
Abstract
This article provides an account of using reflexive participatory methods including study advisory group membership to evaluate a perinatal wellbeing service in an economically deprived area of Scotland. There is little qualitative research that explores the experiences of women accessing perinatal mental health services. This article draws on feminist values and narrative theory to explore the practice, process and ethics of using participatory methods with women in the perinatal period. We explore the blurring of intervention and research group boundaries to consider the service and study advisory group as a space which provided the conditions for collective care and re-storying the self. We explore the study advisory group as an extension of the intervention itself, highlighting the role of community in research practices and in interventions, for women who experience perinatal mental health difficulties. We reflect on the ‘sticky’ practice of navigating epistemic and decision-making power in participatory research, including the dual positionalities of being two academic researchers who come to research with therapeutic training in counselling, psychotherapy and social work. We call for reflexive, community-oriented and flexible approaches when using participatory methods with populations that might be considered vulnerable, marginalised or stigmatised.
Introduction
This article describes the use of reflexive community-based participatory methods in an evaluation of a perinatal wellbeing service in Scotland. Perinatal mental health difficulties can be experienced by anyone, but those who experience social disadvantages, such as poverty (Power et al., 2017), migration (Sharapova and Goguikian Ratcliff, 2018), domestic violence (Howard et al., 2013), extreme stress or lack of social support (Galloway and Hogg, 2015) are at greater risk. At the time of writing this article, despite clinical guidelines and a commitment from Scottish Government to improve access to perinatal mental health services, gaps in service provision still exist (Galloway and Hogg, 2018) and there is limited evidence about the effectiveness of perinatal mental health interventions. We carried out a service evaluation focusing on service-user views.
In this article we describe the process of working with a study advisory group of women who had accessed a perinatal wellbeing service, and who worked with us to design the methods and analyse data. We explore how the study advisory group process became data and to some extent an intervention itself. We consider this blurring of boundaries to have produced a space in which knowledge could be generated, enabling insight into the broader themes we explored in the evaluation. These themes included the importance of establishing trust and safety, the value of meeting others and feeling valued by others including practitioners, the flexibility of the services provided, reducing stigma and isolation, and the need for holistic care including reducing barriers to access.
We draw on narrative psychology to consider the therapeutic nature of giving voice to stories and experiences (Frank, 2013). Narrative theory refers to the idea that storytelling is a key part of how we make meaning and communicate something about who we are (Frank, 2010). It also attends to the role of context, dialogue and relationship, assuming that it is through dialogue and relationship that we story and re-story who we are (Mishler, 1986). Drawing on narrative and dialogical theory, this is underpinned by the assumption that being human is about being in relationship, and it is through these relations that we come to exist (Buber, 1996). As such, we consider how we, the researchers, were part of the process of facilitating a space which we think had a therapeutic effect, and we also consider how ourselves as researchers impacted issues of power. We use narrative theory to consider this research process as a relational practice, through a relational epistemology, understanding that knowledge is produced through a dialogical interplay between researcher(s) and participant(s) (Riessman, 2015). We also discuss the role of feminist values in research such as this. These include aiming for non-hierarchical relationships through collaboration, grounding research in the lives, priorities and understandings of people our research concerned the most, and embracing knowledge production as co-constructed, political and subjective.
Our aims in this article are to (a) explore the use of group participatory methods with women in the perinatal period who are experiencing distress and facing social injustices or stigmatisation, (b) consider the blurring of research and intervention as producing opportunity for knowledge production and (c) to explore issues of power as two researchers working with a group of women experiencing social stigma or difficulties in the perinatal period.
