
Abstract
This paper studies the creation of organisations via people processing (Prottas 1979), taking as its case study a new and developing family centre that aims to offer various social and health services under the same roof. The study draws on ethnomethodology, meaning that organisations are herein understood as being created and continuously produced in and through interaction. The data consist of 11 audio-recorded meetings from the centre’s steering group, which includes managers from different service fields and welfare agencies. In analysing the creation of the centre through people processing, this paper scrutinises how the meeting participants orient themselves toward and produce the centre’s client categories, what characteristics they connect to these categories, and how they do boundary work regarding which categories belong or not to the centre’s target groups. The meeting participants produce three different family based client categories. The first category is ordinary families, those without any special problems who just pop into the centre to see other people. These families are distinguished from the second category, best matching families, who are defined as having problems that would benefit from the integrated, multi-professional work conducted at the centre. The third category, families with too specific needs, refers to client groups whose service needs are at least partly beyond the centre’s expertise and resources. The centre needs these people-processing activities to make sense of its mission, clients and co-partners; this ongoing reasoning process allows the emerging centre to exist and find its place in the local service system.
Introduction
Categorising clients and classifying them into certain groups is a “people-processing” activity inherent in all human service organisations (Prottas 1979). Such organisations must define what their target client groups are and what measures, benefits, and treatments they can offer them (Prottas 1978: 289-290; see also Mäkitalo and Säljö, 2002a, 2002b). These categories enable them to “transform” individual people and their problems into cases and entities that the organisation can recognise, process, and work with (Hjörne et al., 2010: 305; Mäkitalo and Säljö, 2002a: 161). Categorising clients is a powerful linguistic tool, as it can be used to include or exclude people from services and subsume their individual situations into certain ready-made categories.
In this paper, we analyse the interactions taking place in multi-professional steering group meetings in a new and developing family centre (hereafter the centre) that aims to offer various services to different families under “one roof.” The meeting discussions address the planning of the centre’s key tasks and the individuals to whom its services are targeted—and to whom they are not. These meetings can be approached as boundary spaces that facilitate collaboration and the production and sharing of common knowledge among managers from different fields and welfare agencies (Edwards 2011).
We draw from ethnomethodological studies on organisational settings, as they reveal “how the work of the organisation is ongoingly produced in and through their [parties] interaction” (Psathas 1999: 142). Accordingly, we analyse the steering group meeting’s talk-in-interaction and consider how the members create and talk into being (Boden 1994) the centre’s organisation, including its target client groups. Our premise is that these meetings make visible the complex efforts of people processing (Prottas 1979) based on client categorisation (Mäkitalo 2014; Sacks 1990) and boundary work (Slembrouck and Hall 2014) at the managerial level, also revealing how these efforts are carried out through interactions.
Organisations need categorisations and boundaries
According to Prottas (1978: 220, 1979), organisations need to identify themselves with categories. They must categorise who their clients are, what issues and problems they handle, and what the institutions’ overall tasks and duties are (Hjörne and Säljö 2004; Jokinen 2012: 228; Mäkitalo and Säljö, 2002a, 2002b). Institutional categories are often understood as fixed and “embedded in infrastructures,” but ethnomethodological studies approach them as a dynamic aspect of human activities (Mäkitalo 2003: 498). They enable the sorting out and negotiating of problems in institutional encounters (Mäkitalo 2014: 26), and they play a critical role in the production and reproduction of institutional practices through, for example, meeting interactions (Mäkitalo and Säljö, 2002a: 75; Mäkitalo 2014: 42). Categories also enable effective communication within and beyond the organisation (Jokinen 2012: 230).
Mäkitalo (2014: 26) notes that categories are not just resources for understanding; they are also used to achieve something through talk. Human service organisations do the work of categorising and processing people (clients) to determine, for example, what benefits and treatments they are to receive (Prottas 1978: 289). Categorisations are consequential, as they can even provide access to or denial of services (Mäkitalo 2014: 42). Organisations are also said to “emerge through processes of drawing distinctions” (Hernes 2004: 10). Thus, they come into existence through boundary work when their place in the service system is negotiated, such as when they limit the clients and services included or excluded from the expertise of the organisation (Juhila and Hall 2017; Slembrouck and Hall 2014: 73). Overly strict boundaries could lead to situations where people fall into the gaps between institutions (Hjörne et al., 2010: 305).
The family centre as a research setting
Family centres are commonly understood as Nordic innovations, and Sweden is seen as a forerunner in their development; nevertheless, they have also been developed elsewhere, such as in the UK (Bing 2012; Halme et al., 2012). Centres are founded on the following principles: partnership, locality, low thresholds, and responsiveness (Halme et al., 2012). Such centres have recently been developed as part of the Finnish Governments’ adjustment programme for child and family services (LAPE 2015–2019) and its state-level health and social care reform. The family centre studied in this paper was developed and launched as part of this recent key governmental project.
The services and organisations constituting a family centre vary nationwide and in different countries. They can be organised in a concrete building, as service networks, as mobile “out-of-office” services, or as a combination of these service models (Halme et al., 2012). As there is no ready-made or fixed model, the starting point in the creation of an individual centre is to categorise what “we” are as a family centre in relation to the national “standards”: who our clients are, what services we deliver to them, and who the responsible actors are.
Generally speaking, family centres aim to integrate social, health, and educational services and third sector organisations. This integration of services prevents fragmentation and improves citizens’ access, client participation, and multi-agency collaboration (Axelsson and Axelsson 2006; Juhila et al., 2021). Integration endeavours are especially justified when clients are recognised to have complex problems and need various services (Juhila et al., 2021). However, family centres are not intended to target only families with multiple service needs; embodying locality, partnership, and low thresholds, they are also planned to be places where all kinds of families can gather and meet. We argue that this ideal of welcoming all families challenges developing centres in defining their area of operation. It is difficult to create an organisation without identifying more precisely its client categories and drawing boundaries around its institutional work and responsibilities. This issue becomes evident in the centre’s steering group meeting talk and interaction, when the participants negotiate what kinds of people and families the centre serves and simultaneously produce institutional client categories.
