
Abstract
This study examined the associations between a high-K fitness strategy and mental health. These associations were tested on a sample of 1400 disaster workers who had exposure to a singular traumatic event and who underwent psychological evaluations. The results showed that high-K was an important negative predictor of psychopathology, accounting for significant variance in PTSD, general psychopathology, functional disability, anger, and sleep disturbances. Implications of the results are discussed.
Keywords
Introduction
Clinical psychology is one area where evolutionary psychology is having a major impact (see Nesse, 2005, for a review). The persistent, cross-cultural, relatively high incidence of mental disorder in the general population suggests that it might have evolutionary significance. The attempts to explain mental disorder from an evolutionary perspective centered on the possible functions of distinct mental conditions (e.g., Crow, 1991, 1997, 1995; Fiske and Haslam, 1997; Mealey, 2000) or on the definitions or taxonomy of mental disorder (Wakefield, 1997; Wakefield and First, 2003). To this end, disorder is seen either as evolutionary dysfunction—failure of natural design, or as naturally selected conditions having present or past fitness advantages (Nesse, 2005).
For instance, very much unlike the prevalent view that it is a brain disorder (Andreasen, 1984; Valenstein, 1998; Wolpert, 1999), evolutionary psychology attempts to explain depression through the functions it may serve, with some authors arguing that low mood is associated with less likelihood of engaging in risk-taking behaviors (Leith and Baumeister, 1996) and others arguing that low levels of depression seem to be “normal” or functional states (McGuire, Troisi, and Raleigh, 1997; Nesse, 1998; Nesse and Williams, 1994).
Likewise, phobias are explained as “prepared” fears gone awry. Prepared fears are fears of things that were a threat to survival during the environment of evolutionary adaptedness. Most phobias are exaggerations of such fears (e.g., spiders, heights, storms, snakes, strangers, blood, unfamiliar places) (Marks, 1987; Marks and Nesse, 1994) and few develop phobias of modern threats to survival (e.g., cars, cigarettes, or alcohol).
Mental illness has negative effects on fitness. Severe depression is associated with reduced fitness (McGuire et al., 1997), as is schizophrenia (Avila, Thaker, and Adami, 2001; Haukka, Suvisaari, and Lönnqvist, 2003). Women with psychotic disorders have been shown to have lower fertility than matched normal comparison subjects (Howard, Kumar, Lesse, and Thornicroft, 2002). Likewise, people suffering from non-affective psychoses have been shown to have significantly fewer children than their unaffected siblings, with the effect more pronounced for male patients versus well brothers (McGrath et al., 1998).
Mental illness of the parents seems not only to affect their resultant fitness translated in sheer number of children but it also compromises offspring quality. Children of parents with severe mental illness are themselves at increased risk of childhood psychiatric disorders (Cowling, Luk, Mileshkin, and Birleson, 2004) and the risk of offspring with impaired intellectual handicap is significantly increased for schizophrenia and affective psychoses mothers compared with controls (Jablensky et al., 1998).
Purpose of the study
The purpose of this study was to examine the associations between a high-K reproductive strategy and mental illness. According to Life History Theory (e.g., Bogaert and Rushton, 1989; Figueredo et al., 2006; Mac Arthur and Wilson, 1967; Pianka, 1970; Wilson, 1975), for any organism, its available resources are finite, which translates into trade-offs in their allocation for solving various fitness-relevant tasks. For instance, the resources allocated to grow a bigger body cannot be used to pursue mates, and vice versa. The extremes of these fundamental dimensions of reproduction are traditionally termed the r/K theory, with r representing the maximum egg output and no investment and K representing the opposite. Rushton (1985, 1990) extrapolated the r/K continuum of life history strategies to human differences from Wilson's (1975) analysis of cross-species differences in reproductive strategies. In humans, since they appear to be highly K-selected, these dimensions are often referred to as “differential K.”
