
Abstract
Hospital social workers advocate, facilitate and communicate with patients, families, healthcare professionals, and communities. These activities, in which hospital social workers relate to different parties and aim to strengthen relationships between them, have been referred to in the literature as boundary spanning. This study explores hospital social workers’ boundary-spanning competencies associated with their boundary-spanning activities. The data were from in-depth interviews with 19 hospital social workers in Norway. A hybrid analysis was performed, combining initial inductive coding of themes with subsequent deductive coding based upon a conceptual framework. Four themes emerged: (1) Being informed, (2) Content knowledge, (3) Tailoring and (4) Self-knowledge. The findings contribute to specifying central boundary-spanning competencies. Implications of the study for social work practice and education are provided, along with recommendations for further research.
Keywords
Introduction
Social work involves relationships with individuals, between individuals, with individuals in groups, between individuals and organisations, and between organisations (Harsløf et al., 2017; Moon et al., 2019). In the health social work literature, the social worker’s role of strengthening the relationships between different parties has been expressed using different terms: broker (Craig and Muskat, 2013; Moore et al., 2017), glue (Cootes et al., 2021; Craig and Muskat, 2013), negotiator (Schot et al., 2020) and coordinator (Moore et al., 2017). Although these are recognised roles of hospital social workers (HSWs), the research literature has, to a limited degree, specified which competencies are prominent in fulfilling these roles or functions. Despite a range of studies investigating professional competencies amongst HSWs (Bosma et al., 2010; Cootes et al., 2021; Nicholas et al., 2019), the specific competencies that HSWs need in order to coordinate, convey and translate information between different parties has received little attention. Therefore, the current study brings in Van Meerkerk and Edelenbos’ (2020) framework to contribute to understanding the boundary-spanning competencies needed by HSWs to conduct these professional activities, both in the context of acute and critical illness and beyond. Our main research question was: What boundary-spanning competencies do hospital social workers use in their professional practice?
A boundary-spanning framework
Previous health social work research has explored competencies through the lens of specific fields or contexts, such as primary health care (Rowe et al., 2017) and palliative care (Bosma et al., 2010). It has also investigated competencies within concrete categories, such as communication (Koprowska, 2020) and reflection in action (Ferguson, 2018). However, as mentioned previously, few studies have explored the kinds of competence needed to negotiate and coordinate between professionals and organisations. To contribute to such a discussion, we have employed the boundary-spanning framework developed by Van Meerkerk and Edelenbos (2020) on HSWs’ professional competence. According to the authors, boundary-spanning activities, such as relational and networking activities, are essential in the coordination and collaboration processes across professional and organisational boundaries (Van Meerkerk and Edelenbos, 2020). Based on a literature review of boundary spanning in the field of public management and governance, Van Meerkerk and Edelenbos (2020) have specifically defined boundary spanners as people who pro-actively scan the organisational environment, employ activities to collect information and to gain support across organisational or institutional boundaries, disseminate information and coordinate activities between their ‘home’ organisation or organisational unit and its environment and connect processes and actors across these boundaries. (1439)
Thus, collecting and disseminating information to coordinate activities and actors are demarcated as core boundary-spanning activities. Van Meerkerk and Edelenbos (2020) have pointed out that these boundary-spanning activities demand certain competencies, or know-how and skills. Based on a literature review, they identified three categories of competencies: cognitive, social and emotional. These are particularly important because they fulfil the boundary-spanning role in various contexts. Cognitive competencies refer to the know-how and skills needed to process information and to reason analytically. To deal with environmental uncertainty and complexity, boundary spanners need to identify important issues related to the situation and distinguish between what is relevant information and what is not. The ability to be sensitive to salient information, critically assess and analyse important content, and break down problems requires content expertise and cognitive capacities (Getha-Taylor, 2008; Van Meerkerk and Edelenbos, 2020).
Social competencies include communication, listening and conflict management skills (Williams, 2002). The ability to convey and translate information across boundaries and to adapt and adjust communication to a specific context is essential for boundary spanning (Weerts and Sandmann, 2010). The boundary spanner’s listening skills involve ‘a willingness and openness to be influenced by the view of the other’ (Williams, 2002: 115). These skills facilitate collaboration and mediation between different interests and perspectives (Van Meerkerk and Edelenbos, 2020).
