
Abstract
Parents with learning disabilities in England are disproportionately subject to child protection intervention and child removal, yet post-removal support remains uneven and poorly understood. This study examined what support adult and children’s social care and allied agencies provided to these parents, and how professional relationships shaped both access to services and trust. The interviews with nine parents recruited via advocacy and voluntary organisations were open and participant led. Analysis proceeded iteratively from whole-case readings to cross-case thematic comparison and was informed by discussion with an expert-by-experience group of parents with a learning disability. Parents described profound, enduring grief following child removal, often compounded by poor health, bereavement, domestic abuse, and weak informal networks. Views on their experiences of social workers were polarised: fragmented, judgemental communication and staff turnover entrenched mistrust, whereas one consistent, respectful practitioner could transform engagement. Advocacy and specialist learning-disability input helped parents understand processes, manage contact, and, in some cases, retain care of younger children. However, access and provision were patchy and frequently contingent on diagnosis of a learning disability, referral, or geography. Adult social care assessments of a disability and thresholds were variable, and reasonable adjustments were inconsistently applied. Overall, post-removal support for parents with learning disabilities emerged as fragile, inconsistent, and inequitably distributed. Early, proactive involvement (including during pregnancy), accessible communication and assessment, and sustained investment in advocacy are essential. Policy and practice should recognise child removal as a chronic bereavement requiring long-term, relational, and coordinated support across adult and children’s services.
Introduction
Just under one million adults in England have a learning disability (Public Health England, 2016). Many people with a learning disability want to have children (Conder et al., 2011), but when they become parents they feel under pressure to prove themselves (Malouf et al., 2017; Theodore et al., 2018). Parents with a learning disability are also more likely to go through care proceedings and have their children removed from their care (Booth and Booth 2004; Llewellyn and Hindmarsh, 2015; Masson et al., 2008). This has been linked with a complex mix of factors, including co-existing educational and socio-economic disadvantage, abusive partners and professionals’ negative assumptions of parents’ ability (Collings et al., 2017; McConnell et al., 2011; Ward and Tarleton, 2007).
Despite an increasingly robust evidence base demonstrating that there are parents with a learning disability that can parent successfully when appropriate, tailored support is in place, practice remains inconsistent. MacIntyre et al. (2019) argue that this inconsistency is not simply a matter of gaps in service provision but reflects deeper conceptual and professional tensions. Drawing on theories of vulnerability and an ethics of care, they suggest that parents with a learning disability are often constructed as inherently ‘vulnerable’, a framing that can lower expectations of parenting capacity and legitimise intrusive or risk-averse intervention. This double-edged sword of vulnerability may simultaneously enable access to support while reinforcing assumptions of incapacity, contributing to persistent barriers in assessment, support, and inter-agency working.
There is a lack of data on the exact number of children removed from parents who have a learning disability, reflecting both an absence of a clear definition of learning disability and guidance on how to identify and record people with a learning disability (Burch et al., 2019). However, research into the outcomes of parents with a learning disability whose children are no longer in their care has demonstrated both the anguish and sense of powerlessness they experience (Collings et al., 2020; Gould and Dodd, 2014; Mayes and Llewellyn, 2012). Recent evidence highlights how the impact of child removal for birth parents is profound and long-lasting yet remains poorly addressed by services. The Supporting Roots report (Critchley et al., 2023), commissioned by the Scottish Government, conceptualises child removal as a significant and enduring loss requiring timely, compassionate and sustained support. Drawing on both an evidence review and qualitative interviews with birth parents, the report identifies complicated grief, stigma and social isolation as common experiences, alongside limited and uneven access to post-removal support. Although situated in the Scottish context, its findings echo concerns raised in English research regarding the absence of coordinated, long-term responses once care proceedings conclude.
While research has shown that support services are necessary after child removal they are rarely provided (Baginsky, 2025; Koolen et al., 2020). This includes deficits around long-term support beyond that provided at a crisis point and joined-up work across children’s and adults services (Baum and Burns, 2007; Pytlowana and Stenfert-Kroese, 2021; Tarleton and Porter, 2012).
