
Abstract
This article uses data from a doctoral thesis concerning service users’ views on what works for them in relation to their mental health wellness following a suicidal ideation/attempt in Aotearoa New Zealand. In particular, it focuses on the experiences of service users regarding mental health crisis team responses and what they wanted from their crisis teams specifically. Participants indicated that what they wanted was to feel heard, respected and not judged, consistent with the core conditions of therapeutic alliance within such professions as social work, counselling and psychology. Social work has a valuable role to play in emphasising and advocating for social, contextual and non-medical responses within crisis teams and service delivery.
Introduction
While responses to suicide have been widely explored, very little of the exploration has been influenced by the voices of people who actually experience suicidal ideation, or those who have attempted suicide. Until recently, service users have rarely been involved in mental health policy development or in collaborative design and implementation of research (Phillips, 2006). This article presents the suggestions of service users for what they wanted from crisis teams when feeling suicidal, as a subsection of a study that explored the wider question of ‘what works following suicidal ideation/attempt?’ in Aotearoa. Within the larger study, while some participants recalled some good experiences of working with crisis teams, most expressed having had negative experiences (Ali, 2019; Ali et al., 2021). For some, this involved feeling they were not being heard, or well responded to, in a crisis situation. They often sensed that the crisis workers were too far removed from, and unable to relate to, the participants’ crisis experiences. Participants also reported that crisis teams’ lack of time and resources likely impacted upon their experiences.
The article will provide some context to the study regarding crisis and mental health services in Aotearoa New Zealand, followed by a review of the literature about the roles of crisis teams, crisis team response and support for people experiencing suicidal ideation. Relevant literature about what service users want from crisis services will then be explored. The methodology and results of this research will be presented followed by a discussion of some of the implications and recommendations arising from the study.
Throughout this article, ‘crisis teams’ are used to refer to ‘crisis resolution home treatment teams’ (CRHT) and ‘crisis and assessment teams’ (CAT). The terms ‘mental health workers’, ‘professionals’ and ‘clinicians’ are used to refer to the people who are providing mental health services. When referring to individuals who access mental health services, including crisis services, the term ‘service user’ has been used. Aotearoa is used to describe the country of Aotearoa New Zealand.
Context of the study and literature review
Aotearoa is a country of approximately five million people located in the South Pacific (OECD, 2022a). Māori are tangata whenua (Indigenous people of the land) and the country’s colonisation, mainly by the British, began in the early 1800s (King, 2003). Shaped in part by this process of colonisation, and despite its relative wealth, Aotearoa experiences significant social problems including child poverty, violence against women and children and high rates of suicide (UNICEF, 2020).
Aotearoa’s youth suicide rate is the second highest in the developed world at 14.9 deaths per 100,000 adolescents. This rate is more than twice the average among the 41 OECD countries surveyed (6.5 deaths per 100,000 adolescents) (UNICEF, 2020). The latest figures for the general population reveal a rate of 12.1 confirmed deaths by suicide per 100,000 population in 2018, equating to 623 deaths in Aotearoa. The rate of suspected deaths from mid-2020 to mid-2021 was 11.6 deaths per 100,000 population and has remained consistent over the past 10 years (Ministry of Health, 2022a).
The history of provision of mental healthcare in Aotearoa has followed a similar trajectory to many western countries, in terms of deinstitutionalisation and a move towards community-based care occurring throughout the 1970s and 80s. Aotearoa has had strong representation from service users, with the first service users’ rights group ‘Psychiatric Survivors’, being established in the late 1980s (Scott, 2016). This movement was influential in getting the government to espouse a ‘recovery oriented’ (Anthony, 1993) approach in the 1990s (Mental Health Commission 1998) with a growing recognition of service user rights and participation as well as the need to address the impacts of colonisation on Māori (Ramalho et al., 2022). While service user movements have been influential in challenging, and partnering with, mental health services in the country, these initiatives have yet to be fully realised (Elliot, 2017; New Zealand Government, 2018).
