
Abstract
This paper explores the notion of time when undertaking interpreter-mediated Mental Health Act Assessments (MHAAs) from the perspective of Approved Mental Health Professionals (AMHPs). It is based on one theme that emerged from a reflexive thematic analysis of 17 semi-structured interviews with AMHPs undertaken as part of a larger corpus (Young et al., 2023). We found when carrying out interpreter-mediated MHAAs, AMHPs perceive time as luxury; something that they do not have in abundance, and which is made more problematic through the additional exigences when an interpreter is required. The luxury of time to which participants refer is determined ostensibly by resource availability underpinned by risk. Systemic and structural barriers also pertain. Driven by time’s omnipresence, these findings demonstrate fluctuations in how AMHPs use spoken/signed language interpreters and give rise to contradiction and sometimes passivity in practice. These findings are important considerations when undertaking any social work service that might require interpreter-meditation and are especially significant during a MHAA when a person’s liberty is at issue.
Keywords
Introduction
Time is omnipresent in mental health law. It decrees the length of compulsory detention and dictates processes and procedures, including responses by mental health professionals. One such response, Mental Health Act Assessments (MHAAs), involves the undertaking of an assessment of a person where there is concern about their mental health and risk of harm either to themselves or others. This assessment is a complex process carried out to determine the need for hospital admission which can result in a formal detention commonly known as being ‘sectioned.’ A MHAA where the person’s first or preferred language is not English usually means the involvement of an interpreter, or interpreter-mediation, and provides an additional layer of complexity, including a heightened temporal one.
The current legislation which governs mental health in England (and Wales) is The Mental Health Act, 1983 (henceforth MHA). Under this legislation Approved Mental Health Professionals (AMHPs) - previously Approved Social Workers (ASWs) - have a duty to coordinate a MHAA. They also hold the ultimate responsibility for reaching a decision about detention. Equivalents of AMHPs exist in Scotland (Mental Health Officers), Northern Ireland (Approved Social Workers), and Wales (Approved Mental Health Professionals). This paper reports findings of a reflexive thematic analysis of 17 semi-structured interviews with AMHPs in England undertaken as part of a larger corpus (Young et al., 2023). The findings pertain to all equivalent roles, as well as to interpreter-mediation more generally in social work.
Given the potential seriousness of the outcome which could be a deprivation of liberty, effective communication in MHAAs is crucial. These assessments involve several elements one of which, interviewing the person, helps an AMHP to decide whether an application for detention should be made. The statute itself dictates that interviews must be undertaken ‘in a suitable manner’ (MHA section 13.2). As such, being able to understand and be understood throughout a MHAA but especially at interview, the point at which communication is at its sharpest relief, is fundamental. In circumstances where a person’s first or preferred language is not English an AMHP is responsible, as outlined in the Code of Practice (the guidance that accompanies the MHA), for arranging an interpreter (DoH, 2015: para 14.116). However, whilst this guidance outlines what should be done (such as ensuring the interpreter has expertise in mental health interpreting), it does not say how, a gap which the wider research study seeks to address. In this paper we focus specifically on the issue of time. We discuss its omnipresence, the contradictions and passivity that are brought to light through AMHPs’ perceptions of interpreter-mediated MHAAs and the additional intrinsic demands of these situations. This paper is the first to report the perspective of AMHPs specifically focussing on interpreters in MHAAs. Other papers address the current relevant literature (Rodríguez-Vicente, et al. under review) and interpreter-mediated MHAAs from the point of view of interpreters (Tipton et al. under review).
