
Abstract
Introduction
The transition to motherhood, although usually depicted as a joyful experience, is a sensitive period for the development of mental health problems due to the significant challenges it presents to new mothers. 1 Post Partum Depression (PPD) is the most common complication during this period, pre-pandemic studies show an incidence that ranges from 6.5% to 25%.2,3 However, the prevalence of PPD increased significantly during the pandemic in Chile 4 and worldwide.5,6
As PPD has negative consequences for womeńs well-being and for infant development, 7 several face-to-face and internet-based interventions have been developed to treat and prevent this mental health problem.8,9 Online psychological interventions can overcome limitations that prevent postpartum women from participating in one-on-one, face-to-face consultations, such as time, childcare issues, or geographical restraints.10–12 Women also value the anonymity and privacy of these interventions, as they may be susceptible to the stigma associated with experiencing depression or anxiety symptoms during a period that is culturally presented as joyful.11–13
The use of internet-based therapies for mental health issues is accepted as both feasible and effective.9,14–17 Meta-analyses suggest that online interventions may effectively reduce depression and anxiety symptoms in perinatal women, and high levels of satisfaction have been reported toward these types of interventions.9,10,15,16 Internet-based Interventions can be automated (i.e., unguided) or include some form of human support (i.e., guided). This support is usually provided through a messaging system, such as email or chat, synchronously or asynchronously. Most of the evidence available in this area comes from research on self-help approaches, where participants are provided with a web-based, self-help program and have limited but regular contact with a therapist. This “therapeutic guidance” often includes a therapist providing weekly written feedback via email and allowing participants to ask questions.18,19 Evidence has shown that guided online interventions for depression result in better adherence and outcomes than unguided ones.19–22 Also, reports of participants’ perspectives suggest that they value this support and can even perceive a strong therapeutic relationship towards the facilitator of the intervention.11,23,24
Although therapist or/and counsellor's communication may play a significant role in guided internet interventions for mental health problems,25,26 studies on this topic are scarce. 27 Moreover, there is no consensus on the most appropriate way to measure such communication. To our knowledge at least three ways have been used, these include: a) identifying and count specific words, such us pronouns, negations, positive and negative emotion, etc.; 27 b) identifying content categories based on input from written communication between participants and therapists in online therapy programs for anxiety and depression26,28,30 and c) using a coding system based on the performative notion of language, which states that language is not only a reflection of reality but also constitutes part of it, 31 meaning that to say something is to do something. 32
For instance, Efe and cols 27 used the word count approach when studying a German messenger–based psychosocial chat counselling service for children and adolescents. The authors reported that positive and negative emotions, insight, negations, and causation words had very low frequencies (i.e., less than 5%). They also found that increased use of first-person singular pronouns, negations, and negative emotion words was positively associated with the presence of psychiatric symptoms, whereas increased use of first-person plural pronouns and causation words was negatively associated with the presence of these symptoms.
Interestingly, most of the studies analysing the written communication content categories focus on the client's written messages to the therapist and their relationship to outcomes.28–30 For example, a linguistic analysis of communication in therapist-assisted, internet-delivered treatment, conducted in Canada by Dirkse and cols. reported that clients used words of unpleasant content (i.e., indicative of anxiety and negative emotions), and that their use decreased throughout the treatment. 33 Also, they reported that negative emotion words (i.e., hurt, ugly, nasty) significantly covaried with self-reported symptom ratings over the course of treatment, indicating that increased use of any of these word categories was associated with heightened depression, anxiety, and panic symptoms. Likewise, the results of Svartvatten and Cols. suggest that text messages dealing with the therapeutic alliance, as well as texts that refer to positive consequences for behavioural changes, can be used as indicators of treatment progress. 34
Studies on therapist or counsellor behaviour and communication often focus on the types of interventions used rather than how the former communicates with the client. For example, in Sweden, Paxling and cols’ examined the content of therapist emails in an internet-delivered, cognitive behaviour therapy for generalized anxiety and found eight different therapist behaviours: deadline flexibility, task reinforcement (i.e., reinforcing assignments already completed by the participant), alliance bolstering (i.e., including non-treatment specific writings that pertain to interest in the participant's life situation and care for his/her situation), task prompting, psychoeducation, self-disclosure, self-efficacy shaping, and empathetic utterances (i.e., writings that attempt to convey understanding and empathy for the participant's suffering, frustration or general life situation). Task reinforcement and prompting, self-efficacy shaping, and empathetic utterances were related to higher completion of the intervention's modules. 