A participatory approach to evaluate the service
The perinatal service was set up within a family centre run by a third sector organisation. The family centre provided a range of services including early years care and family support and it was where research activities were carried out. We used a participatory approach to evaluate the perinatal service. All qualitative research is participatory in nature (Ellingson and Sotirin, 2020); however, specific to participatory approaches is the aim to work in partnership with people or communities that are stigmatised or marginalised, in an effort to work against the colonising effect of social science research practices that are traditionally postpositivist, rooted in the assumption that researchers can ‘extract’ information, risking exploiting participants (Gullion and Tilton, 2020). A range of methods have been termed ‘participatory’, including participatory action research (Houh and Kalsem, 2015), community-based participatory action research (Wallerstein and Duran, 2010) or critical participatory action research (Fine and Torre, 2019). These approaches aim to involve members of communities in the research design and practice (Ellingson and Sotirin, 2020), and engage in collaborative processes of knowledge production whilst addressing social inequalities and social justice (Lile and Richards, 2018).
We agreed with centre staff, early in the process of conceptualising the evaluation, that the involvement of centre users would be a key consideration in the design of the project. Community-based participatory methods can be an effective way of evaluating services or interventions (Wallerstein and Duran, 2010), particularly those that work with marginalised or socially stigmatised people (Muzik et al., 2016; Smith and Romero, 2010). Acknowledging stigmatisation and marginalisation felt important as many people that accessed perinatal support in this project were experiencing poverty, stigmatisation and significant mental health difficulties. The centre was located in one of the most deprived areas of Scotland (gov.scot, 2020), and the level of deprivation became clear as we learnt staff often used resources to provide families with clothing and basic food. They also worked with migrant and asylum-seeking families, sometimes where English was not their first language or where people did not have English language reading or writing abilities. We understand these issues to be located within broader socio-structural conditions.
Our approach aligns with shared values of feminism and participatory research, in their aim to centre voices of community members, aiming for an egalitarian, non-hierarchical relationship through collaboration (Houh and Kalsem, 2015). Situating our research within feminist values meant aiming to ground our research in the lives, priorities and understandings of the people our research concerned the most (i.e. those in the perinatal period) (Fine and Torre, 2019). It also meant attending to the intersections of methodology and epistemology as we aimed to ‘disrupt and destabilize the characterisation of traditional knowledge production and social science research as objective, apolitical and democratic’ (Houh and Kalsem, 2015: 263). As such, we frame the participatory approach we used around Ellingson and Sotirin's (2020) definition, of aiming to ‘honour multiplicities of knowledges and make explicit the inherent connections between power and knowledge’ (p. 88). We wanted to engage with this interconnectedness of methodology and epistemology in an effort to resist epistemological injustices that are enabled and enacted through most traditional methodologies that can have colonising or marginalising effects (Fox, 2015).
To our knowledge, at the time of writing this article, there were no published studies that have evaluated perinatal wellbeing services in the UK using participatory methods. Most perinatal mental health service evaluations adopt quantitative designs using questionnaires or outcome measures (Lavender et al., 2016). However, participatory approaches have been used in similar studies, for instance, to evaluate primary care and maternal mental health services (Lund et al., 2012), to explore the views of young mothers about perinatal physical and mental health care (Muzik et al., 2016), and to develop e-health apps for women (Gordon et al., 2016). Some of these studies include steering groups or consultation groups, some use what is termed ‘community models’ involving what is sometimes termed ‘community researchers’ alongside academic researchers together (e.g. Smith and Romero, 2010) or peer-interviewers (e.g. Croft et al., 2016).