Research design
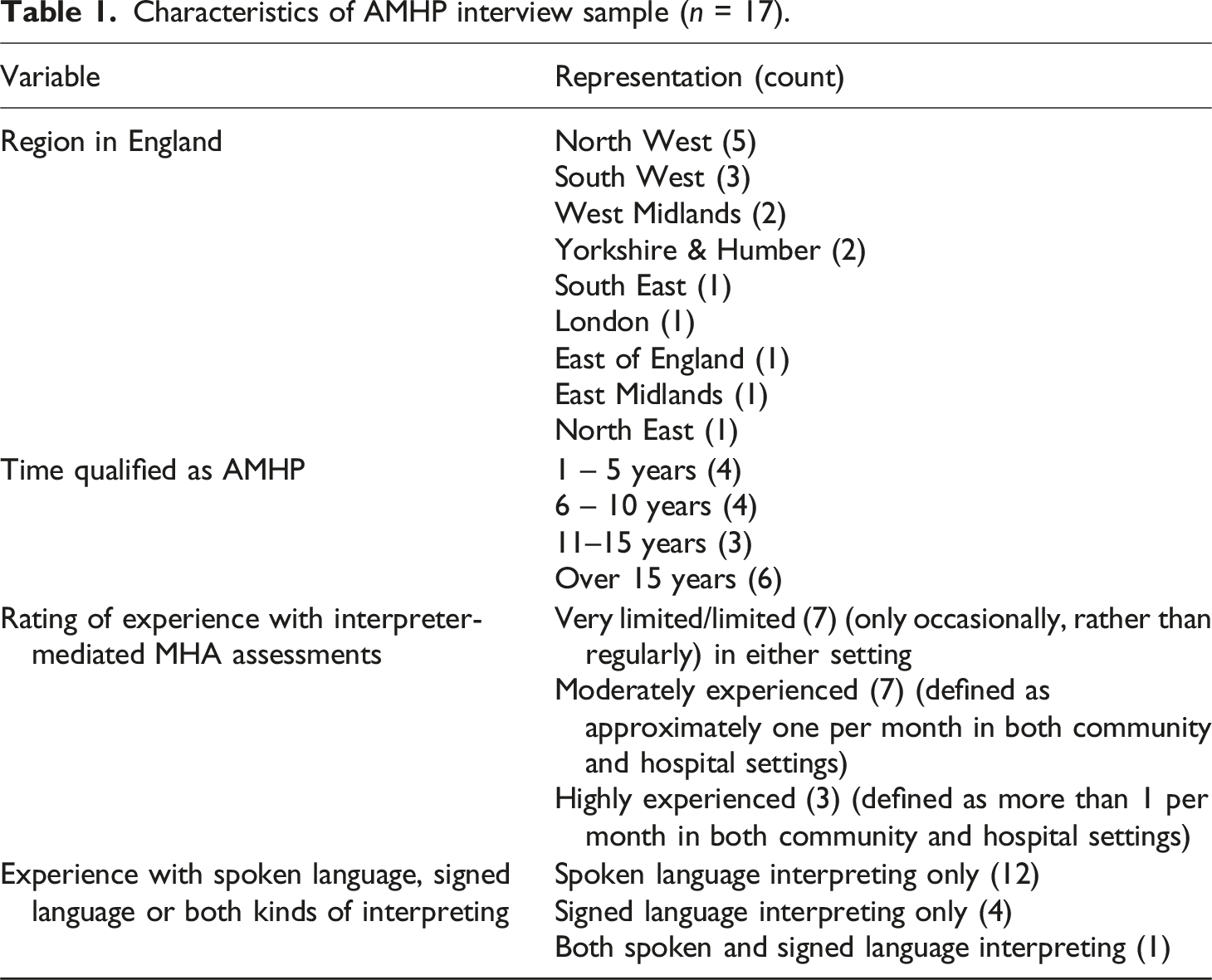
Characteristics of AMHP interview sample (n = 17).
Ethical approval for the study was granted by the University Project number 2021-12163-20436. All interviews were carried out via Zoom or Microsoft Teams depending on the restrictions of the AMHP workplace guidance. The interviewers (authors Vicary and Young) were both registered social workers and former Approved Social Workers (the forerunners of AMHPs) as well as academic researchers. Interviews were video and/or audio recorded through the online platform and automated speech to text recording was used also. All automatically generated transcripts were individually checked for accuracy and amended accordingly. Transcripts were anonymised and any identifiers removed. Participants were interviewed once for up to 1 h.
