
Abstract
Assisting people into bed is in many ways centered around the person’s body—it is the body that needs to be moved and laid down. As a result, the body’s material and tangible properties—the body as an object—are foregrounded. This study demonstrates, however, how care workers, when assisting a person with late-stage dementia into bed, maintain a balance between handling the body of the care-recipient as an object of care and including the person as a co-participant in the activity, highlighting the participatory role of the person, and thus positioning the care-recipient as a partner in the activity of the transfer. Drawing on multimodal conversation analysis, and presenting two cases of transfer, the study shows that the activity of moving into bed is usually organized into three consecutive sequences of (a) preparing the move, (b) transfer proper, and (c) adjusting the resident in bed. In every phase of the activity, caregivers, through careful and coordinated embodied and verbal interactions, manage the care-recipient not only as an object of care and her body as an objective body but also as a lived body, highlighting the agentive and subjective aspects of the resident’s personhood. The results of the study point to care workers’ skillful handling of interactional resources to deal with the social sensitivity of moving assistance-dependent residents to their bed through partner-positioning the resident, and thus (re)subjectifying the person with late-stage dementia despite the objectifying aspects of the transfer.
Keywords
Introduction
In this study, we explore how care workers, when assisting a person with late-stage dementia into bed, deal with handling the body of the care-recipient as an object of care, and also including the person as a co-participant in the activity. We particularly show how caregivers attend to the resident’s agency in the process of the transfer through what we call partner-positioning, that is, using practices through which they acknowledge the co-presence of the care-recipient in interaction, and position them as a collaborative participant in the activity. We aim to instantiate how partner-positioning in interaction may result in (re)subjectifying the care-recipient in the setting of caregiving activities.
Providing care for another lived body is very much about collaborative interaction between the caregiver and the care-recipient. This could however be challenging if the care-recipient has difficulty with the fundamental aspects of human interaction such as recognizing an ongoing course of action, understanding the contribution of others and/or being able to intelligibly respond to them. This may be the case with care-recipients who are severely constrained in their communicative resources, for example, in cases of people with some congenital developmental conditions, people with some types of brain injuries, or people with neurodegenerative disorders, like dementia. Care providers are also guided by the institutional normative context for communication, meaning that care practices are expected to be performed in collaboration with the care-recipient based on mutual understanding, and with respect to the individuals’ agency as well as their right to privacy and intimacy (see guidelines for patient-centered care, for example, in the report of the Institute of Medicine, 2001). For caregivers, therefore, engaging in collaborative interaction with people living with severe communicative disabilities is a constant effort to live up to the care principle of balancing between normative aspects of caregiving and conducting their preplanned daily tasks. This study deals with such a balance and we take a case in point in professional care work involving people living with late-stage dementia. As an example, we present a common but complex situation in which a person with late-stage dementia is assisted from wheelchair into bed by professional care workers.
Dementia is a progressive neurodegenerative condition that diminishes the person’s cognitive, communicative, and physical abilities. With the progression of dementia, at the later stages of the disease, people require assistance even with basic everyday tasks such as tending to personal hygiene, eating, walking, or getting in and out of bed, something that is referred to as personal activities of daily living. As the ability to care for oneself and the performance of activities gradually decrease, assistance to conduct the activities of daily living is increasingly needed. The progression of dementia at the later stages of the disease thus narrows care practices to mainly tending to the corporeal aspects of care work. This shift, which is the consequence of the change in the ability of the person with late-stage dementia, turns the body into an object of care. From an interactional perspective, previous research studies on caregiving practices for the elderly in general (e.g., Backhouse, 2010), and people with dementia in particular, have often focused on the aspect of interactions particularly regarding mutual relations in the progression of care tasks (e.g., Heinemann, 2009; Jansson and Plejert, 2014). How to balance off the social needs of people with dementia in interaction and their participatory status in caregiving situations has not been studied much from an interactional perspective (cf. Backhouse, 2017; but see Kristiansen et al., 2018; Rasmussen et al., 2019). Our study contributes to that line of research and attends particularly to the treatment of people with dementia in caregiving practices. By drawing on conversation analysis (Sacks, 1995) and multimodal analysis of interaction (Cekaite and Mondada, 2021; Goodwin, 2018), we show how caregivers manage the transfer activity, and at the same time, maintain the agentive and subjective aspects of the care-recipient’s personhood.
Organizing supporting activities involving persons with severe communicative disabilities
Studies on the transfer of care-recipients in general centers around nursing and caregiving skills regarding the steps that nursers and care workers should take for the safety and the comfort of the care-recipient in the transfer activity (e.g., McConnell, 1995). Apart from the studies on appropriate methods of transfer (e.g., Cheung et al., 2020; Lia et al., 2015; McConnell, 1995), to our knowledge, there are not many studies on the interactional organization and performance of transfer and how care-recipients are treated by the caregivers during the task of moving into or out of bed (see but Kristiansen et al., 2018). From an interactional perspective, assisting a resident to move is a collaborative joint activity (Hydén et al., 2022; Majlesi et al., 2019, 2021); however, the progression of dementia at the later stages results in severe communicative and cognitive challenges including losing the ability to speak, and leaving the person with dementia with very limited resources to act on (Hydén et al., 2022). The collaboration assumes the recognition of the roles and the agency of all participants involved (Kristiansen et al., 2018). An inability to recognize the agency of the person living with dementia would risk turning the person into a passive participant in care activities as well as being reduced to a mere object of care. The person could thus be described as an objective body, a flesh, something that Merleau-Ponty would point to as “appearing publicly as a thing among things of the world” (Merleau-Ponty, 1968: liv; also p.137). Thus, a particular challenge for care staff is to maintain a balance in providing care for the person with dementia, oscillating between treating the care-recipient as an object of care, that is, providing care for them as an objective body, and at the same time, considering the care-recipient as a lived body, a subjective being with embodied selfhood (Kontos, 2004). This certainly requires interactional work so as not to treat the person with dementia just as an object of care but rather to position them as a partner in interaction, although not with equal footing in the activity, compared to healthy participants.
In order to maintain balance in the abovementioned, the care worker must demonstrably position the care-recipient as an engaged present party, notably a partner to build an alignment with during the activity and showing sensitivity toward their presence as a person with a lived body and not just an object of care in the care task. This can only be accomplished through the organization of interaction and communication with an emphasis on at least two different practices or procedures. The person who is a care-recipient should be considered in practice as an active and ratified participant (Goffman, 1963) in—or at least parts of—the support activity. That is, despite their communicative disabilities as communicative partners, there must be interactional effort to recognize their contributions to the activity (although their contributions may be minimal and through nonverbal means, for example, gaze shifts, hand movements, etc.), as well as to position them as an addressed participant and a communicative partner in interaction (cf. Kristiansen et al., 2018). A second practice is for the staff to design directives—verbal as well as embodied—that will involve the person with severe communicative disabilities as a participant in the activity (cf. Ekström and Majlesi, 2016; Majlesi et al., 2019, 2021).
Including and orienting toward persons with severe communicative disabilities as ratified addressed participants in interaction may be a challenge, as they tend to produce minimal contributions to the ongoing collaborative activity due to their constrained semiotic resources, in particular, the use of spoken language. They are also constrained in understanding, or the display of understanding, others’ contributions (e.g., in case of people with late-stage dementia; see Hydén et al., 2022). Thus, to orient toward their contributions, the care workers must do at least two things.
First, care staff can support the person with severe communicative disabilities by actively organizing and re-organizing resources in the situational ecology: by using more adapted recipient designed (Sacks, 1995) spoken language, for example, simpler utterances or shorter turns in talk with clear content, for instance, when using requests or other forms of directives (see, e.g., Antaki and Kent, 2012; Ekström and Majlesi, 2016), by attending to the care-recipient’s minimal response or embodied reactions (see Rasmussen et al., 2019) and also by using their own bodies to indicate and demonstrate actions, and rearrange artefacts in the surrounding environment (see, e.g., Hydén et al., 2022; Majlesi et al., 2019, 2021). In this way, the caregivers show their understanding of the care-recipient, acknowledge their engagement in interaction or the ongoing activity, and thus include the person with a communicative disability as an active agent in the social situation.
Using bodily indication, for instance, when attending to the embodied cues produced by the person with severe communicative difficulties (see, e.g., Goodwin, 2018), and manipulating the position of the body of a person by arranging or rearranging their body parts, for example, with pointing with the finger, touching, etc. are central to the accomplishment of joint activities that are conducted together with them (cf. embodied directives produced for children in (Goodwin and Cekaite, 2018). These bodily indications and directives can be used both to instruct and to assist the person with disabilities to perform an action (Ekström and Majlesi, 2016; Majlesi et al., 2021) and also position the person with disabilities as an active—and ratified—participant in the activity (cf. Nilsson et al., 2018). Central to the use of embodied directives is their sequential placement in the ongoing practical activity. That is, it is by being issued at a specific point in the ongoing activity that a bodily indication—perhaps together with some verbal utterances—may function as, for instance, an instruction of where to place a hand (as in getting hold of the walker) or when to open the mouth (as in eating).
Second, persons with severe communicative disabilities generally produce, if any, minimal interactional responses and contributions, a shift in gaze or a vocalization (cf. Rasmussen et al., 2019). Quite often, it is even unclear to the caregivers whether the response or contribution should be counted as having a communicative intent or being meaningful. As a result, in this kind of interaction, there is a constant risk of missing or ignoring minimal contributions or responses, or behavior that potentially could be understood as communicatively meaningful. This might result in the person with communicative disability to be treated, at best, as being un-responsive and un-communicative and at worst, as being a “non-person.” This is what has been called the result of “malignant social psychology” (Kitwood, 1990) and “malignant positioning” (Sabat, 2001) with the consequence of social exclusion from interaction and thus human relations (cf. Sabat, 2019).
To counteract this, care staff usually strive for interpreting and responding to the potential or actual minimal contributions of the person with dementia as if they are expressions of (Drew and Heritage, 1992) a communicative intent and thus meaningful. Borrowing a term from, what care staff do is to apply a special “inferential framework” or practice for taking into account minimal contributions of the care-recipients, that is, they will interpret and understand any visible bodily movements, change of gaze, vocalization, etc., as if relevant for the practical purpose of initiating or responding to an action in an ongoing activity.
