVID-19. Unlike traditional rating experiments (e.g., Rule et al., 2013), reverse correlation provides an estimate of traits that are not affected by scale use (e.g., little variability in responses).
Reverse correlation phase 1: generating face classification images
In the first phase, people generate classification images (CLIs) via a face classification task. A CLI is a mental representation of a face quantified by the combined average of all image choices on a given prompt. Here, people were randomly assigned to select which face of a pair looked more like it had COVID-19 (N = 61) or the common cold (N = 71). Men and women were evenly distributed across these task versions, χ2 (1, N = 132) = 0.10, p = .76.
Phase 1 stimuli
Reverse correlation tasks require the selection of a base face. Like prior work (e.g., Ratner et al., 2014), we selected the neutrally expressive average male face from the Karolinska Face Database (Figure 1a; Lundqvist et al., 1998) as the base face. One hundred Phase 1 trials of two faces each were created from this base face by superimposing randomly generated patterns of noise onto it (for details, see Dotsch & Todorov, 2012). Each of 100 trials comprised the base face layered with a unique noise pattern and the base face layered with the reverse of that unique noise pattern.
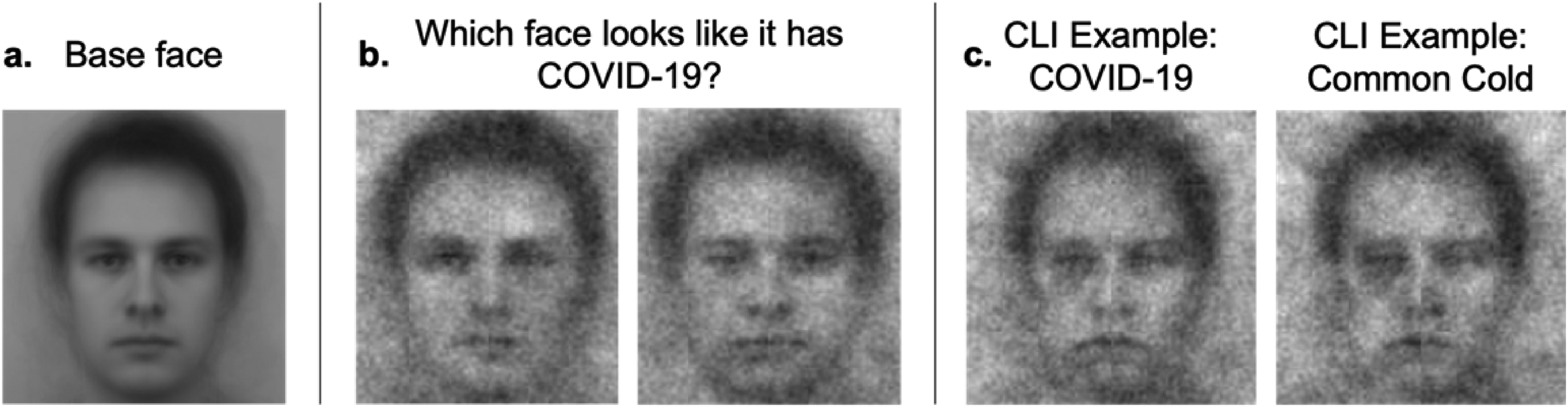
The base image (a) and an example trial (b) used in the first part of the reverse correlation paradigm. Example CLIs from people randomly assigned to evaluate which face looked like it had COVID-19 or the common cold (c).
Phase 1 task
The Phase 1 task consisted of 100 randomly presented self-paced trials. People selected which face of each pair looked more like it had COVID-19 or the common cold, depending on task version (see Figure 1b for an example trial). After being prompted to identify which face looked like it had the common cold, for example, the selected image reflects the representation of any given pair better reflecting the common cold.
Image processing
One unique CLI was generated for each person by averaging the noise patterns from the person's 100 choices and superimposing the averaged noise pattern onto the base face. Each CLI reflects each person's unique representation of the face of someone with COVID-19 or the common cold. See Figure 1c for example CLIs.