Emotional competencies involve ‘the ability to monitor one’s own and others’ emotions, to discriminate among them and to use this information to guide one’s thinking and actions’ (Salovey and Mayer, 1990: 189). Self-awareness, self-monitoring, self-confidence and self-efficacy are all components of emotional competencies. While self-awareness and self-monitoring refer to the perception of one’s feelings and reactions, self-confidence and self-efficacy refer to the belief in one’s ability to perform a task successfully and effectively engage in important relationships, respectively (Van Meerkerk and Edelenbos, 2020). Sensitivity to the interests and needs of others and cognitively processing and emotionally reacting to such interests and needs both “merge” into empathy skills. Adapting one’s attitudes and behaviour to such external socially driven cues contributes – along with social competence – to building relationships with others (Williams, 2002).
While the three categories of competencies are well known within social work literature, few studies have discussed the role of cognitive, social and emotional competence as boundary-spanning competencies. For example, social competencies are often discussed as necessary skills in the negotiation and management of conflicts (Craig and Muskat, 2013; Gibbons and Plath, 2009); as verbal and non-verbal communication skills (Brazg, 2018; Craig and Muskat, 2013; Holliman et al., 2001; Sims-Gould et al., 2015); or as important skills in relationship building (Craig et al., 2020; Lilliehorn et al., 2019; Richards-Schuster et al., 2015). However, they are not often presented, for example, as vital to coordinating activities between health professionals. In the literature on cognitive competencies in social work, we often find studies investigating knowledge areas important for social workers, such as medical knowledge and knowledge of the welfare system (Bronstein et al., 2007; Nicholas et al., 2019) or the importance of having a holistic knowledge base (Craig et al., 2015). Less common are studies on how cognitive knowledge involves the ability to connect and integrate knowledge (Abendstern et al., 2014; Brazg, 2018).
Finally, the literature on emotional competence often explores empathy as critical to social work practice. This emotional competence is considered important in the interaction between social worker and client (Gibbons and Plath, 2009; Grant, 2014; Watson et al., 2022). These and other studies argue that putting oneself in the role and perspective of others is fundamental for understanding and acting adequately. While emotional competencies are important in interactions with patients and families, they are just as relevant for coordinating and getting people and institutions to talk together.
A few studies have used the concept of boundary spanning but failed to systematically elaborate on central forms of boundary-spanning competencies. Brazg (2018) examined HSWs’ boundary-spanning capacities based on a framework of four boundary-spanning competence domains: values and attitudes, habits of mind, knowledge-based competencies and interpersonal competencies (Nurius and Kemp, 2019). The findings suggested that attitudes, beliefs, integrated knowledge and being a skilled communicator were necessary for team functioning (Brazg, 2018). Another study explored social workers’ self-efficacy in the sense of feeling competent when working within acute hospital care (Lloyd, 2021). This study found their self-efficacy to be moderate. To the best of our knowledge, however, no study has used the framework set out by Van Meerkerk and Edelenbos (2020) as a lens for exploring competencies related to HSWs’ boundary-spanning activities.
The role of hospital social workers in Norway
In Norway, there is a lack of state guidelines for hospital social work and regulation of this profession’s work tasks. However, the Norwegian Union of Social Workers (FO) describes an HSW’s overall purpose as providing psychosocial support and counselling to strengthen the ability of patients and their next of kin to cope with the situation (FO, 2022).
In clinical practice, the Norwegian HSW’s personalised interventions do not differ significantly from what is described in previous international studies. Central interventions include providing information on financial and practical arrangements, advocating for resources and service coordination and supporting individuals’ emotional needs based on the unique requirements of each patient and family (Lilliehorn et al., 2019; Mannsåker et al., 2021; Muskat et al., 2017; Pockett et al., 2020; Wiggins et al., 2018).