With this study, we aim to contribute to the line of studies above by demonstrating how the aforementioned interactional conducts—(1) to position the patient or client as a ratified addressed participant, through engaging with them by direct addressing or using embodied indications and (2) to treat their minimal contributions as meaningful responses—change the participatory role and thus situated identity of people with dementia from being treated as an object of care to being treated as a participant in the care activity. Our analysis shows how this change of footing (Goffman, 1981) constitutes the interactional organization of an action we call partner-positioning. The concept of partner-positioning, we suggest, is to be considered as a counter-conceptual contribution to the theory of malignant positioning (cf. Sabat, 2001), that is, to include rather than to exclude a person in social interaction.
Data and method
The data for this study comes from a dataset collected during a span of a year of fieldwork when we recorded different activities including transfer in a dementia unit at a residential care home in a large city in Sweden. The dementia unit accommodated seven people, all primarily diagnosed with Alzheimer’s disease—five of whom were at the later stages of dementia. The video data used for this study consists of two occasions of assisted transfer of two persons with late-stage dementia. Transfer is one of the most typical examples of activities in which the person and their body becomes the focus of interaction and an object of care. We have selected two transfer activities out of our video recordings of seven occasions of transfer of residents with late-stage dementia into bed, each consisting of moving from the common area (the sitting/dining room) and to the resident’s apartment in the care home. The length of the clips is between around 3 min to over 6 min in case of transfer with lifting machine. For lack of enough space, we present two of those cases featuring two different residents. Both residents were primarily diagnosed with Alzheimer’s disease. At the time of recording, they are in an advanced phase of the trajectory of the disease which makes them unable to verbally communicate with others, and too feeble to physically move on their own. One resident, Soraya, is in her 80s and the other, Emma, in her 90s. Soraya is originally from Iran and her mother tongue is Farsi. Emma is from Sweden with Swedish as her first language. Both residents have lost their abilities to verbally communicate. Nonetheless, as our presented data and also our long observations during a year of fieldwork would attest, they are treated by the caregivers as able to comprehend the talk as they are regularly addressed verbally.
Prior to the data gathering, ethical approval was obtained from the Regional Ethical Review Board, and for the process of data gathering, the project strictly followed the Swedish law of Data Protection Act. To protect the identity of the participants, we have given them pseudonyms, and the pictures used in the transcripts are all drawings based on the frame grabs of the videos.
To work with video data, we transcribed the relevant sequences and attended to embodied actions as annotated in the transcripts. We have also added drawing illustrations in the transcripts to make the procedural activity of the studied phenomenon tangible. The work of analysis follows the multimodal conversation analytic tradition (e.g., Cekaite and Mondada, 2021) analyzing the course of activities sequentially and temporally in order to uncover patterns of using caregiving practices (see section Organzing supporting activities involving people with severe communicative disabilities) in the course of care activities.
Analysis
In what follows, we present our analyses of the assisted transfers of two persons with late-stage dementia as they are helped to lay down in their beds. The first occasion (Ex.#1a–1c) shows when Emma is assisted with sit-to-stand transfer followed by stand-to-lie transfer into her bed, and the second occasion (Ex.#2a–2c) shows how Soraya is assisted with the use of a transfer machine from her wheelchair into her bed. In our analysis, we have divided the activities into three phases represented here in three consecutive extracts (a–c) in both examples. In the care home we conducted our fieldwork, the residents are often transferred by two caregivers (it may occur that the transfer is performed by one caregiver, depending on the situation, how the safety of the resident can be secured, and the resident’s level of physical ability to stand or sit with little or much assistance, etc.). The activity of helping the person with late-stage dementia to move to bed (Phase 1) starts with moving the residents in wheelchair into their room, and placing the wheelchair parallel to the bed, and preparing the person to move (Ex.#1a and 2a). This is followed by the transfer itself (Phase 2) which is constituted in a joint effort of lifting the person from the wheelchair and placing them on the bed (Ex.#1b and 2b). The last phase of the moving (Phase 3) deals with adjusting the person’s position on the bed and making the situation comfortable for the resident by tending to how the body is positioned, covered and tucked, etc. (Ex.#1c and 2c).
Extract 1a: Placing and preparing the resident for transfer
Participants: Emma (person with dementia), Paulina (Staff member), Sofia (Staff member)
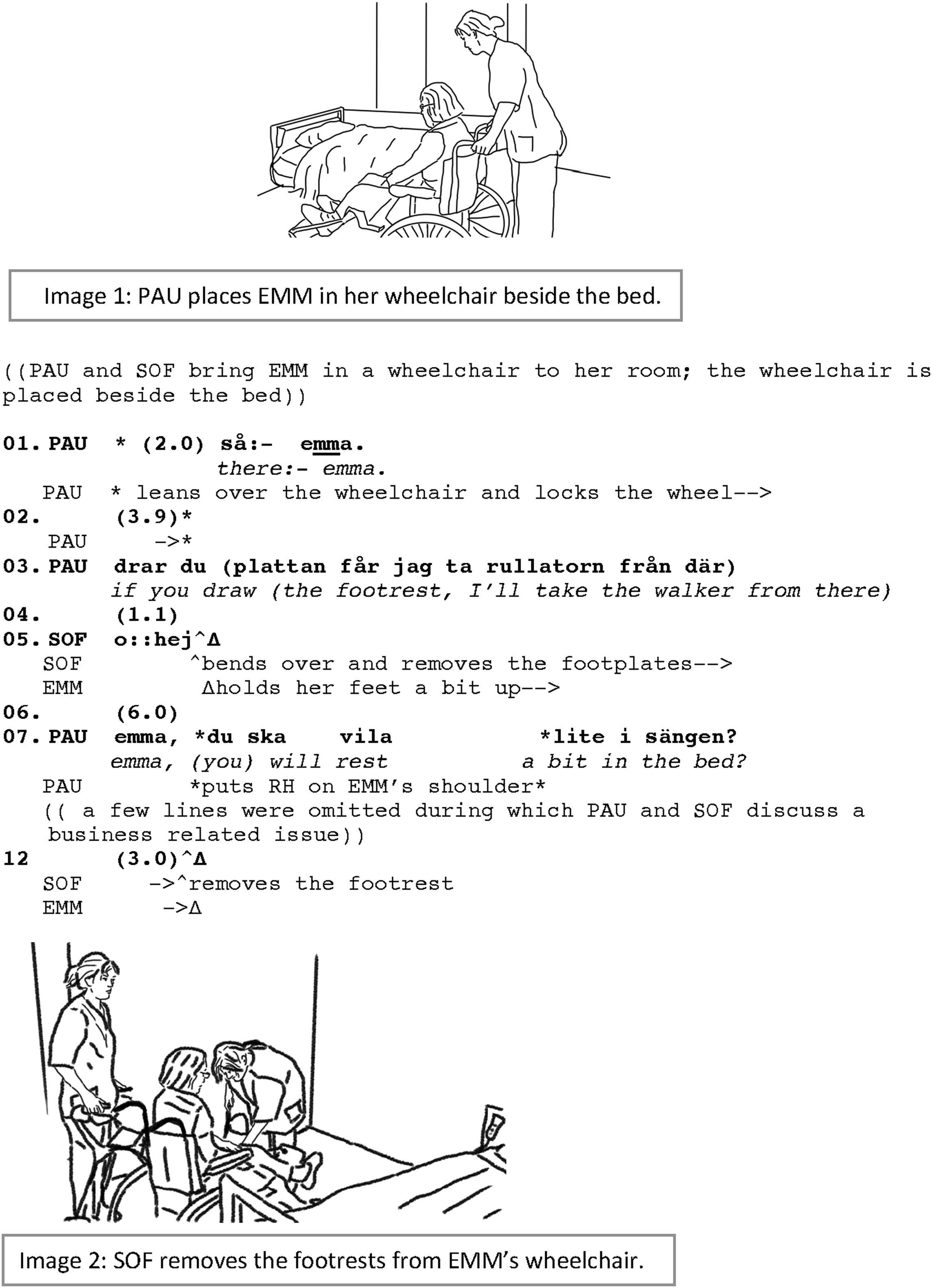
At the very beginning of the assisted transfer activity, Emma is moved into her room in a wheelchair and placed close to her bed (see IMG.#1). After placing Emma next to her bed, Paulina leans over to lock the wheel on the wheelchair while she simultaneously addresses Emma (line 1). Paulina, addressing Emma, does not seem to have the purpose of addressing per se, as Paulina does not continue with either a question or a piece of information; neither does she repeat her address when there is no response from Emma. Instead, Paulina’s turn has the function of acknowledging Emma’s presence in the participation framework of the activity (cf. Clayman, 2012), and also signals the initiation of the preparation for the activity of transfer.
To be able to help Emma to move safely, there are several preparations regarding the material surrounding. The stability of the wheelchair needs to be guaranteed, the footrests should be removed, and Emma also needs a walker for support when moving to the bed. These preparations are performed by Paulina and Sofia without much involvement from Emma. The coordination of the preparations (line 3) is primarily organized in a framework involving the staff with Emma as an unaddressed recipient. As Sofia removes the footrests from Emma’s wheelchair (line 5), she lifts Emma’s feet from the footrest. It is not possible to tell from the video the extent to which Emma is able to move her feet on her own, but as shown in the transcript, Emma displays attempts to lift up her feet and holds her feet a bit up over the footrests as Sofia takes them off (line. 05). Sofia frames the action of removing the footrest to involve an extensive effort by her which is displayed in her “o::hej” accompanied by heavy exhaling as a demonstration of physical strain (c.f. Hofstetter et al., 2021). Sofia’s actions foreground the material and physical properties of Emma’s body (specifically her feet), by framing it as being somewhat heavy for her to move. Simultaneously, her turn “o::hej” is produced publicly for others, including particularly Emma, to hear (Paulina is outside of the room fetching Emma’s walker), thereby acknowledging Emma’s presence through interactionally drawing her attention to her current action.