Reverse correlation phase 2: quantifying mental representations of traits on faces
The second phase consists of a task in which raters unique from people who generated the CLIs rate the CLIs on traits (e.g., sickness). The raters are unaware of what prompt yielded the CLIs. Their ratings quantify trait representations of faces (e.g., how much sickness is represented). We recruited two samples of MTurk raters for this phase. Of interest was 22 raters (Mage = 40.73, SD = 15.07, Myears of education = 15.36, SD = 2.11; 9 female) who rated CLIs on sickness (“How sick/unhealthy does this face look?”) on a scale ranging from 1 (not at all sick/unhealthy) to 5 (extremely sick/unhealthy). An additional 22 raters (Mage = 43.91, SD = 14.21, Myears of education = 15.90, SD = 1.64; 10 female) rated CLIs on aggression (“How aggressive does this face look?”) on a scale ranging from 1 (not at all aggressive) to 5 (extremely aggressive). We collected aggression ratings to explore if an expected positive relation between representations and adaptive health behaviors reflected a sickness effect or broader negativity effect.
Planned missing data design for face ratings
We used planned missing design methods to obtain ratings of the CLIs (Graham et al., 1996, 2001, 2006). The literature on “rater effects” shows that raters are prone to fatigue and diminished motivation when rating a large number of items, which often results in coarsened ratings (e.g., raters start using only the extremes of the scale or giving most objects the same score; Engelhard et al., 2018; Wu, 2018). Here, we expected acute rater fatigue because of the large number of highly similar CLIs. To avert this problem, we applied planned missing rater designs, which are commonly used in large-scale educational assessment when it isn't desirable or possible for all raters to rate all items (Eckes, 2011). In short, items to be rated are sorted into blocks, and raters receive a subset of the blocks.
The Supplemental Material visualizes our anchor test design (Enders, 2010). The 132 CLIs were randomly divided into 12 blocks of 11 faces each. All raters judged the first block (the anchor block) and two other blocks. The other two blocks were assigned according to the planned missing design shown in the Supplemental Material. The design has 11 forms, so recruiting 22 raters enabled the rating design to be completed twice. With 22 raters, the design resulted in all faces being judged by at least 4 raters and in all raters judging 36 CLIs (rather than 132). Although it is not necessary to use a shared anchor block, simulation work shows that it reduces estimation error and that it guarantees that the resulting correlation matrix is linked (Enders, 2010; Silvia et al., 2014).
When every rater judges every item (CLIs, in this case), one can simply average the ratings. For incomplete rating designs like ours, many-facet Rasch models (MFRM; Linacre, 1989) estimate the true score. The MFRM approach can accommodate the missing data caused by the sparse rating design, and corrects for the fact that some raters tend to be relatively lenient (give high scores) and others are relatively severe (Eckes, 2011; Engelhard & Wind, 2017). The MFRM framework is ubiquitous in psychological and educational assessment involving human raters (Myford & Wolfe, 2003; Primi et al., 2019; Robitzsch & Steinfeld, 2018). We estimated a score for each face, based on the ratings given for it, using the package sirt (Robitzsch, 2020) in R. The model was estimated using marginal maximum likelihood, and the resulting expected posteriori (EAP) scores were centered at 0.
Characterizing Illness-Related Attitudes and Behavior
After the first phase of the reverse correlation paradigm, people completed items measuring their adaptive health behaviors and illness threat perceptions as well as the Domain-Specific Risk-Taking (DOSPERT) and Perceived Vulnerability to Disease (PVD) scales in a random order. Listed Cronbach's alphas indicate response agreement for these participants. Significant intercorrelations (Table 1) in the expected directions between the adaptive health behaviors measure, the DOSPERT, and the PVD suggest validity across measures.
Intercorrelations between Sickness Representations and Relevant Participant Characterization Variables in Experiment 1a.
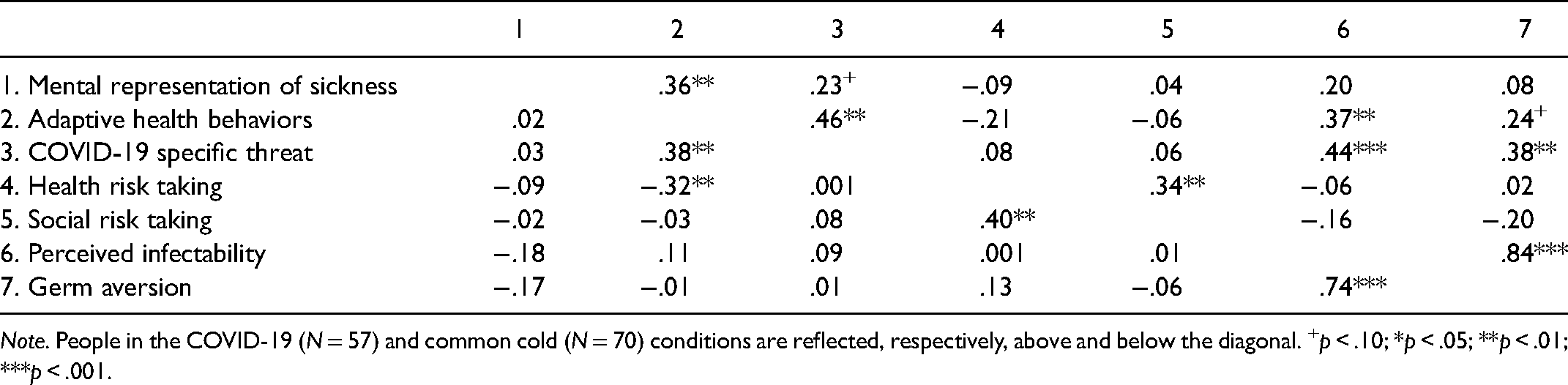
Note. People in the COVID-19 (N = 57) and common cold (N = 70) conditions are reflected, respectively, above and below the diagonal. +p < .10; *p < .05; **p < .01; ***p < .001.