Meetings held within organisations are specific institutional events. They have a preset agenda; the participants meet and act according to their institutional roles and orient towards achieving certain “goals” that result, for example, in decisions and agreements (Asmuβ and Svennevig 2009: 10.) The creation of family centres and their integrated work requires leadership and the coordination of different working cultures and procedures (Hastrup et al., 2016), a project that the managers in our steering group meeting data are undertaking.
Categorisation and boundary work
Our study is ethnomethodologically oriented, as we are studying ordinary, everyday activities and sensemaking practices (Garfinkel 1967; Heritage 1984) in the meetings. In ethnomethodology, organisational settings and the processes that construct and maintain them are not taken for granted; rather, they are understood as a topic for analysis (Psathas 1999: 141).
In line with this methodological commitment, this paper investigates how the family centre is created by “doing” client categorisation and boundary work in the steering group meeting interaction. The objective is to explore how the organisation of the family centre is talked into being (Boden 1994) and negotiated through producing different kinds of client categorisations (Mäkitalo 2014; Sacks 1990, 1992) and boundary work (Slembrouck and Hall 2014) during the managerial-level steering group interaction.
We approach categorisation as a means of enabling people to collectively “share perspectives and make sense of events” (Mäkitalo 2003: 497) to “make themselves, others, and their surroundings comprehensible to each other” (Mäkitalo 2014: 25). Accordingly, by producing client categorisations with certain characteristics, the managers in these meetings make sense of what the centre, as an organisation, is. In analysing this sensemaking, we apply the ideas of membership categorisation analysis (MCA) rooted in Harvey Sacks’ (1992) work. This means focusing in interaction on how the meeting participants orient towards and produce client categories, what characteristics they connect to these categories, and what consequences follow from them (see Antaki and Widdicombe, 1988: 2).
Alongside MCA, we apply the concept of boundary work that we understand as a specific interactional and linguistic device in creating the family centre. Boundary work means negotiations and management of responsibilities and jurisdictions among participants in interaction (Slembrouck and Hall 2014; Hall and Slembrouck 2021). In this article, we use the concept to analyse how the managers jointly approach the dilemmas of organisational divisions and negotiate the boundaries of expertise and remit (Hall and Slembrouck 2021: 83; Slembrouck and Hall 2014: 64) as they relate to the evolving centre. Whilst doing boundary work, the managers construct and sort out the responsibilities towards different client groups (see Saario et al., 2017, 179; Juhila and Hall 2017, 65-66); it is thus closely integrated with client categorisations. Likewise, they negotiate the boundaries between the centre and other service providers responsible for those client groups that are defined to be beyond the centre’s expertise and domain. Boundary work is thus “categorisation in the sense that the professions and organisations differentiate themselves (we) from others (they) by emphasising their particular expertise [in this paper, client groups] and responsibilities in relation to others” (Juhila and Hall 2017: 66).
Data collection and analysis
The family centre that forms the setting for this study is located in a small town in a local health centre’s concrete, physical building. Different social, health care and pedagogical professionals work under the same roof in the centre, although some also operate remotely in, for instance, schools and day care centres. Third sector organisations and citizens are invited to use the centre’s “living room” (the lobby next to the entrance) for their own public-facing activities. Although we focus on the managers’ meeting talk and interaction, significant work has been done elsewhere at both the political and grassroots levels to create and develop the centre. These developments are materialised by visual figures of client pathways and service palettes that represent one form of categorisation and segmentation of clients. These figures are also discussed and reflected upon in the steering group meetings.
Our research data consist of 11 audio recordings of steering group meetings that were held between autumn 2017 and spring 2018 as the family centre was planned, opened, and started to operate. The turn-taking and topic organisation in institutional meetings differ from ordinary conversations, as they are usually administered by a chair (Asmuβ and Svennevig 2009: 10). This is also the case in our data, as meetings were planned, organised, and conducted by the leader of the centre. The other participants represented managers from health, social, and pedagogical service fields. The combination and exact number of participants varied among meetings. The researchers participated in most of the meetings, and they asked questions or were asked for their views on the issues at hand. There were also sometimes visiting participants present. The meetings were held in a meeting room, where the participants, who were quite familiar with each other, sat around a table that allowed face-to-face interaction (see also Asmuβ and Svennevig 2009: 10–11).
We read all the data carefully and coded them using Atlas.ti 9.0, a qualitative data analysis and research software, to identify (adapted from Stokoe 2012: 280) the sequences where the participants built the collections of explicit categories by 1) mentioning the client categories of the centre (e.g. child, family, citizen, etc.), 2) using category-resonant descriptions of the clients’ needs (well-off mothers, families with multiple difficulties, families that need multi-professional care, etc.), and 3) demarcating the services and actors in relation to the centre (which clients belong to the centre and which do not). We located a total of 60 sequences in the meeting interaction that comprise these three dimensions.
These sequences were then divided into three sections according to the client categorisations produced in them: ordinary families, best matching families, and families with too specific needs. These categories are based on the different levels of needs the families are seen to have and the ways these needs must be processed, whether within or outside the centre. They compose a client continuum from minor to major needs and beyond. For detailed analysis, we selected six extracts from six different meetings that best demonstrate the production of these three categorisations and the ways they are oriented and negotiated between managers. The extracts have been analysed in the original language and then translated into English verbatim.
Ethics
The meetings are part of the larger data corpus that was produced by a research project funded by the Ministry of Social Affairs and Health (2017–2018). The project received official research permission from the municipality where the centre is located. Furthermore, consent from each participant was obtained. The data are stored in the university’s secured data drive. Access to the data requires two-factor user authentication (MFA), and only the researchers involved in the above-mentioned project have access. The extracts are carefully anonymised, with all identifiers either removed or changed. Overall, the study was conducted by following the ethical principles of good scientific practice (Responsible conduct of research 2012).