Aotearoa’s mental health system is provided through a combination of public and privately funded care and generally follows a psychiatric, rather than social, model of care (Reed and Field, 2017). Mental health services are delivered initially through general practitioner services with potential referral onward to free community-based secondary treatment (community mental health services) or tertiary treatment within psychiatric hospital wards. In 2022, the country moved to a centralised health service model, Te Whatu Ora, but prior to that the country was divided into regional district health boards, resulting in a fragmented system with variable service provision determined by local need and available resources. Crisis or emergency mental healthcare is usually provided through geographically determined community mental health teams and their attendant after hours and weekend services (Ministry of Health, 2022a). Numerous mental health inquiries – often the instigation for policy change (Elliot, 2017; New Zealand Government, 2018) – have revealed chronic underfunding, long wait times, staff shortages and inconsistencies of crisis response across the country. There is also increasing pressure on mental health support services generally in Aotearoa, including mental health helplines (Lifeline, 2021) and those services provided by crisis teams (McClure, 2021).
Roles, access and availability
Throughout Aotearoa, district-based crisis teams provide emergency support available on a Monday–Friday, 8 a.m.–5 p.m. basis, with a separate phone line for out-of-hours crisis support. Crisis teams aim to provide 24-hour assessment (including risk assessment) and short-term treatment services for people experiencing a serious mental health crisis with associated urgent safety issues. Specialist intervention is provided by crisis teams via home-based treatment as an alternative to hospital admission (Waikato District Health Board, 2022). Crisis teams may be interdisciplinary in nature and can include nurses, doctors, psychologists, occupational therapists and social workers.
Crisis teams have generally arisen out of the community care model of treatment following deinstitutionalisation which occurred in Aotearoa between the 1970s and 2000s (Brunton, 2004). The principal objectives of crisis teams are usually to prevent hospitalisation, act as a gatekeeper to hospital or community mental health services (Morton, 2009) and to reduce risk to self and others. In some instances, they have also been seen as an initiative to move away from more prescriptive use of mental health act legislation (Klevan et al., 2017). The role of crisis teams is sometimes contentious (Klevan et al., 2017), with some people seeing the crisis role being limited to a clinical or medical role (Tobbit and Kamboj, 2011), while others have advocated for a more complex view of crisis response where practical and emotional supports are also provided (Gullslett et al., 2014).
Despite recent proliferation of crisis response services in the United Kingdom (UK), little has been written about how crisis services are organised or how work is done (Hannigan, 2014). There is often a strong medical presence within crisis teams, characterised by nurses often being the most predominant professional group represented. Within the UK, ‘Approved Social Workers’ play an important role in assessment for compulsory treatment, or through ‘matters concerned with service users’ families and finances’ (Hannigan, 2014: 414). In Aotearoa, Duly Authorised Officers (DAOs) are given statutory powers under the Mental Health Act, 1992 (Government of New Zealand, 1992) and are responsible for ensuring that the procedural requirements for compulsory assessment are explained to the service user in the presence of a family member or other caregiver. There is variation around the country about which occupational groups undertake this role, with social workers as a minority profession represented.
In Aotearoa, an individual or their whānau (extended family) can request urgent support from mental health practitioners to conduct an urgent mental health assessment if they believe that the person is experiencing mental disorder as defined by the Mental Health Act 1992 (Ministry of Health, 2022). This assessment may lead to crisis support, including follow-up appointments with a local mental health team (often at home) and, potentially, care from acute inpatient services. Difficulties with these options can arise when those services are underfunded, understaffed and have long waiting lists. As a result, service users may experience unsupportive and unprofessional responses from crisis teams, urgent assessments can be delayed, whānau members may not be listened to and poor standards of care can occur in inpatient units (Ali, 2019; Ali et al., 2021). Home visits by a local mental health team can reduce pressure on hospitals and their inpatient capacity (Jethwa et al., 2007). This ‘at-home’ alternative may mean that access to inpatient care is rationed in times of fiscal constraint. As a result, more people may die by suicide within the community when compared with deaths by suicide when individuals are in inpatient care. Service users, receiving home treatment in the UK, reported that rapid, accessible, crisis-focussed support was an advantage, whereas lack of consistency of staff and appointment unavailability created frustration (Carpenter and Tracy, 2015).
The culture of crisis support services
Crisis workers and practitioners working within psychotherapy, social work and counselling are often influenced by a biomedical model. A tendency for practitioners to define crisis based on particular levels of functioning and a certain set of symptoms (Lyons et al., 2009, cited in Klevan et al., 2018: 255) leads to users receiving mental health services characterised by biomedical/technical practices. As evidenced by the literature, many service users prefer, and report more positive outcomes from, a holistic approach with normalisation of their mental distress. Despite guidelines which support this approach (see Aotearoa’s ‘Let’s get Real’ skills (Te Pou, 2018), many mental health practitioners’ knowledge is largely shaped by institutional practice beliefs. These beliefs, and the dominant culture of the qualified mental health professional, perpetuate the notion of the practitioner as the expert. The use of terms like patient, ill, treatment and expert demonstrate how unaware some practitioners are regarding such ‘competing and often contradictory paradigms, their inscription within them and the connection between language, professional identities and practices’ (Klevan et al., 2018: 263).