The Norwegian HSW’s role can be divided into three categories. Regarding patients and their families, their role is to guide and find solutions to financial and practical challenges, and to identify and support social, relational and existential needs surrounding the current situation (FO, 2022; Mannsåker et al., 2021). Interprofessional collaboration forms another essential part of the role, in which the HSW represents a psychosocial perspective (Lilliehorn et al., 2019) and facilitates the information flow between the family, health care professionals and municipal services. Specifically, the HSW acts as a liaison between the family and the medical treatment team, capturing informational needs and passing them on to support a sufficient understanding of medical information (Gibbons and Plath, 2009; Mannsåker et al., 2021; Nicholas et al., 2019). Finally, the HSW’s role also includes teaching patients, their families and other health professionals in topics such as relevant financial and social rights or psychosocial consequences of illness and treatment (FO, 2022; Mannsåker et al., 2022).
Data and methods
This article draws on data from a qualitative research study on HSWs’ articulation of and argumentation for competencies and practices in paediatric hospital wards in Norway. The study was based on individual semi-structured interviews to deeply explore the HSWs’ unique understanding and experiences (Charmaz, 2006) of the following themes: the needs of families of acutely and critically ill children, interdisciplinary collaboration in the acute stage, and the HSW’s knowledge base and articulation of knowledge. The study was approved by the Norwegian Social Scientific Data Service.
The study participants were social workers practising directly in paediatric acute wards. The 24 identified HSWs and their superiors were informed about the project through an information letter. To ensure confidentiality, the participants were asked to respond directly to the first author, who was responsible for the entire process of collecting and processing the data. Of the 24 invited, 19 HSWs from 12 hospitals accepted. Due to the lack of state guidelines for hospital social work in Norway, these 12 hospitals differed in their organisational structures, expectations of HSW services and requirements for education. Seventeen of the 19 participants had a master’s degree or had additional training beyond a bachelor’s degree in social work. The average duration of their work experience was 24.6 years (13–42 years). All the participants were women of Scandinavian origin.
The interviews took place mainly at the participants’ workplaces. Each participant was interviewed once for an average of 72 min.
The software NVIVO 12 Pro was used to manage the data. The quotes used in this article were translated from Norwegian to English by the first author and reviewed by a colleague.
Analysis
The data on which the analysis of this article was based stem from one of the four code groups that emerged from the initial condensation of the text from the inductive analysis (Malterud, 2012). The code group was called competence and experience. The first author completed the analysis in four steps: (1) identification of associated themes through familiarisation with the data, (2) coding of the preliminary themes into groups based on potentially identified units of meaning, (3) creation of condensates for each coded group and (4) summarising of the content of each group to generalise the description.
Despite the code group’s rich descriptions of competencies and experiences, the inductive approach did not yield surprising findings. Therefore, with the ambition to ‘defamiliarise the known world’ (Timmermans and Tavory, 2012: 176), we proceeded from the inductive orientation described above towards a deductive-oriented thematic analysis (Braun and Clarke, 2006) using the boundary-spanning perspective (Van Meerkerk and Edelenbos, 2020) as a frame to help us identify specific boundary-spanning competencies in the data material. As described by Fereday and Muir-Cochrane (2006) and Ligurgo et al. (2017), such a coding process could be termed a hybrid approach that combines an inductive coding of themes in the initial condensation of the material with a subsequent deductive coding based upon the conceptual framework. In practice, we worked dialectically in the deductive stage of analysis by going back-and-forth between the data set and the theory and interpreting the data in light of the theoretical perspective to identify boundary-spanning competencies. Van Meerkerk and Edelenbos’ (2020) conceptual framework offered a structure for exploring competencies based on activities harmonising with typical HSW performance.