The study advisory group
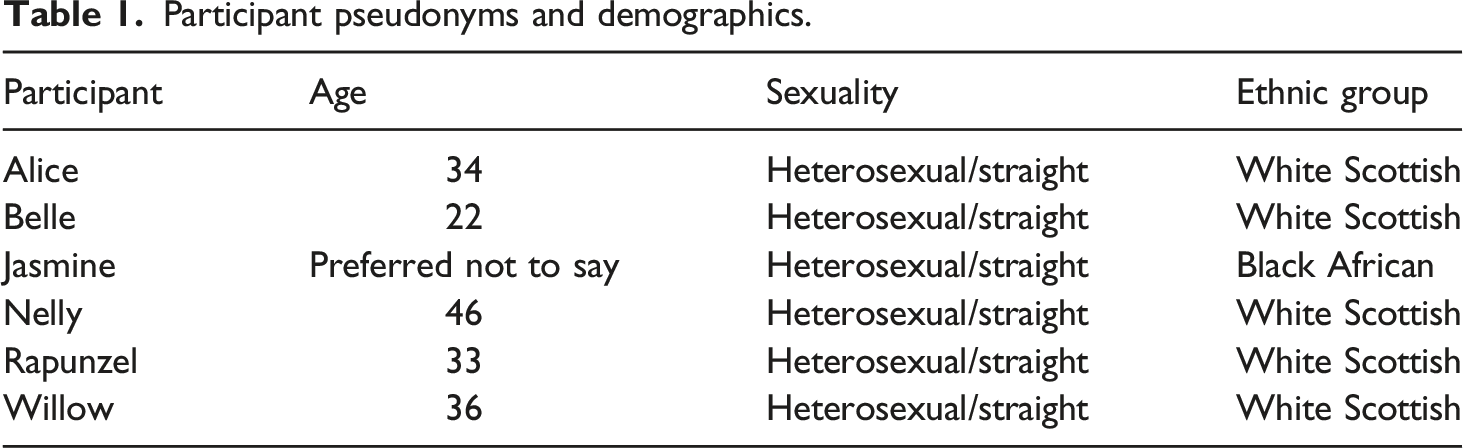
We worked with centre staff to recruit a study advisory group of six women who had used the perinatal wellbeing service. Centre staff advertised the project in groups at the centre and invited women they thought would be interested and in what they thought to be an appropriate place with their mental health to participate. We received ethical approval from the University of Stirling (approval number: GUEP479). The inclusion criteria were that women had completed the maternal mental wellbeing project, meaning we were likely to recruit women who were experiencing poor mental health during pregnancy and up to 3 years postnatally. Some women had participated in the same groups, so some were familiar with each other.
Participant pseudonyms and demographics.
Developing the evaluation with the study advisory group
We held four study advisory group meetings over a period of 5 months, covering study design, data collection and initial data analysis. Meetings took place at the family centre every 6 weeks. Each meeting was 2 h, and the final meeting was 3 h. We gave time for comfort breaks, research-oriented discussion, and time to check in and explore issues that emerged during group discussions. A creche was provided for participants’ children, centre staff provided transport or travel costs, and we provided food and drink. We provided vouchers for attendance at each meeting. We regularly invited feedback about the level of participation and engagement that felt appropriate and desired.
A mixed methods approach was used for the evaluation. This included peer interviews, women writing their own case studies, a focus group with service staff, a focus group with women accessing the service, a questionnaire for external professionals and a questionnaire for women using the service. For this article, we focus on the process of working with the study group advisors. We expand on the use of peer interviews and how this data informed the evaluation.
The first research meeting centred on introductions, making working together principles, outlining the purpose of the study and gaining permission to collect data from the meetings. The women decided on naming themselves ‘research assistants’. As they also acted as research participants, and explicitly consented to this role, they will be referred to in this article as participants, study advisory group members, or women. We discussed women’s experiences of the service, we agreed on the research aims and objectives, and planned for the next meeting.
At the second meeting, we introduced methods of data collection (interviews, focus groups and questionnaires) and the methods and recruitment strategies that were most amenable to other women accessing the wellbeing service. We then planned data collection. A key distinction at this stage was that the women, being former or current participants on the wellbeing programme, held important knowledge and experiences and felt they wanted to be research participants themselves in addition to other participants. We discussed the level of involvement participants wanted, deciding that women would be involved in interviewing other participants about their experiences of the service, analysing data, and they would be involved with the dissemination activities but did not wish to heavily contribute to writing. They were happy to read and check what the researchers wrote, rather than lead or co-lead themselves. We planned subsequent meetings accordingly.