A high-K strategy in humans is theorized as a specific and cohesive fitness strategy, in which the individual invests in somatic and parental effort to produce a fewer number of “fitter” and more competitive offspring. Measures of high-K strategy have been shown to correlate with offspring quality and with resultant fitness (Giosan, 2006). Traits associated with a high-K strategy are long-term thinking and planning, commitment to long-term relationships, extensive parental investment, existence of social support structures, adherence to social rules (e.g., altruism and cooperation) and careful consideration of risks (Figueredo et al., 2006; Giosan, 2006).
Because a high-K strategy is associated with greater somatic effort as opposed to reproductive effort, “slow” strategists should manifest the benefits of this in terms of better mental and physical health. Likewise, low-K (“fast”) strategists should exhibit increased psychopathology and increased physical illness, because these individuals do not allocate sufficient somatic effort to prevent such problems. Indeed, in one of the first studies on this topic, high-K strategy was shown to be an important negative predictor of depressive symptomatology, accounting for 20% in the variance in the Beck Depression Inventory scores, after controlling for risk factors in depression such as demographics, prior trauma, prior psychopathology, or recent negative life events (Giosan, 2007).
Expanding on these findings, the principal aim of this study was to explore the associations between a high-K fitness strategy and a larger array of mental conditions, including PTSD and related psychopathology, sleep disturbances, anger, and functional disability. The overarching hypothesis tested in this study was that a successful high-K strategy is a negative predictor of mental illness.
Materials and Methods
Participants were a sample of n = 1400 disaster workers who were deployed to the World Trade Center in the immediate aftermath of the 9/11 attack. They were administered a full battery of self-reports and a subsample of 436 (31%) respondents were also administered a structured clinical interview conducted by doctoral level clinicians.
Measures
Clinician-Administered Measures
Clinician-Administered PTSD Scale. The Clinician-Administered PTSD scale (CAPS; Blake et al., 1995) is a structured interview for posttraumatic stress disorder (PTSD) that yields both a dichotomous (present/absent) diagnosis of PTSD and a continuous measure of its severity. The CAPS assesses the frequency and intensity of each PTSD symptom on separate 5-point rating scales (0 – 4). Frequency and intensity may be summed for each item to yield a nine-point (0 – 8) severity rating, and these ratings may be summed across items to yield a severity score for the full PTSD syndrome.
The Structured Clinical Interview for the DSM-IV (SCID; First, Spitzer, Williams, and Gibbon, 1997) is a semi-structured clinical interview designed to determine DSM-IV diagnoses, and its psychometric properties have been well-established (First et al., 1997). The SCID and selected modules for the DSM-IV, which included past major depression, past panic disorder, and past generalized anxiety disorder, were administered and collapsed into one variable (past psychopathology present or absent).
The WTC Exposure Questionnaire was developed by a panel of trauma experts to assess occupational exposure through performance of disaster work as well as personal exposure to the WTC attacks (e.g., loss of loved ones). The development of the exposure index in this study began with variables that were shown in the disaster literature to predict PTSD and revised with questions that emerged as unique to working at the WTC site. For the purposes of this study, a total exposure score was calculated by summing up the items that the participants reported as having experienced.
Self-reports
High-K Strategy Scale (HKSS; Giosan, 2006). HKSS is a 26-item scale tapping into various indicators of high-K strategy. These indicators include upward mobility (high-K strategists seek opportunities to gain resources for greater investment in their offspring), health and attractiveness (high-K strategists invest in somatic, rather than reproductive, effort, therefore they should enjoy better health and be, consequently, more attractive), social capital, or risk consideration. As predicted, this construct correlated significantly with perceived offspring quality (through the fact that high-K strategists invest their time and resources in parental effort). It also correlated negatively with number of previous marriages (because high-K strategists are committed to long-term relationships). Also, it correlated with objective measures of health, educational level and social support (because high-K strategists invest in somatic, educational opportunities and social capital for gaining better access to resources for their offspring). As expected, this construct showed a weak but significant correlation with actual number of children (the net result of a successful high-K strategy is fitness, but characterized through smaller number of children). Lastly, since a high-K strategy is theorized as a cohesive reproductive strategy, the indicators that make it up were predicted to have high internal consistency. Indeed, HKSS's Cronbach's α was .92 (Giosan, 2006). The items of this scale are summed up to yield a total score.