These conflicting paradigms can result in labelling practitioners as lacking in empathy and having an insufficient and atomistic understanding of the service user’s life (Smith and Grant, 2016 cited in Klevan et al., 2018: 263). Service users’ understandings of, and preferences for, a helpful culture are likely to be at odds with the dominant technical culture. What might work for them in crisis resolution/treatment/support, what they want and what they expect to receive will invariably differ from what they experience.
This variation between a person-centred approach and standardised, efficient help (Karlsson, 2015) contradicts more than just discourses. According to Klevan et al. (2018), it also undermines the fundamental principle of the importance of developing therapeutic relationships.
What people want from their crisis teams
The way in which practitioners deliver crisis services (process as opposed to content) can significantly affect outcomes. Rather than intervening to restore normal functioning via specific interventions, the non-directive approach of person-centred treatment and recovery can be used to identify a service user’s experience of crisis through empathetic attunement, and subsequently help to move away from the notion of needing to be fixed towards normalisation of the crisis; the practitioner is an equal, not an expert. This is reflective of what service users say that they find helpful, not what they often receive (Klevan et al., 2017; Morant et al., 2017).
Service users have highlighted the value of being visited by a professional when and where they preferred (Winness et al., 2010). Behaviours that promoted equality, responsibility and respect led service users to feel able to follow the process of recovery on their own terms (Hopkins and Niemiec, 2007; Karlsson and Hultberg, 2007, cited in Winness et al., 2010: 80). Consistency of care was also noted to be important where ‘service users and carers greatly valued the same staff visiting them over time, because of the opportunities this provided to develop therapeutic relationships, emotional support and trust’ (Morant et al., 2017: 6).
The importance of demonstration of respect within trauma-informed approaches to mental health service provision has been identified (Sweeney et al., 2018). Traumatic experiences greatly impact on mental and physical health and experiencing trauma is associated with a greater likelihood of attempting suicide, of self-harming, higher levels of prescribed medication and longer and more frequent hospital admissions (Mauritz et al., 2013). Trauma-informed approaches that involve the practitioner offering an understanding and acceptance of the person and their situation have been found to reduce the possibility for further trauma – unjudgmental recognition of the person and their trauma can promote positive change and recovery (Sweeney et al., 2018).
Listening without judgement has been identified as the most identified ‘helpful’ action from professionals and non-professionals when responding to suicide risk (Nicholas et al., 2020). Service users and carers have also indicated valuing of a ‘combination of interpersonal skills (non-judgemental listening, a caring attitude and providing emotional support) and professional skills (experience, reliability and clarity of information provision)’ (Morant et al., 2017: 11).
Being treated by practitioners as an equal, ordinary and normal person has led service users to feel more responsible for their own recovery process (Hopkins and Niemiec, 2007). In another study, participants praised the ability of crisis teams to normalise service users’ crisis experiences: ‘[The two CAT team clinicians] were just nice and calm, and they just went about their normal conversation [which] put me at ease, because I wasn’t being treated as some sort of freak’ (Boscarato et al., 2014: 290).
The importance of ‘genuine care’ has been interpreted by service users in Aotearoa as being motivated by a genuine desire to help and was seen as one of the most important aspects of recovery. Professionals being their real selves when supporting service users, and who appear motivated by a genuine desire to help, have been found to decrease service users’ acute distress (Magill et al., 2021).
The importance of developing a therapeutic relationship has been identified as paramount (Hopkins and Niemiec, 2007). Conditions and worker traits that seemed to help this develop included kindness, rapport with the person and their family/carers and a having a therapeutic, professional and nurturing disposition. Within this at-home crisis treatment, quality was identified as: ‘“being listened to”; “not being treated as different”; the crisis worker “not being phased by it all” and being “almost like a friend”’ (Hopkins and Niemiec, 2007: 313). Participants described these aspects as comforting, containing and reassuring as well as engendering hope during a time of crisis.