In preparation for the third meeting, we constructed questionnaires for professionals and facilitators using questions designed by participants, we also distributed a questionnaire for other women participating in the wellbeing service and attempted to setup a focus group. At the meeting, we shared the questionnaires that had been created and updated the group on the challenges of recruiting other women to participate. Discussing the challenges of participant recruitment prompted women to discuss their own experiences relating to parenting, pregnancy and engagement with the service. At this point the women offered to include their own experiences and following further ethical approval, we decided to carry out peer interviews and case studies about their experiences of the service.
The fourth research meeting focused on analysing data with study advisory group. We had interview recordings transcribed, and as there was a time limit, we began initial coding of transcripts prior to this meeting. In the meeting we read transcripts, invited discussion, and continued coding and note-taking together. In particular, we invited the women to work with the transcripts from the peer interviews, as this felt most pertinent to explore in the group. To end the group, we invited reflection on what it had been like to participate in the study advisory group, and we planned how to keep in contact for further project-related activities, including reviewing reports and planning for an end of project event. We checked again for participants’ wishes regarding their level of involvement with subsequent activities, mindful that official project time, and as such, payment for time, had come to an end. One participant volunteered to be a contact for reviewing reports written from the evaluation, and another participant volunteered to be a contact person for organising an end of project event.
The research process
Overlapping layers – the process of research became research data
Ellingson and Sotirin (2020) suggest that ‘participatory process data (can) enrich the project through multiple overlapping layers of meaning’ (p. 92), which can relate to and enrich the research findings. We found that in study advisory group meetings, conversation fluidly shifted from broader life topics to research-focused topics. Most of the themes discussed during study advisory group meetings, and most of our observations became research data, with full awareness and consent from the participants. For example, the group became a supportive and caring space where women discussed their broader lives, families and experiences as they related to what was coming up in the research. These included fears of deportation due to asylum-seeking status, experience of a family member’s suicide attempt, grief, despair, experiences of seeking counselling, traumatic births and family relationships. Women also spoke about fears around accessing the service and getting mental health support, reflecting broader literature which suggests motherhood ideologies around being a ‘good mother’ often shape people’s internal stigmatisation and produce barriers to seeking help (Moore et al., 2016). We consider the family centre as a community that made it possible for women to voice these experiences. It is likely that the women’s earlier and ongoing involvement with the centre may have influenced the way they opened up as this was a community space that existed prior to this research project and would continue after. In some way, this blurred the boundaries between the interventions we were evaluating, and the study advisory group. This boundary blurring made sense; the topics discussed such as mental health and experiences of the service, were directly related to the women’s everyday lives. It is also noteworthy that as researchers, both of our backgrounds include training that made us well positioned to work with emotive or distressing material. TF is also a psychotherapist and counsellor, and SL is a registered social worker.
The boundary fluidity may have happened because some elements of the study advisory group meetings almost replicated the structure of the interventions participants had accessed, such as checking-in at the start of meetings, and talking about feelings in a group setting. The group dynamic formed organically, enabling us to get to know participants in ways that extended beyond the research aims and enriched how we understood the evaluation. We came to see this fluidity as a site of insight and knowledge where layers of meaning ‘overlapped’, producing opportunities for enriching knowledge and understanding.
A further development was the evolution of the women’s role in the project. Their involvement was initially conceptualised as advisory in nature, to help us to better understand the perinatal project and ways to engage with current attendees. But during the process of working together, their role changed as they became key informants, largely in their peer researcher role. We gained additional ethics approval for this amendment, with explicit written consent from the participants and agreement from the project partners at the service. The women were publicly named as advisory members in the evaluation report and end of project event.