Braun and Clarke’s (2019) reflexive thematic analysis guided the analysis process as it was essential to elucidate both key themes and the reflexive stance of the AMHPs in how they interpreted their practice under interpreter-mediated conditions. The positionality of the researchers as practice professionals (whether AMHPs/ASWs or interpreters) taking an active role in knowledge production through the use of their disciplinary lenses to interpret the data could also be foregrounded through this approach. In addition, the collective sharing of perceptions of these data through a reflexive discussion of nuances of interpretation, of contradictions and of consistency of judgement gave rise to agreed themes, one of which is the subject on this paper.
Turning to the process in more detail, a sample of five transcripts were independently reviewed by three team members, the two original interviewers and another whose background is in interpreting and translation (author Rodriguez-Vicente). Each generated a set of potential top-level codes. These codes were then compared and discussed to identify points of concordance which nonetheless might embody subtle differences in perspective, unique suggested codes not identified by others, and expansion and definition of what might be encompassed in the top-level code. This individual and shared reflexive process resulted in a list of 11 codes with initial definitions of their scope. The method of drawing from team members from differing disciplinary and academic backgrounds was important in an interdisciplinary project that was seeking to explore and report on a trans-disciplinary professional experience. Reflexivity mediated through the medium of language has been significant for the wider research study and is currently being analysed, the results of which we also plan to analyse and publish.
The 17 transcripts were divided between the three team members who were also coders and text under each code identified and marked with the assistance of the qualitative data analysis software QSR NVIVO 12 plus. Texts collated under the initial codes across the 17 interviews were then examined in depth to iteratively generate the thematic structure under which the findings are presented below. In what follows we consider experiences of interpreter-mediation in MHAAs from the perspective of AMHPs through the notion of the luxury of time. The findings from the analysis of this one unifying theme are illustrated using verbatim quotes. Each AMHP participant is allocated a numerical code which denotes an excerpt of their individual evidence but has no other identifiable trait.
Findings
Quotes capturing the omnipresence of time dictated by risk or the absence thereof provide the overarching theme for this analysis: you know you are on a deadline (AMHP 003). need to dig quite deep, and that takes up time which you don’t necessarily have (AMHP 008). when we’ve got the time to do it [interpreter-mediation] as well as we can and we’ve got the and the risk indicates that we’ve got that time, when it's really high risk, it still happens, and we do the best we can (AMHP 014).
As noted earlier, it is a statutory requirement as part of any MHAA that a person who may be deemed (medically) mentally ill and a risk to themselves or others must be interviewed in a suitable manner. However, where the mediation of this suitability requires interpretation because of the person’s first language preference, the data indicate that securing such interpreter-mediation is perceived as a luxury of time determined by sensitivities around harm to the person or others: there was the luxury of time to be able to do that ‘cause the person/the patient was safe, and they were in a safe environment, and I was able to leave them there and rebook (AMHP 004).
Based also on the potential for harm, other time pressures vary according to the living situation of the person being assessed and underscore the perception that having time is a luxury. For this next participant, being in the community affects the decision about the immediacy to act or ability to wait: The risk wasn’t high enough for them to need an assessment immediately (AMHP 014).
The rationalisation made later by this same AMHP is that a postponement is ‘allowed’ as the person is relatively safe; in the AMHP’s perception an assessment can be delayed for the enablement of interpreter-mediation if there is absence of risk for the person (or of others). To emphasise this decision-making process, the same AMHP also goes on to suggest that the person’s living situation may have meant that to delay was not possible because of risk – delay would be a luxury of time. Of particular note is the justification made in the hope that to go ahead despite not accessing appropriate interpretation was ‘sufficient,’ as to do so balances the need for a timely assessment against the potential for harm to the person that any delay may cause: Had it have been a crisis assessment in the community. I may not have been had the luxury to be able to do that would depend on risk, so yeah, it would be very dependent on the situation. I would have had to have just continued to go forward, and although I didn’t feel it was the best and hope that it was sufficient (AMHP 014).
That said, this same AMHP proposes the idea that, on some occasions, it may be necessary to stop and start/resume the process of a MHAA according to interpreter availability. In so doing it can be suggested that the priority may not be with enabling an interpreter-mediated assessment but in managing what transpires as the MHAA proceeds: So, we still try and fit in where we can (AMHP 014).