35 In a later study developed in Canada, Schneider et al. (2016) identified the presence of the same eight therapist behaviours plus three additional ones: administrative statements, questionnaire feedback, and asking clarifying questions. This research found mixed results regarding to participant outcomes. Some therapist behaviours -alliance bolstering, deadline flexibility, psychoeducation, and task prompting- were associated with worse participant outcomes, such as increased symptom severity at posttreatment. However, giving feedback to clients about symptoms or other submissions and their meaning (i.e., “questionnaire feedback”) was associated with a positive outcome. This behaviour and task reinforcement were associated with higher participant ratings of the therapeutic alliance. 36 In summary, therapist texts aim to prompt interventions with empathetic content, such as positive reinforcement of desirable and healthy behaviour in the client and conveying empathy and understanding for the participant's difficulties, suffering, or life situation, have shown to be key factors in promoting positive therapeutic outcomes in internet-based interventions.35,36
Lastly, studies of verbal communication in face-to-face psychotherapeutic interventions using a coding system that assumes the performative notion of language (communications actions), indicate that some communication styles are associated with subjective change and positive therapeutic outcomes in Chile.37–39 and internationally.40,41 These studies show that during interaction segments of psychotherapy sessions where a client's positive change occurs, the therapists have a propositional discourse, characterized by frequent use of assertions and questions and low use of negations. 37 Also, therapists re-signify and attune more with their clients, which means they understand, provide feedback, and align themselves with the contents verbalized by the client. This is relevant, because attuning with the patient discourse is significantly more frequent in successful than in non-successful therapies. 42 Additionally, within this communication style clients are more likely to provide information, clarify, or direct their attention toward specific contents of the conversation,38,39 which promotes positive change.
As discussed, research on text messaging has mainly focused on “what is said” in a therapeutic context and not on “how it is said” or the purpose behind it, which would address communication as a “Communicative Action”. Also, to our knowledge there are no studies investigating communication actions in counsellors’ messages in guided, preventive, mental health, internet-based interventions; thus, many questions about this style of communication remain to be answered.26,27 Conceiving communication as a “Communicative Action” allows accounting for “how things are said”, capturing how the communication objective of the therapist and/or counsellor, who provides the human support during the therapeutic and/or clinical intervention, operates. This line of research can offer clinical insights, for example, to help therapists and/or counsellors by providing information on what type of communication is likely to be helpful or unhelpful, thus serving as a guide for future interventions involving written communication with clients.25,26
The current study analyzed written messages from the counsellor to the participants in a feasibility-controlled trial of a 5-week, guided, internet-based intervention oriented to prevent the development of symptoms of depression and anxiety in first-time mothers. 43 The study was exploratory, and its objectives were: To describe the formal structure of the communication (Basic Forms) and the communicational intentions (Communicative Intentions) used in the messages sent by the counsellor; and determine if the characteristics of the counsellor's language were related to the post-intervention's outcomes.
Material and methods
Participants
The current study is part of a feasibility trial of “m-What Were We Thinking” (m-WWWT) a digital intervention to prevent anxiety and depression in first-time mother. 43 Participants were adult (>18 years), first-time mothers to a healthy infant between 4 to 10 weeks old, who received health care in the primary public health system in Santiago, Chile. To be eligible for the study, women had to have access to a mobile phone with an instant messaging service (i.e., WhatsApp) and be fluent in Spanish. Exclusion criteria included presenting severe mental health problems (i.e., schizophrenia, actual substance abuse) and/or psychosocial problems (i.e., the victim of domestic violence, cognitive disability), as reported by the psychologist of the health centers where recruitment was conducted. Additional information concerning client recruitment and screening can be found elsewhere.43,44 The study was registered (Clinical Trials.gov registration ID: NCT04847076) and was approved by the Ethics Committee of the Eastern Metropolitan Health Service, Santiago. All participants included in the feasibility trial provided their digital informed consent form and were randomized to an m-health preventive intervention (intervention group, IG, n = 59), or a waitlist (as a control group, n = 57). For the current study, only the 53 participants in the IG that received at least one personalized WhatsApp message from the intervention counsellor were included.
Intervention & feasibility results
“What Were We Thinking” (WWWT) is a psychoeducational, preventive intervention for both parents of first babies that targets modifiable risk factors for the development of postnatal symptoms of depression and anxiety in first-time mothers. Its aims are to promote confident parental caretaking, optimize functioning in the intimate partner relationship, improve infant manageability, and reduce common postnatal mental disorders in women.45,46 For example, the counsellor provides parents with practical support and strategies for managing problems that may emerge during the postpartum period, such as sleep deprivation and crying. 46 WWWT has been culturally adapted to the Chilean context45,47 and has been modified to be delivered as an m-health intervention (i.e., m-WWWT).