In terms of how these changing roles and blurring boundaries can be safely managed for and with participants, this speaks to ethical issues not always captured by institutional ethics review boards. We co-wrote a group contract at the beginning of the project in an effort to hold boundaries and manage expectations from the beginning. The research group members were embedded into the service, which provided a bridge for participants to access support should it be needed. As the project evolved, we made several adjustments to the project protocol and as such, returned to our institutional ethics review board each time a new method was decided or a decision was made by the group which required approval. Regulatory approaches to research ethics have been critiqued as an emphasis on following rules, governance frameworks and institutional ethics review procedures is at odds with the dynamic, complex and values-based nature of ethical issues that often occur in participatory research processes such as collaboration, boundary blurring and community relationship processes (Banks et al., 2015). The relational and values-based ethical issues that occurred were therefore not captured in the institutional ethics approvals, and were instead, reliant on continuous dialogue with the group members, including boundary setting at the beginning of each meeting by processes such as setting agendas and returning to agreed planned activities. This felt to be more aligned with a commitment to democratic decision-making and knowledge production (Janes, 2015). However, this commitment presents a tension with the hierarchical power structures of researcher-researched (Janes, 2015) and institution-service user (Groot et al., 2022). In line with Groot et al. (2022), we consider that relational reflexive work that attends to power is appropriate in participatory work, and an ethical commitment to bring people together for solidarity, support and advice can be fruitful.
Research space as a therapeutic space? Mirrored processes and multiple selves
In this section we discuss the development and co-construction of what we consider to be a therapeutic space in the research group, and we consider issues around epistemic power. Before this discussion, it feels important to locate ourselves and our own positionalities.
SL was Principal Investigator and is a social work lecturer. She is a white woman who at the time of writing had a child and was pregnant during research group meetings. SL has experience of postnatal depression and although did not directly share this with group members was able to relate to some of the difficult parenting experiences they shared. TF was a PhD student at the time. TF is a white, cisgender woman who is not a parent, though does have her own experiences of accessing mental health services at various points in her life for an eating disorder. She could relate to some of the participants’ experiences of distress but did not disclose this.
We kept field notes and used car journeys to and from research meetings to discuss how the meeting had gone, especially if it had been particularly impactful for us. Four years after completing the project, coming together to write this article prompted further reflection via informal discussions, which we believe deepened our understanding of ourselves situated within this project.
The therapeutic frame and the research frame both have different purposes. However, we want to consider how our own ways of being contributed to how we understand the therapeutic qualities of the research group, and how we understand the blurring of boundaries that we discuss in this article. Because the study group mirrored some of the group interventions the participants had taken part in (e.g. time, regular meetings, familiarity of people, location), it made sense that this mirroring might mean participation in the research group was experienced as therapeutic in a similar way. However, we consider that our own therapeutic trainings in social work (SL) and counselling and psychotherapy (TF) informed our approach as researchers. Whilst we did not intend to facilitate a therapeutic group, as researchers, we do not leave our ways of being and values outside (Bondi and Fewell, 2017). From that view, we almost certainly played a role in shaping not only the therapeutic qualities of the group, but also how we understand the way that played out.
Following Dickson-Swift et al., (2006), researchers can take up what feels like multiple roles, such as researcher and friend, or researcher and therapist and similarities exist between research interviews and psychotherapy as both provide a space to talk, they might aim to empower the person, the researcher or therapist has a ‘listening’ role and the client or paricipant discloses personal information. Also, research interviews and therapy can be projects of meaning-making (Bondi, 2013) which might involve topics that are sensitive or difficult to talk about (Hydén, 2014). Bondi (2013) has suggested that the researcher can become the ‘third person’ – bearing witness to and validating the participant’s story; not unlike the therapist in psychotherapy. From a narrative perspective, we consider that this third person – or in our case – multiple-person witnessing and listening, can offer opportunities for participants to consider themselves in new or different ways by making meaning through dialogical and relational storytelling (Frank, 2010).
In our case, the participants also bore witness to one another, demonstrating similarities to group and community-based processes of healing. This had implications for identity and meaning-making. We found that mothers were deeply aware of social expectations around motherhood and they regularly spoke about how the singular caregiving relationship can be tough. The horizontal relationships that developed during the group research process between participants enabled the difference between maternal subjectivity and idealised motherhood to be openly explored. For example, during Nelly and Rapunzel’s peer interview, Nelly explained that due to the loss of her mother there were times when it did not feel like the right time to be sat in a group. Rapunzel suggested that alternatively, ‘maybe it was’. This alternative perspective offered a different way for Nelly to story herself and construct a version of her story that may have had a different meaning; where loss and grief were a welcome experience and her distress did not necessarily imply a not ‘good-enough’ mother. This can be understood from a relational and dialogical identity perspective too, as participants’ identities came into being in relation to each other. Lawler (2008) argues that people become tied to specific identities through subjectivation and become subject-ed to rules and norms that engender these identities.