Empathy in crisis workers has also been found to be important. Participants in a study by Giménez‐Díez et al., (2020) described feeling best when nurses demonstrated considerable confidence and experience, and shared personal situations with them when considering solutions. They described the nurses as empathetic, reliable and willing and able to help. Empathy has also been identified as important for crisis workers engaged in risk assessment, as it created a better therapeutic relationship and allowed them to be better attuned to a service user’s risk levels (Sacks and Lliopoulou, 2017).
Having considered the context of mental health care in Aotearoa and with a literature review of what service users’ find helpful, this article now turns to what was learnt from research about ‘what works?’ conducted by one of the authors.
Methodology
The second author of this paper undertook to explore the question of ‘What works for service users, with regard to their mental health wellness following suicidal ideation/attempt?’ within her doctoral thesis (Ali, 2019). The first and third authors supervised this work and both were social work academics with histories of having worked in mental health services in Canada and Aotearoa. While reviewing the data from the study, the authors were surprised by the degree of strong, negative feeling that emerged when participants described their experiences with crisis teams. The first author re-reviewed the interview transcripts with the question in mind of ‘what do participants want from their crisis teams?’
Ethics consent for this study was obtained at several levels and took approximately one year to complete. The research was first approved by the country’s Health and Disability Ethics Committee, and later was also approved through locality assessments with relevant district health boards. Consultation was also sought from appropriate Māori iwi (tribes). There was tension between ethics’ requirements for extensive risk prevention (e.g. the requirement that a psychologist needed to be present for focus groups – in the end only individual interviews occurred) versus autonomy of participants and their rights to participate. This is consistent with some of the philosophical tensions between risk and recovery paradigms (Heller, 2015).
The safety of participants was paramount during the study and numerous safeguards were put in place to allow them to share their experiences. These were informed by the authors’ experiences and knowledge as well as by the ethics committee requirements. Building relationships with participants; conducting therapeutic interactions; asking hope-inducing questions and debriefing participants when the interview ended were some of the ways the second author adhered to ethical principles. Contact numbers were also provided for relevant support services and follow-up phone calls/emails were carried out to see how the participant was feeling post-interview.
This research used a constructivist methodology (Cresswell, 2009), using the voices of service users to answer the research question. The sensitive and personalised nature of this research was consistent with a qualitative approach consisting of in-depth, semi-structured interviews following an interview guide.
Participants with experience of suicidal ideation or attempt, who were over the age of 18 and not experiencing current suicidal crisis, were recruited via posters in mental health/support agencies and by letters sent by service providers. People were invited to contact the researcher directly and an interview was arranged following informed consent being given