Creating the family centre through client categorisations and boundary work
The results demonstrate how the participants in the meetings construct the spectrum of the centre’s service and client categories, starting from ordinary families, continuing to best matching families, and ending with families with too specific needs.
The ordinary families
This client category is constructed in the meeting talk by differentiating and negotiating between the ordinary families that recurrently attend the centre’s low-threshold activities that target every family and the “not-just-ordinary families” that need more support than just these social activities. These low-threshold services and activities that are discussed in the meetings occur physically in the centre’s “living room” and are usually organised by the third sector actors or church members.
In the first extract, the participants are talking about the relevant services and target groups of the centre and how they could reach the families that would benefit from the centre and its activities. The meeting was held approximately two weeks after the centre’s opening day. Meetings usually have “certain technologies for displaying information” (Asmuβ and Svennevig 2009, 10). Also in this meeting, before and during the extract, the participants are discussing a PowerPoint presentation about the centre and debating what ought to be included in it. The leader of the centre, who is in attendance, will present the slides to the municipal council. Before the extract, the participants (the researcher, the leader of the centre, and managers from health care and pedagogy) had been discussing the target groups of the centre. The conversation continues about the slides and the impression they might give:
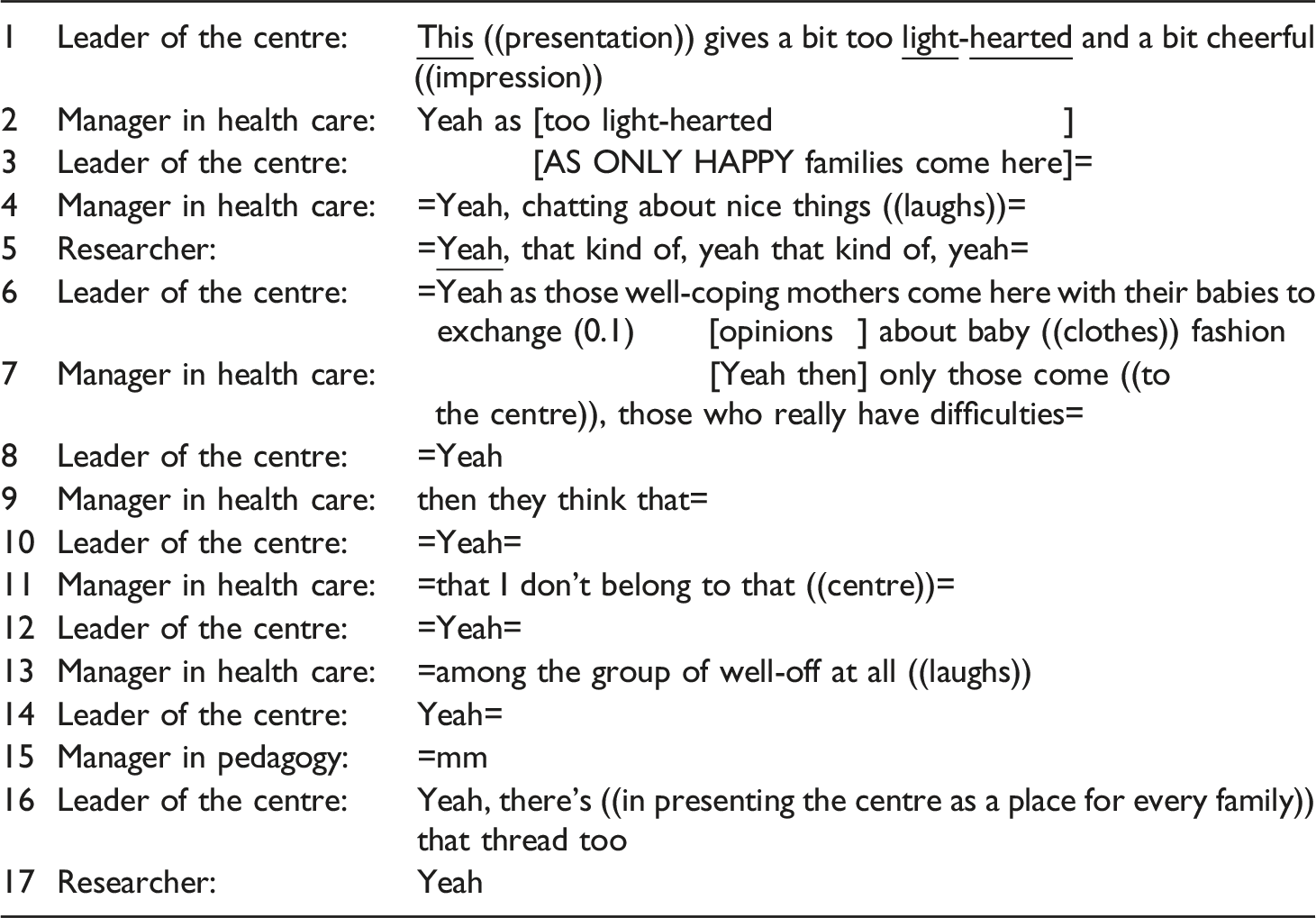
The participants make sense of their potential client groups by establishing a difference between “ordinary” and “not-just-ordinary” families. The category of the ordinary family is attached jointly by the leader of the centre, the manager in health care and the researcher’s partly overlapping and rapid turn-taking to characteristics such as “happy,” “healthy,” and “well-off,” and such families come to the centre to socialise. The mothers of these families are linked with category-bound activities (Stokoe 2012, 281) of “chatting about nice things” and changing opinions about baby clothing. The participants mutually recognise that in marketing the centre as a place for ordinary families, there is the risk that the centre itself will be pictured as too light-hearted, a place that excludes the not-just-ordinary families. This category includes families that do not define themselves as ordinary families and who experience difficulties in life. In particular, the leader of the centre raises concern about whether the presentation to the municipal council gives an excessively general impression of the centre and its clientele. The manager in health care gives preferred responses as she agrees with and confirms what the leader is saying (turns 2, 4, 7, and 9). The participants are all doing exclusionary boundary work here, as they do not depict the ordinary families as the “core” target group of the centre or as its main responsibility, although these families are welcome to gather at the centre. Instead, the centre is constructed as a place for those families who are characterised to “really have difficulties.” The participants come jointly to the conclusion that it will threaten the centre’s main philosophy and aim if these families exclude themselves from the centre.