The Good Practice Guidance on Working with Parents with a Learning Disability (Working Together Parents Network, 2021) states that parents with a learning disability should receive emotional and practical support when the child protection process has resulted in their child no longer being in their care. There is insufficient evidence to show how this is being done in English local authorities, if at all. This study, of which this article is one part, aimed to begin to address this gap and it looked at the support that was or was not available from adult social care and from other agencies. The study was made up of four work packages. The first two included: • A rapid desk based evidence review of the support available to parents with learning disabilities whose children are no longer in their care. • A practice review involving interviews with key informants in all the professionals working with these parents and more detailed data collection with 22 local authority adult service departments.
The third work package involved case studies in eight English local authorities, including interviews with professionals in the statutory, voluntary and advocacy organisations, as well as interviews with parents with a learning disability whose children were no longer in their care. This stage was supported by an expert by experience (E-by-E) group of parents with a learning disability who, in turn, were supported by staff from the Elfida Society. It is the interviews with parents that are reported in this article. The fourth work package was an attempt to develop a model that showed the savings or costs to society of providing or not providing appropriate support for parents with learning disabilities whose children are no longer in their care (Baginsky and Thomas, 2025).
Methodology
Recruitment, sample and consent
It was agreed not to recruit parents through the eight case study local authorities to avoid both any conflict of interest and additional burden on social work staff. Instead we approached local advocacy and voluntary organisations in the case study areas. The research team approached 57 organisations between April and September 2023, including local specialist advocacy services, disability organisations, advice centres, in-house specialist local authority teams and national advocacy organisations. These organisations explained the project to potential participants and also used an Easy Read Participant Information Sheet developed collaboratively by the E-by-E Group and the researchers.
Recruitment was shaped by the sensitive and emotive nature of the research topic. Parents were aware that they would be asked to reflect on their experiences of support after their child was no longer in their care, an area strongly associated with grief, stigma and loss. As a result, several parents who initially expressed interest later chose not to take part. For example, in one peer-support drop-in session attended by a researcher as part of the recruitment process, parents explained that they did not want to discuss their experiences because it would be too painful.
Practical barriers also influenced recruitment. Parents were sometimes difficult to reach because of frequent changes of address and telephone numbers, loss of contact with key professionals and their struggles to read and understand written communications. Nevertheless, some parents agreed to take part because of strong, trusting relationships they had developed with advocates or staff in voluntary organisations. For instance, one parent had stayed in touch with her advocate despite having moved to another part of the country and, as a result, agreed to take part. Another parent, who did not use email or text, agreed to participate through the direct encouragement of a voluntary organisation staff member with whom he had developed a positive relationship.