We consider that group participatory projects such as this have the potential to co-produce spaces that can be experienced as meaning-making projects whereby participants can re-story themselves or hear their stories reflected back in new ways, demonstrating similarities to not just a client-therapist dyad, but the therapeutic value of group and community spaces too.
The group setting became a nurturing space, in which the participants shared their experiences and difficulties of parenting, while there were divergetnt experienced amongst the group there was a commonality of singular care giving by the mothers, commensurate with Western values of autonomy and individuality. In the context of parenting in Scotland, and following (Everingham, 1994) the dominant experience is of singular care giving, and the normative expectations, is that it is overwhelmingly the mother who accepts the personal responsibility for the care of her child.
Through sharing experiences and stories, the group seemed to become one of solace and strength, which was maintained by a sense of collective and community care. Drawing on narrative psychology (Frank, 2013; Holloway and Freshwater, 2007), there is potential for empowerment and transformation through storytelling with others. This resonates with our experience as we observed the potential for healing and relationship building through the sharing of stories and experiences that are socially stigmatised.
The family centre, and by extension, the study advisory group, functioned to provide a space which helped to enable survival against injustices and a space to build relationships with those who came up against similar barriers or injustices. Participants reflected on the value of the space that had been built through their participation in the research, but they also acknowledged that ‘you need to feel open and ready to participate’. Drawing on narrative psychology, voicing experiences and stories can help people to regain a sense of power (Holloway and Freshwater, 2007) or construct a new or re-storied identity (Frank, 2013). Law et al. (2021) conducted interviews with women in Canada about their experiences of perinatal mental health difficulties. Consistent with other literature, and with findings of this study, they found that that sharing experiences with others had the potential for healing and self-care, bolstering a sense of self-worth in the face of societal norms surrounding mothering and being a ‘good-enough’ mother that were experienced as harmful (Law et al., 2021). In this sense, the study advisory group acted as a space that one participant described as ‘it keeps me going’, another reflected that ‘I forget I have problems’, and another described as ‘it feels like we’re helping others’. This aligns with existing research which suggests that peer support can not only be of therapeutic benefit (Jones et al., 2014) but engaging with peers can also offer space where shared experiences have a container or a shelter, and this can bring about a sense of solace and healing (Law et al., 2021).
We were also struck by participants’ choice of Disney princess pseudonyms. Assigning pseudonyms is typically done by the researcher, under the premise that protecting participant identity is an ethical issue. However, the process of naming also speaks to issues of power and voice (Allen and Wiles, 2016). Women were already subject of the gaze of professionals (Everingham, 1994) and increasingly scruitinise themselves and their own mothering practices. Using cultural symbols – in this case, Disney princesses, fictional narratives and characters could have the capacity to narrate their journey and identities. Rules and customs around naming were meaningful in particular ways to the participants for this research. Pseudonyms may not only mask identities but also may act as a ‘nuanced form of anonymity’ (Miyazoe and Anderson, 2011: 184). Participants chose names that encapsulated both interest in life and also the key story told in relation to the research topic. Acts of naming are political and personal, and as Nespor (2000) points out, where pseudonyms have previously been thought of as ‘devices for protecting participants’, they might in fact be considered as ‘strategic tools that play important roles in constituting objects of inquiry’ (p. 546). As such, renaming participants has psychological meaning to both the participants and the content and process of the research (Allen and Wiles, 2016). Taking up the names of Disney princess characters might have been a mechanism through which participants’ accounts could enable them to escape the specificity of their situation through a shared group identity bound up with notions of fantasy and escapism, associated with princesses and heroines. This kind of characterisation in the context of voicing survival, echoes a survival ethos, mirroring what participants were experiencing. Through fun and fairytale names, this naming process can be understood as a particular way of representing their lives and the depths of their trauma.