The PTSD Checklist (PCL; Weathers, Herman, Huska, and Keane, 1993) is a DSM-correspondent, 17-item self-report measure of PTSD. Using a five-point rating scale (1 = “not at all,” 5 = “extremely”), respondents indicate how much they were bothered in the past month by each of the DSM-IV PTSD symptoms. The PCL is psychometrically sound and has been used in nearly two hundred studies across a variety of trauma populations (Weathers et al., 1993). The PCL yields both a continuous severity score and a PTSD diagnosis.
Brief Symptom Inventory. The Brief Symptom Inventory (BSI; Derogatis, 1993) is a 53-item abbreviated version of the Symptom Checklist 90-Revised (Derogatis and Spencer, 1982) that assesses a broad range of symptoms of psychopathology. The BSI yields scores for nine symptom dimensions as well as global indices, based on the calculation of mean item responses. In the present study we used the Global Severity Index (GSI) from the BSI, where higher scores indicate more severe overall psychopathology.
The State Trait Anger Expression Inventory-2 (STAXI-2). The STAXI-2, a revised 57-item version of the STAXI (Spielberger, 1988), provides concise measures of the experience, expression, and control of anger. For the purposes of this study, the 15-item STAXI State Anger (S-Ang) scale was used to assess total state anger. The Cronbach's α for this scale in this study was 0.93.
Sheehan Disability Scale. The Sheehan Disability Scale (SDS; Sheehan, 1983) is a 10-point visual analogue scale that assesses disability across three domains: work, social life, and family life. The three items may be summed into a single dimensional measure of global functional impairment that ranges from 0 (unimpaired) to 30 (highly impaired), which was used in this study. This scale has been widely used in psychopharmacology randomized controlled trials and has strong internal consistency (Cronbach's α = 0.89 for the three-item scale).
The Sleep Index is a modified version of the Pittsburg Sleep Quality Index (PSQI) (Buysse, Reynolds, Monk, Berman, and Kupfer, 1989), and was used to assess sleep disturbances and their frequency. PSQI has been widely used to measure sleep difficulty in different populations (Chesson et al., 2000) and has good reliability and validity (Buysse et al., 1989; Doi et al., 2000). The Cronbach's α of the sleep index in this study was acceptable (Cronbach's α = 0.77).
Statistical approach
Examining the independent effects of high-K on measures of psychopathology was the main goal of the study. To this end, correlations between high-K, demographics (age, race, education, marital status), past psychopathology (dichotomized: “yes” for presence of past psychopathology, “no” for absence), prior trauma, self-reported (PCL) and clinician-administered (CAPS) PTSD severity score, general psychopathology (GSI), anger (STAXI-2), disability (Sheehan), sleep disturbance (total Sleep Index score) and Exposure to 9/11 total score, were first performed.
Simultaneous regressions of the outcomes examined (PCL, CAPS, GSI, STAXI-2, Sheehan and total Sleep Index score) on the variables that were significantly correlated with them were then performed to identify the variables that account for significant variance (tolerances greater than .8) in these outcomes. To examine the unique contribution of high-K, variables that showed tolerances greater than .8 were then controlled for in regressions of the outcomes on high-K.