When the stability of the wheelchair is guaranteed, simultaneously as Sofia completes the removal of the footrests, Paulina, again, addresses Emma and announces the upcoming event for Emma with a statement (line 7). Doing so, Paulina places a hand on Emma’s shoulder and leans into her visual field with her gaze directed toward Emma’s face. The preparation phase, therefore, includes not only placing and physically preparing the wheelchair and the resident before the transfer, but also preparing the resident cognitively by announcing the upcoming activity. Throughout the physical preparations of the upcoming transfer that foregrounds Emma’s material properties—she is moved around in her wheelchair and her body parts are relocated in the chair without her being asked beforehand—Paulina and Sofia use several practices to counter the potential risk of Emma being reduced to an object of care. Caregivers, through addressing the resident, using gentle touch to secure her attention and trying to gain eye contact, include Emma as a ratified participant and an addressed recipient in interaction (see Goffman, 1963) rather than an object of care that the care task is operated on.
After Sofia removes the footrests, Paulina places a walker in front of Emma. While removing the footrest and fetching the walker, the staff members also talk about their last staff meeting (between lines 7 and 12; not shown in the transcript). Such conversations which are done parallel to the current care tasks in hand are observably common in the care home in multiparty interactions (see Haddington et al., 2014 on multiactivities). During the dyadic conversation regarding a subject unrelated to the resident whom the caregivers are taking care of, the resident is positioned as an overhearer (Goffman, 1981), and even more as an object (of care). The parallel conversation shapes a new participation framework in which Emma’s participatory role changes from an active participant into to an object that is being manipulated during the time the caregivers are engaged in their own conversation—as if she is just something to be handled or operated on as part of a routine task or activity. This change in the participation framework, however, does not last long (see Deppermann, 2014 for quick transitions between different tasks in cooccurring joint projects). Having made the walker ready for Emma to hold on to, Paulina prepares for the next phase of the move, which is the sit-to-stand transfer; Emma, once again, becomes the center of the interactional focus.
Extract 1b: Transferring the resident to the bed
Participants: Emma (person with dementia), Paulina (Staff member), Sofia (Staff member)
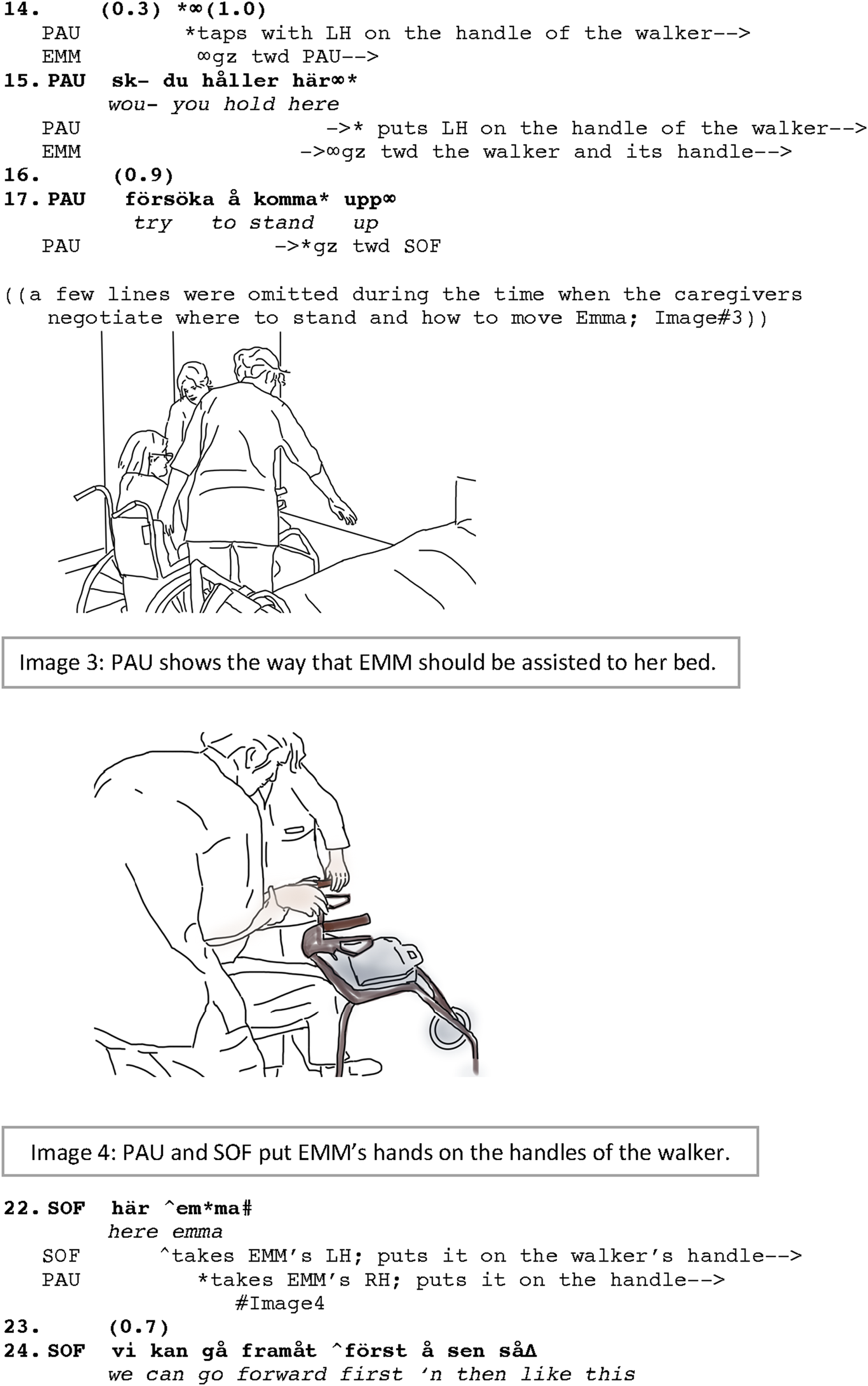
The phase of the transfer proper, which includes a sit-to-stand, followed by a short walk and a stand-to-lie, is not possible without the coordination of the caregivers and also communicating with the resident as how the move is going to be made. Although it would also be plausible to go through the assistance to move without directly addressing the resident, in our data, as much as the resident is able to move her own body (or part of it), the caregivers encourage the resident to take some responsibilities in the process. This helps with less weight-bearing for the caregivers and is also a preferred strategy in nursing to help the residents to use their own abilities as long as they can. To include the resident in the process of manual transfer has some interactional consequences as well. By addressing Emma during this part of the transfer, the caregivers attend to her as an agent with both will and ability (although without equal footing). This is evident in lines 14 and 15 when Paulina taps on the handle of the walker and gives Emma a directive to hold the handlebar and visibly shows the handle although Emma could not possibly fulfill the request on her own. It is worth noticing that tapping on the walker’s handle, which even comes before the directive is produced, is observed by Emma. As soon as Paulina moves her hand toward the handle to tap on it, the move is immediately attended to by Emma when she turns her gaze toward Paulina (line 14) (cf. the occurrence of the bodily coordination before issuing verbal directives in Mondada, 2018). After giving the directive (line 15), Paulina also provides an account of why she asks Emma to hold the handle as she explains that Emma needs to “try to stand up” (line 17).
The transfer of the resident also requires coordination among the caregivers themselves. This happens immediately after the introductory directives given to Emma (not shown in the transcript between lines 18 and 21). The significant part of the negotiation is about who to stand on the left or right side of Emma to help her stand and which path to take to bed. Meanwhile, the caregivers coordinate their moves. Emma is sitting still but following, with her gaze, the caregivers who are changing their positions and moving to her sides. As shown in IMG.#3, Paulina is standing on the right side of Emma and Sofia on the left. Paulina shows the way they should take to transfer Emma to her bed. Sofia and Paulina then (line 22) put the left and right hands of Emma on the handlebar of the walker (IMG.#04). As Emma also holds the walker’s handle (line 24), Paulina and Sofia hold each of Emma’s arms with one hand, and with the other, they hold the waistband of Emma’s pants on her back (lines 22–25). While they steadily hold the resident, they also talk to her (lines 25 and 26). Although the resident cannot verbally respond back or is essentially silently following the procedure, her being addressed during the transfer involves her in the participation framework as an active participant. Emma’s embodied response by following the directives and joining the lifting to stand up is indicative of her being active in the process of transfer.
