
Abstract
Diabetic foot ulcers (DFUs) are common and disabling, giving rise to significant morbidity and mortality as well as worldwide socioeconomic problems. Despite treatment, DFUs readily become chronic wounds and may lead to major lower limb amputations. The pathogenesis of DFUs is complex and the main aetiologies are peripheral neuropathy, ischaemia from peripheral arterial disease and biomechanical abnormalities. Microvascular disease is also a significant problem for people with diabetes and contributes to foot ulceration. Successful management of DFUs consists of debridement, infection control, the use of offloading appliances and revascularisation where necessary. Foot ulcers are usually associated with infection and inflammation which lead to surrounding oedema of the foot. Standard offloading devices such as total contact casts and removable cast walkers do not actively reduce foot oedema. There is promising evidence that active oedema reduction by intermittent pneumatic compression in the diabetic foot improves ulcer healing. The objective of this article is to review the association of foot oedema and DFUs, including the role of appliances which reduce oedema. The information presented is vital to those involved in the management of DFUs.
Abbreviations:
DFU diabetic foot ulcer
TCC total contact cast
Introduction
The prevalence of diabetes worldwide was estimated at 131 million in 2000 and is forecast to increase to 366 million by 2030. 1 In the UK, 2.8 million people were registered as having diabetes in 2010. 2 Patients with diabetes are at increased risk of developing neuropathy, peripheral arterial disease and infections and are therefore at high risk of developing foot pathologies including ulceration. The results of cross-sectional community surveys in the UK showed that 7.4% of patients with diabetes had a history of active or previous foot ulcers. 3 They have up to 25% lifetime risk of developing foot ulcers, 4 which have a high risk of deteriorating and ultimately leading to major lower limb amputation. DFUs precede 84% of amputations, and nearly one in six patients with DFUs eventually require an amputation. 5,6 The incidence of major lower limb amputation in people with diabetes is between 0.5 and 5.0 per 1,000 people and survival after a major lower limb amputation is poor, with a perioperative mortality of 10–15% in the UK. 3
Evaluation of DFUs includes vascular and neurological examinations as well as accurate wound assessment. Successful management of DFUs consists of offloading with appropriate devices, management of infection, wound care including debridement and revascularisation when indicated. DFUs are usually associated with infection and inflammation which lead to oedema of the foot. Currently, most appliances use function only to alleviate mechanical load on ulcers and do not actively address the associated oedema, which can potentially be detrimental to ulcer healing. The objective of this article is to review the association of foot oedema and DFUs, including the role of appliances which reduce oedema.
Aetiology and classification of diabetic foot ulcers
The pathogenesis of DFUs is complex and has multiple contributing factors. The major underlying aetiologies of diabetic foot ulceration are peripheral neuropathy, ischaemia, foot deformity and infections 7 caused by the production of advanced glycation end products secondary to hyperglycaemia. The incidence of neuroischaemic ulcers is 52.3%, neuropathic ulcers 36% and ischaemic ulcers 11.7%. 8 Neuropathy includes sensory, motor and autonomic components. Deficient protective sensation leads to ulceration on high pressure areas; motor neuropathy results in biomechanical abnormalities and autonomic neuropathy causes decreased sweating and dry skin which is more prone to hyperkeratosis and ulceration. Ischaemia is caused by peripheral arterial disease, resulting in decreased blood supply and tissue perfusion, which significantly compromise ulcer healing.
Peripheral arterial disease in patients with diabetes tends to be multifocal and commonly affects the infra-popliteal vessels. Furthermore, disease progression is usually accelerated, 9 and together with microvascular disease, results in poor outcomes. Endothelial dysfunction appears to be the main cause of both the macrovascular and microvascular disease and mechanisms which contribute to this include persistent hyperglycaemia, increased advanced glycation end-products, oxidative stress, endothelial inflammation and reduced nitric oxide activity. 10,11 In addition, an increase in thromboxane A2, a vasoconstrictor and platelet aggregation agonist, has been associated with hyperglycaemia in diabetes, leading to an increased risk of plasma hypercoagulability. 12
Impaired wound healing has also been implicated in patients with diabetes. The normal wound healing process entails a complex interplay between connective tissue formation, cellular activity, and growth factor activation. All three of these physiologic processes are altered in the diabetic state and contribute to the poor healing of DFUs. 13 Instead of progressing through the normal stages of wound healing, it is now clear that diabetic ulcers remain in the inflammatory phase of the wound healing process. During this delay, there is a cessation of epidermal growth and migration over the wound surface. 14,15
Analysis of fluid from these chronic wounds has demonstrated elevated levels of matrix metalloproteinases directly resulting in increased proteolytic activity and inactivation of the growth factors that are necessary for proper wound healing. Additionally, these chronic wounds have been found to exhibit deficiencies in growth factors and cytokines along with elevated levels of inhibitory proteases. 13 Therefore, impaired wound healing is manifested in aberrant protein synthesis, cellular activity and growth factor secretion.