Adaptive health behaviors
People indicated their engagement in adaptive health behaviors in response to COVID-19 over three randomly presented items. People characterized their handwashing (“Are you washing your hands more than you usually would because of COVID-19?”), social distancing (“Social distancing is the act of limiting exposure to groups of people by avoiding large gatherings, public events, and crowded rooms. Are you engaging in social distancing more than you usually would because of COVID-19?”) and self-quarantining (“Self-quarantining is when you stay home and avoid contact with all other people. Are you engaging in self-quarantining more than you usually would because of COVID-19?”) using a scale ranging from 1 (not at all) to 7 (very much). Responses (Cronbach's α = .86) were averaged to create a composite adaptive health behavior score (M = 6.11, SD = 1.11).
Illness threat
People responded to three randomly presented sets of three items each measuring illness threat. Two sets measured threat regarding COVID-19 and the common cold (“Overall how threatening to do think COVID-19 [the common cold] is to you [your family and friends; all Americans]”) using a scale ranging from 1 (not at all threatening) to 7 (extremely threatening). Responses regarding COVID-19 (Cronbach's α = .88) and the common cold (Cronbach's α = .95) were averaged to create two threat composites (MCOVID−19 = 4.92, SD = 1.49; MCommon cold = 3.10, SD = 1.75). A third set measured the relative threat of COVID-19 (“Relative to other illnesses (e.g., common cold), how threatening do you think COVID-19 is to you [your family and friends; all Americans]),” using the same scale. and responses (Cronbach's α = .87) were averaged to create a relative threat composite (M = 4.98, SD = 1.48). For exploratory analyzes, we focused on relative threat because it isolates threat specific to COVID-19.
Risk taking
The Domain-Specific Risk-Taking Scale (DOSPERT) is a validated scale assessing risk-taking behaviors (Weber et al., 2002). People completed the social and health subscales to measure the extent to which they make risky decisions in both domains. The subscales consist of 16 items (seven for the health and nine for the social) rated on a scale ranging from 1 (very unlikely) to 7 (very likely). Higher summed scores represent more risky behavior.
Disease vulnerability
The Perceived Vulnerability to Disease Scale (PVD; Duncan et al., 2009) is a validated scale consisting of two subscales with items rated on a scale ranging from 1 (strongly disagree) to 7 (strongly agree). The perceived infectability (PI) subscale consists of seven items measuring beliefs about the functioning of the immune system and susceptibility to infectious diseases (e.g., “In general, I am very susceptible to colds, flu and other infectious diseases”). The germ aversion (GA) subscale consists of eight items measuring aversive affective responses during situations that present a high chance of contracting a disease (e.g., “It really bothers me when people sneeze without covering their mouths”). Higher summed scores indicate more perceived vulnerability or GA. Each subscale also includes 3 reverse scored items (Duncan et al., 2009, p. 542).
Other measures
We collected additional measures unrelated to the goals of the current work for future lab research (see Supplemental Material). After completing these measures, people were asked if they had heard of COVID-19 as a manipulation check. People also indicated the extent to which they paid attention and followed task instructions using a scale ranging from 1 (not at all) to 7 (completely) (M = 6.86, SD = 0.44). People lastly provided demographic information.
Of interest was identifying a positive relation between representing faces of people with COVID-19 as sicker and engagement in adaptive health behaviors in response to the illness. We took a conservative approach to testing this relation by excluding five likely overly influential datapoints over three standard deviations away from the means of the relevant measures before conducting analyzes.