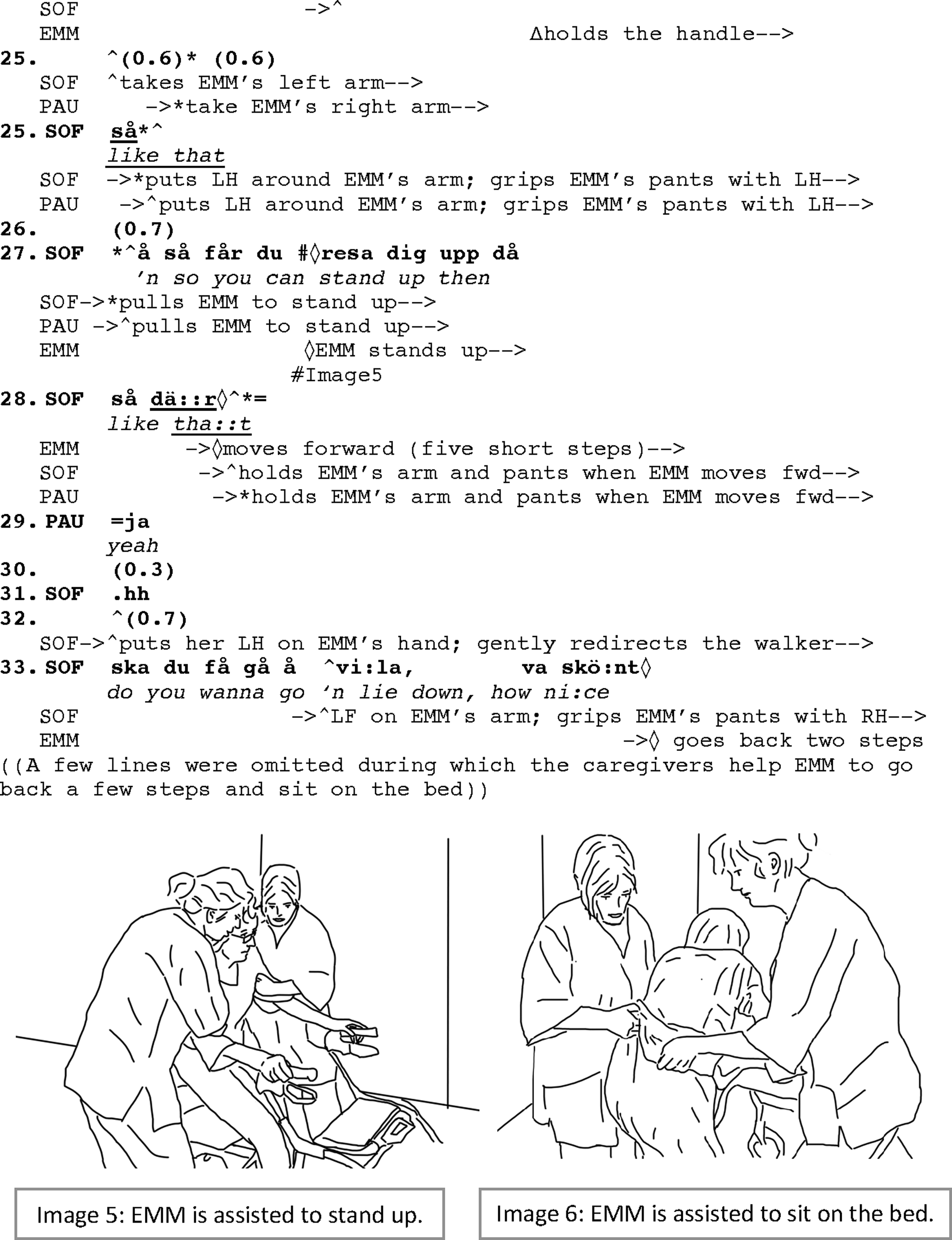
The sequence continues by the caregivers gently pulling Emma up on her feet while Sofia tells Emma what she is going to do: “so you can stand up then” (line 27). This results in Emma standing up (IMG.#5) which is also completed and signaled by the expression “så
Giving directives to Emma despite her inability to perform the requests by herself (lines 15, 17, 24, 27), directly addressing her (line 22), and announcing to Emma the upcoming event with a positive assessment, which also provides a post-hoc account for the whole transfer process (line 33), all demonstrate how the activity is designed to position Emma as a co-participant in the activity, bearing part of the responsibilities in accomplishing the task. It is Emma who should “hold,” “try,” “walk,” and “stand up,” even though, as shown in the transcript, these actions are performed with great support from Paulina and Sofia in coordination (see also Mondada, 2018: 99, on the priority of the organization of embodied coordination before verbal directives). Emma’s hands are placed on the handles (IMG.#4), she is raised to an upright position by Paulina and Sofia holding her by her arms and lifting her (IMG.#5), and she is also assisted to walk. Through Paulina’s and Sofia’s careful manipulating Emma’s body and their addressing her, Emma is not treated only as an object of care but also as a lived body to work with, and she is thus partner-positioned throughout the activity.
Extract 1c: Laying and adjusting the resident on the bed
Participants: Emma (person with dementia), Paulina (Staff member), Sofia (Staff member)
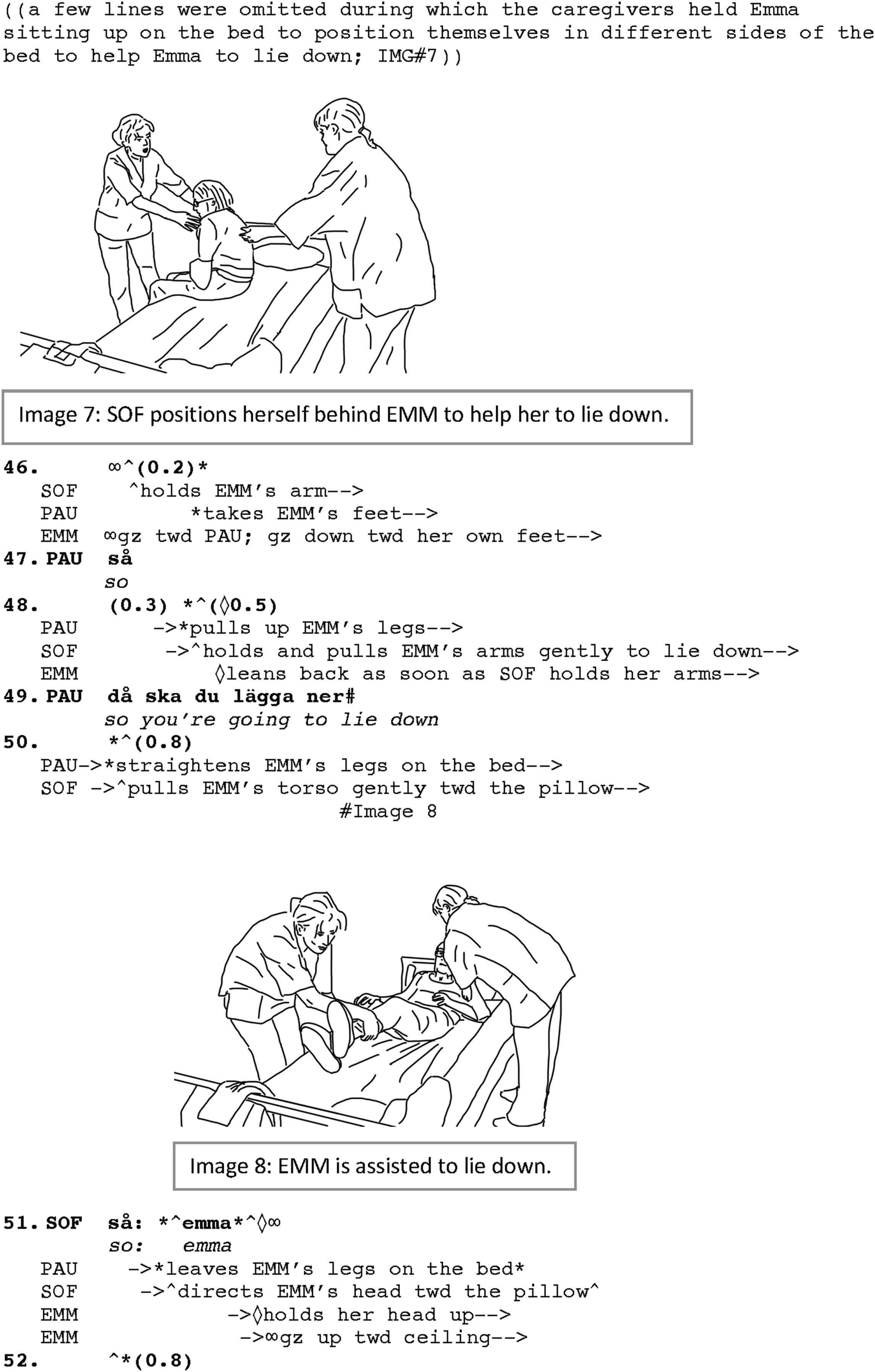
With Emma sitting on the bed now, Paulina carefully holds her until Sofia moves to the other side of the bed so that they can arrange holding Emma from both the front and back of her body to lay her down. Sofia leans forward to hold the neck and the back of Emma; Paulina moves down along the bed to hold Emma’s feet and legs. From the time that the caregivers are in their positions, it takes less than a couple of seconds to lay down Emma on the bed. From her sitting position, almost a 90° rotation is needed to turn Emma’s body in a right direction to lie down. Emma’s body is therefore rotated toward her left, so her head could be laid down on the pillow. The end of the rotation is signaled by “so” (line 47) which is also a sign to start helping Emma to lay down on the bed (see research on “so” as a discourse marker showing the boundaries of the activities, for example, in Thelander et al., 2005; cf. Bolden, 2008 for “so” in launching new activities; see also Raymond, 2004). As soon as the rotation is ended, Sofia holds Emma’s arms, Emma leans back and lets her body be laid down (line 48). This is immediately followed by pulling Emma’s legs up and moving them toward the footboard. This is also commented on by Paulina, addressed to Emma: “so you’re going to lie down” (line 49; IMG.#8), while she also begins to straighten Emma’s legs (line 50). The end of this part of the transfer is announced by using the discourse marker “so” and calling Emma’s name: “so emma,” marking that Emma is now in a resting position on the bed (line 51). Emma, who has now been following the move by looking at Paulina holding and lifting her feet (see lines 46–51), upon getting into a lying position, however, holds her head uplifted (line 51) until the pillow is adjusted under her head (line 55). By holding her head uplifted, Emma displays (a) her knowledge, understanding and thus her orientation toward the routine activity of the transfer; that is, she will wait until the pillow is made ready for her to put her head on. She also demonstrates (b) her own initiative to make the next action possible. This is a demonstration of Emma’s agentive role in interaction which is also recognized and responded to by Sofia when she readjusts and fluffs up the pillow for Emma (line 55).