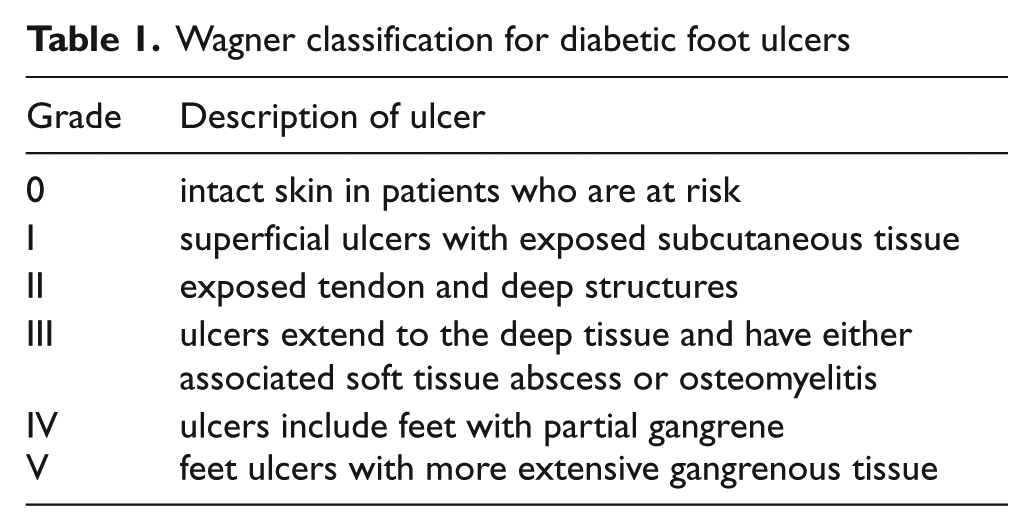
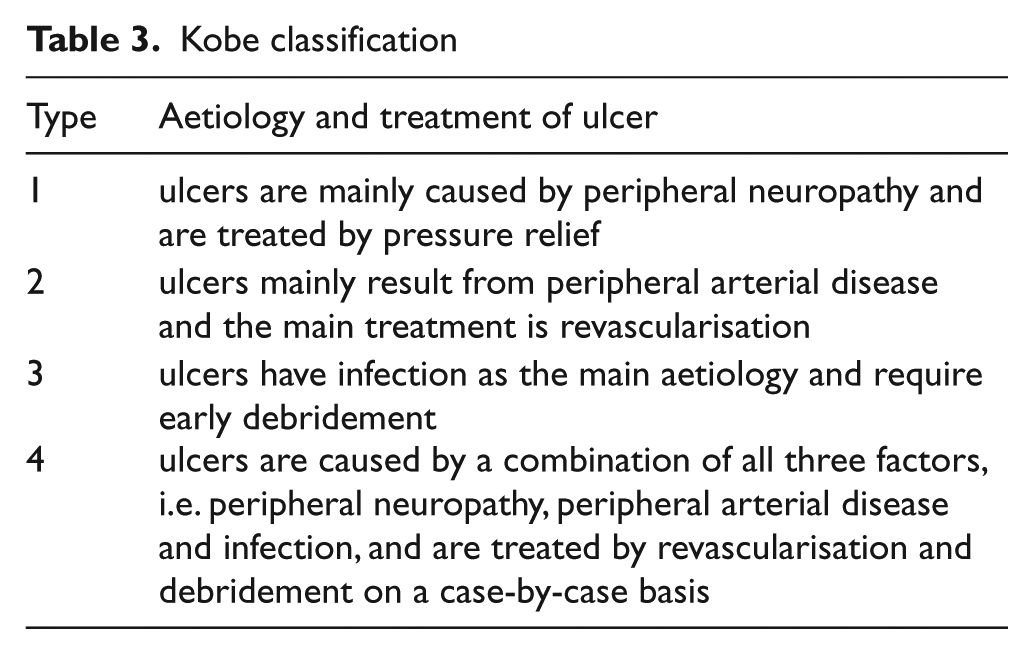
Classification systems have been developed to grade the severity of diabetic foot ulcers, provide prognosis on healing and aid in the formulation of treatment plans. The widely used Wagner classification for diabetic foot ulcers (table 1) assesses ulcer depth and the presence of osteomyelitis or gangrene. 16 The University of Texas system assesses ulcer depth, the presence of wound infection, and the presence of clinical signs of lower-extremity ischaemia. 17 This system uses a matrix of grade on the horizontal axis and stage on the vertical axis (table 2). A prospective study of 194 patients comparing the two diabetic foot ulcer classifications concluded that the University of Texas classification is a better predictor of outcome. 18 Increasing stage, regardless of grade, is associated with increased risk of amputation and prolonged ulcer healing time. Recently, the Kobe classification has been proposed which focuses on the main aetiology of ulcers and proposes appropriate treatment (table 3) 19 . These classification systems illustrate the complexity and multi-aetiological nature of diabetic foot ulcers. However, none of the many grading systems take into account any associated oedema of the foot, illustrating that this remains a poorly understood aspect of DFUs.