The m-WWWT intervention includes three components (see Figure 1):
Psychoeducational information about infant care and the interpersonal challenges women and their partners – if present- face during the transition to parenthood. This information was delivered in 14 modules involving a 3-to-5-min video and an invitation to read some questions to promote self-reflection. The modules were delivered by the program counsellor three times a week for a five-week period using a messaging service for mobile phones (WhatsApp). Individual contact with the program counsellor to ask questions that arose from the psychoeducational modules and share their personal experiences. Women initiated contact voluntarily, and the counsellor tailored the answers according to womeńs needs. The counsellor responses focus on promoting the understanding and elaboration of the contents and providing emotional support. Participant-counsellor interaction was conducted via WhatsApp. A group, 1-h virtual meeting with the program counsellor to offer the participants and their partners (or support person) the opportunity to share their experiences about parenthood (see Figure 1). A detailed description of the m-WWWT intervention has been published elsewhere43,44

Components of m-WWWT.
Coo et al. (2023) reported that m-WWWT is feasible for implementation and has high levels of acceptability from the participants’ perspective; even though preliminary effectiveness was not supported. All communications between the users and the program's counsellor were established through instant messages. Mothers who participated in the feasibility trial of m-WWWT reported that the counsellor responded promptly, providing a space to address their doubts, and giving clear and empathic responses. Also, participants described her as close, affectionate, and proactive in her communication. Lastly, the women mentioned that the messages provided emotional support and positive feedback regarding their feelings of isolation and loneliness during the pandemic-related confinement and their worries and insecurities about being a mother, which contrasted with their idealized vision of motherhood. 43
Intervention counsellor
The counsellor was a psychologist with experience in clinical and psychoeducational interventions for perinatal women. She was trained in the intervention model and had previously facilitated the WWWT psychoeducational intervention in its original face-to-face format.
Procedure
The counsellor's communication with the intervention's participants included two types of messages: standardized and personalized. The standardized messages were sent to all participants and were accompanied by a psychoeducational video. Standardized reflective exercises were suggested, along with questions about possible doubts and/or difficulties about the intervention content which participants could experience. For example, the counsellor would greet the participant before sharing the educational video. After each specific video, she would send a standardized message such as “Was the information in the video useful to you? Do you have any doubts, concerns, or difficulties you would like to share regarding this topic?”. The language used varied to offer a more humanized interaction. Participants could then respond to the counsellor by sharing their questions, reflections, or experiences via instant message. The personalized messages which were analyzed in the current study, were the counsellor's responses to the questions and experiences shared by the participants and had the purpose of offering educational information as well as socioemotional support. The content and quantity of messages were specific to each participant.
The messages were transcribed literally, preserving the structure of the conversation. Although in the present study only the messages from the counsellor to the participants were analyzed, the participants’ statements were considered during the coding process so as not to lose the dialogue meaning. Following the procedures of the SCAT-1.0 coding system, each instant message was coded in its Basic Form (BF) and Communicative Intentions (CI). Each message was divided into segments depending on whether the BF or CI changed along the message text, thereby the number of message's segments depended on the use of different FB and CI, and not by its sentence's length. Specifically, a segment within a message corresponds to a subunit of the text with a specific BF and a specific CI. The variation of the BF or CI in the text generates a new segment. For example, if a message has one BF and one CI, it has only one segment, but if it has two BF and the same CI, there are 2 segments; if what varies is the CI and the BF is maintained, there are also 2 segments. 48
The application of SCAT-1.0 requires expert coders, with theoretical training in the instrument and experience in coding therapeutic communication. In this study, 2 expert coders from the research team (NA, OF), who are psychologists with a PhD. degree and high proficiency in utilizing TACS-1.0, performed the coding independently. To determine the inter-rater agreement, 360 message segments (55% of the total) that had been independently coded were taken. Cohen Kappa was k = 0.85 (p < .001) for BF and k = 0.80 (p < .001) for CI, indicating an adequate level of reliability. Differences in coded segments were reconciled through intersubjective agreement between coders. If agreement was not obtained, the segments were submitted to a triangulation process with a third researcher of the team (SF), until intersubjective agreement was reached.
Instruments
Communicative Actions. The Therapeutic Activity Coding System (TACS-1.0) 49 was developed to manually code patients’ and therapists’ verbalizations during relevant episodes of face-to-face psychotherapies. It is a coding system based on speech acts theory,31,32 and it has a performative notion of language. This notion states that language is not only a reflection of reality but also constitutes part of it, 31 in the sense that to say something is to do something. 32 It includes three “action” domains, namely Basic Form (BF), Communicative Intention (CI), and Technique, and two content codes (i.e., Domain and Reference). In this study, only BF and CI were used. The BF captures the formal structure of the utterance, distinguishing between the following communicative actions: “agreement”, “assertion”, “denial”, “question” and “direction”. CI accounts for the communicative purpose of the person's verbalization, that is, what the speaker wants to achieve with it. It includes “exploring”, “attuning”, and “re-signifying”. 49 The categories’ description and their examples are presented in Figure 2.