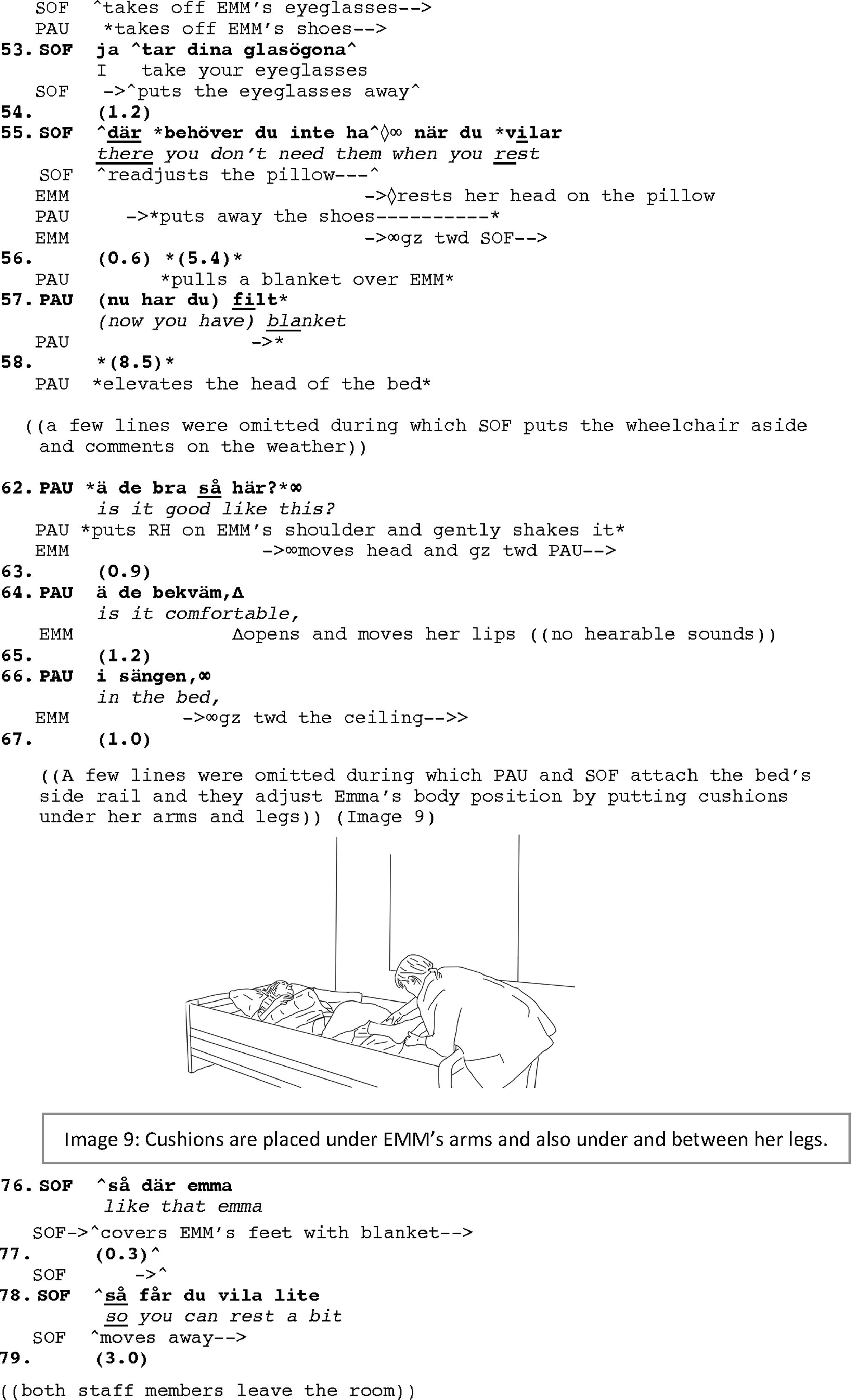
While Emma is still holding her head uplifted (around 5 s), Paulina takes off her shoes and Sofia her glasses (line 52), meanwhile, also, explaining what she does (line 53). She immediately readjusts the pillow under the still uplifted head of Emma, as she provides an account for taking off Emma’s glasses (line 55): “
Receiving no display of discomfort in Emma’s face, Paulina and Sofia continue the rest of the care work by securing Emma’s position on the bed. They attach back and secure the siderail of the bed which was detached from the bed during the transfer. Their work of transfer and assisting the resident to lie on the bed finishes with some measures to help Emma become more comfortable. They put cushions under Emma’s arms, and under and between her legs (IMG.#9). The sequence ends with addressing Emma again while also signaling the end of the transfer and leaving Emma to rest: “like that emma” (line 76), “
Addressing Emma during the activity, for instance, in the beginning of laying Emma on bed (e.g., line 49) and when adjusting her body in bed, taking off her eyeglasses (lines 52–53), when raising the head section of the bed (lines 58–66) and also when putting cushions to support her arms and legs (lines 76–78), all the talk and the way that Emma’s body is treated gently and with care, contribute to (re)subjectifying Emma and foreground her as a person rather than an object of care, and her body as a lived body and not just a material body that needs to be moved and positioned in bed. Therefore, the whole sequence shows how the care task is turned into a joint activity involving the person with late-stage dementia partner-positioned as an addressed participant in the activity.
The next example deals with moving Soraya to bed. Similar to Extract 1 (a, b, c), we have divided the whole activity into three phases of preparation, transfer proper, and laying and adjusting the body. In this example, because of the severe challenges that Soraya has, the caregivers use a lifting machine for the transfer. Apart from some short exchanges of talk between the caregivers and also with Soraya, the activity is managed through embodied interaction. Therefore, we present the activity with more drawing images illustrating the care work as it temporally unfolds.
Extract 2a: Placing and preparing the resident for transfer
Participants: Soraya (SOR, person with dementia), Boonsri (BOO, staff member), Edina (EDI, staff member)
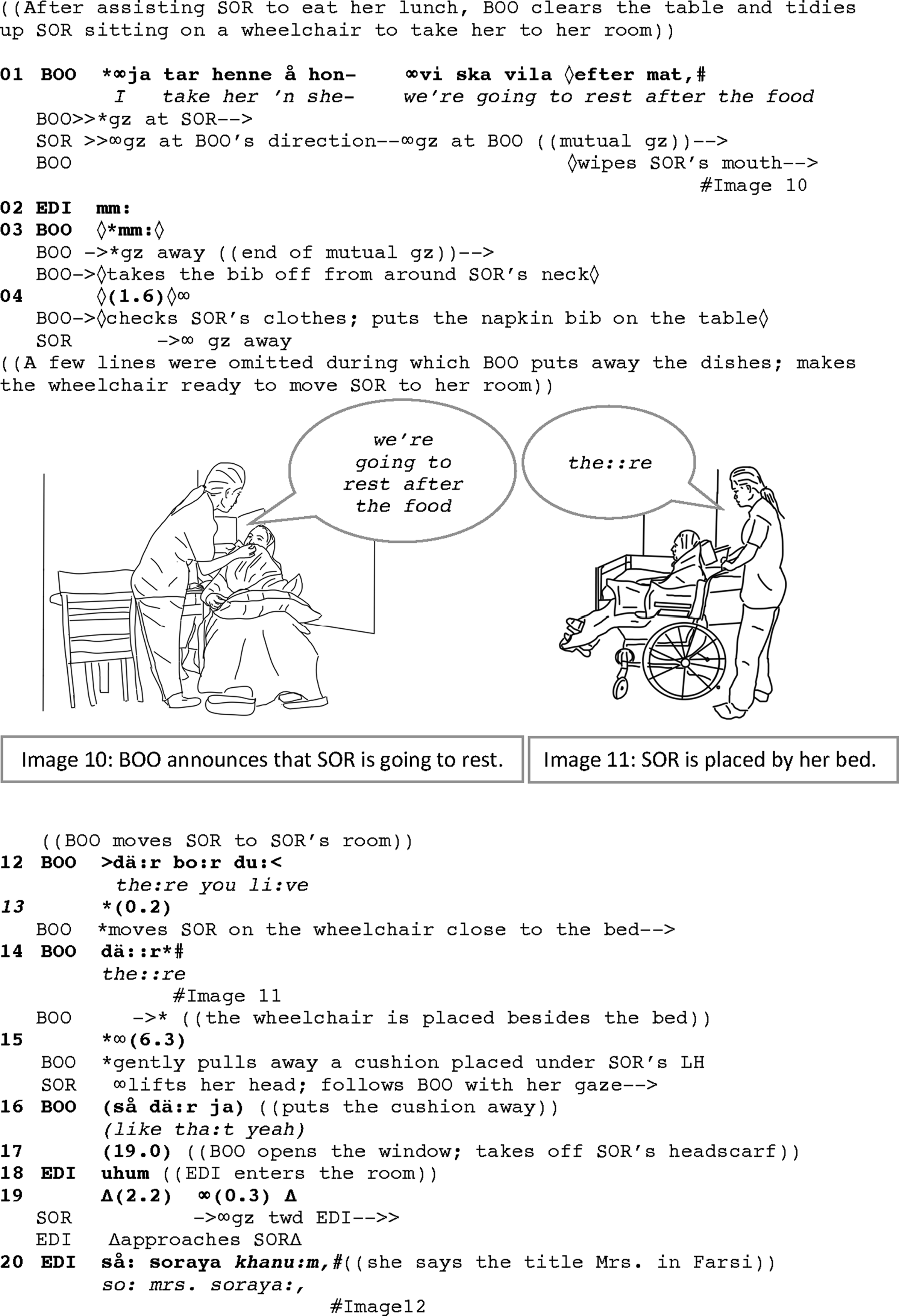
The preparation sequence starts right after finishing the meal when Boonsri, the caregiver who assisted Soraya with her lunch, takes her in a wheelchair back to her room to rest. The first thing Boonsri does before moving Soraya to her room is loudly announcing what she is about to do. In her announcement, Soraya is addressed in a third person showing that the turn is aimed for Boonsri’s colleague who is present in the room (line 01). In the middle of her turn, however, when Soraya directs her gaze toward Boonsri, she restarts the turn: “I take her ‘n she-we’re going to rest after the food” (line 1). Boonsri changes the position of Soraya in her syntax from a third person to a first person, when she restarts and directly includes Soraya in the construct of the subject in her talk. By using “we,” she not only changes the position of Soraya from being a topic of her talk to a subjective agent, but also turns the activity into a joint one as she changes the subject to a first person plural (cf. Nilsson et al., 2018). This also occurs at a moment when the participants have a mutual gaze (IMG.#10). The shift of gaze direction initiated by the resident is responded to by the caregiver through including the resident as a direct addressee in the participation framework. The duration of the mutual gaze starts from the time that Boonsri leans over Soraya to wipe her mouth (line 01), and finishes when she takes off Soraya’s napkin bib (line 03).