This article now turns to findings generated from research that encompassed consideration of service user experience of crisis teams in Aotearoa and what they wanted from these services.
Results
Demographics of Participants.
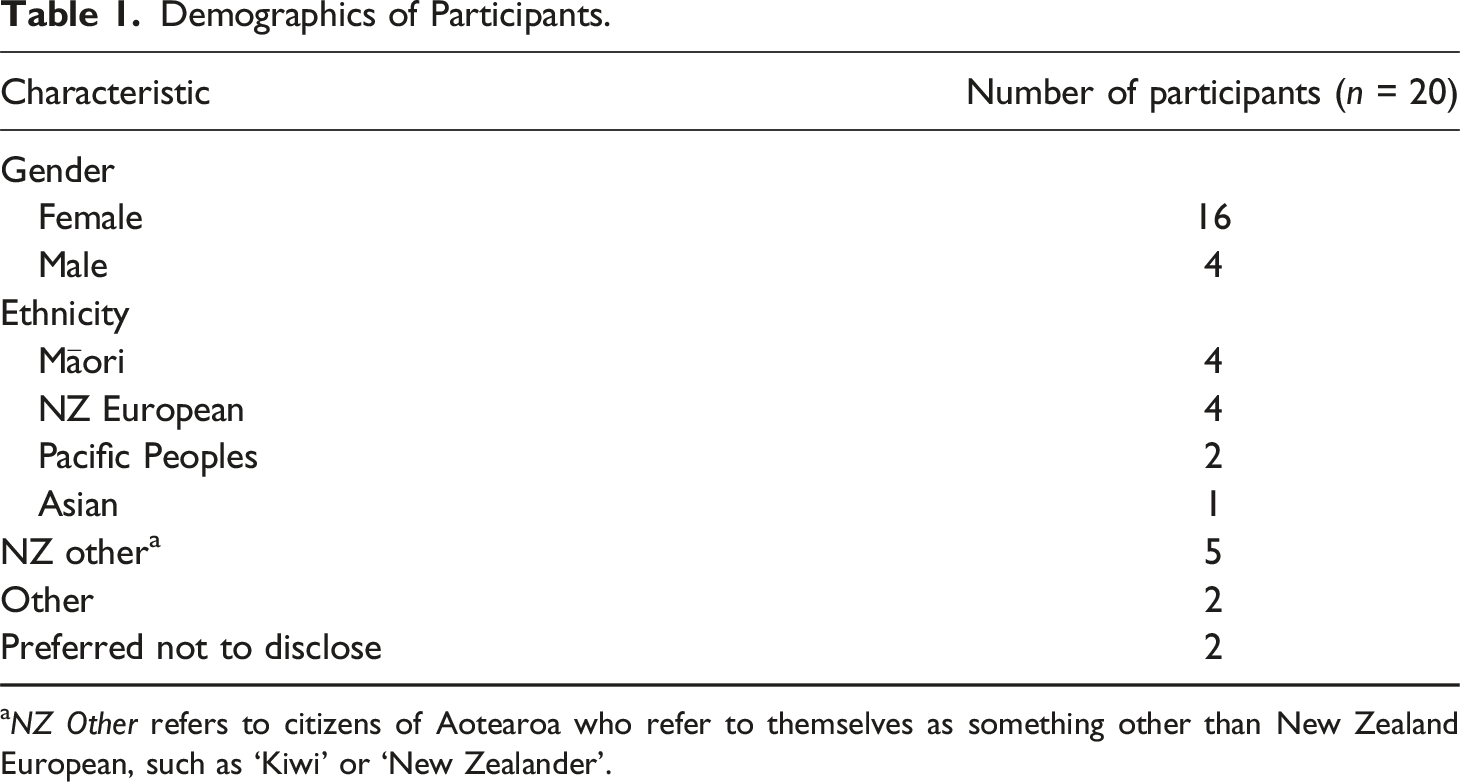
aNZ Other refers to citizens of Aotearoa who refer to themselves as something other than New Zealand European, such as ‘Kiwi’ or ‘New Zealander’.
The findings were constructed through analysis within NVivo software of the original 20 interview transcripts using the research question ‘what do participants want from their crisis teams?’ Braun and Clarke’s (2022) six stage model of reflective thematic analysis was used which includes refamiliarisation with the data, searching for themes, reviewing themes and then defining and naming those themes.
Qualitative findings
Five main themes regarding what participants found helpful were constructed from the data, with various sub-themes emerging. There are many overlaps between the themes but, overall, they included that participants wanted to experience recovery-oriented values or behaviours which demonstrated genuineness, acceptance, empathy, respect and care and compassion from their crisis teams. Each of these themes is illustrated below with participants’ quotations. Participants decided their own research identifiers: some used first names, while others chose pseudonyms.
Genuineness/congruence
Participants in this study expressed a strong desire for their crisis workers to appear genuine. They felt that in order to feel trust in the relationship that the crisis worker needed to be able to present as ‘human’. Self-disclosure, listening and being non-judgemental were also part of being seen as genuine.
One important aspect of establishing rapport, particularly in Aotearoa, where whakawhanaungatanga (relationship building) is crucial for working with Māori, is the ability to share parts of oneself in order to build trust. Bob explained that, as well as practising through use of ‘best practice’, that it was also important to use self-disclosure in building rapport ‘... for the practitioner to relate to the client in terms of maybe explaining some of their own experiences and letting the clients see they are actually a human being too’.
People described feeling accepted when they were listened to and not judged. These aspects form part of unconditional positive regard. At the time of her interview, Taimi was working as a mental health support person and described the biggest complaints she heard were about mental health crisis services not listening to people. She related that there was more that could be done in listening and responding: I think the biggest thing that we are missing though is listening to people when they tell us that they need help … So if someone asks for help we need to give it to them at the time they are asking and we keep talking about every door is the right door, …but we need to unlock it, we need to leave the door ajar a little.
Anita was very clear about the important role that listening had to play in her experiences and what she wanted from crisis intervention: I think I just wanted the CAT team to listen. I just wanted them to say ‘ok well let’s have a meeting, let’s discuss this, let’s see what is going on’, because I knew something was not right. I knew it wasn’t right and I think I just wanted someone to listen.