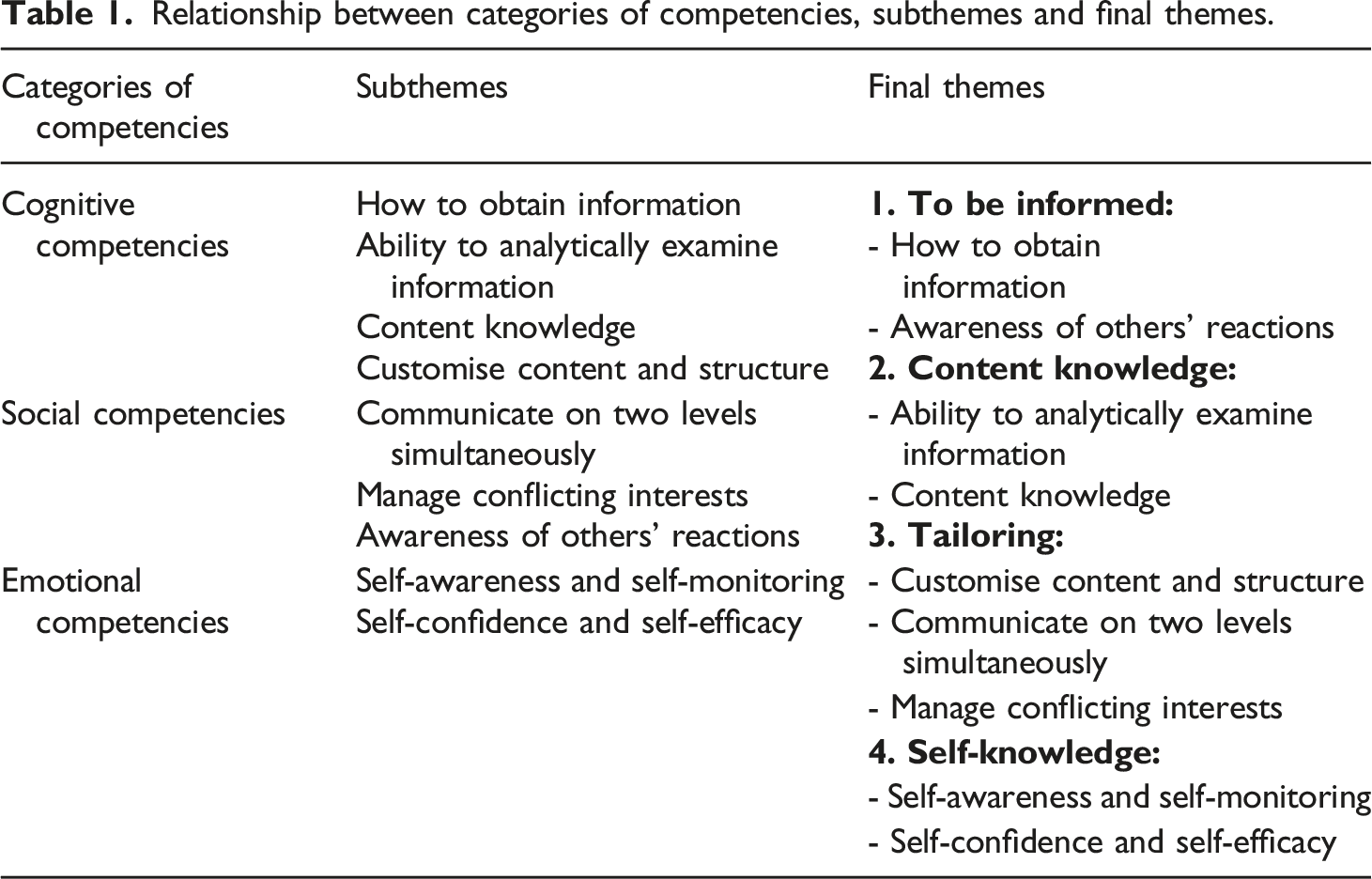
Based on the framework’s focus on the link between boundary-spanning activities and competencies, the first author began reading the data set by asking, ‘What kind of boundary-spanning activities do the respondents say they perform’? The categorisation of the activities that emerged largely corresponded with the one presented by Van Meerkerk and Edelenbos (2020). Descriptions of different competencies emerged while identifying extracts from the participants’ depictions of their activities; these competencies were identified and abstracted. The subthemes evolved through a back-and-forth between the abstracted data extracts and the framework’s description of the three categories.
Relationship between categories of competencies, subthemes and final themes.
Findings
The four main themes emerging as a result of the deductive stage of the analysis process were as follows: (1) to be informed, (2) content knowledge, (3) tailoring and (4) self-knowledge. The findings will be presented separately.
To be informed
The first main theme concerns being informed, that is, having a sufficient understanding of a situation. To be or become informed on several matters and in various ways was perceived as essential to acting adequately.