Data also show the desire to try and slow things down and for one respondent the responsibility of ensuring appropriate communication is actively acknowledged: We are going to have to somehow delay it (AMHP 003).
Practice which the same AMHP repeats so that interpreter-mediation can be sourced:
You should delay the assessment if at all possible (AMHP 003)
Aside from the availability of an interpreter, time pressures may also be affected by the disposal of other resources, both of which are required should the patient require hospital admission, namely a bed: five people waiting [for a bed] in the wings (AMHP 007)
and an ambulance: because you have got an ambulance (AMHP 007)
Similarly, the presence or indeed imminent departure of the doctor is an added time pressure: Because when the doctors come in, they very often have to rush off to the next assessment. They don’t have the time for you to hang around, and an interpreter might not have been early because stuck in traffic or whatever (AMHP 007)
One other respondent further reiterates the pressure of time as a direct consequence of a doctor’s schedule. This participant also reinforces the perception that there is the added pressure because of the time-limited availability of the interpreter: things happen very quickly sometimes, particularly when the doctor’s late, and then the interpreter’s saying, well I’ve got to go (AMHP 013).
The perception of not having any or of just having limited time influences actions. It is interesting to note in these data the uncertainty expressed about the impact of going ahead without an interpreter along with the indication that such situations are not common, or at least are not prepared for. Again, the thought is posed by one AMHP that interpreter-mediation may have enhanced the process but is seemingly not the priority. Time instead dominates: it [the interview] may have been enhanced by the use of an interpreter but yes, I think that we get limited or non-existent time to think about and prepare for these kinds of situations before they arise (AMHP 017).
This sense of unpreparedness concerning interpreter-mediation in MHAAs and the discomfort experienced is echoed by another participant who also suggests that such situations are not commonplace: it doesn’t happen at all on a regular basis, but those times it does happen, it’s not comfortable is it? Because you’re weighing up quite a lot of things and you’re also pleading with the interpreter to stay (AMHP 013).
That the AMHP feels the need to plead with the interpreter suggests that they are under time pressure to not lose the resource over which they also appear to have little control. The unfamiliarity, along with uncertainty of the process of arranging for an interpreter, is also reported by another respondent. This is in turn made more complex by pressure of time as they ‘rush around’: then I think perhaps related to the infrequency of needing to arrange an interpreter, there then is always a rush-around of how on earth do we do this, what arrangements do we have with them in terms of paying agencies and therefore then get the information off of our systems about…with all the other stuff that you’re having to think about this, trying to find the policy and whatever reference that you might need, to provide to an agency (AMHP 017).
Even in circumstances where interpreter-mediation takes place, aspects of practice vary. First, the use of remote communication and the acknowledgement that such methods are not ideal:
you know, carry out the assessment in a in a timely and safe manner. I have used… I’ve had to use an interpreter over the phone, which wasn’t an ideal situation and handing the phone back and forth with the person who’s you know, and quite acutely unwell at the time and I’ve used it on, on like an iPad where you can actually see on the screen which was quite… that was that was better (AMHP 015)
There is further evidence suggesting that in some MHAAs effective interpreter-mediation is understood and practised. Each of the following examples are influenced by time but the influence of it is used in an active way. The first concerns the importance of being able to request an interpreter in advance and to do so for a sufficient amount of time:
is important to actually making sure that you book an interpreter for a sufficient amount of time, book it for an hour or longer so they’re not needing to like rush off to another job, or something else (AMHP 007)
The second concerns briefing. It is recognised that in interpreter-mediated MHAAs AMHPs need to spend time with interpreters beforehand, albeit this respondent suggests that this is not consistent practice: as a matter of course, some people do, some people don’t, try to spend time with the interpreter, to brief them and talk to them before an assessment happens (AMHP 013).
In other circumstances the opportunity to undertake a briefing which is recognised as good practice by this participant is compromised through time pressures. In this AMHP’s eyes there is a return to anxiety concerning the person’s safety that dictates the process; the unknown risk for the person is a factor in this situation that heightens the perception of the lack of time and in turn impacts on the opportunity for an effective briefing: We haven’t seen the person. There were worries about their safety. I got an interpreter within the hour. I briefed her on the walk up to the house (AMHP 014).