In the next extract from another meeting, the managers from health care, and pedagogy service fields, the leader of the centre, and a researcher are in attendance. The extract demonstrates, in addition to the first extract, how the participants negotiate the straightforward idea of the centre as a “common” living room for ordinary families and how this image could threaten the centre’s institutional task to serve those who need professional support:
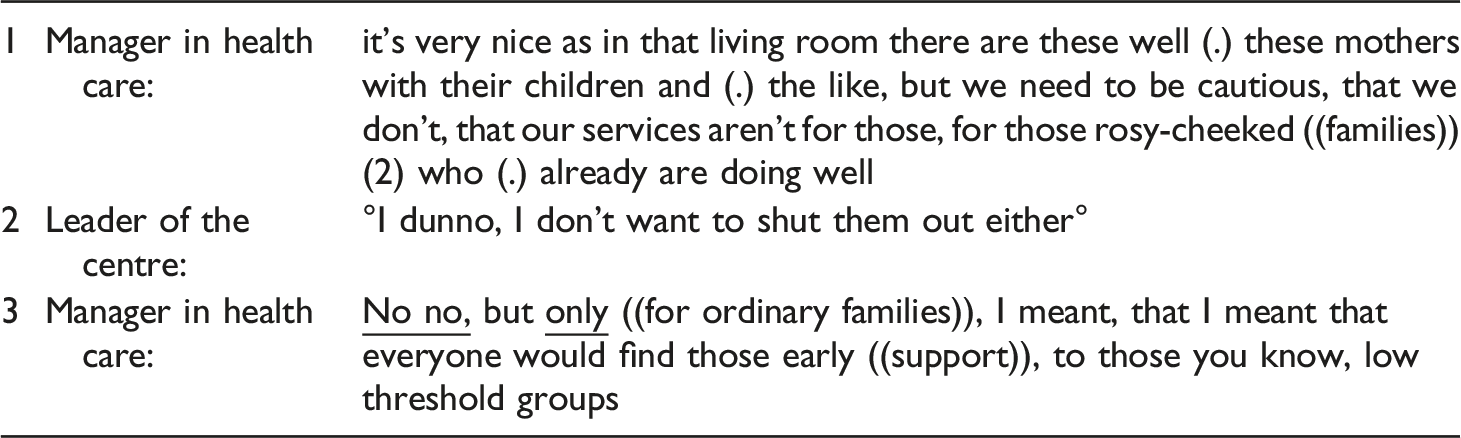
The manager from health care service field categorises the “living room” users as mothers with children and characterises them as “rosy-cheeked” families who are doing well. She is doing exclusionary boundary work by noting that “we”—the family centre—need to be “cautious” that the services are not for those who are already doing well. Her turn suggests that there is a need to set some problem-based criteria for the centre’s users; it should be targeted at those who are not currently doing well. The leader of the centre gives a non-preferred response (Pomerantz 1984) because she does not want to exclude this well-doing group from the centre. In turn three, the manager in health care displays agreement with the leader by correcting herself. She clarifies that she would also include ordinary families in the centre; she would simply not aim the services “only” towards them.
The best matching families
The client category of the “best matching families” is tied with the needs that fit well with the centre’s resource and service repertoire. These families are characterised as having multiple needs, yet not too complex for the centre. The managers produce these families to require the multi-professional services that constitute the “cornerstone” of the centre’s professional work and its main offering. The services for these families are regarded as preventive and primary. When the participants produce the category of the best matching clients, they also talk into being the different tools and artefacts that can be used to identify and segment the clients’ needs and suitable services fitting the recognised needs.
Before the next extract, the participants were talking about a consultative group that needs to be established for the “premium” clients of the centre. The issue had been discussed earlier in another meeting held with the manager who is in charge of the region’s child and family development program. Two managers from health care, one from the social service field, a researcher, and two project workers from the regional child and family development program are present at this meeting.