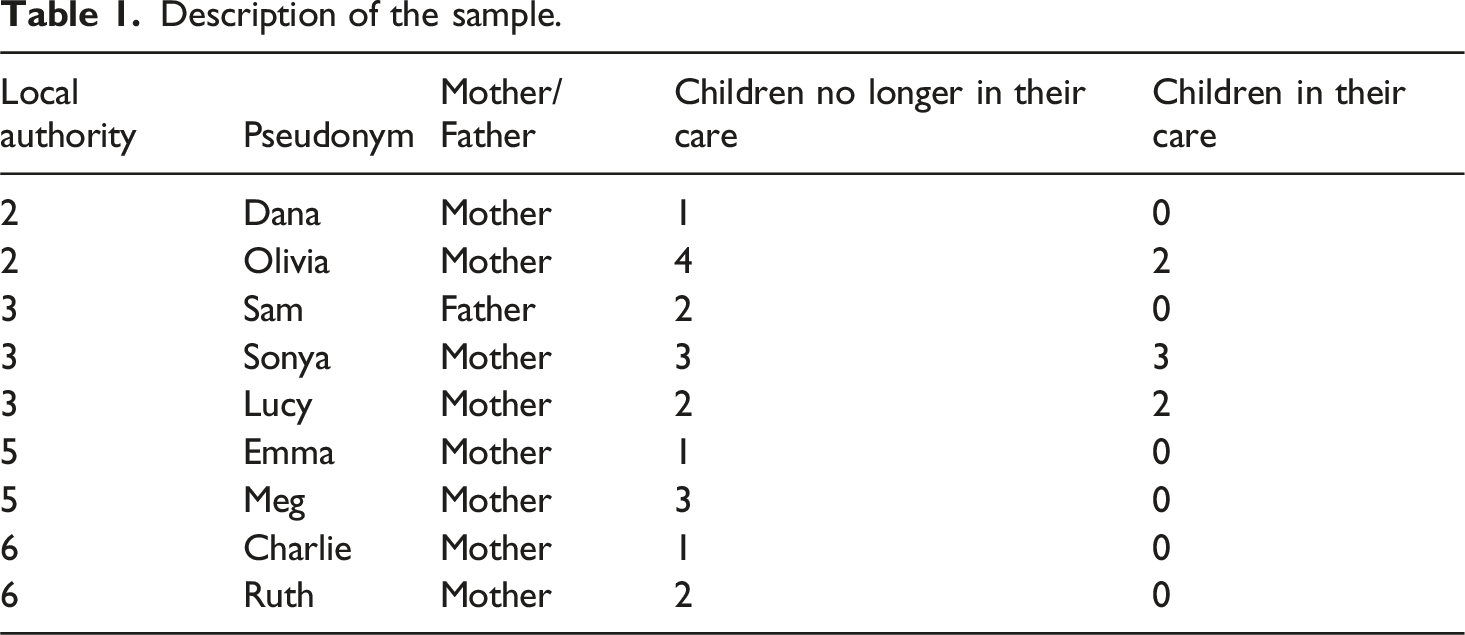
Eight mothers and one father from across four local authorities, agreed to be interviewed. All the parents were British born, six were White, two were Afro-Caribbean and one had an Asian background. We have used pseudonyms to protect the parents’ identity and removed any identifying details, such as specific life events, particulars about family relationships and named health conditions. Consent was sought in person using a consent form which, again, had been developed with the study’s E-by-E Group of parents with learning disabilities.
Description of the sample.
Interviews
All parents were interviewed by one of the authors who has experience of working with adults with a learning disability. They all took place in person in their homes or in the organisation that had supported their engagement with the work. All the interviews were audio recorded with parents’ consent. We encouraged parents to have an advocate, carer or family member with them to provide support during the interview and six parents did so. Those who accompanied the parents consented to assist not steer them and maintain confidentiality over what was said. The information provided on their role made it clear that they were present to support the parent to express their own views, not be a substitute for them.
Interviews lasted between 30 min and two hours. We adopted an approach that was intended to balance the need to try to elicit comparable information across interviews with the aim of allowing participants to shape and guide the direction of the conversation towards areas that meant most to them. As a result the interviews were very open and participant-led, designed to be flexible and conversational. Prompts were used only where necessary to support communication, seek further elaboration or return to relevant areas of interest. The intention was always to prioritise accessibility, using clear language, pauses for reflection and provide opportunities to revisit or clarify any point. Participants were offered breaks, and most also took time during the interview to pause or process strong emotions. An approach such as this is particularly important in work with parents with a learning disability, where more structured approaches may risk silencing or misrepresenting participants (Booth and Booth, 1996).
Analysis
Analysing these very open interviews required a flexible and iterative approach. The data were rich but often non-linear, with parents sharing stories that moved between different times and themes. To capture this, each interview was first considered as a whole, in line with Reissman’s (2008) emphasis on preserving the integrity of narratives, before moving to cross-case thematic comparisons (Braun and Clarke, 2006). This process highlighted how the interaction between participant and researcher had determined the direction and content of the interview (Atkinson and Silverman, 1997; FitzGerald and Mills, 2022).
Attention was paid to what was said, and how stories were told, including the use of pauses, repetition and language, reflecting Silverman’s (2017) observation that meaning in qualitative data is conveyed through both form and content. The analysis sought to remain sensitive to parents’ voices, while also identifying common themes across accounts, in an attempt to balance the need for thematic coherence with respect for the individuals’ voices.
We then met with the E-by-E group to discuss the emerging themes. This group reflected on how the findings resonated with their own experiences, highlighting similarities as well as differences. Their input also shaped the interpretation of the data, as they suggested refinements to the themes and identified areas where practice could be improved.