For some AMHPs the experience of working with interpreters is viewed as collaborative and beneficial because of the expertise that can be shared. One example concerns deaf mental health services that employ interpreters in-house, in which working as a team is celebrated, including the need for briefing, debriefing, and shared learning: I’ve always worked with interpreters that were part of the team. So, they developed a lot of experience, so that was really good. It means you have time to think about it, discuss before, like debriefing, debriefing afterwards, and explaining what the difficulties are, how I can improve for next time (AMHP 010).
The use of relatives as interpreters is an aspect of practice which although not recommended can in some instances be a pragmatic response where that pragmatism is linked with perceived lack of time and/or the impact of not acting in a timely manner. In the incident that follows the AMHP recounts their concern at being let down by an interpreter despite having made plans in advance. Mindful of the possible impact of further delay (especially on the continued availability of doctors), this AMHP went on to use a relative as interpreter acknowledging that actually in so doing the mediation was poor: So, I had actually arranged for a physical interpreter to come but then they didn’t turn up and I think we had some communication to say that they would be half an hour late. So, we waited half an hour, and they still weren’t there but the person’s father was there and yes, it was a case of do we proceed with the father or do we not, do we wait. I mean actually waiting wasn’t really an option for the doctors, so it would then be a case of waiting and then rearranging the assessment when the interpreter came. So, I think that probably was unrealistic, to be able to achieve, so we did actually then assess with father interpreting, and I think that I had commented, also when I wrote it up that one of the problems with that is dad kept answering the questions without relaying…even before relaying them to his son. So yes, that did pose issues with the reliability of what we were hearing. (AHMP 017).
In summary, our data show that when carrying out interpreter-mediated MHAAs, AMHPs perceive time as luxury; something that they do not have in abundance, and which is made more problematic through the additional exigences when an interpreter is required. We now discuss these findings (luxury of time and delay, systemic and structural barriers, passivity and pragmatics) in the light of our transdisciplinary knowledge and relevant literature.
Discussion
The clock motif depicting time is not an unusual one that is invoked when AMHPs are asked about conducting a MHAA (Vicary, 2021). It is interesting to ponder what in these current data lies behind such omnipresence and the perceived pressure that accompanies interpreter-mediated MHAAs. First luxury of time and delay.
Luxury of time and delay
In the true sense of the term a luxury is something desirable but costly or hard to get, something adding to but not absolutely necessary. In these data delaying an interview to enable interpreter-mediation is perceived as a secondary consideration when the circumstances with which the AMHP is faced constitutes a risk to the person (or others). Justification for not enabling interpreter-mediation in such instances is reported as the interview would be ‘sufficient’ or an admission that the interview ‘may have been enhanced’. But let’s consider this further. First, delay. In most instances two medical recommendations are required before an applicant, usually an AMHP, can sanction a formal detention. These recommendations, although they do expire, do not do so immediately. In fact, they can remain ‘live’ for 14 days (Department of Health, 2015 para 14.92: 129). Arguably delay (or at the very least the fact that an AMHP has up to 14 days to decide before the recommendations expire) should be a normal consideration during a MHAA, the need for interpreter-mediation notwithstanding. There are some instances in these data when delay is promoted, but these are couched in the concept of the luxury of time, and it is this juxtaposition that requires further exploration - it seems the need for interpreter-mediation is eclipsed by considerations of risk even when there are acknowledged communication needs. Herein lies a contradiction; a formal admission which might be an outcome of a MHAA is a powerful and potentially harmful intervention - to delay so that an appropriate interpreter-mediated interview can take place could mean that formal detention is averted. To not delay and to conduct an interview without interpreter-mediation albeit justified by the avoidance of harm could lead to poor communication and the possibility of an unlawful detention. There is then a dilemma; delay is not to ignore the fact that the person being assessed is likely to be in a crisis (as risk is an important consideration), but we question the process in these data which appears to override interpreter-mediation because of it, a justification which seems to be based on the protection of the person. Ironically, to not enable interpreter-mediation and thereby appropriate communication could mean harm. The dissonance between the protection of the person and not in effect undertaking an interview in a suitable manner where there is the potential to restrict liberty and potential harm is stark.