Frances also saw that best practice was demonstrated first through listening and paying attention to what people had to say. I think it is about hearing what the patient is saying and accepting what the patient is saying and not dismissing it so quickly [it] should be a therapeutic relationship … they need to actually sit up and take note and really listen to what the patients are saying [about] anything whether it be suicide, medication…
Participants in the research study indicated that they often felt judged by crisis clinicians (Ali, 2019) and related that having a non-judgemental stance was critical. This was exemplified by Ghost, who described the impact of feeling judged by practitioners, which she believed could inhibit someone asking for help. We thrive on being spoken to with respect and we know when someone respects us and when they don’t. We know when someone is judging us and they may not verbally say it but we pick up the discrete cues … they make you think there is something wrong with you … they judge you.
Carol and Bob both suggested that crisis workers should be taught or reminded about the importance of how they came across. They both discussed how service users would be able to spot any trace of judgement on the part of the practitioner. Carol stated, ‘they will pick up on that attitude’ while Bob stated … you can’t judge. In my job, they trained us for ages how to express empathy and how not to judge people and how to truly take a stance of egalitarianism on certain things in their responses and even their facial expressions, like you can tell they are judging you.
Empathy
Participants described that they wanted to feel empathy by their crisis team members. Behaviours that demonstrated empathy included attempting to understand and validate feelings, showing that the person was not alone and seeing that a person had ‘walked a mile in their shoes’ and understood what they may be going through.
Empathy is demonstrated through clinicians’ understanding and validation of service user experience. While peer support workers are often seen to best understand service user experience, Taimi expressed that people do not need to have gone through experiences to show validation: But experts can do that. They don’t have to have lived experience to just have a bit of compassion and validation. Obviously, validation is the most important skill anyone working in mental health services can [have].
The importance of validation is well documented in literature on personality disorders (Linehan, 1993), but participants in this study noted that there were times when they did not experience validation and that this was extremely detrimental to building trust and a good rapport with their crisis teams. Someone will read low risk, they will read personality disorder, they’ll read suicidal and go, you know, ‘go and have a cup of tea and use your skills’ … And they will change their tone of voice and you will feel the shift in the energy and what I read in the shift in the energy is ‘you don’t matter, like we don’t believe you, we don’t believe your stress is real’. (Willa)
Similar to having experiences normalised, Delia described the importance of having a decreased sense of isolation by knowing that she was not alone. Good crisis clinicians were ‘quickly able to help people that are unwell [to] see that you are not alone in that, you know, there are lots of other people that have felt the way that you do have considered or tried to take their lives’.
Participants discussed finding it helpful to work with peer support workers, or with people that they knew had had similar experiences, that they could, in fact, understand. This is often referred to as someone having good understanding through having ‘walked a mile in my shoes’. Bob discussed how peer support workers or other clinicians were able to build relationships when they are, ‘… someone who has actually been through that same shit and knows how it feels. They will always be able to talk to you and establish rapport and a relationship with you on a different level’.
Taimi described that she would often hear that people would feel comfortable working with her as a peer support: … because people know you get it, whereas those on the other side of Crisis line or police 111, they don’t get it. They haven’t been there and they can be quite patronising. While there are many people working in mental health who have lived experience of mental distress, they do not always feel safe or comfortable disclosing this.
Respect
Participants expressed that they wanted to feel respected by their crisis workers. This was shown by crisis professionals not being patronising, providing time for people, and keeping promises they had made. Similar to genuineness, and being treated like a fellow human being, participants appreciated respect, when they felt that they were being treated as ‘equals’ and not feeling like they were being ‘talked down to’. Annie described her experience of a key worker/social worker who treated her this way: I’ve got my social work degree and she didn’t really treat me like a patient. She almost treated me like an equal. Like the way she talked to me and shared things. She was awesome and because of that, that made my recovery start faster. She would take me out for lunch and we [would] sit and talk about work and life … A lot of key workers don’t do that. They are very much above their clients.
Willa described that what people need ‘more than anything, is to be taken seriously and to be met as a person and to be given respect’. When asked about what best practice would look like, Anita described: I think [it] has to be respect … So being offered that respect and at that time and being listened to respectfully, being spoken to respectfully is absolutely key. If you are talked down to, if you are not listened to, if you are not taken seriously, it is actually really quite destroying.