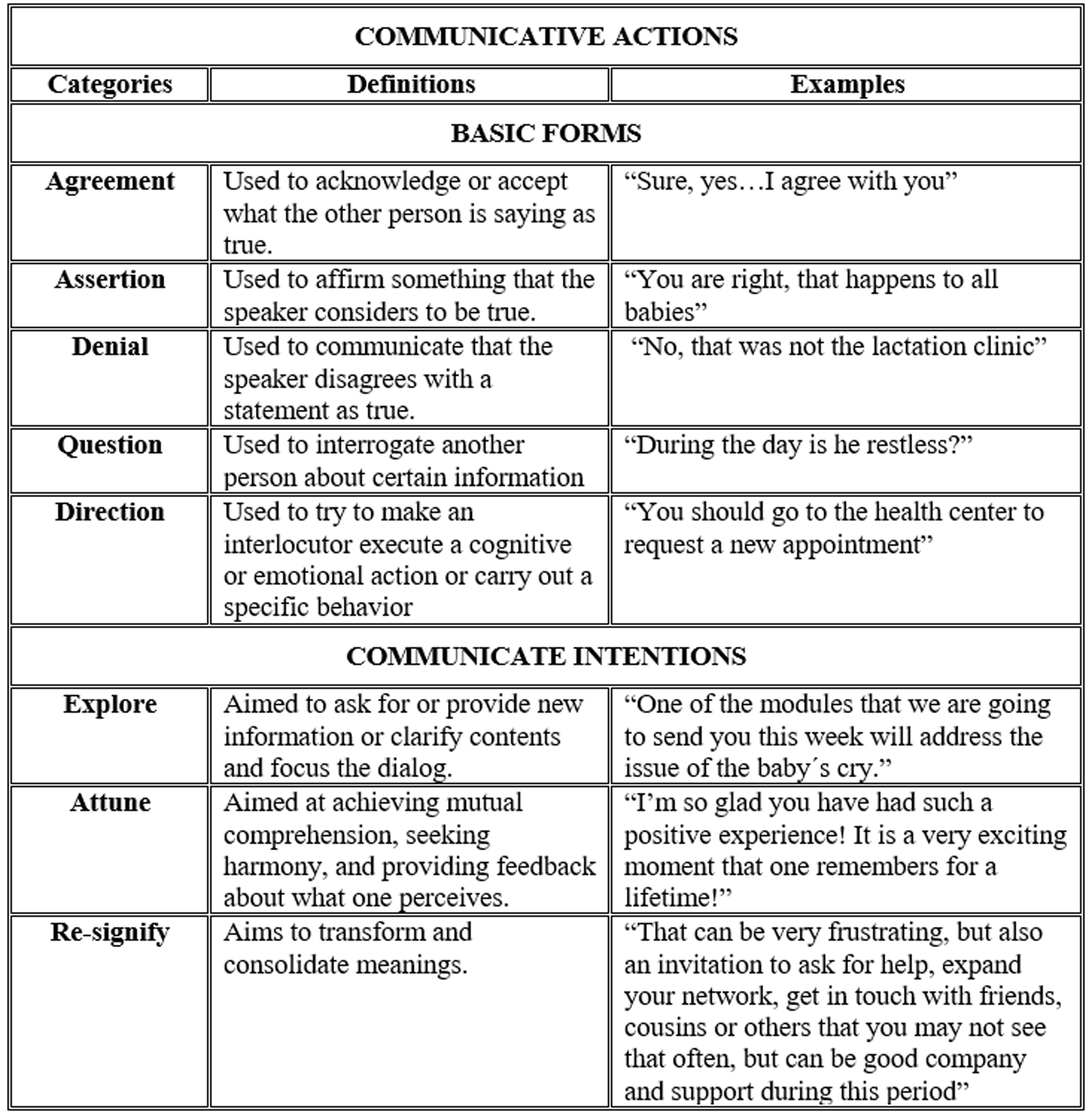
TACS’ Basic Forms and Communicative Intentions categories.
Edinburgh Postpartum Depression Scale (EPDS). 50 It is a 10-item self-report instrument that screens for symptoms of depression over the past week using a 4-point scale (scale range 0 to 30). Higher scores are indicative of a higher risk of presenting postnatal depression. The EDPS has been validated in Chilean populations. 51 This scale was applied pre- and post-intervention.