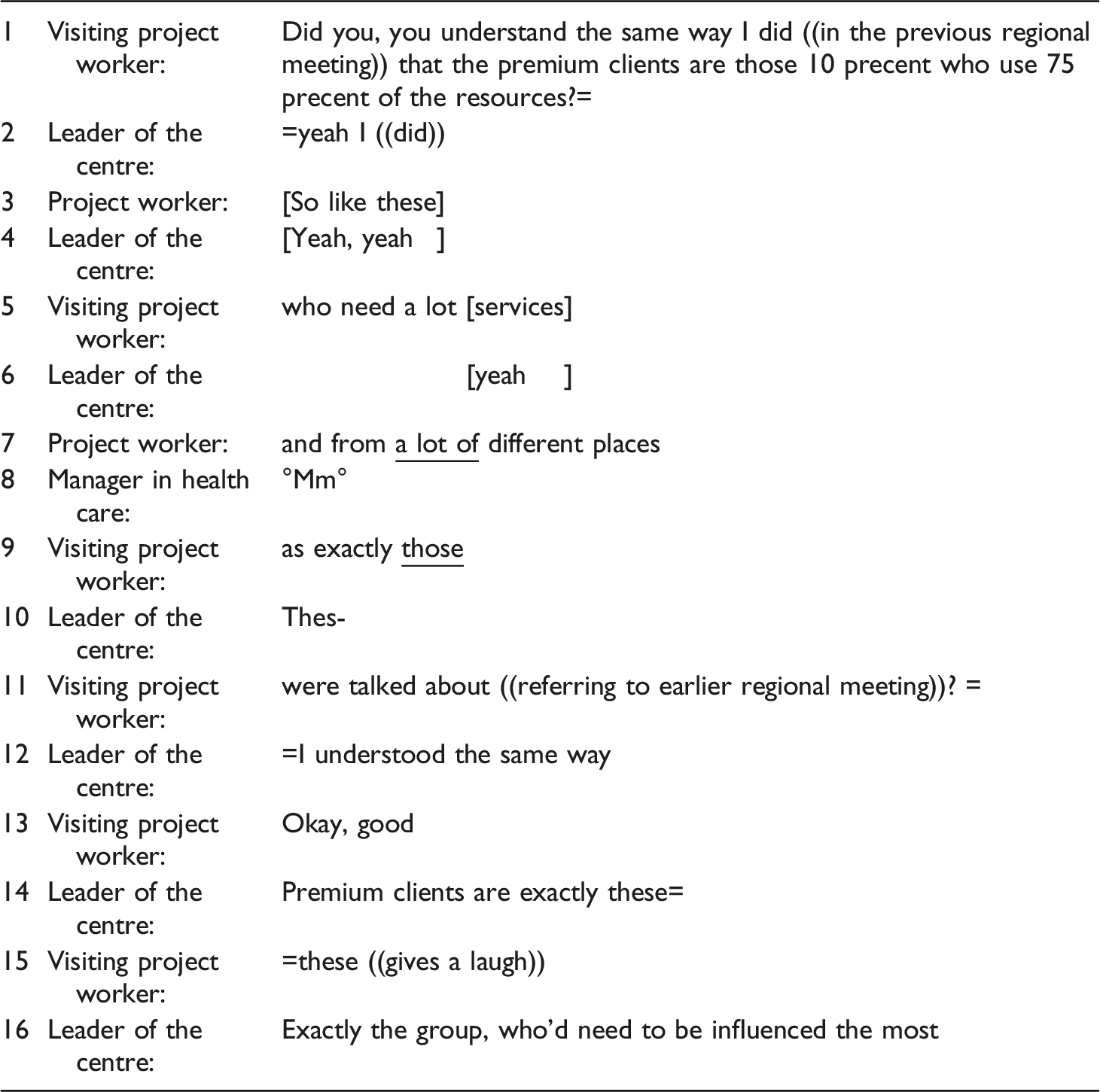
The visiting project worker verifies whether she understands correctly what is meant by the client category of “premium client” presented in the earlier regional meeting. She uses category-bound activity (Stokoe 2012, 281) to refer these clients as those who “use most of the centre’s resources.” She characterises this client category as including those who need a lot of services from different places. The leader accepts this characterisation of the centre and has the same understanding. She adds that this group of “premium” clients are those who need to be “influenced” the most and produces them as the core, or best matching, clients of the centre. The participants are doing inclusionary boundary work here by recognising and naming jointly this client group as belonging to the centre.
Before the next extract from another meeting, the manager from the field of social services brought up the need to clarify the practices and agreements concerning different multi-professional teams operating at the centre’s grassroots level and aiming to work with clients with multiple needs. Managers from health care and pedagogy service fields participate in this conversation about how to recognise and choose the “right” clients to work with the teams. Another manager from health care service field and a researcher are also present at the meeting. The participants wonder how the teams can best be established and for whom:
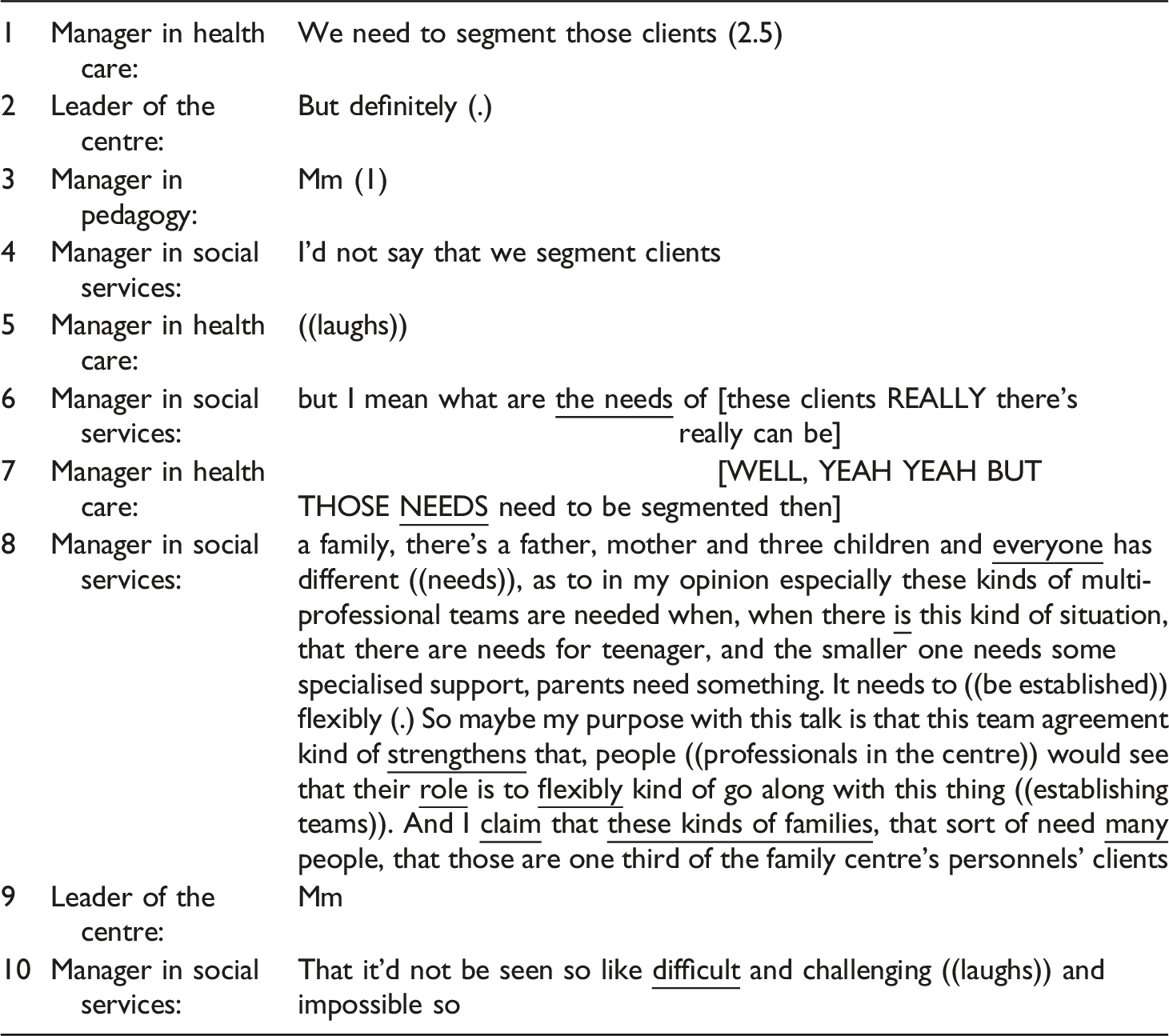
The manager in health care suggests that the “segmentation 1 of clients” would assist in the formation of different multi-professional teams and their target groups. The leader of the centre and the manager from the field of pedagogy agree on that point. On the other hand, the manager in social service field gives a non-preferred response by disagreeing and correcting the idea of segmentation (Pomerantz 1984). She would not segment the clients, and instead she emphasises the importance of recognising the various needs within families. In her next turn, the manager in health care displays acceptance that the emphasis