Results
People generating representations of faces with COVID-19 and the common cold were equated on characterization and demographic variables, ts < 1.69, all ps > .09. See Table 2 for descriptive and inferential statistics.
Descriptive (M, SD) and Inferential Statistics on Participant Characterization Measures in Experiment 1a.

Preliminary Analyzes: Characterizing Threat toward COVID-19 and the Common Cold
An independent-samples t-test showed that people perceived COVID-19 (M = 4.92, SD = 1.49) as more threatening than the common cold (M = 3.10, SD = 1.75), t(126) = 10.75, p < .001, d = 0.95. A one-sample t-test against the scale midpoint (4) verified that people perceived COVID-19 as more than a moderate threat than other illnesses (M = 4.98, SD = 1.48), t(126) = 7.44, p < .001, d = 0.66.
Hypothesis 1: There is a Positive Relation between Mentally Representing Sickness in Faces with COVID-19 and Engagement in Adaptive Health Behaviors
We first conducted correlations to explore the hypothesized relationship between mental representations of sickness and engagement in adaptive health behaviors. See Table 1 for intercorrelations between representations of sickness in faces with COVID-19 and the common cold as quantified by the Phase 2 raters and the above-described relevant measures.
Supporting Hypothesis 1, people with sicker COVID-19 representations on faces reported engaging in more adaptive health behaviors in response to the illness r(55) = .36, p = .006 (Figure 2a). This relation remained significant when controlling for social risk taking, health risk taking, PI, and GA, r(51) = .29, p = .04. The relation between mentally representing sickness related to the common cold on faces and engaging in adaptive health behaviors in response to COVID-19 was non-significant, r(68) = .02, p = .88.

In Experiment 1a, mentally representing sickness related to COVID-19 (but not the common cold) on faces positively related to self-reported adaptive health behaviors in response to COVID-19 (a). An exploratory analysis showed that having sicker mental representations of COVID-19 on faces partially explained a positive relation between threat-specific to COVID-19 and self-reported adaptive health behaviors in response to COVID-19 (b).
Support for Hypothesis 2a: Engaging in more Adaptive Health Behaviors was Specific to Mentally Representing Faces with COVID-19
To determine whether representing sickness in faces and engaging in adaptive health behaviors in response to COVID-19 was specific to mentally representing sickness related to COVID-19 on faces, we conducted a linear regression using Model 1 in PROCESS for SPSS (Hayes, 2012). Condition was dummy coded (0 = common cold, 1 = COVID-19). Sickness ratings from Phase 2 of the reverse correlation task were mean-centered.
The model was significant, F(3, 123) = 2.95, p = .04, R2 = .07. An interaction between Illness and Sickness emerged, b = 0.91, SE = 0.43, t = 2.10, p = .04. Supporting Hypothesis 2a, representing sickness related to COVID-19 on faces positively related to engaging in adaptive health behaviors in response to COVID-19, b = 0.95, SE = 0.34, t = 2.83, p = .005, but not the common cold, b = 0.04, SE = 0.27, t = 0.16, p = .87. Overall Sickness, b = 0.04, SE = 0.27, t = 0.16, p = .87, and Condition, b = 0.18, SE = 0.19, t = 0.94, p = .35, effects were not significant.
We repeated this regression using representations of aggression to explore whether the moderation reflected a tendency to engage in adaptive health behaviors when more negatively representing illnesses on faces. This model was non-significant, F(3, 123) = 0.35, p = .80.
Hypothesis 3: Mentally Representing Sickness in Faces with COVID-19 Mediated the Positive Relation Between Perceived Illness Threat and Performing Adaptive Health Behaviors
We conducted exploratory mediation analyzes to identify whether representing sickness related to COVID-19 on faces mediated a positive relation between COVID-19-specific threat and engaging in adaptive health behaviors using Model 4 in PROCESS for SPSS (Hayes, 2012) with 5,000 bootstrapped samples for bias-corrected confidence intervals (Figure 2b). Supporting Hypothesis 3, sicker representations of COVID-19 on faces mediated the relation between COVID-19-specific threat and engaging in adaptive health behaviors in response to it, b = 0.05, SE = 0.03, 95% CI [0.003, 0.11]. Whereas COVID-19-specific threat positively related to engaging in adaptive health behaviors, b = 0.27, SE = 0.09, t = 1.89, p = .006, it also had a marginally positive relation to representing sickness related to COVID-19 on faces, b = .06, SE = .04, t = 1.76, p = .08. Representing sickness related to COVID-19 on faces also positively related to engaging in adaptive health behaviors, b = .77, SE = .32, t = 2.35, p = .02. Although all paths were not statistically significant, they were in the predicted directions. Significance across paths is not needed to identify an indirect effect (Hayes, 2012).