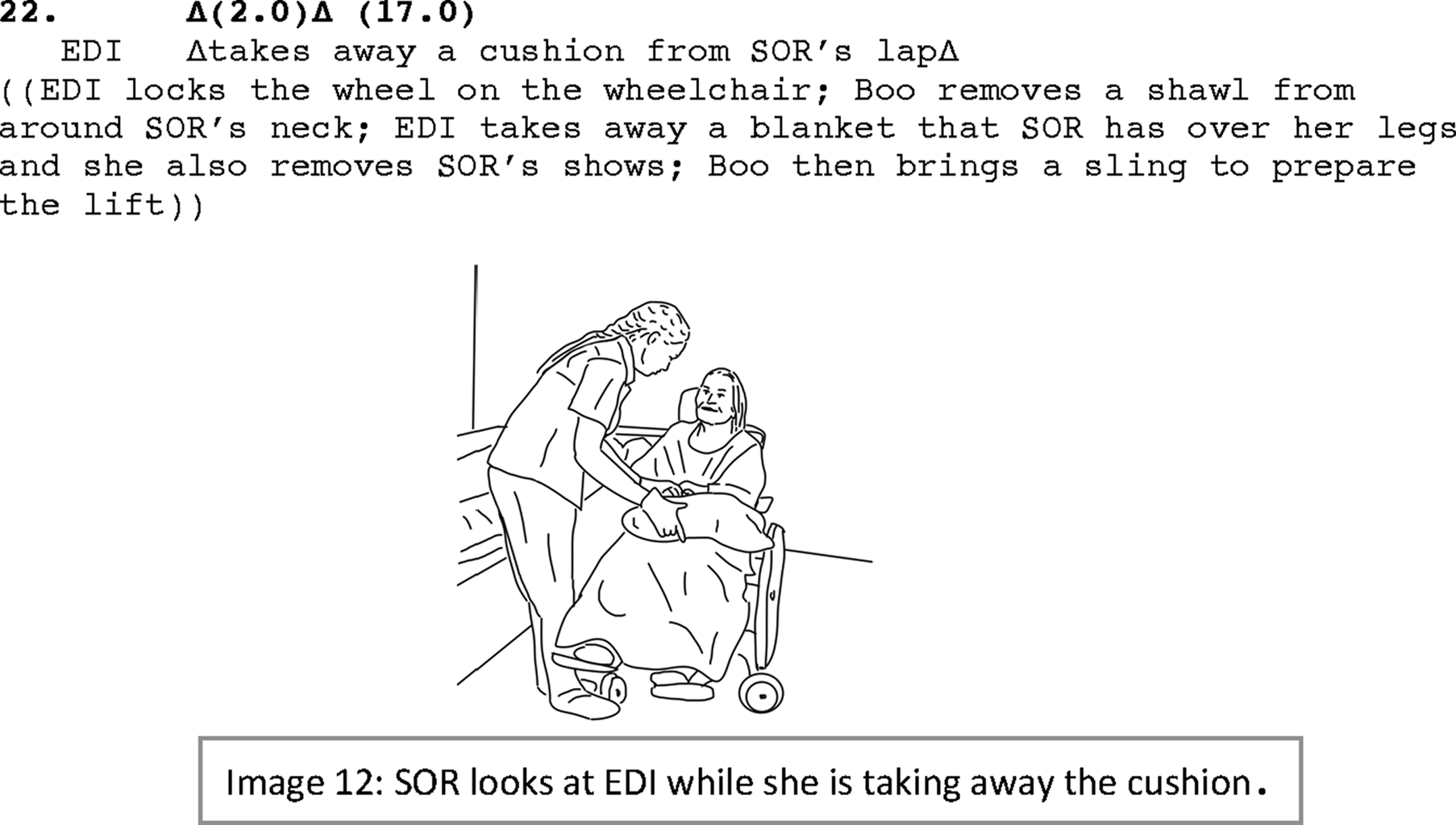
Boonsri, then, checks Soraya’s clothes (perhaps in case she needs to wipe off any dropped food on her clothes), puts away the napkin bib (line 04) and gets to the task of moving Soraya to her room to prepare her for the transfer into bed. While moving toward Soraya’s room, she continues talking directly to Soraya (e.g., lines 12–16). After entering the room, like in Ex.#01a, the wheelchair is placed by the bed (IMG.#11). Preparing Soraya for the transfer requires some of the routine moves (see Phase 1 in Ex.#1a): the path for the move should be cleared off obstacles, the resident should not have extra outerwear, the wheelchair should be secured, etc. Boonsri therefore begins with removing the cushions that Soraya usually has under her arms when she sits on the wheelchair (due to her kyphosis, the cushion is used to keep her back straight) (line 16). She also removes Soraya’s headscarf (line 17). All Boonsri does is closely watching Soraya who actively follows Boonsri with her gaze (lines 15–19). At this point, Edina enters the room to help out. She gets straight into the work and joins Boonsri in the transfer activity without receiving any directives (Boonsri is senior to Edina at work), something that shows the caregivers follow a routine at this stage. She immediately helps with removing the cushion from Soraya’s lap. As she approaches Soraya, Soraya shifts her gaze toward her, and when Edina enters into a face-to-face position with Soraya (without engaging in mutual gaze with Soraya), she uses an address term in Farsi which is Soraya’s mother tongue: “så soraya khanum” (“so mrs. soraya,” line 21; IMG.#12). Edina knows only a few words in Farsi. So, the address term in this example (like in Ex.#01, line 1) is not used for initiating talk in Farsi (Soraya is also unable to produce spoken language) nor does it seem to be used for the purpose of addressing per se, for example, to gain attention, but perhaps for directly acknowledging Soraya’s presence in the participation framework of the activity (cf. Clayman, 2012), and also signaling some affiliative move and showing affect for the resident. With no response taken (or expected to be received due to Soraya’s loss of spoken language), the preparation phase is completed by securing the wheelchair, removing Soraya’s shoes, and bringing the sling to prepare for the lift (line 22).
Extract 2b: Transferring the resident to the bed
Participants: Soraya (SOR, person with dementia), Boonsri (BOO, staff member), Edina (EDI, staff member)
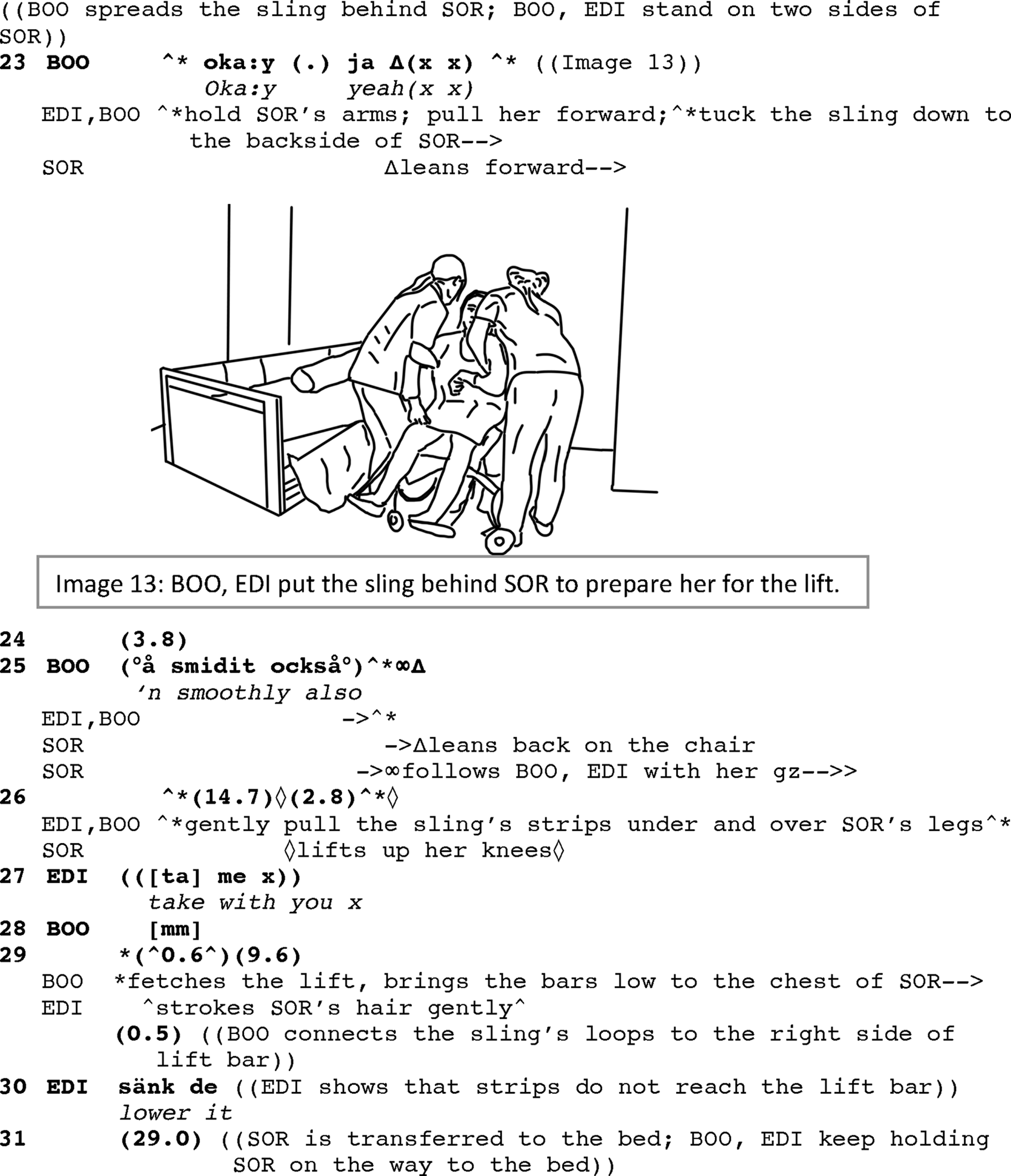
With an exchange of a few words, the caregivers coordinate to secure Soraya’s body in the sling that will be used for the lift and transfer. They start by standing on each side of Soraya, holding her arms and gently pulling her forward to slide the sling behind and under Soraya’s body (line 23; IMG.#13). The gentle pull of the body is a bodily indication of the expected move, an embodied directive that is also performed jointly with the assistance of the caregivers (line 23). The beginning of the action to alter Soraya’s body position is coordinated with the discourse marker “OK,” which similar to “so,” may show the boundary of an activity (see Ex.#1c). Even the connector “and” (e.g., its short form “‘n” in line 25) is used for a similar purpose to show the end of the activity and beginning of coordinating to help Soraya lean back in the wheelchair. The coordination is managed vis-á-vis the body that they are handling. How the caregivers manipulate the care-recipient’s body is evidence to their consideration of the care-recipient as a lived body and not just an objective body even if the main task is to treat the body as object to move. The caregivers gently pull Soraya forward (line 23), smoothly help her to lean back (line 25), and again gently pull the strings of the sling under and over Soraya’s legs (line 26). They finally attach the strips’ loops to the lift bar (lines 29–30). With a bit of coordination to lower the lift and securing the connection of the lift and the sling (line 31), they start the move. Soraya is monitoring the activity all the time (line 25 and onward). The lift and the transfer take place in approximately 30 s during which the caregivers keep holding Soraya on the way to the bed for ensuring the safety of the move (line 31).