Ethical approval for the study was provided by King’s College London MRA-21/22-29065 13/3/2022 and modification approval 2/12/2022 and by HRA London - Camberwell St Giles Research Ethics Committee IRAS Project ID 31401 22/12/2022.
Funding was received from National Institute for Health and Care Research School for Social Care Research (102645/CM/KCLJM-P203).
Findings
The impact of children no longer being in their parents’ care
Most parents described experiencing profound and lasting loss after their children were removed from their care. Only Dana, whose child was placed with the father, described a sense of relief; she felt better able to sustain a positive relationship with her child, whom she still saw regularly.
The losses which were described had a marked impact on parents’ mental health. Emma described herself as having gone ‘off the rails’ following her child’s removal, turning to alcohol and self-harm and experiencing a serious mental health crisis. Although her situation later stabilised, she explained that her grief continued: I mean, yeah there’s some days you don’t want to deal with it and you want to die. Like Christmas and birthdays are hard without [child] in the house, knowing [child] is calling someone else ‘mum’…not knowing where [they] are
Charlie also experienced a crisis after her child was removed at birth. She has been told that she went missing for a period, although she could not recall for how long or what she did. Other parents also found it difficult to remember the time immediately following removal, reflecting on how painful those memories remained. And, similar to Emma, there were also references to struggling with the uncertainty of not knowing where their children were or how they were progressing.
Parents often described experiencing loss alongside other major life challenges, including physical and mental health problems, domestic abuse and bereavement. Three parents spoke about abuse in adult relationships and two said it had stirred memories of being abused in childhood. In two cases partners had died since the removal. For some, the absence of a strong support system deepened their feelings of isolation, particularly among those who had grown up in foster care or residential children’s homes. Meg illustrated this layering of difficulties: When I had [children] … it broke my heart because they lived here and then it's just like they just took them.
Her grief was compounded by her partner’s death: I feel like I've been let down, I’ve been lied to, I’ve had no support, I’ve lost my husband, I've had three kids removed.
Parents accessing support services after child removal
Some parents were referred either by children’s social workers and by others to support services for parents whose children were no longer in their care, which they all found valuable. Sam and Sonya had attended a local advocacy service with the specific remit to support parents with a learning disability. Both had been supported through care proceedings and after their children’s removal. Sam first attended when he was with his ex-partner, while Sonya came across the organisation after moving to the area. Emma and Meg were referred to a different generic advocacy service for parents going through care proceedings; although they worked with the same organisation, they were supported by different advocates.
However, there were also references to the absence of support when older children had been removed. Meg, for example, had three children. When her two older children were removed she had not received any specialist input, but, as referenced above, during later proceedings relating to her youngest child she had been referred to an advocacy service by the child’s social worker. There she worked with both an advocate and a counsellor, which she described as having been ‘really helpful’. She thought that such support would have made a difference to earlier outcomes if it had it been available. Sonya’s experience was similar. When her first child was removed she did not recall receiving any support, but after moving to a new town she became involved with an advocacy service for parents with learning disabilities that then supported her when her second child was taken into care.
Similarly, Lucy did not recall receiving any support during the removal of her two older children. However, when she had a third child she was referred by a social worker from children’s services to a specialist service. This service included both learning disability nurses and advocates. She considered that the support she had then received was what had allowed her to keep her younger children in her care. The advocacy and nursing input had provided crucial guidance in helping her to develop as a parent and keep her family together.
Not all parents accessed specialist services. Dana, Charlie, and Ruth had each sought other forms of support through local disability organisations not specifically focused on parents with learning disabilities. Charlie joined a self-advocacy group after applying for a job, and Ruth began attending these meetings, encouraged by a friend. Dana had sought support after being diagnosed as being autistic; a support worker then assisted her with navigating benefit changes following her child’s removal.
Four parents – Sam, Meg, Emma and Charlie – all recalled receiving counselling following the removal of their children which they had found helpful. Sam initially resisted counselling, but after struggling with the loss of his child he was encouraged by his child’s social worker to attend and described the experience as very positive.