The Perinatal Anxiety Screening Scale (PASS). 52 It is a 31-item self-report questionnaire that assesses maternal anxiety during the past month. The scale uses a 4-point Likert scale (0 = Never – 3 = almost always; scale range 0 to 93), with higher scores suggesting higher anxiety. The PASS has been validated for its use in Chilean mothers. The Spanish version of the instrument has good psychometric properties and includes four subscales: general worry and specific fears; social anxiety; acute anxiety, adjustment difficulties and trauma; and perfections and control. 53 This scale was applied pre- and post-intervention.
The Multidimensional Perceived Social Support Scale (MSPSS). 54 It is a self-report instrument with 12 items organized in 3 subscales that address perceived social support from family, friends, and significant others. Items are rated on a 7-point Likert scale (1 = very strongly disagree; 7 = very strongly agree), with higher scores suggesting higher perceived social support. The MSPSS has been adapted to be used in Chile55,56 but not specifically in perinatal populations. This scale was applied pre- and post-intervention.
The Parental Evaluation Scale (PES). 57 It is a self-report questionnaire that includes ten items rated on an 11-point scale (0 = strongly disagree; 10 = strongly agree, scale range 0 to 100) to measure motherhood-related satisfaction and self-efficacy. This scale was applied pre- and post-intervention.
Demographic and obstetric information. A questionnaire was developed to assess the participant and children's sociodemographic characteristics at the beginning of the m-WWWT intervention.
Statistical analysis
We used descriptive statistics (i.e., means and SD for continuous variables and percentage for categorical variables) to explore the sample characteristics and units of analysis. As a preliminary result, the correlation between the counsellor’s number of messages and maternal characteristics was estimated used non-parametric tests (i.e., Spearman correlation coefficient, Kruskal-Wallis test, etc.) because the assumptions required to conduct parametric analyses were not met.
To account for the first article objective, we conducted a descriptive analysis (frequency and percentage) of each one of the communication actions in the written communication from the counsellor towards the participants. Although this allows the identification of the frequency with which single communication actions are used, most of the communication involves a joint use of FB and IC Thus, to capture this pattern we identified attractors. Theoretically, attractors are recurrent states that occur more frequently than others, or which are difficult to swap for other states.58,59 This means, identifying the most frequently used combinations of BF and CI based on the number of events in which a certain BF and CI occurred simultaneously.
To do it, once SCAT codes were obtained, this database was imported into the GridWare SSG software. 60 The SSG allowed the joint analysis of the data, considering both the BF and CI throughout the messages. As shown in Figure 3, the X-axis represents CI categories, and the Y-axis represents BF categories. In this sense, an attractor was defined as that cell (or quadrant) with the most significant number of “events” within the 15 possible combinations of language use. An “event” is a distinct episode occupying a particular cell, with an onset and an offset. 59 Attractors in this state space were identified through a winnowing procedure, which is an iterative procedure using the average number of events of all the messages in each of the occupied cells. Expected values were calculated from the number of total mean events divided by the number of cells (as used in Chi-square calculations), and the sum of squared deviations (observed minus expected, then squared) was divided by the number of cells in the analysis to obtain a heterogeneity score. Each winnowing run denoted the grid cells with the greater number of events which removal decreased the heterogeneity score. After the steepest drop in heterogeneity (scree value), the remaining cell or cells comprise the attractors.61,62 In this study, the two cells of BF/IC with the higher mean events were considered attractors.

Basic Forms/Communicative Intentions Attractors in counsellor messages.
Lastly, to account the second article objective, Spearman correlations were estimated between the event score of the two BF/IC attractors and change scores of outcome variables (symptoms, social support, and parental self-efficacy); due to the non-normal distribution of the former variables. The BF/IC attractor’ score were adjusted to control their correlation with the number of messages sent by the counsellor (assert to attune: r = .89, p < .001 and assert to explore: r = .66, p < .001). These attractor scores were transformed by dividing the total number of segments, indicating the proportion is which a certain communication pattern was used (i.e., 0.10 = in one out of every 10 message segments a certain BF/IC pattern was used vs 0.90 = in 9 out of 10 message segments a certain BF/IC pattern was used). Score changes were calculated to capture improvements from basal to post-intervention in all variables, a positive score change refers to improvement (i.e., increase in parental self-efficacy) and a negative score change to deterioration (i.e., increase in reported depressive symptoms or decrease in parental self-efficacy).
Results
Participants demographics and basal measurement
The 53 participants who received at least one personalized WhatsApp message from the m-WWWT counsellor had a mean age of 25.36 (SD = 4.16) years. All of them were Latin American and the great majority (87.3%) was Chilean. Most participants (52.7%) were unmarried but cohabited with their partner and 49.1% had a paid job. Most women (74%) referred that their pregnancy was unplanned and 49.1% of them had a cesarean section. Most of their infants were male (52.7%). Please see the original trial for a detailed description of the whole sample. 43
The 53 mothers reported mean scores of the EPDS (i.e., depression) of 8.15, SD = 5.01) and of 28.81 (SD = 20.45) in the PASS (i.e., anxiety). The average score for parental self-efficacy was 74.26 (DS = 16.91) points. Regarding social support, the average for the family network was 13.60 (DS = 2.90) points, and the mean scores for friends and others were 11.60 (DS = 4.37) and 13.83 (DS = 2.28) points, respectively.