Extract 2c: Laying and adjusting the body of the resident on the bed
Participants: Soraya (SOR, person with dementia), Boonsri (BOO, staff member), Edina (EDI, staff member)
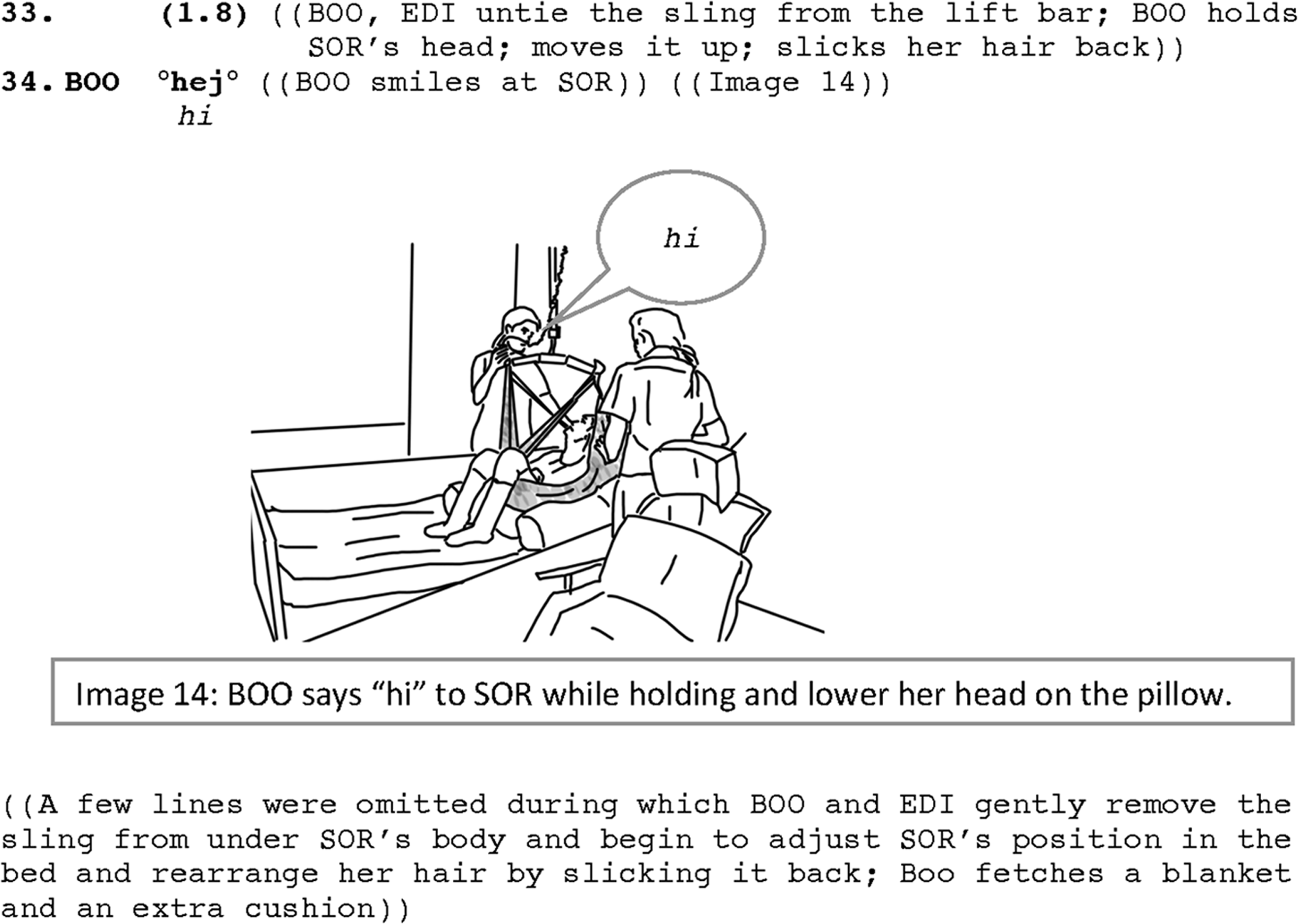
When Soraya is transferred to the bed, the caregivers first untie the lift bar, and then remove the sling. While doing this (line 33), as Soraya is unable to hold her head up, Boonsri tends to Soraya’s head, holding it up, and when it is left on the pillow, she slicks her hair back. When touching her head, Soraya turns her gaze toward Boonsri and at that time, Boonsri not only is in bodily contact with Soraya but she also smiles and verbally communicates with her by saying “hi” (line 34; IMG.#14). Saying “hi” is timely produced when the lift bar is untied and the sling from under Soraya is removed. Closely attending to Soraya through slicking her hair back and saying “hi” to her seems to mark the end of carrying Soraya and displays also an attempt to reconnect to Soraya as a participant in the activity, turning the activity of transfer into an interactional activity. In other words, having eye contact with the resident, tending gently to her body (to her head position and her knees), together with verbally communicating with her (saying “hi”), interactionally positions her as a co-participant in the activity. These practices do not allow Soraya’s situated identity to remain to be an objective body to transfer but to shift an objective treatment of the body into a subjective treatment of the resident. Soraya is therefore partner-positioned as an addressed participant in interaction, rather than just an object of care in a care task.
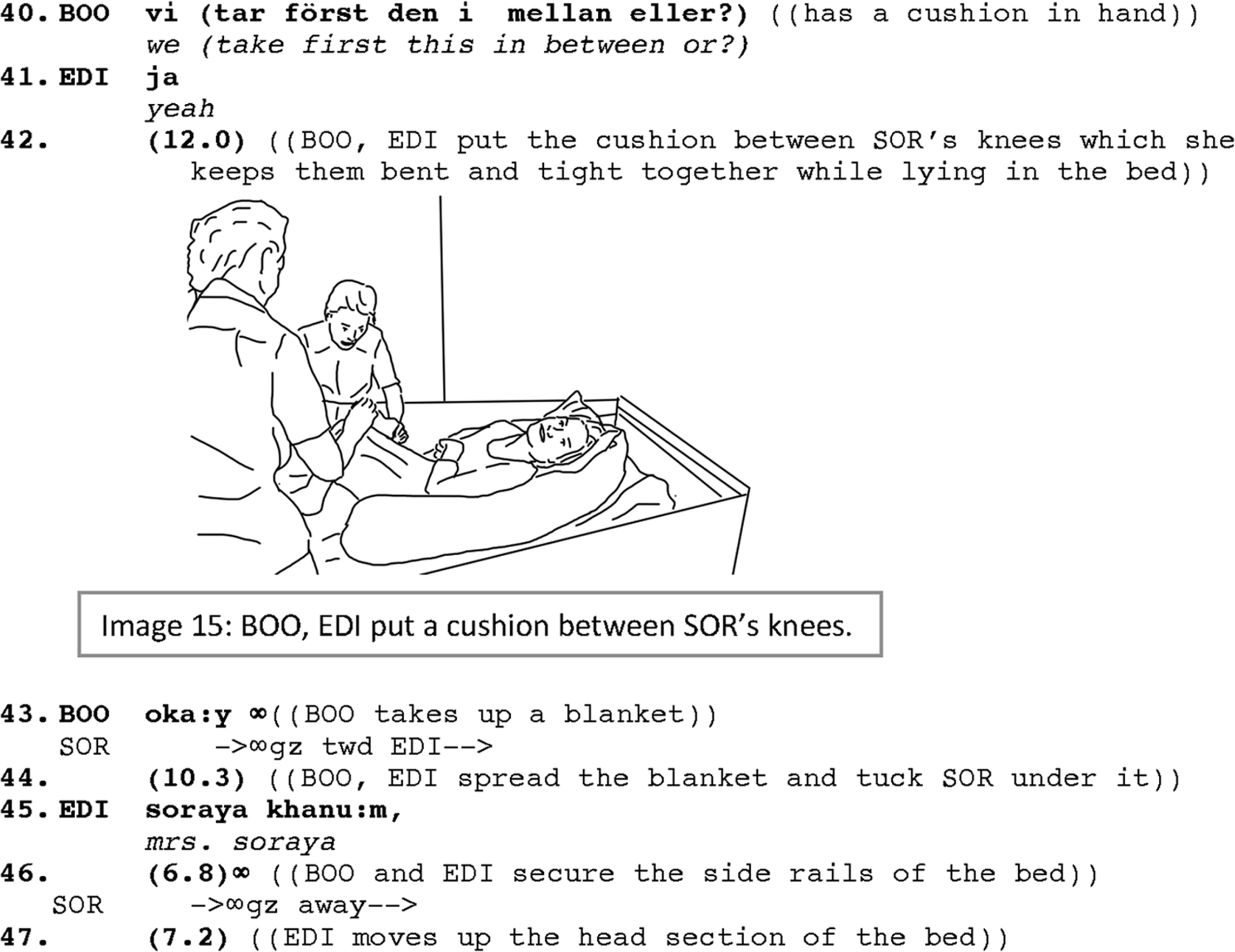
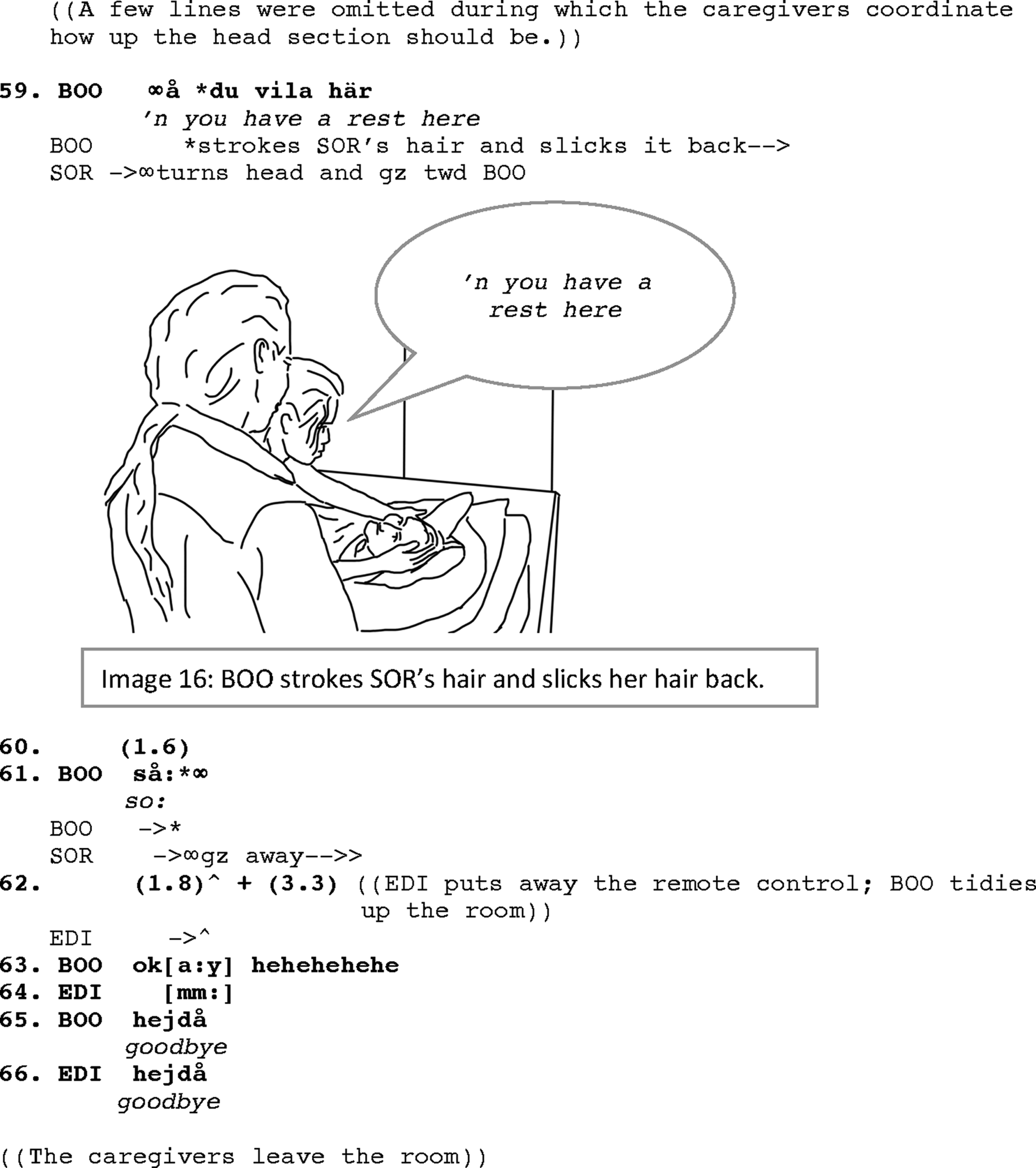
The caregivers now adjust Soraya’s body on the bed by putting a cushion between her knees as Soraya usually keeps her knees tight together (lines 40–42; IMG.#15). After finishing putting the cushion between her knees, as Boonsri fetches a blanket to cover Soraya, Soraya shifts her gaze toward Edina. This gaze shift, even if not immediately, is also followed by Edina addressing Soraya directly again in Farsi (line 45; like in Ex.#2a). The addressing is not pursued by Edina to receive any response and seems to be produced for its affiliative purposes, that is, showing social engagement with Soraya and acknowledging her presence at the moment. The caregivers, meanwhile, continue tucking Soraya under the blanket, and securing her bed by putting back the siderail (line 46). Then, they raise the head section of the bed and exchange a few turns about how much the head section should be raised (not shown in the transcript). When they are done with adjusting the body and the bed, Boonsri, while stroking Soraya’s hair and slicking it back, directly addresses her: “‘n you have a rest here” (line 59; IMG.#16). She finishes her turn addressing Soraya with “so” signaling that they are done with the last phase of the transfer (line 61). Saying “so” while withdrawing the hand from engaging with Soraya is immediately followed by Soraya directing her gaze away (line 61). This co-occurrence could be marking a mutual understanding of disengagement. Edina puts away the remote control of the bed, and they tidy up the room before saying good bye to Soraya (lines 65 and 66) and leaving the room.
Concluding discussion
People with late-stage dementia, due to the advancement of the disease, may gradually be faced with decremented cognitive and communicative as well as physical abilities. Therefore, they constantly require assistance for personal activities of daily living such as eating, walking, changing clothes, managing their personal hygiene, etc. With their diminished social relations, and inability to participate in social activities on their own, they are at risk of getting in what is known as “malignant position” (Sabat, 2001). This requires some effort to work against in their social life and particularly in caregiving situations where there is also a higher risk of treating the people as only objects of care and not participants in care tasks. Therefore, care workers, particularly in care homes, when tending to the person with late-stage dementia, face a practical challenge. On the one hand, they have a care task to attend to, and on the other hand, they should organize the care activity according to the guidelines for patient-centered care that emphasize respecting the individuals’ agency in the care task (Institution of Medicine, 2001; There are also studies that show the significance of patient-participation, see, for example, Lehtimaja and Kurhila, 2022). As a case in point, in this study we have shown how caregivers tackle this challenge, when transferring persons with late-stage dementia to bed, through turning the activity of transfer into a joint activity, engaging with the person with dementia through verbal and nonverbal means. Through such an engagement, caregivers acknowledge the person with dementia as part of the joint activity, lifting the interactive nature of collaboration in the care activity, and thus recognize the agentive role of the person with dementia as an interactional partner, something that we call “partner-positioning,” a social action for inclusion, that works against the impacts of “malignant positioning.”