‘Sticky’ considerations of epistemic power and decision-making
Reflexivity is a way of engaging with and examining how researchers are part of the research process in personal, relational and political ways. For this project, reflexivity offers a way of positioning and reflecting on the ‘self’ in and amongst the voices and stories of others, guided by the assumption that researchers shape the unique way in which the stories of others are told and interpreted and (Finlay, 2002; Wilkinson, 1988).
Drawing on Lenz Taguchi's (2012) conceptualisation of reflexivity as a transcorporeal process, we consider that we, as researchers, were both affected by the research process and the women’s stories, and we also affected how we make sense of the research process and the data. We draw on Ellingson and Sotirin’s (2020) description of the ‘sticky’ discomfort of doing reflexivity as we grapple with issues of epistemic power in this project. In this section we provide a brief account of our use of reflexivity as a practice to support us to stay with these ‘sticky threads’ (Ellingson and Sotirin, 2020), acknowledging that to stay with what we are affected by through research practice can offer meaningful knowledge (Chadwick, 2021). Our reflections are based on informal discussions about our own positionings and our outsider (and insider) statuses.
Some of our reflections have centred around how participants were paid for participation by providing vouchers at each research meeting. When we asked women about why they participated in the study advisory group, one of the participants, albeit almost jokingly, stated they participated ‘to get the voucher’ and then followed up by saying she was ‘only joking’. Whilst there is an element of humour, we also sincerity in what she said. Paying participants is a somewhat debated issue due to concerns around coercion, incentivisation versus the importance of acknowledging participant expertise and labour (Head, 2009). We wanted to acknowledge participants’ time and labour, but it felt uncomfortable to pay participants, as payment becomes a symbol of our own privilege in our position as researchers in the project.
Issues around decision-making and power also became sticky to navigate. We wanted to address issues of power by using an approach where participants shaped the research methods used, but this did not work how we hoped. Participants advised us on which methods to use to gather data from other people using the service. We decided to use questionnaires as women felt this method would be less time consuming and less intrusive than interviews or focus groups. We provided questionnaires with return envelopes to the family centre staff who agreed to sit with women, if they wanted, whilst they completed the questionnaire. They sent the questionnaire to 14 people but received only one response despite our efforts to follow-up. We also struggled to recruit for the focus group meaning we had two participants.
This struggle to reach participants felt difficult to address and explore. We followed guidance from the study advisory group, but it had not produced the outcome we hoped. Through dialogue with the study advisory group, and from our own observations, we were able to understand broader barriers to participation, which highlighted broader barriers to accessing the service we were evaluating. The women felt that it takes time to build trust and that sometimes you are ‘not ready’ to talk. It is also possible that some people may not wish to participate, or might not be in a place where participation is possible or meaningful to them. It is common to experience challenges recruiting participants who are at a vulnerable time in their lives, and there are ethical implications for doing so (Smith, 2008). Being asked to complete evaluations or feedback forms might be overwhelming or burdensome. Our struggle to recruit participants from the wider service highlights these challenges. While the research had not progressed as planned, our dialogues with the study advisory group deepened our insight into these challenges.
Due to the social inequalities and barriers faced by the women, we felt it was important we did what we could to provide participants with the resources they needed to make participation possible. However, as argued by Janes (2015), no matter what kind of material compensations are provided to participants, researchers cannot change the unequal power sharing between researchers and participants. Researchers can be criticised for using colonising research practices where they go into communities, take the data they need, and leave – sometimes referred to as a ‘helicoptering’ (Mayan and Daum, 2016). Janes notes even with efforts to power-share, ‘working with community may be neither emancipatory or egalitarian, but complicated and colonial’ (p. 75). Even with openness and humility, researchers do, to varying degrees, assert epistemic dominance over participants due to our academic training and our institutions’ taken for granted assumptions about what counts as trustworthy and reliable knowledge (Gullion and Tilton, 2020). Theoretically, participatory approaches can resist positivist assumptions of objectivity and neutrality and they aim to embrace an epistemology of multiplicity and relationality, but in practice, they can still fail and fall short (Wagner et al., 2016).