Discussion
Mentally representing COVID-19 on faces as sicker positively related to self-reported adaptive health behaviors in response to it. This relation complements the ecological approach to social perception positing that impressions of faces have functional value by guiding behavior to ensure survival (McArthur & Baron, 1983; Slepian et al., 2017; Zebrowitz & Montepare, 2006). It also compliments work showing a positive link between perceiving specific illness threats and performing adaptive health behaviors such as mask wearing (MacIntyre et al., 2021), social distancing (Franzen & Wöhner, 2021), and other behaviors (e.g., avoiding physical contact, coughing into sleeve; (Jørgensen et al., 2021). Just as inferring that actual faces are sick relates to a self-protective hesitance to interact with afflicted individuals (Bressan, 2021; van Leeuwen & Petersen, 2018), mentally representing sickness on faces may also reflect that self-protective motive. Exploratory analyzes supported this possibility. Sicker representations of COVID-19 on faces partially explained the positive relation between perceiving COVID-19 as threatening relative to other illnesses and performing adaptive health behaviors. Notably, these analyzes complement work on the behavioral immune system in that illness threats should elicit self-protective avoidance responses. Mentally representing sickness on faces may reflect one way that illness threats translate into self-protective behaviors that ensure health and survival.
This positive relation emerged when representing COVID-19, but not the common cold, on faces as sicker. This pattern suggests that representations of a specific illness relate to behaviors in response to specific illnesses and has implications for public health messaging. For example, it may be important to link performing adaptive health behaviors to specific illness threats paired with images of afflicted individuals or consequences of illness rather than to more generally suggest that people perform them. Indeed, specific relative to more general messaging is important to elicit positive responses among people evaluating such messages (Carico et al., 2021; Robinson & Eilert, 2018).
Although people evaluated COVID-19 as being more threatening than the common cold, sickness representations of COVID-19 and the common cold did not differ. This pattern might seem surprising but is worth considering in the context of the task itself. Here, illness was manipulated between-participants. One possibility is that people may have a general dimension on which they represent sickness in faces. If so, representations may shift on this dimension based on how many illnesses people are thinking about. For example, if thinking about the common cold at the same time as COVID-19, the COVID-19 representation may appear sicker than if thinking only thinks about one illness. Indeed, the context in which people think about category members shifts representations of group member faces (Hutchings et al., 2021). Alternatively, whereas people may have indicated that COVID-19 was threatening through their explicit evaluations, these evaluations could be more influenced by societal expectations than their attitudes. Given substantial variability in risk perceptions of COVID-19 (Dryhurst et al., 2020) and divergent messaging about it (Niemi et al., 2021), explicit evaluations may not have always matched people's implicitly held perceptions (e.g., Petsko et al., 2020).
Experiment 1a provides initial proof of concept that mentally representing sickness in faces holds functional value in that it relates to engaging in adaptive health behaviors. To validate and assess the generalizability of these findings, we designed Experiment 1b to conceptually replicate Experiment 1a by examining expected adaptive health behaviors in response to a hypothetical illness threat.
Experiment 1b
In Experiment 1b, we sought to further support that representing sickness in faces has functional value. In a random order, people read two vignettes describing a more or a less threatening hypothetical illness. For each illness, people were asked which face from an array of faces selected from the Experiment 1a COVID-19 CLIs depicted how someone with the illness might look. People also evaluated the threat posed by each illness and their expectations of adaptive health behaviors in response to it.
We predicted more expected adaptive health behaviors in response to a more versus a less threatening illness (Hypothesis 1). We also predicted that, consistent with Experiment 1a, people would represent faces depicting a more, relative to a less, threatening illness as sicker (Hypothesis 2). Finally, we predicted that a tendency to expect more adaptive health behaviors in response to the more relative to the less threatening illness would be mediated by representing the face of people with the more relative to the less threatening face as sicker (Hypothesis 3). See the Supplemental Materials for two additional experiments validating Experiment 1a.
Method
Participants
Of interest was replicating the effect of perceived illness threat on adaptive health behaviors through mentally representing sickness identified in Experiment 1a. A power analysis (https://schoemanna.shinyapps.io/mc_power_med/) using correlations of .35 and the default application settings estimated 120 participants for 80% power to detect this indirect effect. Although indirect effects require fewer participants when estimated within-participants (Montoya, 2020), we oversampled 150 adults from MTurk who did not participate in the previous experiments to be conservative. We excluded people as previously described. We excluded 30 people on suspicion that they were “bots,” 12 for failing the attention check, and four for not entering an Mturk code, yielding an analyzed sample of 112 people (Mage = 38.11, SD = 11.57; Myears of education = 15.37, SD = 2.55; 40 female).