Other subliminal parlance in these data gives rise to further contradictions; the weighing up of risk against the extra or luxury of time required suggests that a MHAA with an interpreter and one without are not equivalent, as the former needs more time. Consequently, it could be argued that different kinds of decisions will be made in the marginal cases whereby waiting for an interpreter is not possible - time creates the risk that otherwise would not be there if an interpreter was not needed and the MHAA could go ahead without delay. The apparent reluctance to delay may not just be a matter of ensuring that risk is responded to in a timely manner. These data also indicate that it is seemingly acceptable to delay or to go ahead and rush an assessment depending on who is causing the delay. Delaying a MHAA when a doctor is not available or arrives late does not seem to be a ‘standard’ afforded where an interpreter cannot be available in time. Such seemingly contradictory reactions might suggest that it is the systematic pressures and perception of medical importance that is driving the process rather than concern for appropriate communication, a finding to which we later return. In one instance in the data the pressure of time and the possible impact on doctor availability led to the use of a relative as interpreter. In balancing their concerns about delay with access to interpretation, the process and outcome described is poor, as is acknowledged by the AMHP. Decisions made with the ‘short term’ interest in mind (such as using the relative as interpreter) and the long term which might seem impractical in the short term give rise to a further contradiction.
Systemic and structural barriers
Turning to systemic matters indicated in these data, first preparedness. Many AMHPs in this sample feel unprepared for interpreter-mediation. But, according to our research (Young et al., 2023) interpreter-mediation in MHAAs is not uncommon. Unpreparedness suggests uncertainty of practice which might impact on its effectiveness, but the data show that this perception is not universal, and instances of mitigation are given. For example, one respondent reports practice in terms of teamwork highlighting that there is a shared relationship between the AMHP and the interpreter which can be mutually beneficial including briefing, debriefing, and learning from the expertise of each (Tipton et al. under review). In broad social work practice, research (Tipton, 2010) finds that there can be an unwillingness to share background information with interpreters that help to contextualise the interactional encounter. The concept of teamworking therefore is not necessarily shared or actively pursued by all interpreters or primary service providers. In the high-stakes context of MHAAs, this highlights the importance of the briefing process and an openness on the part of both professionals to information exchange relevant to the situation at hand.
To enable such collaborative practice is a difficult balance for an AMHP who as the legal decision-maker also holds the ultimate responsibility. However, recognition that interpreter-mediation is a shared process which warrants time is nonetheless a recommendation that we make. For instance, it is likely to be the case that briefings are not undertaken for lack of time. Instead, it is our view that an appropriately briefed interpreter will actually enable a more effective process and ultimately save time. To not build in time to carry out an effective briefing is therefore a further contradiction. Unpreparedness can also be addressed through readily available access to appropriate interpreter services, depicted on several occasions in these data as an obstacle to good practice. We are aware that most interpreters work freelance, and there are recognised supply-demand issues (Napier et al., 2022). This is a systemic issue outside of the control of AMHPs, but if as one AHMP suggests they make the interpreter booking request for a longer time period this challenge can be mitigated. Such barriers are a matter for commissioning authorities, rest with local agreements and can be influenced by financial pressures. They are nonetheless structural concerns that add to the complexity of interpreter-mediated MHAAs and underpin the undoubted time pressures.