Conclusions and recommendations
This article has provided an account of our experiences of a small-scale participatory group project to evaluate a perinatal wellbeing service in a deprived area of Scotland. Establishing a study advisory group provided opportunities to engage with women’s lives and stories in a way that enriched the study findings, and in a way that participants felt enriched their sense of community and wellbeing. In some ways, the study advisory group became an extension of the perinatal service and the interventions within it. This blurring of intervention and research boundaries presented ethical tensions which institutional ethics review boards could be better prepared to support researchers to attend to, for instance, by a values and relationship-led approach to democracy, community and power hierarchy. This blurring of boundaries, whilst presenting ethical tensions, can also be considered as offering meaningful sites of knowledge and insight. We recommend that particularly if the researcher(s) also have therapeutic training and skills, these can be a welcome skillset and also a positionality to be aware of through reflexive practice.
Drawing on feminist values and narrative psychology, participatory methods can facilitate the re-storying of the self in potentially useful ways. Peer interviews and group participation may provide opportunities for participants to draw on experiential knowledge, enabling participants to offer lived experience-based challenges that can facilitate the re-storying of the self. In the context of perinatal wellbeing, which we situate in broader socio-structural conditions of social injustice and marginalisation, collaborative methodologies can resist postpositivist epistemologies and embrace an epistemology of multiplicity, recognising the value of multiple sources of knowledge. The group research process also speaks to aspects of group and community healing and solace, in terms of relational and dialogical identity construction, narrative meaning-making and survival. However, we have explored the limitations of our attempts to adopt a participatory approach, as we have grappled with power and its implications for methodology and epistemology. While study advisory group involvement felt successful for the purpose of this evaluation, wider involvement from centre users was not achieved despite using methods suggested by participants. This was difficult to navigate. We suggest that researchers commit to continued and ongoing reflexive practice around decision-making and epistemic power, continuing to reflect on who is making the methodological and analytical decisions, what will happen if there is disagreement between researchers and participants, or between participants, and how to discuss what happens when the research does not go to plan. Additionally, naming and the use of pseudonyms speaks to issues of voice and power. Researchers are ethically bound to protect participant identity, but also to engage with participants over how pseudonyms are chosen. This is part of a larger dialogue about the rights of participants to choose how they wish to be represented in published research outputs.
One alternative to research practices which may be colonising or ‘helicoptering’ may be to avoid going into communities at all. However, this may further marginalise and exclude some already marginalised communities from research. We align our argument with existing community-based and feminist participatory research scholars, by suggesting that community-led or defined research aims and priorities could help to address this. Specifically, a reflexive, community-oriented and flexible approach to participatory methods, particularly with people who are dealing with circumstances that require care and sensitivity, is necessary. We suggest that reflexivity embracing and engaging with issues relating to power may support researchers to stay with difficult dilemmas and decisions. This commitment to reflexive relational practice may assist researchers in navigating the ethical, methodological and epistemological complexities and tensions associated with participatory methods that seek to collaborate, address power, and resist colonising practices whilst acknowledging that we cannot leave academic training, practice training, personal experiences and institutions at the door.
Footnotes
Acknowledgements
We express our deepest thanks to the people who participated in this study, particularly those who participated in the study advisory group. We also thank staff at the family centre we worked with who made the project possible. Finally, we thank the Centre for Child Wellbeing and Protection at the University of Stirling, for supporting our work on this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was commissioned by Quarriers, who received funding from Comic Relief and the Tampon Tax Fund. For the purpose of open access, the authors have applied a Creative Commons Attribution (CC BY) licence to any Author Accepted Manuscript version arising.