How to obtain information
Knowing how to obtain information to be prepared for encounters with professionals or parents constitutes one aspect of being informed. For the participants, considering what information was relevant and how to obtain relevant information from available sources were insights built up through working experience. For my part, it’s a lot about being prepared in every way; you also have to know what you’re going for. Preparing for something perhaps also comes with experience […] Talk about it [the medical situation] with physicians, get some explanations, some knowledge. (No. 4, 21 years of work experience, 11 years as HSW)
Receiving medical information directly from physicians or nurses was an important source of knowledge for specific medical conditions. Reading the patient’s medical record and attending pre-rounds or interprofessional meetings provided access to advanced information about the social and psychosocial aspects of the patient and their family.
Awareness of others’ reactions
Another way of being informed is by being aware of others’ reactions in face-to-face encounters. This emotional competence refers to an ability to perceive other people’s emotional states and use this information to guide the manner of engagement with those people. Making this observation meaningful also involved cognitive skills, as exemplified by this HSW: [When I meet the parents], I use a technique that involves asking [about the situation and special needs] a little bit, right, to check if I have them with me. If I see someone’s eyes flicker, then I say, “We can get back to it.” (No. 10, 42 years of work experience, 28 years as HSW)
Content knowledge
The second main theme is content knowledge. Content knowledge – of the welfare system, medical issues, psychosocial needs and legal frameworks, for instance – contributed to a better understanding, recognition and assessment of relevant information. This knowledge often formed a basis for further exploration or for filling responsible roles in certain situations. As an example, several of the participants had experienced that health personnel tended to pass the job of reporting concerns about a child’s care situation and risk of harm to the HSW even if they were not involved in the case. Having knowledge about legal frameworks and guidelines made it easier to keep the guiding role, as illustrated by the following quote: “No, I can’t take over the case, but look here, the guidelines for how to report a concern are there. What you have to do is …” Right? Then, I can guide them a bit along the way and give them a bit of confidence in what to do next. (No. 16, 13 years of work experience, 2 years as HSW)
Another HSW underlined the necessity of having knowledge in oral and written communication, but also of the ongoing development of content knowledge in daily practice: What I think is important is that you have basic knowledge of talking to people, different types of people in different life situations. And I actually think it is very important that you can write properly and have knowledge about and use legal frameworks (…) You must not know everything, because that will be too general, but you must be able to familiarise yourself with things and learn as you go, around the exact topics you will be working with. (No. 3, 21 years of work experience, 10 years as HSW)
Furthermore, using content knowledge also led to further inquiries. For instance, being familiar with legal frameworks and legal support could make the HSW able to assess whether the situation demanded assessments beyond the guidelines, and thus avoid potential legal pitfalls, as illustrated in the following quote: I had a case the other day where I felt that here we must find out what is right and wrong. And then, I had to call the hospital legal counsellor to clarify the legal issues before I consulted a colleague to find out how we should handle them further. (No. 16, 13 years of experience, 2 years as HSW)
Tailoring
The third main theme is tailoring. Tailoring concerns context-sensitive ways of communicating with parents or health professionals adapted to their needs and preferences, with the expectation that this individualisation will lead to a larger intended effect. ‘You have to adapt the information to where people are’ was the prevailing message of the participants regarding communication skills. Tailoring was expressed in several ways.
Tailoring content and structure
The ability to adapt content and structure to a specific communicative context is an important part of tailoring. An HSW’s reflection on her communication strategy with community service staff provides an example: We must be clear about our professional assessments, what we have found in the examinations. Be as clear as we can about what their needs are. […] Both writing in the applications and orally on the phone and in meetings, I can say that the child has such and such needs and has such and such [diagnosis], and the difficulties for the parents are like this, and they are completely exhausted, and so on. (No. 5, 27 years of work experience, 17 years as HSW)
Another HSW with 17 years of experience with interprofessional collaboration from contexts other than hospitals reflected on her experiences of communicating with physicians during her first year at the hospital: As a social worker, I have to somehow find a way towards each individual physician. I have to learn to get to know how they work. I have to find small openings when they have time to talk to me. […]. It’s a completely different culture here. There is more fast-paced, it’s more case-oriented. I have to be quicker when I present something. It’s a different language. (No. 17, 17 years of work experience, 1 year as HSW).