should be on needs but does not give up on the idea of segmentation. The manager in social services explains further her point of view of a needs-based approach. She describes the reality of many families with multiple needs and categorises these families as those who need the most multi-professional, team-based services and who represent “one third” of the centre’s clients. She does inclusionary boundary work, articulating that the professionals need to recognise and involve especially those families that need the centre the most and fit best with its scope.
Families with too specific needs
The client category of “families with too specific needs” is characterised as families that have needs and problems too specific to be straightforwardly handled by the centre. However, this category is the least clear cut and rather under constant negotiation. This negotiation manifests in, for example, how the managers produce uncertainty about which family or case is actually “too specific.” If the centre would just have enough resources, the criteria for defining families as having too specific needs to be dealt with at the centre would be high.
In the following extract, the participants again discuss a PowerPoint presentation (presumably the same presentation as in extract 1) that the leader of the centre is preparing for an upcoming municipal government briefing. The purpose of the presentation is to, for example, present the various actors and services of the centre.
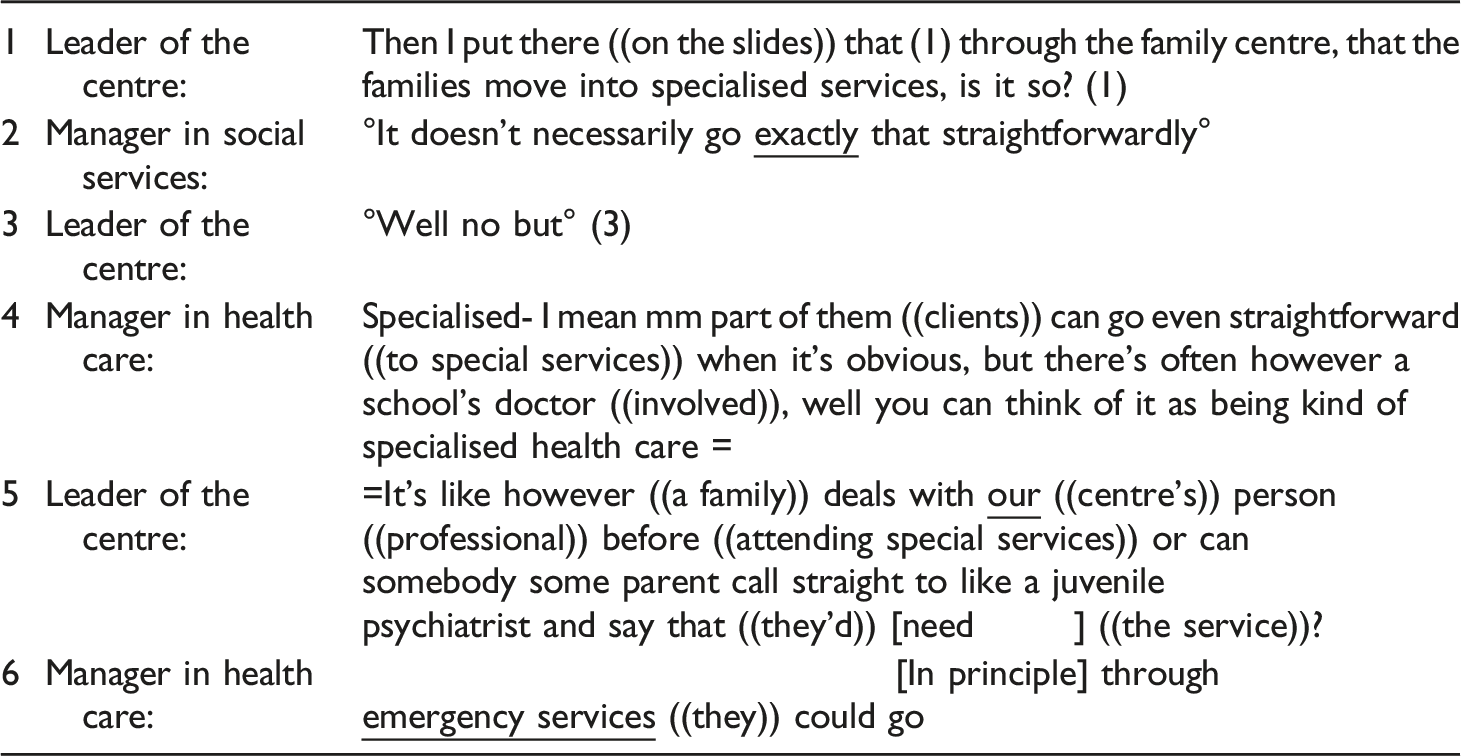
The leader of the centre describes how she has “put” on the slides the process by which clients move into specialised care through the centre and asks for the other participants’ approval: “Is it so?” The manager from the field of social services gives a non-preferred response as she does not agree (Pomerantz 1984) that the process is so linear. The leader of the centre agrees somewhat: “°Well no but°.” After a short pause, the manager in health care service field takes a turn and notes that some cases can proceed straightforwardly “when it’s obvious,” without specifying what these cases are.