Results
Demographics
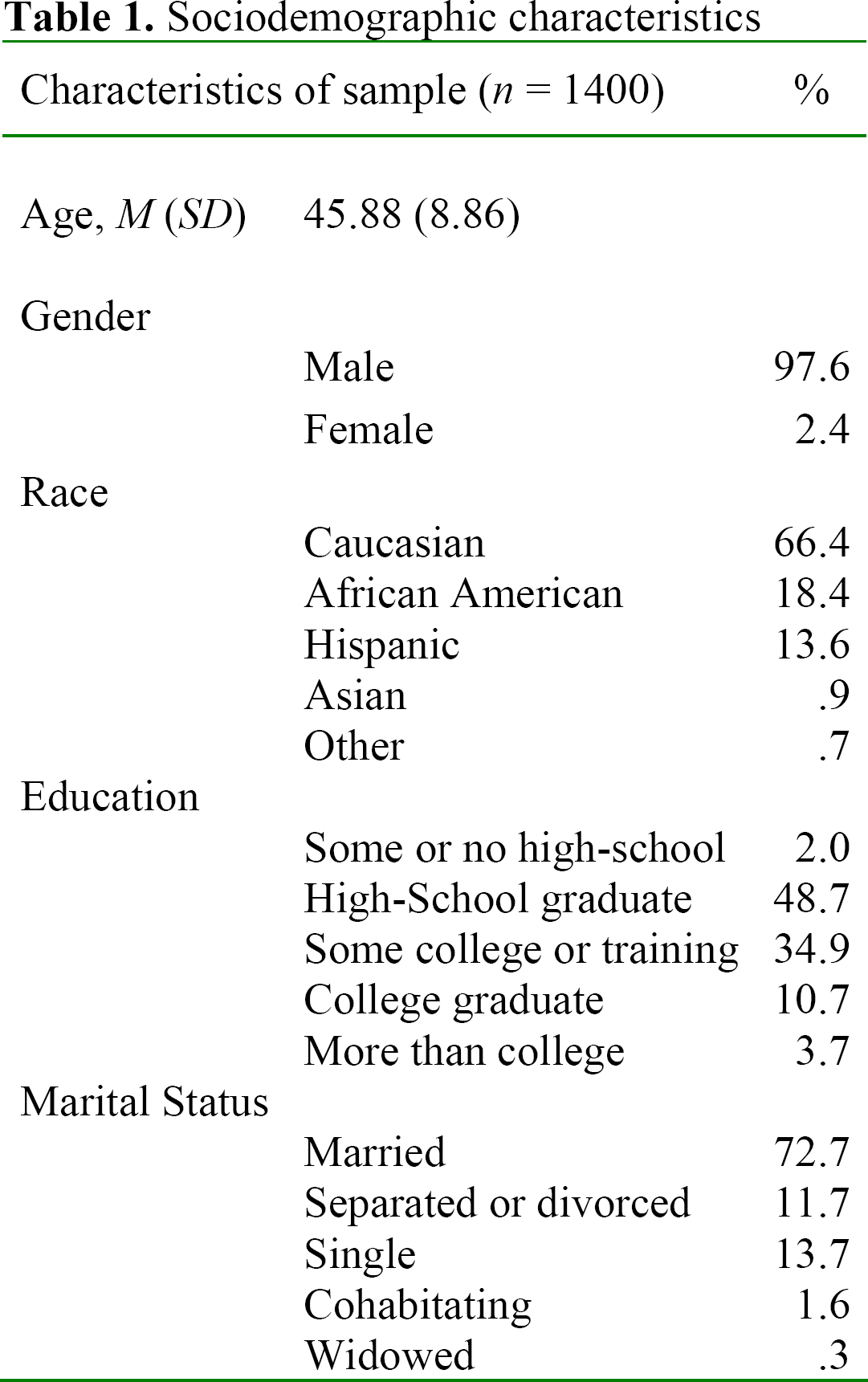
Table 1 depicts the demographic characteristics of the sample (n = 1400). Overall, the sample consisted of primarily middle-aged, white, married men with the majority having at least a high-school education.
Sociodemographic characteristics
High-K and psychopathology
The correlation table for all the measures is presented in Table 2. Significant correlations between high-K and age, marital status, prior trauma, Clinician-Administered PTSD Scale total severity score, PTSD checklist total severity score, Global Severity Index, State-Trait Anger Expression Inventory score and Sheehan Disability Scale score, were found (all ps ≤ .01).