Adult social care needs assessments and support
Four parents spoke about working with an adult social worker to access care and support. Lucy was the only parent to have this involvement during care proceedings, partly due to an existing health condition. After her older children were removed, she became pregnant with her third child and requested additional help. As described above, she and her partner received input from learning disability nurses and a key worker, and access to Direct Payments enabled her to employ a Personal Assistant to accompany her to ante-natal appointments. Lucy reflected: I said I couldn’t face going through a whole nine months, having the feeling of a baby kicking me, and going to the hospital, having all these scans and seeing the pictures on the scans, just for them to come along and say, right, we’re taking this baby away. As soon as I said that that’s when they turned round and said, ‘right, we’ll put in all the help and support you need to keep this one’.
Other parents received support from adult social care immediately after their children had been removed. Emma worked with a social worker for six to 12 months, who had helped her to access appropriate mental health support. Charlie also received support from an adult social worker and a key worker who helped her find suitable supported living accommodation and link her with a mental health support worker. Several parents explained that although they did not have a Care and Support Plan, they had been able to access weekly contact with an advocate or support worker in adult services.
For some parents a lack of a formal diagnosis of ‘learning disability’ had been a barrier to being able to access specialist care and support. Three parents explained that they had not received a diagnosis during the care proceedings after which their children had been removed. Only later, once diagnosed, did they begin to access appropriate support. Emma reflected on the long process of getting the right diagnosis: [Professionals] always knew something wasn’t right, during court, after court. But trying to get the right diagnosis didn’t happen until adult social care in [town], mental health services in [town] got their heads together and went ‘yep this is it’.
Meg said she only had a cognitive assessment when a children’s social worker became involved with her third child. Her older two children had been removed without such assessment: They had thought I had a learning disability but nothing come of it.
However even when Meg had the diagnosis it not lead to support, as like Dana, the decision was that she was not meet the eligibility threshold for adult social care. Similarly, while Ruth had been eligible for support from adult social care in the past, after moving to a different area she no longer met the threshold for support.
While some parents felt that having a formal plan in place would have been helpful, Dana felt her autism diagnosis had not led to any useful support: So this psychiatrist, she just said go to Autism [regional] and that’s it, there’s nothing else... when you think about all the other things that could be linked to it and not really checking up, it’s not very good really, I think. The social workers said it was not their problem.
She reflected on how difficult it had been to communicate her situation and needs relating to contact with her child: I think I was just overwhelmed by everything, and it was trying to explain my problems about [named child] they just focused on other things... they’re not very understanding when it came to it… and I didn’t really have the skill or the understanding of my own problems, it was, it was very hard.
Professional relationships, trust and mistrust
Parents’ interactions with professionals, including social workers, psychologists, advocates, and midwives, were often difficult in the period leading up to the removal of children. Their experiences left many with feelings of injustice that then shaped their later engagement with services and had a specific impact on their willingness to trust social workers. For some, this distrust stemmed from their childhood experiences in care that were reinforced by later encounters as parents. Lucy, for example, recalled how, soon after the removal of her child, she felt unsupported when hospital staff told her that a close family member had died following an accident: You can just imagine hearing from a doctor... how hard it is to hear that your [family member] has basically gone, and you’re just there on your own, and you haven’t got no social worker if you need any kind of support whatsoever
She linked this to earlier experiences of what she described as dismissive attitudes from social workers while growing up in care. When her two eldest children were removed, those earlier poor relationships confirmed her distrust. With the exception of one support worker, who took time to learn about the abuse she had endured, she felt no one else had bothered to try to understand her circumstances. Emma, who had also grown up in care, said early experiences of social workers who ‘came and went’ left her wary of children’s services. Although she later developed a trusting relationship with her child’s social worker, she remained sceptical of others whom she believed had not been honest with or about her. Others described similar levels of mistrust. Ruth felt that while family and friends were supportive, her experiences with social workers had been wholly negative. For Sam, distrust was so strong that he avoided adult social care altogether: No. I’ll be honest, I wouldn’t have a social worker. It’s a child take away service… Why do I want a social worker when you just take my kid away?