The clients who need specialised services and who are thus categorised as families with too specific needs are attached to characteristics such as “being obvious,” experiencing an “acute crisis,” or needing “emergency services.” These features and needs are excluded from the centre’s responsibility. In addition, families with too specific needs are defined as those going through the centre, needing it mainly for a referral, or bypassing it all together. The path to specialised services involves the centre, “our” professionals who assess the clients’ needs before they can be sent on. The participants are jointly doing inclusionary boundary work here to strengthen the centre’s role and expertise in processing clients along the service path to specialised services. The extract also demonstrates how the boundaries and divisions of responsibilities between primary and specialised services come into being when constructing the client categories of different services.
In the next extract, the topic concerns special care “problems” and explores how they could be treated at the centre if there were enough resources and professionals. The participants (three managers from the service fields of health care, as well as a researcher and the leader of the centre) have been talking about children with emotion regulation problems and in which instances they should be treated. These problems are not included in the psychiatric illnesses, and the category of children with emotion regulation problems is not obviously entitled to special care. Two managers from the health care service field wonder about the managing of responsibilities between the family centre and child psychiatry:
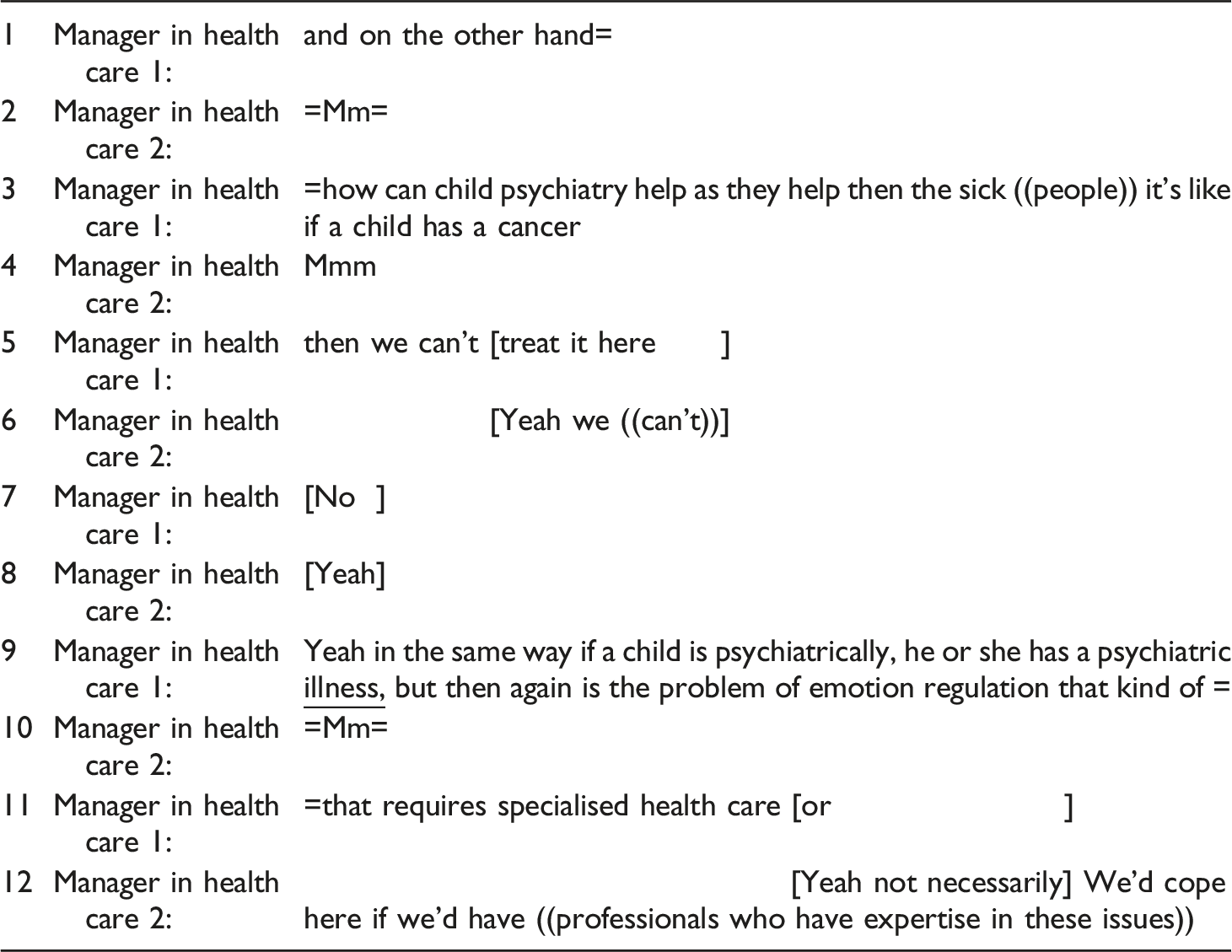
The managers are producing the demarcation between the centre’s primary services and the specialised services offered in other places. The category of families with special needs is linked with problems that are demanding but not easy to define or manage within the service system. The clients defined as having emotion regulation problems do not belong in the specialised services given that they are not ill in a traditional sense, as the manager from the field of health care 1 notes in turn 3. In the discussion, problems of emotion regulation are not treated as psychiatric illnesses that need special health care but as something that could be included in the centre’s expertise and responsibility as well. Serious illnesses and diseases, such as cancer, are easy to exclude from the centre’s responsibility, but the question for the participants is whether “the problem of emotion regulation [is] that kind of” family problem. It seems that the managers would be willing to take these particular families with special needs into their scope of responsibility. However, the issue seems to be that the centre does not have enough resources and expertise for this client group; otherwise, they could treat them. Constructing the end point of the client continuum raises the following question: Who can help if specialised services and the centre cannot?