Wagner classification for diabetic foot ulcers
The University of Texas system
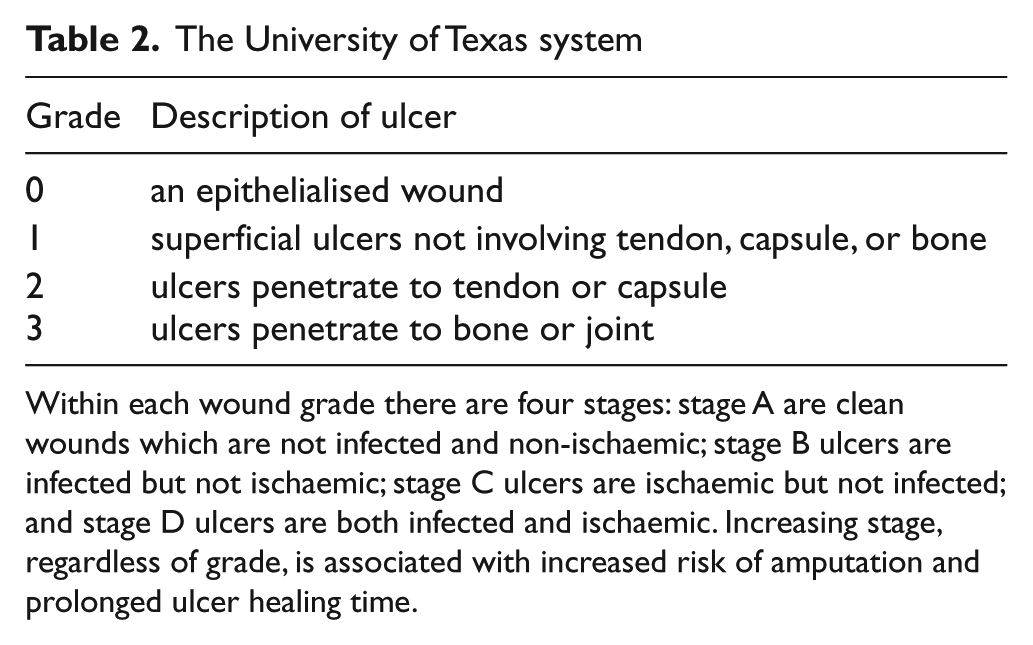
Within each wound grade there are four stages: stage A are clean wounds which are not infected and non-ischaemic; stage B ulcers are infected but not ischaemic; stage C ulcers are ischaemic but not infected; and stage D ulcers are both infected and ischaemic. Increasing stage, regardless of grade, is associated with increased risk of amputation and prolonged ulcer healing time.
Kobe classification
Diabetic foot ulcers and oedema
The involvement of the microcirculation in diabetic microangiopathy contributes to foot ulceration. In addition, diabetic microangiopathy, characterised by an increase in skin flux at rest, decreased veno-arteriolar response, and increased capillary permeability results in oedema, reduced skin partial oxygen tension and increased carbon dioxide tension. 20 In this condition, capillary exchange is altered and nutritional alterations eventually lead to skin lesions and ulcers.