As our study shows, turning the care activity into a joint one means that the accomplishment of the activity will not be possible without the cooperation of the participants to sustain the focus of attention and coordination for the progressivity of the activity (through addressing each other, making joint actions, etc., see “focused interaction” in Goffman, 1963). In case of asymmetrical relations between the caregivers and the resident, the resident with late-stage dementia would obviously not be expected for equal coordination at the same level with the caregivers. However, as we showed in our analysis, the care-recipient, during the activity, is constantly treated as a party in the activity’s embodied participation framework (Goodwin, 2018). The caregivers orient to the fact that even with the minimal contribution to the activity (by virtue of their presence, their gaze directions, etc.), although they cannot talk, the resident is still acknowledged as the receiver of care, and a main participant in interaction.
In all three phases of transfer activity that we studied here (preparation, transfer proper, and laying and adjusting the body on the bed), we have observed a ubiquitous practice of verbal and intercorporeal engagement in interaction with people with late-stage dementia which position them as collaborative partners. The caregivers not only verbally and bodily are in close contact with the care-recipients, but they also closely attend to the care-recipients’ minimal contributions to interactions, for example, through their head movements and gaze directions. These interactional efforts from both sides help the participatory status of the person with late-stage dementia to be recognized, their recipiency in interaction gets heightened (e.g., through being directly addressed) and their agentive role is acknowledged. Much of this interactional effort is done through showing affiliation through talk and other embodied resources such as touching, stroking, etc.
In sum, this study shows how professional care workers live up to the principles of care stipulated for patient-centered care (see, e.g., the Institution of Medicine, 2001), by which care practices are expected to be performed in collaboration with the care-recipient based on mutual understanding, and with respect to the individuals’ agency as well as their right to privacy and intimacy. In the context of caregiving for people with late-stage dementia, we have shown how professional care workers use interactional practices so as, on the one hand, to conduct their care tasks according to their daily schedule, and on the other hand, to orient to the social aspects in the interactive work of caregiving to maintain the individuals’ integrity. They do so by engaging in collaborative interaction with people with late-stage dementia: they organize the care activities in a way that the person with late-stage dementia and their body is not just handled as an objective body but rather interactionally treated as a lived body. Therefore, the person with late-stage dementia is (re)subjectified as a partner in interaction rather than just an object of care.
Footnotes
Acknowledgments
This study could not be conducted without the collaboration and participation of the staff members in the residential care we studied over a year. The study is indebted and dedicated to the people with dementia and their relatives who allowed us to study their activities during our fieldwork. We are also grateful to our colleagues in the Center for Dementia Research (CEDER) at Linköping University for their comments on the earlier version of this article. We would also like to extend our sincere gratitude to the editors of this special issue and also to two anonymous reviewers for their constructive comments and valuable remarks.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Forskningsrådet om Hälsa, Arbetsliv och Välfärd (2016–07207).
Appendix
.hh
In-breath
hh. or heh, hihi
Out-breath or laughter
°°
Quieter than surrounding speech
Capital letters
Louder than surrounding speech
< >
Slower than surrounding speech
> <
Faster than surrounding speech
( ) or (x x)
Unheard or unclear utterance
[ ]
Overlapping speech
(.), (0.2), (1.0)
Pause in seconds
(( ))
Transcriber’s comments or descriptions
@ @
Smiley voice or face
=
No discernible silence between utterance
:
Prolonged speech
?
Intonation rise-to-high
,
Intonation rise-to-mid
;
Intonation fall-to-mid
.
Intonation fall-to-low
lines in italic
Nonverbal action
lines in gray
In original language (Swedish or Persian/Farsi)
* * or ^ ^
Delimit descriptions of one speaker’s actions
#
Exact place of an illustration in the stream of the talk
*-->
Action described continues across subsequent lines
-->*
Action described continues until the same symbol is reached
>>--
Action described begins before the beginning of the excerpt
-->>
Action described continues even after the excerpt ends
…..
Action’s preparation
,,,,,
Action’s retraction.