Unit of analysis
The counsellor sent a total of 438 messages to 53 participants. The participants received 7 messages as a median (IRQ = 9), with a minimum of one and a maximum of 55 messages. The counsellor's messages had different lengths depending on the participant's query. We divided the 438 messages into 652 segments. Messages had a median of 1 message segment (IRQ = 1), with a range of 1 to 6 segments each.
Preliminary analysis: association between the counselloŕs messages number and maternal characteristics at the beginning of the WWWT intervention
The number of messages sent by the counsellor in response to the participant messages was not associated with the participants’ self-reported mental health symptoms, perceived social support, or parental self-efficacy at baseline (-.08 < rs < .20, all p > .05), nor with the participantś age (rs = -.24, p = .08) or relationship status, KW = 2.62 (1 df.), p = 0.106. However, a significant association was identified between the educational level of the participants and the number of messages received; the counsellor sent more messages to participants who had less schooling, KW = 6.72 (2 df.), p = 0.035. The median number of messages was 10, 7, and 2 messages per participant with primary or secondary education, higher technical education, and higher university education, respectively.
Description of communicative actions
The BF most frequently (82%) used by the counsellor was assertion. For example, the counsellor comments to the participant, “Colic can be a very challenging issue, and it can cause a lot of discomfort in babies”. The BF of question was used in only 10% of the segments. The other BFs were rarely used by the counsellor (“agreement” = 2%, “denial” = < 1%, and “direction” = 5%).
Regarding the CI, the counsellor attuned in 52% of the message segments and explored in 39% of them. Examples of these CI are “I know how difficult waiting is” (in response to the participant's concern on the necessity of waiting for an inter-consultation for her child) and “There are certain routines that can help a little to have a calmer first part of the night, for example, giving him a long bath and then a massage”, respectively. The counsellor re-signified only in 9% of the message segments, saying for example, “In this period it is so important for both parents and babies to be able to rest enough”.
The attractors of the Space State Grid were identified to determine the most frequent communication patterns in the message segments written by the counsellor, considering both the BF and the CI. These results indicated that two attractors characterized the communication: a) The use of assert to attune with the participant, and b) assert to explore (see Figure 3). Although questions to explore were frequently used by the counsellor, this communication pattern did not constitute an attractor.
The communication pattern “asserting to attune” captures the certainty with which the counsellor expressed herself, mainly to make the participant feel validated and understood regarding what is being expressed; and -in other occasions- to offer or clarify information, or to motivate the participant to elaborate on what has been stated. Examples of this communication pattern are: “I am so glad you and your partner are both enjoying your little one and working as a great team in this beautiful and demanding period”, or “Although motherhood […] can make us face situations in which we can feel pushed to the limit. Whether due to lack of sleep, physical or psychological discomfort, as you have shared with me”.
The communication pattern “asserting to explore” captures that the counsellor expressed with certainty when providing -or asking- new information or when clarifying contents and focusing the dialog. Some examples of this communication pattern are: “It is natural for babies to want to sleep next to or on top of their mother; it is where they feel most secure. As he gets older, it will be easier for him to be apart, but it is a slow process. If you are getting enough rest and it does not bother you to have him in bed with you, don’t get frustrated if it doesn’t work for you to leave him in the crib for long periods; it is very common for this to happen”.
Association between counsellor communications and intervention outcomes changes
The number of messages sent by the counsellors to the participants was not associated with a change in maternal mental health symptoms, perceived social support, or parental self-efficacy reported by the participants. (-.11 < rs < .20, all p > .05).
Regarding the BF/IC attractor's score, the results indicated that more frequent use of “assert to explore” increased change in parental self-efficiency in the participants. In other words, more “assert” messages sent by the counsellor that provided information and clarified doubts about the womeńs concerns and actions, were related to an increase in parental self-efficacy. As the following message addressed to one of the participants illustrates: “It´s normal to see variability between each night and between babies. Some babies have many awakenings during the night, and others can sleep through the night at earlier ages”. No other significant associations were found (see Table 1).
Counsellor-participant communication and associated change in maternal mental health symptoms, social support, and parental self-efficacy.

Note. aAttractor indicators were transformed by dividing the total number of segments, indicating the proportion in which a particular communication pattern was used.