Structural barriers, particularly access to services and supportive systems so that AMHPs can fulfil their obligations, are however not a new concern. They underpin a long-held debate concerning the origin of the AMHP role which purports that AMHPs are mere administrators undertaking a bureaucratic process primarily to ensure a person is assessed and admitted as needed (Bean, 1980). The need for alternatives therefore should not be of concern in the fulfilment of the AMHP role. Later commentators suggest that the AMHP role as conceived is not possible to achieve given that few, if any, alternatives services to formal detention are available (Barnes et al., 1990; Prior, 1992), a standpoint echoed by Karban and colleagues (2021) whose exploration of the social perspective which is said to be the aspect AMHPs bring, is deemed compromised by lack of alternatives. Furthermore, when considering the fundamentals of the role, AMHPs must (along with others to which the MHA applies) uphold the principles of the MHA as currently laid down in the Code of Practice. There are five principles (DoH, 2015: 2) each concerned with upholding the rights of the person being assessed and these too have also been seen to be compromised in the literature. For example, the notion of trust needed between the AMHP and the person in order to uphold rights during MHAAs have been seen to be negatively impacted on by systems (Abbot, 2021). Likewise, the voice of the person is reported as lost during and to some extent because of the process of MHAAs according to views of those who have been subject to them (Blakely et al., 2022). Most recently one commentator reported that AMHPs themselves question who the role is for, being caught between a technical-rational endeavour and a moral one, both compromised (Hemmington, 2023). Being (un) able to uphold such value-based practice during MHAAs is a debate to which we now turn as there is an interesting dynamic present in these data which we are referring to as passivity, a finding which resonates in this debate about the pragmatics of role fulfilment and also seen previously through AMHPs’ perspective of another (medical) role in MHAAs.
Passivity and pragmatics
In a recent research study also exploring MHAAs from an AMHP perspective, the medical role is deemed fulfilled, that is the role is over once the medical recommendation is complete (Vicary et al., 2019). Furthermore, in a play on words the same article questions whether AMHPs roll over (Vicary et al., 2019). This apparent passivity is discussed as shift, the notion that those workers who perceive themselves as having more worth move work to those who less privileged in this regard and who actually end up doing it, however dirty (Vicary et al., 2019). This sociological concept of ‘dirty work’ has been applied to psychiatric occupations since the early 1970s (Brown, 1989; Emerson and Pollner, 1976). More recently it has been applied to the AMHP role in which MHAAs are not viewed as dirty work but instead legitimised either as therapeutic (Quirk et al., 2000) or providing status (Morriss, 2016). Dirty work as understood through the notion of shift questions this legitimisation suggesting instead that AMHPs are passive participants in MHAAs (Vicary et al., 2019). Our data also demonstrates such passivity or an indication of a lack of assertiveness on behalf of the AMHP in MHAAs where interpreter-mediation is required. There is a seeming lack of control over the process highlighted through the presence or absence of interpreter-mediation As discussed earlier, the availability of interpreter-mediation is ostensibly a structural matter, but it may be that such apparent passivity is a pragmatic response by AMHPs whose role during MHAAs is nothing if not multifarious. Said to comprise legal, administrative, and practical functions (Hargreaves, 2000), the AMHP role and responsibility is increasingly attracting research interest, including about its origin (Rapaport, 2006), motivation for doing the role (Stevens et al., 2018), the similarities and difference of decision-making based on risk according to professional background (Stone, 2019; Vicary, 2023) and thoroughness of assessment and need for greater collaboration at the point of a referral (Simpson, 2024).
As the professional responsible for coordinating the MHAA, AMHPs have to balance the process with the pragmatics that transpire, a finding that is not new. For example, in research commissioned by the Department of Health during the first attempted reform of the MHA, in overseeing the MHAA process, Approved Social Workers (AMHP forerunners) were said to be contingency managers; their role involving juggling, improvisation, cajoling and persuasion to get various busy professionals to the same place at the same time (Quirk et al., 2000: 6). In much the same vein, more recent research suggests that AMHPs are hybrid professionals; they use knowledge from different fields, (now) come from different professional backgrounds and straddle multiple roles both as AMHPs and in doing a ‘day’ job (Leah, 2023). The need for contingency management continues in our data but where in previous research this refers to corralling doctors, ambulances and beds, our data for the first time adds interpreters.