Several parents believed health conditions or physical limitation had been used against them in parenting assessments. Lucy was convinced social workers had decided she could not look after her children even when she proposed practical solutions. Sam recalled being asked how he would prioritise his child if his own condition deteriorated, a question he experienced as accusatory and stigmatising. These accounts reflect a level of distrust rooted in long histories of negative experiences which persisted even when individual professionals attempted to build positive relationships. In some cases, it actively deterred parents from engaging with services that might otherwise have provided support.
However, some parents contrasted their more recent, positive experiences with children’s social workers to earlier negative ones. Emma described receiving an exceptional level of commitment from one children’s social worker, who was available ‘at all hours’ and became a crucial source of support during care proceedings and afterwards: She would be there at 11 o’clock at night if I needed her, but then she left social work, saying she had enough.
Meg, Lucy and Sonya all felt that relationships with their current social workers from children’s services were better than those they had encountered during previous child protection proceedings. Sonya explained that her youngest child’s social worker helped her maintain contact, enabling their relationship to continue. Meg described her most recent adult-services social worker as pivotal in building rapport and facilitating access to advocacy: She listens to me. If I have any concerns I just talk to her… all in all they’re brilliant, I can’t fault them.
She also valued her child’s social worker, who ensured support after court proceedings and helped shift her view of children’s services: It just takes that one person to show that you can trust them… I can’t now say anything bad about social services.
These experiences show how consistency, honesty and accessible communication can foster trust and engagement, whereas fractured relationships, turnover and perceived judgement can entrench mistrust and limit access to help.
Communication between parents and professionals
Six parents said they had been offended, distressed or confused by how professionals communicated with them, even when their learning disability (or suspected learning disability) was known. Sam recalled being left bewildered by decisions in a Mother and Baby Unit after his partner experienced a mental health crisis and left. The assessment of his parenting capacity seemed to slow down, before he was suddenly told that proceedings were moving to court. At that point he said he had no idea what was happening or why.
Charlie also described experiencing deep confusion. She had not known she was pregnant until late on, and after giving birth felt overwhelmed by her new role. Her child was removed soon after birth, which she experienced as a denial of the chance to learn parenting skills, but before that happened she had felt bombarded by the demands of professionals and unsupported in her transition to motherhood: First of all she [the midwife] took [the child] and then she came back and put [the child] straight on me... it doesn’t sink in for a while what I’ve got to do.
Other parents spoke of poor communication at critical points. Dana said her child’s social worker gave her no guidance about how to arrange contact visits during the pandemic, despite knowing she had a learning disability. Meg described her cognitive assessment with a psychologist as confusing and intrusive, particularly when questions turned to her past relationship: It was like a barrier to me and I just didn’t want to talk about it... it was just too much information for my brain.
Across these accounts, parents described communications they perceived as being abrupt, accusatory or insufficiently adapted to their needs. This had reinforced their mistrust of professionals and left them feeling marginalised in decisions about their children.
Lack of consistency
All parents described times when there had been inconsistency in their interactions with professionals. Sam highlighted how the child protection process with his second child was far more confusing and frustrating than with his first. He recalled having to work with a succession of social workers, with gaps in between: We had about five, six different social workers… one went abroad, another went on maternity leave without telling anybody… for months we had no social worker… then we got someone else but we couldn’t understand what he was saying… again he didn’t last because he got put onto another team.
Parents often found it difficult when support they had been able to access ended. Dana said the women’s support group she attended at a regional autism centre had suddenly stopped due to funding cuts. As noted above Ruth had lost access to adult social care after moving to a new area where she no longer met the threshold. Emma also described the shock of moving areas and losing the support network she had built: I went from all these people to one person [named domestic abuse support worker], and it’s a shock to the system.
She valued the professionals who had supported her and was acutely aware of her dependence on them: For me it was difficult because I didn’t have my family around me… I still had some professionals, even though half of them were shit - mental health services were like chocolate fireguards.
These reflections highlight how inconsistency - whether through frequent staff changes, sudden withdrawal of services or variations in professional commitment - shaped parents’ trust and engagement with support.