The postural regulation of blood flow is impaired in patients with diabetic neuropathy. This disturbance is compatible with a loss of sympathetic vascular tone and arteriovenous shunting. 21,22 In particular, the capability of effective precapillary vasoconstriction on standing is reduced. This exposes the capillary bed to a high hydrostatic load, resulting in hyperperfusion and increased shear force in the microcirculation on dependency which in turn leads to thickening of the capillary basement membrane and oedema of the feet and lower legs. 23
In a prospective study of 314 patients with DFUs, the presence of oedema indicated a poorer prognosis 24 : peripheral oedema was more common in patients who required amputation (58%) or died (55%) than in patients with primary healing (26%, p<0.001). A tentative predisposing factor was identified in 95% of the patients, the most common factors being neuropathy, congestive heart failure, and previous deep venous thrombosis.
The principles of management of DFUs include proper assessment and treatment of different lesions of the foot, including infection control, debridement, wound management, revascularisation, other surgery, metabolic control and off-loading. Compression therapy may be used to reduce lower limb oedema to aid ulcer healing. Layered compression therapy and, more recently, diabetic socks with mild compression have been found to be safe and effective in diabetic patients with adequate or mildly reduced arterial blood supply. 25,26 The following sections further discuss the two methods associated with oedema reduction, offloading and compression therapy, in the management of DFUs.
Offloading devices in the management of DFUs
Appropriate offloading is a key component in the management of diabetic foot disease. The use of TCCs has been reported to result in excellent ulcer healing rates and associated with faster healing compared to other removable devices in a randomised controlled trial. 27 The TCC is considered to be the gold standard offloading device for plantar neuropathic ulcers, yet it is still not widely used in clinical practice. 28 It works by transmitting load from the forefoot to the heel and directly to the leg via the cast walls. 29 Its main disadvantage is that its application is time-consuming and often associated with a learning curve. Most centres do not have a physician or cast technician available with adequate training or experience to safely apply TCCs. Moreover, TCCs do not allow assessment of the foot or wound on a daily basis and are therefore often contraindicated in cases of soft tissue infections or osteomyelitis.
Iatrogenic ulceration where ulceration occurs whilst within the cast due to pressure or friction from cast materials is a concern, but the risks are reduced by proper casting techniques. 30,31 Other patient complaints include impaired activities of daily living, such as difficulty sleeping comfortably, and bathing difficulties while trying to avoid getting the cast wet, which reduce patient concordance. Certain designs of TCCs may also exacerbate postural instability. 32
Removable cast walkers are cast-like devices that are removable to allow inspection of the wound and application of topical therapies. Further, removable cast walkers can be easily converted into instant total contact casts by wrapping the removable cast walker with cohesive bandage or plaster of Paris. 33 Wound healing efficacy of instant TCCs has been demonstrated to be comparable to TCCs in several randomized controlled trials. 34,35
Although these standard offloading devices are believed to reduce oedema by enabling patients to remain relatively mobile, there has been no objective published data confirming this. Instead, immobilisation of the ankle with reduced function of the calf muscles which act as a venous pump, can theoretically impair venous return and potentially result in increased foot oedema.
Reducing oedema in the management of DFUs
In managing DFUs, foot elevation has generally been recommended to reduce oedema and prevent other sequential problems. However, foot elevation may decrease tissue oxygenation of the foot relative to the dependent position, which allows an increase in blood flow within the arterial system. The transcutaneous partial oxygen tension has been shown to be reduced on foot elevation of patients with DFUs. 36
In diabetic patients with lower limb oedema, mild compression therapy (18–25 mmHg) applied via socks or hosiery during the day was found to decrease calf and foot swelling by reducing oedema, without compromising vascularity in a study of 18 patients who have normal arterial circulation. 26 In the treatment of DFUs, compression therapy has been used effectively and safely to reduce oedema in a diabetic population with adequate arterial circulation whilst reduced compression was beneficial in patients with arterial compromise in a prospective clinical case review involving 44 patients. 25 Patients with adequate arterial circulation were treated with a four-layer compression bandage system while the highly elastic third layer was excluded in the patients who had compromised peripheral arterial circulation. Healing occurred in 81% of patients with adequate peripheral arterial circulation and 67% of patients with compromised peripheral arterial circulation. There was no acute progression of lower limb ischaemia in the study. However, patients with diabetes have a high risk of developing peripheral arterial disease and many clinicians may be reluctant to use compression therapy.