Formulating the message precisely in medical terms improves accuracy and helps strengthen the relevance of the message. However, medical terms could have the opposite effect when talking with parents. Thus, the HSWs assessed whether they should minimise the use of medical terms and speak in a simpler manner when communicating with parents.
The skill of customising communication was also necessary when providing reports in medical records. The medical records represented an information channel towards other health professionals. At the same time, they also had to keep in mind that patients have access to their medical records, and the information would also be available to them. Thus, the medical records represented a communication medium that had to safeguard several interests.
Communicating on two parallel levels
Another example of tailoring is when HSWs sought to communicate on two parallel levels with parents under high stress. Talking about practical issues with the parents was a way to simultaneously attend to their stressful state and convey information. As one HSW emphasised: When you get the practical stuff sorted out and fixed the economical things, that we have control over this, so and so it is, you will do this, I will do this, we will get it together, eh, then I feel that they breathe. (No. 1, 18 years of experience, 5 years as HSW)
Another HSW talked about how they must appraise the information provided so that it conforms and attends to the parents’ emotional state: Everyone reacts differently, but it’s just to be there with them and make the situation safe. Not too much information, but not too little, either. But just right. And try to tune in and be a bit sensitive. (No. 17, 17 years of experience, 1 year as HSW)
Ability to facilitate and negotiate
Applying communication and listening skills in order to customise contributions was just as relevant when managing conflicting interests. Contributing to finding solutions and compromises acceptable to each party required an ability to facilitate and negotiate in context-specific ways. The following quote illustrates a typical situation in preventing the development of a conflict between parents and health professionals. Here, the HSW explains how she balanced her efforts: I can either give advice to the parents on how to present their problem, or I ask like this: ‘Do you want me to get in touch and convey this?’ But then I have to be careful. I must not put the parents in such a situation that they are looked down upon because they go to the hospital and complain... So, I try, when I call the municipality, to highlight the positive aspects, that the parents are very happy that they get assistance three nights a week, they are very grateful for that, but they need more. […]. Whether it’s the patient, or those I’ll be working with at the hospital, or those I’ll be working with in the municipality [I will ask myself] how does it look from their point of view? (No. 10, 42 years of work experience, 28 years as HSW)
Self-knowledge
The final theme emerging from our analysis is termed self-knowledge. Self-knowledge involves the ability to recognise one’s own feelings and emotions and develop strategies to handle them.
Self-awareness and self-monitoring
While self-awareness is about being aware of one’s feelings and emotions, self-monitoring refers to understanding what feelings and emotions express and what triggers them. The findings specifically emphasise understanding one’s needs and the drivers of one’s emotional reactions, as well as helpful strategies for being emotionally prepared for whatever may come. One participant used a constructivist argument to illustrate how language creates ways to see the world, which, in turn, affects thoughts and emotional reactions: It had been completely different if I had entered the room and thought or said to myself that now I am going to meet a family in a deep, deep crisis... because then I turn on some completely different switches compared to when I say that now I will go in and meet some people who are having a hard time. For me, it’s a huge difference. (No. 13, 24 years of work experience, 18 years as HSW)
Choosing words that opened up alternative actions helped her to be in a mood that had a calming effect on herself as well as the parents. Being prepared emotionally by intentionally tuning in to a mood appeared as a central skill among the HSWs. The mood enabled them to take a step back, analyse the situation and sort out what could be the right thing to do or say in a given situation.
Some of the HSWs talked about their awareness of how their own emotions could be evoked when issues were recognisable from their own lives. The ability to distinguish between their own feelings and those of others required ‘some knowledge that makes you understand what’s going on with you, […] so that I am able to, to a certain extent at least, connect it to things that are more about my life’ (No. 2, 35 years of experience, 1 year as HSW). This exemplifies how knowledge or theoretical concepts contributed useful perspectives on experiences that, in turn, could increase self-awareness. Furthermore, being able to distinguish between one’s own reactions and those of others seemed to increase their confidence while feeling emotionally affected in the encounters, as this quote illustrates: What should I do about the feelings that arise during a conversation? […] That it is allowed to say that “now … as you can see, this affects me…. I can handle it, but just know that your child actually is important”... that you do not meet a person who is completely switched of when your child is very ill. (No. 1, 18 years of experience, 5 years as HSW)
Self-confidence and self-efficacy
Self-confidence is about having confidence in the relevance of one’s assessments and contributions. Confidence in one’s ability to communicate and promote one’s contributions will be referred to here as self-efficacy.