Advocacy and voluntary organisations
For some parents advocacy services or voluntary organisations became the only professionals they felt able to turn to for support. Six parents had developed strong working relationships with advocates. Meg and Emma had both worked intensively with specialist advocacy services, receiving regular home visits or weekly meetings. They described this support as invaluable for managing court processes and daily challenges. Meg reflected: [Advocate] helps me out a lot and she’s brilliant… if I didn’t have [advocate] I would probably just not know where to start.
Sam had a longstanding relationship with an advocate whom he trusted: [Advocate] has been there more for me than like a social worker… she’d support you through it and it feels like not just having things done to you.
Other parents described more practical or community-based support. Sonya’s advocate, for example, primarily helped her manage bills but had also supported her through the time when her child had been removed. Dana, Charlie and Ruth had not worked with specialist advocates, but drew strength from disability organisations and self-advocacy groups that they said gave them confidence and a sense of belonging.
Impact of support
Parents emphasised that strong professional relationships helped them make sense of their experiences, sometimes by reframing a child’s removal as less of a personal failure. Emma, for example, described the experience as ‘the toughest of my life’ but had been able to cope because of the professionals who had supported her. Dana similarly felt reassured by professionals who acknowledged her efforts: People were like very, very quick to jump up and say, ‘it’s okay… you did the best’, they were really trying to help me.
Discussion
This study highlights the enduring impact of the removal of children on these parents. Most described the loss as ongoing grief rather than a discrete event, often compounded by other adversities including bereavement, poor health and experiences of abuse. As such it was not a one-off event but a long-term source of trauma and exclusion. These findings resonate with previous research that frames child removal as a chronic trauma for parents with learning disabilities (Booth and Booth, 2005; Collings and Llewellyn, 2012). The feelings of grief and loss were exacerbated when parents lacked strong informal networks and relied almost exclusively on professionals for support which was not always available and could be disrupted. The depth and persistence of grief described by parents in this study mirrors findings from Critchley and colleagues (2023) who characterised the removal of a child as a form of chronic bereavement rather than a discrete event.
The quality of those professional relationships was a key factor in shaping parents’ experiences. Mistrust of social workers was a feature of many of their accounts, often rooted in their own histories of growing up in care and reinforced by negative encounters in adulthood. Poor communication, staff turnoverand perceptions of being judged deepened this mistrust, consistent with Booth and Booth’s (1996) observations of how such barriers may silence parents’ voices. These findings also resonate with MacIntyre et al.’s (2019) argument that constructions of vulnerability can obscure parents’ strengths and reinforce pessimistic assessments of capacity. Parents’ accounts suggest that once their children were removed, this framing often persisted, shaping the nature and limits of post-removal support rather than prompting a coordinated, reparative response.
Negative working relationships with professionals in the lead up to and following their child’s removal often dominated the parents’ understanding of what had happened and confirmed their feelings of injustice. This is significant when considering the majority of professionals working in non-specialist learning disability professions have been found to lack the knowledge and skills to work with parents with a learning disability (MacIntyre and Stewart, 2012; Pytlowana and Stenfert-Kroese, 2021). The experience of one or more negative relationships with social workers could lead to a mistrust in the whole social work profession. This, in turn, would make it more difficult for them to engage with professionals and services that sought to help them.
At the same time, parents described how a single strong relationship with a social worker or advocate could transform their engagement with services. The parents’ accounts illustrate that even within difficult circumstances, consistent and respectful professional relationships could help parents maintain trust, access support and process the loss of their children. These findings underline the pivotal role of relational practice suggesting that building and sustaining trust is not an optional extra but a core requirement for effective support (Ferguson, 2011).
Access to specialist services was a recurring theme. This is an area where there are significant gaps in services for parents, both for those with and without a learning disability, whose children are no longer in their care (Broadhurst and Mason, 2020; Mason and Wilkinson, 2021). Parents also valued advocacy and other support services, but opportunities to engage with them were uneven and often dependent on diagnosis, referral or geography. For some parents, support was only put in place after repeated removals or late diagnoses of a learning disability. In some cases, parents reflected that earlier access to support might have changed the course of care proceedings, echoing much earlier concerns about the ‘postcode lottery’ of support (Tarleton et al., 2006).