The use of intermittent pneumatic compression by the A-V Impulse System has been shown to be safe and effective in other clinical areas such as the reduction of posttraumatic swelling and postoperative swelling following ankle and femoral neck fractures where the rate of proximal deep vein thrombosis was also reduced. 37 -39 The A-V Impulse System was developed to mimic the natural physiological processes which maintain blood flow and has been shown to improve venous return and arterial blood flow in the extremities. 40,41
The proposed mechanism of action is that intermittent pneumatic compression leads to improved emptying of the lower extremity veins and lowered venous pressure which in turn results in an increase in arterio-venous pressure gradient and an increase in lower extremity arterial blood flow. 42 -44 In a cohort study of 40 lower limbs of 30 subjects, the application of intermittent pneumatic compression to calf and foot greatly enhanced popliteal artery blood flow. It was suggested that the flow increase is due to a dramatic drop in the peripheral vascular resistance as the peak systolic and end diastolic flow velocities increase and the reverse-flow component diminishes. 45 A direct reduction in peripheral resistance has also been postulated with intermittent pneumatic compression via release of nitric oxide, secondary to shear stress increase in the venous radicles. The action of diffused nitric oxide on adjacent arteriolar resistance vessels causes them to dilate transiently with concurrent flow enhancement. 46
As discussed previously, there is evidence that in patients with diabetes, peripheral arterial disease is more aggressive, difficult to manage and associated with poorer outcomes. 47 A systematic review demonstrated that an intermittent pneumatic compression programme appeared promising and may be used in patients with severe peripheral arterial disease who were not candidates for surgical or endovascular revascularization. Claudication distance, rest pain, and rates of limb salvage were improved across the spectrum of trials performed, associated with increased arterial blood flow, peak systolic velocity, end diastolic velocity and pulse volume. 48 A small randomized study with 12 months follow-up (n=30) in patients with stable intermittent claudication concluded that walking distance improved in these patients. 49 In addition to improved walking distance in stable claudicants, a prospective randomised controlled study with 1 year follow-up found an improvement in the ankle brachial pressure index, which is a measurement of peripheral haemodynamics, and improvement in quality of life. 50
A more recent study in patients with chronic lower limb ischaemia found a significant improvement in wound healing and limb salvage rates in the treated group. The intermittent pneumatic compression was delivered at an inflation pressure of 85–95mmHg, applied for 2 seconds with rapid rise (0.2 seconds), three cycles per minute, for three 2-hourly sessions per day. 51
In DFUs, a double blind randomised controlled trial with 12 weeks follow-up also showed that oedema reduction by a pneumatic foot compression system increased the proportion of wound healing. 52 Fifty-nine patients with diabetes were allocated to receive a functioning pulsatile pneumatic foot compression system achieved by way of a pump and wrap system following debridement of infected foot ulcers. The system included a bladder containing a foot wrap and a pump that intermittently fired bursts of air through tubing to the wrap, thereby emptying the foot veins. This group was compared against a placebo group of 56 patients who received a non-functioning device. Patients were asked to use the device 8 hours a day, in addition to weekly standard wound care that included wound debridement and offloading. Patients treated with active foot compression had a 75% healing rate compared with 51% in the placebo group (p<0.02; odds ratio, 2.9; 95% confidence interval, 1.2–6.8) and a greater degree of oedema reduction as shown by mean foot circumference measurements (23.8 vs. 25.7 cm, p<0.001) than those in the placebo group. However, a substantial number of patients in both groups found that it was inconvenient to have the device on and elevate their legs for 8 hours a day.
It would therefore appear that an intermittent pneumatic compression device with offloading property will have a potential combined effect of oedema reduction and offloading of high pressure areas, both of which are likely to improve diabetic foot ulcer healing. Randomised clinical trials, looking at a range of DFUs, are warranted to assess these effects on ulcer healing.
Conclusion
Treatment of oedema may further improve the outcomes of DFUs, over and above standard therapy. A device which is comfortable to increase concordance, able to provide intermittent pneumatic compression to actively reduce oedema, and allow offloading can be useful for this purpose but further investigation will be required to provide a strong level of evidence.
Key messages
Diabetic foot ulcers are commonly associated with oedema
Oedema reduction may improve healing of these ulcers
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest Statement
J.T. and R.D.L. provide clinical advice to the Diabetic Boot Company Ltd.