The participants’ self-confidence in their competence and point of view was most often articulated when they had to advocate for the influence of social determinants on health issues. They experienced a correlation between regularly reminding other health professionals about this perspective on the one hand and patients’ socioeconomic situations on the other hand and the rates of referrals to the HSWs. Self-confidence also came to the fore concerning defined tasks. For example, clarifying ‘the application and the legal basis for why they [the patients] can apply [for financial support], and then I send it electronically to the doctors and ask them to write a doctor’s statement’ (No. 7, 17 years of experience, 4 years as HSW).
Their confidence in their ability to handle unexpected scenarios represents another example. For instance, when the parents asked a question that the HSW could not answer, she felt ‘so confident that I can say that I’m not quite sure, but I can find out … and then I can come back’. (No. 1, 18 years of experience, 5 years as HSW)
The HSWs thus expressed having self-efficacy when it came to handling challenges in encounters with patients and families. However, their self-efficacy seemed to depend on the context when it came to proclaiming their contributions to other health professionals. In contrast, in situations traditionally dominated by physicians, such as pre-rounds, none of the HSWs showed confidence by taking the initiative to challenge the existing order or to speak up, even if they could provide relevant information or were missing information. We [the HSWs] have discussed if we should do it [attend at pre-rounds]…there is no room to bring in anything there […] The physicians are clear that pre-rounds are for medical issues. (No. 4, 21 years of experience, 11 years as HSW)
Discussion
Four main themes of competencies emerged when exploring HSWs’ boundary-spanning competencies in the context of acute and critical illness. The first two themes referred to forms of cognitive competence. The first entailed ways of being sufficiently informed, being sensitive to different types of salient information from several sources and putting together information to get a clearer picture of a particular situation to act adequately. Although sharing information is identified as a social work competence (Bosma et al., 2010; Cootes et al., 2021), less is known about strategies on how to be informed. The findings thus contribute to specifying prerequisites to the competence of sharing information. In this respect, the importance of having a foundation of content knowledge was emphasised in the second theme. Having knowledge from different disciplines enabled the HSWs to differentiate, analyse and identify the situation. This comprehension further formed a basis for exploration and clarified their professional roles.
While previous research (Bosma et al., 2010) has emphasised social workers’ content knowledge, it has not sufficiently investigated content knowledge as a boundary-spanning competency, that is, knowledge necessary to negotiate and coordinate between individuals, professionals and organisations. As described previously, the cognitive dimension of HSWs’ boundary-spanning competency – their content knowledge and ability to obtain, distinguish and synthesise knowledge from physicians and nurses (for example) – enhanced their understanding of situations and ways to handle problems at hand. In other cases, this led to further inquiries.
Creating communication personalised for the recipient and with the expectation of an effect beyond message processing (Hawkins et al., 2008) represented the third theme. Tailoring, as a form of social competency, involves the ability to customise content and structure, communicate on the cognitive and emotional levels simultaneously, and manage conflicting interests. In social work research, person-centred communication or interpersonal knowledge and skills have been emphasised as vital skills (Clark, 2010; Koprowska, 2020) in building good relationships with service users or negotiating and managing conflicts (Craig and Muskat, 2013; Gibbons and Plath, 2009). However, as Van Meerkerk and Edelenbos (2020) argued, being able to tailor or adapt information and knowledge across actors and boundaries in context-sensitive ways could also be viewed as a boundary-spanning competency. The communication and listening skills of boundary spanners facilitate the collaboration and mediation of interests from different actors, such as when HSWs communicated on two parallel levels with parents under severe stress or when preventing the escalation of conflict between health professionals and parents.