There are other pragmatics involved; pleading with an interpreter to stay is perhaps a realistic response as this is the resource available at that time and if lost may not be replaced. The availability of resources such as a hospital bed or an ambulance, or of doctor or interpreter presence (or indeed the pressure of their imminent departure) are matters that must be managed practically during a MHAA. Likewise, such pragmatics might also dictate the use of remote interpreting. For instance, an uncommon language could make it difficult to locate an appropriate interpreter and a decision might be taken to have access remotely rather than not at all. Similarly, interpreters tend to be concentrated around larger rural areas, remote assessments may therefore be more prevalent in rural areas. Despite remote MHAAs been determined as legal only if undertaken in person and recently confirmed in respect of renewing detention (Derbyshire Health Care NHS Trust v Secretary of State for Health and Social Care [2023] EWHC 3182 (Admin), it is nonetheless increasingly being suggested that assessment of some services can be undertaken remotely, albeit in less complex circumstances (Department of Health and Social Care, 2023). Remote assessment by interpreters remains a practice in MHAAs and might then remain an accepted norm despite what might otherwise be deemed best practice. Lack of assertiveness, or passivity, might actually reflect the reality of the situation. It is much reported in MHAAs that hospital beds are in high demand yet short supply and that AMHPs there should be supported by commissioners to ensure bed availability, which is after all a doctor’s responsibility (Department of Health, 2015: para 14.77) but delegated. Realistically, availability of interpreters and their use remotely might also be subject to this continued outcome and may be symbolic of the long-held debate about what the AMHP role is; a pragmatist doing what they can to uphold rights but compromised by structures and systems.
One final passive matter arising indirectly from this research and to which we referred briefly earlier concerns what is for us a masked issue. As reported in a recent editorial, (Bamford et al., 2024) England is a diverse nation, increasingly so, and the need for interpreter-mediation is likely to remain yet is hidden. The disproportionate numbers of detentions of people from black and minority ethnic communities is one of the reasons driving a second but now stalled reform of the MHA (Department of Health and Social Care, 2018). However, whilst attention, rightly, is on such disparity, it may be at the neglect of underlying communication needs as a result of language preference, whether spoken or signed. Whilst not known (as data is not collected in this respect (Rodríguez-Vicente, et al. under review), people from such communities will not all use English as their first or preferred language. It is also likely that when in crisis situations a person will revert to their preferred language. Furthermore, for deaf British Sign Language (BSL) users, even if they are highly bilingual in BSL and English, there will still be a need to work with interpreters in this context in order to be able to carry out a MHAA ‘in a suitable’ manner.
Conclusion
This paper discusses the findings of one aspect of a larger research study which set out to explore best practice in interpreter-mediated MHAAs. Using data drawn from semi -structured interviews of AMHPs’ experiences of interpreter-mediated MHAAs and a reflexive thematic analysis of them, time emerges as a theme that determines practice. We found that time and its omnipresence in interpreter-mediated MHAAs give rise to contradiction and passivity. Time-related pressures are couched in the concept of time as a luxury; pressures of time dictate whether or not to delay an interview weighed by perceptions of harm, which is an inherent contradiction and a negative impact on best practice. Decision-making rests on systemic matters such as availability of an interpreter (as well as other resources). Undoubtedly interpreters should be a critical part of a MHAA if the person being assessed does not have English as their first or preferred language. Weighing risk against delay we found is an aspect of the MHAA process and could also mean lack of equivalence.
This is not to say that all practice is wanting. Other elements of this theme reveal effective practice in interpreter-mediation and include preparedness, briefing and debriefing, and collaborative working based on trust. That interpreter-mediation is a shared process which warrants time is nonetheless a recommendation that we make and now available in the Guidance and Resource produced as a research output. It our view that an appropriately briefed interpreter will actually enable a more effective process and ultimately save time. However, whilst indications of good practice are shown, these are also on occasion influenced negatively by the pressure of time. We suggest that the awareness of, and confidence in, the best practice for working with interpreters during MHAAs fluctuates and tends to be a passive reaction perhaps based on pragmatics underpinned by access to, or lack of availability of, interpreter resource and heightened by perceptions of harm.
This article for the first time adds interpreters into the understanding of AMHPs (and their equivalents) as contingency managers but finds that their use is at best masked. Sadly, this mirrors the lack of attention given to interpretation in the now stalled reform of the MHA. We suggest, in light of the increasingly diverse population in England that interpretation in mental health services particularly at the point of a MHAA becomes a more robust element of policy and of its application in practice. Similarly, we recommend that assessments (whether MHAAs or otherwise) that require interpreter-mediation are undertaken in person and that this is recognised as proportionate in such practice.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NIHR School for Social Care Research (Grant No. P172).