Correlation matrix

p < .01
p < .05
Legend: Pastpsych = prior psychopathology
CAPS = Clinician-Administered PTSD Scale total severity score
PCL = The PTSD Checklist severity score
Sleep = Sleep Disturbances score
Sheehan = Sheehan Disability Scale total score
Staxi = The State Trait Anger Expression Inventory score
GSI = Global Severity Index, where higher scores indicate more severe psychopathology.
Exposure = The WTC Exposure score
Regressions of PTSD Checklist (PCL) scores on high-K, after controlling for marital status, exposure and past psychopathology—variables that had tolerances greater than .8 in simultaneous regressions of PCL on variables that correlated significantly with it—showed that high-K accounts for an important 10% of the variance in the PCL (negative relationship) (Table 3).
Regressions of PCL and CAPS on high-K

p < .01
p < .05
Regressions of Clinician-Administered PSTD Scale (CAPS) severity scores on high-K, after controlling for past psychology, prior trauma, and exposure to 9/11 score, showed that high-K accounts for 5% in the variance (negative relationship) (Table 3).
Regressions of Sheehan total disability score on high-K, after controlling for age, race, marital status and prior trauma, showed that high-K accounts for 7% of the variance (negative relationship) (Table 4).
Regressions of Sleep disturbance and Sheehan on high-K

p < .01
p < .05
Regressions of Sleep disturbance on high-K, after controlling for total exposure score, prior trauma and past psychology showed that high-K accounts for 7% of the variance (negative relationship) in the sleep index (Table 4).
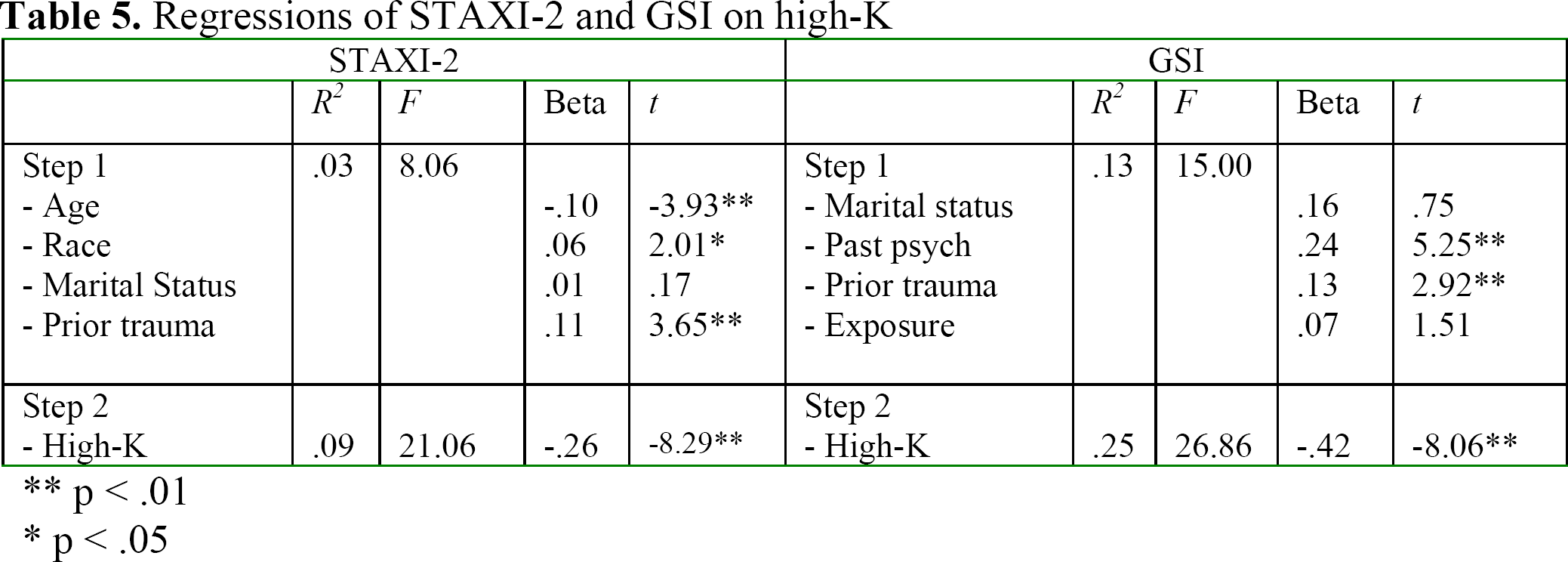
Regressions of the Global Severity Index (GSI) on high-K, after controlling for total exposure score, marital status, past psychopathology and prior trauma, showed that high-K is a negative predictor of general psychopathology, accounting for on important 12% in the variance (Table 5).