* p < .05
Discussion
The present study is – to our knowledge – the first to account for the quality of verbal communication (“how it is said”) expressed through text messages written by the counsellor of an m-Health intervention in response to the spontaneous messages of women involved in a preventive program for postpartum depression.
Understanding verbal written interactions between clinicians or counsellors and clients in the context of therapeutic and preventive interventions is essential for comprehending psychotherapeutic-related processes and identifying effective verbal interactions. This insight is particularly relevant in the digital era, where interventions often occur remotely and rely on textual communication. While prior research has highlighted the importance of relational and subjective aspects in the communications in psychological interventions, exploring these dimensions further remains crucial for enhancing adherence and outcomes in text-based therapeutic or preventive interventions.
Our results indicate that in the dialogue with the first mother, that assertion was the most frequently BF used by the counsellor (82%), followed by question, while others BFs were rarely used. The predominant use of assertion could reflect an assertive way of communicating from the counsellor, which conveys certainty without ambiguity. It may be possible that new mothers need a counsellor to “guide” them with certainty, and to diminish their uncertainties and insecurities that accompany the new experience of parenting. It seems that the counsellor assumes a role of directive care in her communications, comparable to a “parental supportive” role, promoting a secure environment for the mothers in this moment of highly emotional demand. On the other hand, assertive BF can also be linked to the expert role acquired by the professional in helping relationships, who is socially recognized in this role, 63 which confers an asymmetric characteristic to the relationship, 64 allowing her to exercise influence and persuasion on others.
Greater heterogeneity was found with respect to IC, with attuning being the most frequently used, followed by exploring. The use of attune’ IC in the texts would indicate that the counsellor intends their dialogue to express mutual understanding, acceptance of emotions, and create an atmosphere of trust between the participant (i.e., the mother) and her. On the other hand, the explore IC, which consists of both asking for or providing new information, may reflect an assertive desire to learn about the other's experience, as well as to provide information tailored to the mothers’ needs.
In addition, when considering the BF and CI together, our results indicate that two attractors stand out more in the therapist communication: the use of “assert to attune” and the use of “assert to explore”. The attractor “assert to attune”, describes a way of communication that validates with firmness (or certainty) the feelings and experiences lived by the mothers, giving confidence, and understanding to her subjectivity. In fact, this BF/IC pattern could emulate the “empathetic content” category of Paxling et al. (2013) and Schneider et al. (2016) studies.35,36 From this perspective, the counsellor's communicative style could be described as assertive, emotionally attentive, and sympathetic, which provides security and calm to the participant while generating an experience of being accompanied and understood. This could be comparable to fulfilling the holding function 65 or the mentalizing function of the mother. 66 Perhaps it is a communication style that favors the development of a digital therapeutic alliance. 67 Thus, the quality of the counsellor's communication would allow the participants to generate a relationship or bond with him/her. It is possible that this attractor could be at the basis of participants’ perception of the counsellor as “welcoming, affectionate, close, and being caring”, who “offers clear and empathic responses”. 43
The attractor “assert to explore” describes a way of requesting and delivering information in an assertive way, which transmits reliability and security to the interlocutor. In this research this communicating form was related to an increase in parental self-efficacy, indicating that this type of dialogue empowers the mother in her parenting skills. This finding is consistent with other studies that address the association of the content of therapeutic communication with the results of the interventions, indicating that only some of them are directly related to better therapeutic results.35,36 In fact, given that new mothers are highly demanded by parenting and emotionally sensitive, they need to receive information, clarification, and affirmation of their experience, which orients and validates their role. This form of communication would facilitate the achievement of learning in a psychoeducational intervention that hopes to achieve significant learning in the participants. 68
It is important to mention that the intervention group of m-WWWT did not show changes in parental self-efficiency compared to the control group, but post-hoc analyses indicate that a subset of participants who received the m-WWWT benefited from it showing an increasing in their level of parental efficacy. 43
From a sociocultural perspective it is important to consider where the counsellor-mother communication takes place. Specifically, while developing rapport is a critical aspect to the treatment of all populations, it acquires a more relevant role in the interventions with Latino populations, for whom some of their components are influenced by important cultural concepts. 69 Personal relationships are valued in Latin culture, where warmth and engagement with others are considered vital to fostering interpersonal relationships and qualities sought in their treating clinician.69,70 In fact, in Chile and other Latin American countries, most of interventions for the prevention and treatment of mental health pathologies based on technologies are less effective than in other contexts, such as North America and Europe.71–73 Given the contextual and cultural specificities of the Latin American population, future studies should explore in detail how important human support is for this populations to increasing engagement and adherence as well as improving outcomes in online interventions.