Procedure
People read and responded to two scenarios presented in a random order. The scenarios differed by whether a depicted illness was less or more threatening. The scenario for the more [less] illness read, “Imagine that you are reading a newspaper story about a new illness spreading through your state. How many people are infected with the illness is unclear, but the number is assumed to be quickly [slowly] growing. People known to be infected are experiencing life threatening [very mild] symptoms.”
People then rated their perceived illness threat using a scale ranging from 1 (not at all threatening) to 7 (extremely threatening). People then responded to three adaptive health behavior questions in a random order (“Given this scenario, do you think people would [wash their hands/engage in social distancing/engage in self-quarantining] more than usual?”) using a scale ranging from 1 (not at all) to 7 (very much). Responses in the more (Cronbach's α = .79) and less (Cronbach's α = .91) threatening illness conditions were averaged to create two composite adaptive health behavior scores.
Next, people saw 11 face representations in a randomly order (e.g., Figure 3). The representations were CLIs depicting COVID-19 in Experiment 1a that were selected based on their sickness quantified by EAPs from the Phase 2 raters. Two representations were among, respectively, the sickest and the least sick representations. We also selected a representation at the midpoint of the EAP distribution. Finally, we selected eight representations at approximately 10% increments along the EAP distribution. In the presented image array, each representation had a letter paired with it. Text in the more [less] sickness condition read, “Recall that how many people are infected with the illness is unclear, but the number is assumed to be quickly [slowly] growing. People known to be infected are experiencing life threatening [very mild] symptoms. Based on this scenario, choose the letter associated with how you think someone with this illness might look.”
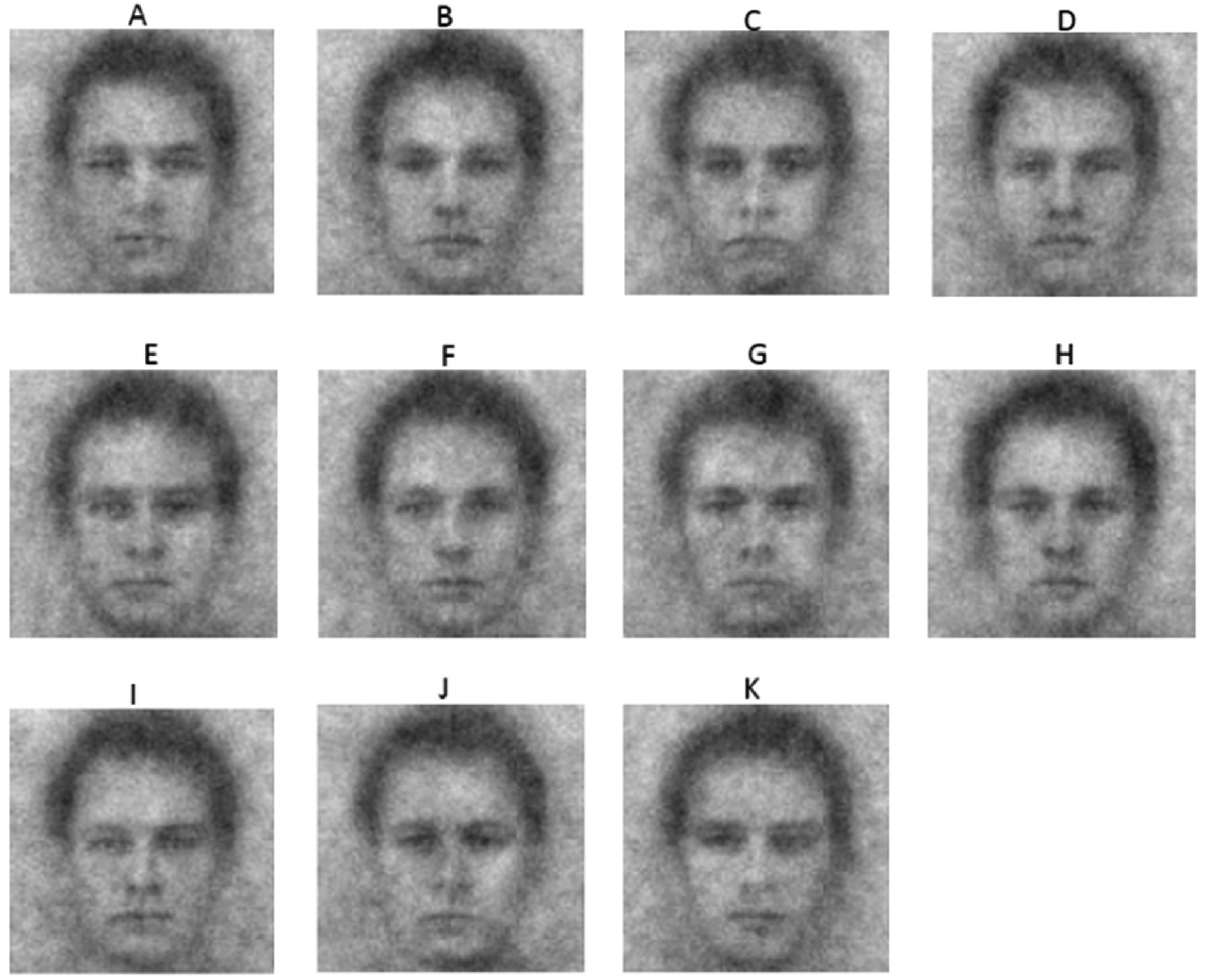
An example randomly ordered array of face representations reflecting sickness to different extents used in Experiment 1b.
People then completed the social (M = 28.88, SD = 5.63) and health (M = 21.00, SD = 7.76) subscales of the DOSPERT and the PI (M = 24.58, SD = 7.91) and GA (M = 35.51, SD = 6.40) subscales of the PVD. in a random order. People then indicated the extent to which they paid attention and followed task instructions using a scale ranging from 1 (not at all) to 7 (completely) (M = 6.49, SD = 0.93) and chose whether the depicted faces had an illness or a new job. Twelve were excluded for incorrectly responding. People then gave demographic information.
Results
Hypothesis 1: More versus Less Threatening Illnesses Elicited More Expected Adaptive Health Behaviors