Participants indicated that they felt respected when professionals spent time with them. This was significant in people’s ‘treatment’ and should not be undervalued. Willa described the close relationship between respect and crisis workers taking time, giving someone attention and the role that could play in future suicide prevention: … mental health professionals need to be reminded that the biggest healing thing they offer is their respect and their attention … because more than anything else, even when people aren’t getting what they are hoping for, they are still feeling a lack of support. You have just actually given them an experience of being respected and that is protective for future experiences of being in distress or being suicidal.
Taimi discussed how doctors rarely appeared to have time to listen to people and that it was really the nurses who made the difference. [They] are the one who go and sit with someone and talk to them at 4 o’clock in the morning when they can’t sleep. [They] tell them to go back to bed and give them their sleep meds and have a cup of tea with them and find out about their life. [They] treat them as real people.
Ralph also described the importance of people taking time to listen and how that had appeared to shift over time, as increasing fiscal restraints took hold: I’ve experienced [clinicians getting] more and more stretched. And so often, sometimes it feels like a lip service kind of thing, and they are not actually giving you time. I think in that way that is one main thing they need to be under less pressure so they can actually take their time to listen to people.
Participants indicated that when a crisis worker follows through on commitments, this demonstrates that someone is important and deserving of respect. Carole described how, for people in distress, what someone says may take on even more meaning than at other times, particularly if there are not many things to occupy their time or if they are feeling a lack of hope. So what one of them says they are going to do, you remember that. And then if they don’t do it you actually get quite upset because that is your whole world and quite a few will say ‘I’ll do this or I’ll do that, I will ring you next week’ and they don’t, whereas they shouldn’t make those promises and then don’t carry them out….
Care and compassion
Showing care and compassion was the final theme that participants indicated they wanted from their crisis teams. This was shown through crisis workers being there for someone physically and emotionally and showing humanity. Participants tended to see this being combined with many of the traits mentioned in previous themes. I think best practice-wise I think definitely comes down to that being listened to and just that respect and kindness. (Anita)
Amy described the importance of listening compassionately. … it goes back to actually listening to the person and creating an environment anywhere where it’s clear that what you disclose is not going to be used against you. I guess in a non-judgemental compassionate way that person gives you time … So yeah, they need to be listening and patient and, yeah, not judge you…
Similar to validation, Willa described how some mental health workers may not demonstrate the compassion that is so important for people who experience personality disorders, or chronic suicidality: … the thing is so much of it I feel like our mental health workers are just tired that they are overbooked and that it is far easier to save your compassion for people that are obviously dealing with something that looks more [like] an illness.
Pearl discussed a sense of respect that she held for two crisis clinicians who exhibited compassion and empathy towards her. This was significant as they were very different to her in both age and gender. I found them really supportive and even though they never really disclosed it, it was quite obvious … they were speaking from experience, not just having read stuff […] or learned it on the job. There was a compassion and an empathy [versus] compassion which is hard to fake.
Pearl summed it up nicely when she described the X factor that good workers bring to their relationships: I think people can see when someone gives a damn and when someone doesn’t.
Discussion
Several areas for consideration arise from this research. Consistent with previous literature (Magill et al., 2021; Morant et al., 2017) participants indicated that, they wanted to be heard, respected, understood and accepted by people who were real and who cared for them. These factors are all related to recovery-oriented perspectives, consistent with social work values (Kourgiantakis et al., 2020). Participant desires can be related to changes and recommendations at individual, organisational, societal and political levels and are discussed in this order below.
Results of this study revealed the importance of crisis workers being able to engage in relational practice and being real people. The Aotearoa New Zealand Ministry of Health has determined that all mental health services should be delivered through a set of ‘Real Skills’. The first of these is that ‘People accessing health care have their mana (status and worth) protected and enhanced, experience respect, engage in shared decision-making and receive support to achieve their health and wellbeing goals’ (Te Pou, 2018). Continuing professional development for all crisis responders that emphasises the importance of relational practice is important. The skills of warmth, genuineness, respect and empathy are the bread and butter of social work practice (Staniforth, 2015) and social workers can play a role in teaching and role modelling these skills. Social workers often advocate for person-centred responses on multi-disciplinary teams (Francis and Forbes, 2020) and they are also equipped to fight for greater systemic and social change. Even within a risk paradigm, Sacks and Lliopoulou (2017) emphasise the importance of staff development and self-reflection so that they can build rapport and understand their clients’ points of view as part of an ongoing risk assessment process.