Regressions of STAXI-2 and GSI on high-K
p < .01
p < .05
Regressions of State Trait Anger Expression Inventory (STAXI-2) scores on high-K, after controlling for age, race, marital status and prior trauma, showed that high-K is an independent negative predictor of anger, accounting for 6% in the variance (Table 5).
Discussion
The present study examined the associations between a high-K fitness strategy and psychopathology, assessed both through clinician-administered measures and self-reports. It was found that people who had higher scores on HKSS were also those who reported lower levels of psychopathology, and that high-K emerged as a significant predictor of psychopathology. This pattern was not singular, but was found across a range of psychopathologies, including PTSD, sleep disturbances, functional disability, anger, or overall psychopathology.
These findings, along with previous findings that found high-K to be strongly inversely related to depressive symptomatology (Giosan, 2007), suggest that high-K appears to be an important buffer of psychopathology. In our study, high-K accounted for variance ranging from 5% to 12% in the different psychopathologies assessed, the greatest variance being found in the General Symptom Inventory total score.
The strong negative association between high-K and PTSD seems to speak against an evolutionary view that argues for the adaptive value of PTSD symptoms (e.g., Nesse, 2005), at least for this particular reproductive strategy. Our results show that lower scores on high-K, which are associated with reduced fitness (Giosan, 2006), are also associated with increased severity in PTSD symptoms. Since the findings documented in this study show that this reproductive strategy correlates negatively with the severity of PTSD, this result may offer indirect support to the view that holds that PTSD is the expression of an overlearned survival response in vulnerable individuals (Silove, 1998), which, when it develops, may have significant negative effects on those individuals' fitness.
Despite these important findings, several caveats are in order: First, as in any correlational study, the direction of causality cannot be established with certainty. One can argue that people score highly on the high-K precisely because they enjoyed better mental health in the first place and their resources could thus be channeled to the indicators that make up the high-K factor. This is a legitimate claim and testing the direction of causality is not a small feat. Further longitudinal studies examining the associations between changes in high-K and changes in psychopathology are needed to address such questions. Second, the logistics of the data collection biased the sample toward white males, which may raise questions about the generalizability of these results to other populations. Further studies on different populations need to be done to address this aspect. Third, one might argue that the relationships found in this study might be the result of a broad association between general mate quality/value and psychopathology. The design of the study did not have mate quality in the list of the variables examined therefore it could not address this question. Further research aimed at clarifying these complex associations should be done.
Despite these limitations, the present study, to our knowledge the first to link high-K and psychopathology, offers evidence that this specific life history strategy is strongly negatively linked to, and a negative predictor of, a broad range of psychopathologies.
Directions for further research
The ramifications of the findings in the present study are multiple. One avenue of research is to examine the effects of interventions on high-K on psychopathology. Indeed, since many of the indicators making up the high-K independent criterion of fitness are modifiable (e.g., appearance, social capital, personal safety, status) the question of whether active interventions on such indicators would translate into decreased psychopathology gains practical and clinical significance. A positive answer to this empirical question would likely aid therapists in their quests of finding more effective interventions.
Also, the high-K measure used in this study is understood as a unidimensional construct tapping into “slow” life history strategy, with high scores representing successful resolution of the challenges associated with a high-K strategy, and low scores representing a faulty high-K fitness strategy and not necessarily “fast” life history strategy. It would be important and complementary to this work to examine whether faulty fitness strategies in general—being they faulty high-K or faulty low-K—are associated with mental illness.