A paired-samples t-test showed that people perceived the illness to be more threatening after reading the more (M = 5.86, SD = 1.18) relative to the less (M = 4.14, SD = 1.74) threatening scenario, t(109) = 8.49, p < .001, d = 0.81. Supporting Hypothesis 1, a paired-samples t-test showed that people expected more adaptive health behaviors based on the more (M = 5.93, SD = 0.92) relative to less (M = 4.34, SD = 1.65) threatening scenario, t(111) = 8.79, p < .001, d = 0.83.
Hypothesis 2: More versus Less Threatening Illnesses Elicited Sicker Mental Representations of Faces
Supporting Hypothesis 2 and conceptually replicating Experiment 1a, a paired samples t-test showed that people had sicker face representations after reading the more (M = 0.27, SD = 0.60) relative to the less (M = 0.11, SD = 0.58) threatening scenario, t(111) = 2.24, p = .03, d = 0.21.
Hypothesis 3: Mentally Representing Faces as Sicker Mediated a Positive Threat Effect on Expected Adaptive Health Behaviors
We next tested whether sickness representations mediated the threat effect on expected adaptive health behaviors using the MEMORE macro for within-participants designs in SPSS (Montoya & Hayes, 2017). Using 5,000 bootstrapped samples, the 95% CI for the indirect effect of illness threat on expected adaptive health behaviors did not contain zero, 95% CI [0.01, 0.25], supporting mediation and Hypothesis 3.
Discussion
Experiment 1b provided more evidence that mentally representing faces as sicker has functional value. First, people perceived the more relative to the less threatening illness as more threatening. Second, people expected more adaptive health behaviors and had sicker representations of faces in response to the more relative to the less threatening illness. Third, sickness representations mediated the relation between illness threat and expected adaptive health behaviors. A tendency to expect more adaptive heath behaviors in response to more threatening illnesses appears due, at least in part, to a tendency to represent faces with these illnesses as sicker. Experiment 1b thus further supports that face representations have functional value in guiding behavioral expectations.
General Discussion
The current work provides proof of concept that mentally representing more sickness in faces is functionally adaptive in guiding behavior in response to illness threats. In Experiment 1a, we showed that people who had sicker representations of COVID-19 on faces self-reported more adaptive health behaviors in response to the illness. These sicker representations explained, in part, a positive relation between perceptions of COVID-19 as threatening and adaptive health behaviors. We replicated these findings in Experiment 1b when experimentally manipulating illness threat, showing that the patterns shown for a specific illness may reflect broader adaptive responses to illness threats.