Discussion and conclusions
The analysis of managers’ meeting interaction demonstrates how the family centre’s target groups, tasks, and responsibilities are ongoingly produced in and through multiparty interaction (Psathas 1999: 142). The meeting interaction demonstrates how people-processing activities are done by client categorisation (Prottas 1978, 1979) to make sense of and identify what they are as a family centre, who their “actual” clients are, which professionals are needed, and with whom they are cooperating. Thus, the steering group meetings reveal the various efforts carried out through interaction to set common targets and purposes for the emerging centre. They also showcase the allocation of resources, the professionals’ roles and responsibilities, and the provision of services. Managerial-level negotiations about the management of organisational divisions and the boundaries of expertise and remit (see Hall and Slembrouck 2021: 83; Slembrouck and Hall 2014: 64) play an important part in the creation of the centre. This constant and ongoing reasoning is what facilitates the emerging centre finding its place in the local service system. Thus, the analysis demonstrates how welfare organisations are built and sustained by managerial-level negotiations and sensemaking work.
The category of ordinary families—at the first end of the client continuum—is produced as the families who are using the centre’s “living room” and attending the low-threshold groups organised by the third sector or church. The managers jointly, turn-by-turn, make distinctions between ordinary families who are doing well and families who “have difficulties” and need the activities. The meeting interaction demonstrates how the centre, as an inclusive organisation welcoming all “rosy-cheeked” and “well-coping” families and thus having hardly any boundaries, causes potential risk of excluding certain families. This issue raises negotiations and varying views concerning whether there is a need to draw some boundaries or criteria for the centre’s low-threshold activities. These negotiations also make visible how the client categorisations both include and exclude citizens from the services.
In the middle of the client continuum is the category of best matching families, those who are defined as a best match with the centre’s principal aim and mission. They are produced in the meetings as the “premium” client families with multiple needs, “one third” of the clientele, who need to be recognised and influenced the most and who are approached as ones truly needing the centre’s multi-professional, integrated, and consultative teams and professional services. These families have specific needs that are not seen as too complex for the centre, and the services required are still regarded as preventive and primary. Managers talk into being these client groups with various problems and describe how their needs must be segmented or recognised while also identifying that overly strict preset categorisations can hide the complexity of situations.
At the end of the continuum are families whose needs are categorised as too specific for the centre. These clients are assessed to benefit from “next level” services—for example, specialised health care—that are not offered at the centre. The meeting interactions demonstrate negotiations about which situations and needs demand specialised care and support and where to draw the boundaries between the centre’s primary services and specialised services outside the centre. These negotiations demonstrate that sometimes responsibilities are easily allocated to specialised services, for example, in the case of serious diseases. The boundaries are easier to draw when the clients can be offered services and help elsewhere. The meeting talk also illustrates that moving cases into specialised services is sometimes ambiguous and even problematised, especially when the problem category is not medically diagnosed. The centre’s boundaries are extended when arguing that it could be able to handle more complicated cases, such as children with problems of emotion regulation, if there were more resources and expertise. The role of the centre in relation to the local service system is emphasised, as “we” professionals need to be consulted before a client can move into specialised services unless there is an acute crisis or need for emergency services. This client category is not clear cut; it is a “messy” and ambivalent category that the managers need to reason through. They must negotiate what client characters constitute the very end of the client continuum, the termination point for client hood at the centre, and its responsibilities. This is a relatively complex ethical issue.
Categorisation and boundary work are powerful tools, as they can include or exclude people and services from the centre (Hjörne et al., 2010: 305; Mäkitalo 2014, 26). It seems that the managers are acting ethically, as they try to avoid service gaps by doing inclusionary boundary work and extending the centre’s boundaries. On the other hand, they do negotiate whether there is a need to exclude families that are either “too well-coping” or have needs that are “too specific.” The three family based client categorisations produced in the meetings reflect the earlier versions of the centre’s client pathways and service repertoire, which are also displayed in the meetings (Asmuβ and Svennevig 2009)—the managers to make sense of, negotiate, and recreate.
Overall, the variety of services at different levels of the welfare system and the confusion related to the allocation of services and resources illustrates how the family centre is created in interaction in relation to other organisations, as well as to the whole welfare system. It is also talked into being in a situation where there is a lack of “ready-made” models and expectations available for the local family centre organisation to categorise its own target groups and services and through that, to build its own models and procedures. However, performing categorisation to determine which clients are processed in the centre is also an ethical issue, as people who need services would be “forced” into certain “ready-made” client groups, and there is the risk of falling between categories and not finding a proper service solution. Although client categorisation is accomplished in relation to the centre’s resources and expected expertise, it has consequences for the whole service system. In their meeting interaction, the managers create certain organisational-level boundaries for the centre, but more empirical research is needed to investigate how client categorisations and boundary work are present and applied in street-level client–worker interactions at the family centre.
Footnotes
Acknowledgements
We would like to thank the Family Centre’s managers for their contribution to the study and the members of the DANASWAC, MARGI and INSOTE groups for their valuable comments regarding our paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by the Ministry of Social Affairs and Health of Finland (STM/4250/2016 and VN/25203/2020).