Additionally, our results indicate that the counsellor established contact in response to the participants’ messages with 96% of the participants, who received, on average 8 to 9 personalized messages. This information could be useful as a proxy of use. As most of the participants used this component of the intervention, thus overcoming one of the main problems presented by interventions measured by associated technology: the participants’ limited use.47,70 Different causes could explain this result. First, the m-WWWT allows two-way communication, in which either the counsellor or the participants can initiate a conversation. In fact, the counsellor frequently approaches the participants through the questions accompanying the delivery of the psychoeducational material. On the other hand, the communication style described above, fosters the establishment of this digital therapeutic alliance, 67 which might explain the high rates of the individualized communication component of the intervention. This is especially interesting because there is no face-to-face contact, and all communication between the counsellor and participants was written.
The number of messages sent only showed a significant association with participants’ education, with those who had lower educational levels receiving a greater number of messages. This finding is promising, to the extent that it is these participants who could benefit the most from preventive interventions such as this one, which seeks to promote confident parental caretaking, optimize functioning in the intimate partner relationship, improve infant manageability and reduce common postnatal mental disorders in mothers. 46 This is particularly relevant when considering that lower socio-economic status has been associated with lower parental self-efficacy in mothers. 74
Our results should be considered in the light of some limitations. Firstly, only the counsellor WhatsApp messages were analyzed in this study, and participantś messages were only read to give context to the counsellor communication. It is possible that the identified attractors are responses to the content of the participant messages, thus future studies could analyze both counsellor and participantś messages. Also, the messages analyzed in this trial came from only one counsellor and it is not known whether these communicative patterns can be generalized to other facilitators of the intervention. Considering that the intervention had a duration of 5 weeks, the temporality of the messages sent was not considered. In addition, the small sample size limits the study's power to detect correlations of moderate (or larger) magnitudes between communication styles and outcome variables.
Nevertheless, to our knowledge, this is the first study in which the counsellor communication in an online preventive intervention is analyzed as communicative actions (i.e., on the base of their performative notion), and where it is association with treatment outcomes was explored. A larger sample size would be of great interest in future research. Additionally, future studies should include different counsellors, and determinate if a specific pattern of communication can be trainable.
Once the usefulness of a communication pattern in achieving the intervention's goals and its trainable nature is established, the use and usefulness of such communication patterns in other guided interventions using instant text messages and/or in other pathologies could be explored.
Conclusion
This research adds to previous studies that have explored written communication in guided, Internet-based mental health interventions, providing findings about the form/style of counselor’ communication: “how it is said”. It's novelty and contribution also rely on addressing communication in a preventive intervention - and not a therapeutic process itself -, revealing that the communication's purpose is relevant in interventions with different aims.
Our results suggest that in this online intervention, an assertive communication style that conveys the intention to understand and empathize with the participants is valued by them and seems to contribute to the intervention outcomes. Using a communication style that allows the counsellor to connect with the specific needs (“assert to explore”) and emotional tone (“assert to attune”) of the participants contributes to the development of an emotionally assertive, attentive, and understanding care relationship with the participant, that can provide a sense of security. This style of communication could be particularly relevant in Latin American contexts.
The results of this research regarding “how it is said” in remote digital interventions solely via text underscores the presence of relational and subjective aspects, such as metacommunication, 75 in such interventions. In current times where digital health interventions are becoming increasingly common, continuously delving into relational aspects is fundamental for improving adherence and outcomes in therapeutic or preventive interventions via text. Understanding the nuances of verbal interactions between clinicians or counsellors and clients in digital interventions not only enriches our comprehension of these processes but also facilitates the training of professionals capable of fostering positive changes in clients.
Footnotes
Acknowledgments
We thank all of those who participated in the m-WWWT trial study.
Author contributions
OF and JCP intellectually designed this study. JCP obtained funding for the feasibility pilot study. SC and MIG adapted the WWWT to mHealth intervention and delivered the intervention. OF, NA and SF coded the instant messages content. JCP did statistical analysis. OF, JCP, NA, SF, PF, SC, MIG, MA wrote the manuscript. All co-authors read and approved the final manuscript.
Author's note
Sofía Fernandez, Facultad de Psicología, Universidad de Valpariso, Valparaiso, Chile.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval was obtained from the Ethics Committee of the Eastern Metropolitan Health Service, Santiago. A modification to the original protocol was approved to collect qualitative data.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Millennium Institute for Research on Depression and Personality MIDAP (Grant ICS13_005) and ANID BECAS/DOCTORADO NACIONAL (Grant–21190745, PF). Funding source had no role in data collection, analysis and interpretation of the results.
Guarantor
JCP
Informed consent
All the participants are asked to provide informed consent before joining the study. The intervention counsellor signed informed consent form. Data will only be accessible to the research team, individual information about participants and potential participants will be confidential and only de-identified data will be available for analyses. Publication of the study results will not include any identifiable information about participants.