Diagnosis often functioned as a ‘gateway’ to specialist provision yet delays or absence of assessments meant that several parents were unsupported at critical points and felt they were initially left alone to fend for themselves. McConnell et al. (2011) criticised how structural barriers to timely identification continued to shape outcomes for parents with a learning disability.
The findings also expose the fragility and inconsistency of support systems. Parents’ accounts in the present study suggest that support was often time-limited, crisis-oriented or contingent on geography or diagnosis, reinforcing concerns that post-removal needs remained marginal within both adult and children’s services.
Parents described how sudden loss of services due to staff changes, funding cuts or changes in eligibility thresholds had left them disoriented and unsupported. For those without strong family networks, these shifts had significant consequences. Again, this highlights structural issues in how services for parents with a learning disability are resourced, coordinated and sustained.
Several implications for practice and policy emerge from these findings. Firstly, early and proactive support, particularly during pregnancy, could help to prevent escalation into care proceedings. Secondly, reasonable adjustments in communication and assessment are essential to ensure parents’ rights under the Equality Act 2010 are upheld. Thirdly, the descriptions of the advocacy services parents used indicate that they were trusted and effective, yet they remain patchy and precariously funded. Finally, recognising child removal as a source of chronic grief may prompt more appropriate long-term support for parents, rather than short-term crisis responses.
Limitations of the study
While this study provides insights into the experiences of parents with a learning disability following the removal of their children, there are several limitations that must be acknowledged. The sample was small and self-selected, recruited through advocacy and voluntary organisations. Parents who agreed to take part may have been those who have been more engaged with services or more willing to discuss painful experiences. As a consequence the perspectives of those who declined or could not be reached are not represented. Recruitment through these organisations also meant that parents without links to advocacy or voluntary services were not included, potentially skewing the findings towards those who had at least some form of support. The study was conducted in a small number of areas of England, where local service structures shaped parents’ experiences. The findings may not transfer directly to other local contexts.
In most interviews an advocate or family member was present. Although they very rarely contributed, and only then to remind the parent of a particular incident or help bring them back to the subject, parents may have altered their answers - consciously or unconsciously - because of their presence, either to fit with what they thought was expected or to avoid disclosing potentially embarrassing events (Hall et al., 2025).
The openness of the interview approach enabled parents to shape the conversation which meant the data reported were co-constructed between participants and the researcher. They were also influenced by parents’ willingness to disclose experiences which may have been shaped by trust, mood or prior experiences with professionals. While the interviews generated rich and nuanced accounts, the extent to which comparisons could be drawn across the group. Several parents also described difficulty recalling events around child removal due to the trauma involved, which may have created gaps or inconsistencies in the data. In addition, some parents were only diagnosed with a learning disability after their children were removed, reflecting the complexities and complications surrounding this population but also limiting their ability to reflect on experiences of support at that time as a ‘parent with a learning disability’. Future research could build on these findings through larger and more diverse samples, attempting to include parents outside formal support networks, and applying imaginative ways of working with parents in study design and analysis.
Conclusion
By putting the voices of parents with a learning disability at the centre this study showed both the damage caused by inconsistent practice and the potential for relational, accessible, and well-resourced practice to make a significant difference. It has highlighted the central role of professional relationships in shaping the experiences of parents with a learning disability during and after child removal. While mistrust of social workers was common, rooted in both childhood and adult experiences, parents also described how a single consistent and respectful relationship could transform distrust into trust. However, access to support was uneven, sometimes contingent on diagnosis or referral, reflecting structural inequities that have long been noted by others. The findings point to the need for systemic changes to ensure early, accessible and consistent support, alongside recognition of the consequences and longevity of the grief experienced by parents after a child has been removed.
Footnotes
Acknowledgements
The authors wish to acknowledge the support provided by Elfrida Society and the society’s parents’ group. We also recognise the input from the parents who contributed their experiences, and the families and advocates that supported them, whom we are not able to name but to whom we are extremely grateful.
Ethical considerations
Ethical approval provided by: King’s College London Ethics Committee MRA-21/22-29065 HRA London - Camberwell St Giles Research Ethics Committee IRAS Project ID 31401 22/12/2022.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the NIHR School of Social Care Research Ref: 102645/CM/KCLJM-P203.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.