The functional value of face impressions is framed by their guiding approach motivations (Slepian et al., 2017). Indeed, a basic reflex among organisms is to approach things that ensure survival (e.g., food) and to avoid things that do not (e.g., predators) (e.g., Brunyé et al., 2013; Rinck & Becker, 2007). It has also been theorized that people have a behavioral immune system evolved to detect and avoid disease-causing organisms (Schaller, 2011; Schaller & Park, 2011) That people report more adaptive health behaviors when representing faces of people with COVID-19 as sicker suggests that face perception and, relatedly, mental representations of faces, may be a novel way to examine the behavioral immune system. By reporting increased social distancing, for example, people avoid stimuli potentially threatening their survival (e.g., people with COVID-19 who may transmit the illness to them). More broadly, the current work suggests a larger role of face perception in preparing to respond to threats. Beyond reactions to the faces people encounter guiding subsequent behaviors, mere thoughts of faces may be enough to guide behaviors.
Whereas Experiment 1a revealed a positive relation between people's sickness representations of COVID-19 and their self-reported behaviors in response to it, Experiment 1b focused on expectations of others’ behaviors in response to hypothetical illness threats. One reason for this change was practical. We reasoned that in the early stages of the pandemic, self-reports of adaptive health behaviors would approach ceiling levels. Implicit in this assumption was that it would be normative to report more adaptive health behaviors in response to illness threats. One theoretical benefit of this change, then, was that it could assess this possibility by gauging what people would expect others to do in response to new illness threats.
Showing that people expect others to perform more adaptive behaviors in response to sicker representations of faces (Experiment 1b) suggests that one function of face representations could be that they ensure survival through setting expectations. Supporting this idea, descriptive norms have been theorized to serve social coordinative functions helping people to manage threat (Gelfand & Harrington, 2015). Indeed, setting descriptive norms that people are not engaging in risky health behavior is important to promote healthy intentions (Rivis & Sheeran, 2003; Trafimow, 1994). Speculatively, sicker representations of faces with an illness may trigger a norm that people are behaving more adaptively in response to it. Future work may test this possibility.
The current work holds exciting possibilities for public health messaging, which has recently begun exploring the impact of faces in various messages (e.g., Morris et al., 2014; Sajjacholapunt & Ball, 2014). For example, when shown images of their face with dark, blotchy, and uneven skin tones and a message warning them about the risks of UV damage, people reported greater intentions to engage in sun protection and took more sunscreen samples relative to when people were shown a regular photo of their face (Morris et al., 2014). The current work suggests that providing images of afflicted faces in public health messaging at the onset of a pandemic, for example, may engage the public in self-protective adaptive behaviors better than pandemic warnings alone.
Providing further implications for public health messaging, past work has shown that people's mental representations of faces can change based on incoming information (Cassidy & Krendl, 2019; Hutchings et al., 2021; Klein et al., 2021). If sickness representations help explain how people expect others to behave, future research may explore how information from public health messaging changes people's representations of sickness in faces to alter their expectations of others’ behaviors and even their own behaviors. People have received widely divergent messaging about COVID-19 based on their selected news sources (Niemi et al., 2021) and, not surprisingly, substantial variability in COVID-19 risk perceptions have emerged worldwide (Dryhurst et al., 2020). One possibility is that underlying these variable risk perceptions are widely diverging sickness representations of COVID-19 based on where people are receiving messaging about the illness. If sickness representations inform adaptive health behaviors, measuring representations may be one way to gauge the potential efficacy of interventions aimed to prevent illness spread before they are widely implemented.
An ecological approach has been an influential account of why facial appearance predicts people's behaviors (Zebrowitz & Collins, 1997). We provide evidence that merely thinking about what people who are sick looks like affects how people behave and expect others to behave in response to illness threats. These findings may thus broaden the scope of how face perception is theorized to affect human behavior and has implications for future work on the behavioral immune system and public health messaging. The mere idea of facial appearance may be enough to affect self-protective behaviors that ensure people's survival.
Supplemental Material
sj-docx-1-evp-10.1177_14747049221109452 - Supplemental material for Mental Representations of Sickness Positively Relate to Adaptive Health Behaviors
Supplemental material, sj-docx-1-evp-10.1177_14747049221109452 for Mental Representations of Sickness Positively Relate to Adaptive Health Behaviors by Jonathan T. Ojeda, Paul J. Silvia and Brittany S. Cassidy in Evolutionary Psychology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent Statement
All participants provided informed consent.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.