Participants in this study discussed the benefits of being supported by peers, as they understood and didn’t judge. The Substance Abuse and Mental Health Services Administration., (2022) in the United States has provided advice regarding the importance of including peer support workers in crisis response services. They describe that including peers can strengthen engagement in treatment and provide recovery messages that encourage and give hope to service users. They caution though that peer support workers may experience stigma from crisis clinicians schooled in the medical model. There has often been a false dichotomy created between people who use mental health services and those who deliver them or in defining who is a ‘clinical worker’ and who is a ‘peer support’ worker. This is increasingly evident as cuts and stretched services further impact upon the wellbeing of mental health workers (Reynolds, 2017). In this research, Taimi described that it would be helpful if more mental health professionals were able to be open about their experiences of mental distress but that things such as ongoing stigma and organisational cultures may prevent this. This points to the ongoing importance of societal change through the provision of such things as destigmatising campaigns.
The benefits of peer support are being further explored through research by Banfield et al. (2022) who aim to explore peer supported ‘safe spaces’ as an alternative to hospitalisation and medical model treatment in Australia. They describe environments which ‘include the application of lived experience and strength-focused social and practical support to foster hope, connection and healing to those in crisis’ (2022: 2). This approach seems consistent with the desire of participants in this research and may contribute ideas on how respite services for people in crisis can best be provided in Aotearoa.
An ongoing tension in crisis mental health work is managing risk and working according to recovery principles. This is especially prevalent working with people who experience suicidal ideation or have engaged in attempts. Risk cultures seek to attribute blame and do not encourage self-determination of people and relational practice. Crisis team members need to feel supported in balancing risk and recovery and responding as human beings first and foremost. This requires organisations which recognise the benefit of tolerating risk to ensure longer term gains and which are not reactive to blaming and shaming and sensationalised press coverage. This support needs to start at the top so that crisis staff feel safe and contained in order to engage in creative and supportive practice.
The cultures of crisis teams and their organisations are also important in determining service responses. Like the risk/recovery tension, some organisations are strongly medically oriented, where resources are more aligned to medication, whereas others have more holistic approaches. The professional make-up of crisis teams may also reflect these different perspectives. Social workers can make a valuable contribution to crisis teams by emphasising the importance of how people are responded to. Reed and Field have called on social workers and occupational therapists to challenge current norms to ‘ensure that the ideals of recovery and social and occupational justice are embedded in legislation and service delivery while, in turn, ensuring that, care and treatment takes place in the least restrictive environment’ (2017: 64).
The literature has discussed how while community-based care may have initiated the proliferation of crisis teams, the medical model has remained ingrained (Brunton, 2004). The perceived and contracted roles of crisis teams have undoubtedly shaped how and by whom services are delivered. Government policy in Aotearoa has shifted towards a view that mental health care needs to be considered within a wider context of poverty, cultural dislocation and family violence (Ministry of Health, 2021a, 2021b), very much the purview of social work practice. This policy shift could inform how crisis services could be delivered which considers a more holistic view of crisis and the support required. This is consistent with views expressed by Ramalho et al. (2022), who state that we believe there is broad support for reducing the emphasis on individualized approaches to mental wellbeing and moving all systems and structures towards models inclusive of social context, including approaches that incorporate service users’ perspectives, family, communities, and culture. We look forward to policy and services with a much stronger orientation to the diverse needs of our population. (p. 60)
This shift will however require long-term changes, and different ways of governments working together, so that one government does not undo the forward momentum of its predecessor. Social workers have a role to play in the macro context to advocate for more non-partisan collaboration between political parties which places the wellbeing of people at the centre of government policy (Staniforth, 2021) for both crisis and long-term involvement with mental health services.
Conclusion
Twenty people in Aotearoa, who have experienced suicidal thoughts or attempts, have provided a rich account of their experiences with crisis support teams, and what they wanted through these encounters. Their perspectives validate a relational, person-centred approach to practice that emphasises warmth, genuineness and caring. Knowing that someone understands you and your experiences is also important. These conditions are often at odds with overstretched, medically oriented, risk-averse settings where crisis support services are often located.
This article discussed the importance of responses at various systemic levels to enable best practice for people experiencing suicidal ideation or previous attempts in their interactions with crisis teams. Social work can make a significant contribution in all of these areas. This article once again makes the call for crisis teams to engage in more holistic, recovery-oriented practices that demonstrate respect and value for all people.
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of the 20 participants who gave freely of their time, knowledge and experience.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.