The last theme, self-knowing, was about the ability to recognise one’s feelings and emotions, develop strategies to handle them, and make them a resource for different encounters and contexts. Emotional competence or self-reflective practice is considered essential to HSWs’ professional competence (Bosma et al., 2010). A central argument in the literature is that awareness of one’s own and others’ perspectives and emotions is fundamental in interactions with service users or clients (Gibbons and Plath, 2009; Grant, 2014; Watson et al., 2022). The role of social workers’ empathy is also emphasised in the literature. However, as Van Meerkerk and Edelenbos (2020) suggest, emotional competencies are also relevant for coordinating and getting professionals and institutions to talk together. As indicated in the findings, HSWs’ self-confidence, a component of emotional competencies, facilitated advocating a social determinant-perspective on health towards other health professionals. For instance, HSWs made other health professionals aware of the correlations between patients’ socioeconomic position and health. They also tended to take responsibility for coordinating applications for financial support to patients and families in close collaboration with physicians.
These competencies and activities, which we have framed within a boundary-spanning perspective, are well recognised within social work (Fjeldheim et al., 2015; Harsløf et al., 2017; Moon et al., 2019). As early as 1922, in her theory of social casework, Mary Richmond described the social worker’s indirect work with and through external resources (Fjeldheim et al., 2015), suggesting that social workers span professional and organisational boundaries. Other and more recent examples are studies conceptualising these roles (Abbott, 1995; Cootes et al., 2021; Craig and Muskat, 2013; Moore et al., 2017; Schot et al., 2020).
As argued in our introduction, although boundary spanning constitutes an important part of what social workers do in different occupational contexts, there is a paucity of studies exploring the specific activities and competencies needed in professional practice. As Van Meerkerk and Edelenbos (2020) argue, drawing on an extensive literature review, professionals often engage in relational and networking activities to coordinate, collaborate and connect with other professionals within and beyond organisational boundaries. They argue that specific competence is necessary to perform these activities and establish a linkage between actors and systems. In the current study, we have applied the boundary-spanning perspective of these authors to delineate the specific boundary-spanning competencies needed by health social workers working in a paediatric context. Our analysis constitutes a novel lens through which to bring certain competencies to the fore and gain more insight into them. Within the applied framework, the cognitive, social and emotional aspects of competencies are taken into closer consideration. We argue that using this threefold distinction, various qualities of the competencies can emerge more clearly.
Implications for practice, education and research
Our study has several implications. First, it allows a more precise identification and operationalisation of boundary-spanning competencies and their different facets. This, in turn, may strengthen the articulation of social workers’ contributions in collaborative contexts. Second, considering that interprofessional collaboration is an important means of improving health outcomes (Reeves et al., 2009), competencies that may strengthen interprofessional collaboration and collaboration with patients and parents are warranted. Third, our study has implications for professional training and development. Providing training programmes on boundary-spanning competencies for novice and experienced health social workers will increase their understanding of professional competencies and facilitate the integration of boundary-spanning competence into their daily practice. Fourth, our study is relevant to the curricula of educational institutions. Didactic and experiential teaching and learning could enhance students’ understanding of the boundary spanner role. For example, training students to perceive different facets of information as a basis for a personalised approach, and emphasising the development of self-knowledge, could strengthen their self-confidence and self-efficacy for the position of a boundary spanner in hospitals and other complex organisations. Finally, given the paucity of studies on boundary-spanning competencies in social work, more research is required to further develop our understanding of the knowledge, skills and attitudes specific to the boundary spanner role. A thorough and systematic comparison of the boundary-spanning competence framework with existing social work competence frameworks is also needed.
Limitations
Although the 19 participants represent 12 hospitals all over Norway, more studies should be encouraged to provide additional knowledge about boundary-spanning competencies in different contexts. Furthermore, this study primarily provides insight into HSWs’ perceptions of their own competencies. Thus, an ethnographic study design could be useful for further exploration and for generating supplementary insight. Despite this limitation, understanding competencies in the framework of boundary spanning represents a contribution to the existing literature on social work competencies.
Conclusion
In this article, we have explored boundary-spanning competencies of paediatric HSWs in the context of acute and critical illness. The competencies were operationalised within four areas of ability that appeared particularly prominent within this context: (1) the ability to be informed, (2) the ability to acquire and use content knowledge, (3) the ability to customise contributions and (4) the ability to know oneself. These boundary-spanning competencies are important for carrying out tasks, activities and roles. Our study has implications for social work practice and education, although further research is needed to develop our understanding of the specificities of boundary-spanning competencies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.