
Abstract
There is a growing recognition of the importance of the social work contribution within community mental health services. However, although many texts describe what the mental health social work contribution should be, little empirical evidence exists about their role in practice and the difference it might make to service users. This qualitative study sought to articulate this contribution through the voices of social workers and their multidisciplinary colleagues via focus group discussions across four English Mental Health Trusts. These considered the impact of the social worker on the service user. Thematic analysis resulted in the identification of three over-arching themes: social workers own perceptions of their contribution situated within the social model; the high value their colleagues placed on social work support and leadership in a range of situations and the concerns for service users if social workers were withdrawn from teams. Key findings were that social workers are the only professional group to lead on the social model; that this model enhances the whole teams’ practice and is required if service users are to be offered support that promotes long-term recovery and that without social workers, the community mental health team offer would be more transactional, less timely, with the potential for the loss of the service users’ voice. If social work is to make a full contribution to community mental health team practice, it must be clearly understood and provided with the support to enable social workers to operate to their full potential.
Introduction
Social work has long been regarded as a core component of mental health support internationally. In England, social workers have routinely been members of community mental health teams (CMHTs) since the 1990s (Onyett, 2003) and recognised as one of a core group of professions working in multidisciplinary teams alongside medics, nurses, occupational therapists, psychologists and support workers (Huxley et al., 2011). Their role and contribution to these teams, however, is often described as unclear (Woodbridge-Dodd, 2018) and their potential as ‘underdeveloped’ (Allen, 2014: 5). Reasons given for this include the complexity of the social work role, the dominance of the medical model within mental health (Gould, 2010) and the rise of generic roles within CMHTs, where professionals from a variety of backgrounds share a range of non-specialist tasks (Bailey and Liyanage, 2012) and, in England, the increasing statutory obligations of the profession (The College of Social Work, 2014). Additionally, the limited evidence of the effectiveness of integrated CMHT practice has potentially undermined the social work contribution as their membership has been regarded as a hallmark of an integrated team (Huxley et al., 2011; Wilberforce et al., 2011).
Social work is a complex profession, underpinned by specific values, skills and knowledge, including the social model of disability; communication expertise and command of legislation. In the mental health context, it seeks to promote long-term recovery: the rebuilding of a ‘worthwhile life’ for service users through gaining control, being connected socially, having valued social roles and positive self-identity (Tew et al., 2012: 444). Definitions of social work are also complex as well as ‘contested and evolving’ (Moriarty et al., 2015: 3). This can make it difficult for those outside the profession to understand what social workers do or how they add to an individual’s care (Larkin and Callaghan, 2005; Woodbridge-Dodd, 2018). Some evidence suggests that even social workers find their role challenging to explain (Morriss, 2017; Roysum, 2017). In a description of findings from interviews with social workers seconded to CMHTs, Morriss (2017) reported that participants struggled to positively articulate their role, describing it as ‘operating in the gaps left by other professions’ (1348). Others have suggested that social workers believe that how they undertake their role is more important than what they do (Roysum, 2017). Social workers within CMHTs have been found to undertake a range of roles and tasks including assessment and care coordination, therapeutic interventions, support to access a wide range of services, the management of complex multi-agency meetings and provision of support under the auspices of mental health legislation.
In 2014, The College of Social Work, set up to represent, strengthen and support the profession, and operational between 2012 and 2015, published five key areas of practice for social work in adult mental health. These are: enabling people to access advice and support to which they are entitled; promoting a personalised social care ethos and discharging statutory duties; promoting recovery and social inclusion; providing professional leadership and skill in complex, risky and ambiguous situations; supporting individuals and communities around resilience and active citizenship and leading the Approved Mental Health Professional (AMHP) workforce, additionally qualified social workers and other professionals who undertake a range of roles authorised by mental health legislation. The document also noted the importance of local government (typically social workers employers), health trusts (where mental health social workers are often based within multidisciplinary teams) and service commissioners, in promoting the crucial role of social workers in the mental health sector, stressing that such recognition cannot be taken for granted (Allen, 2014).
This is in part due to the dominance of the medical or biomedical model in mental health practice which remains a challenge for social workers, schooled in the values of social models (Wilson and Kirwan, 2007). Whilst the 1970s and early 1980s saw the rise of the biopsychosocial model in psychiatry, it has been argued that a ‘bio-reductionist orthodoxy’ has since re-emerged (Gould, 2010: 17). Nevertheless, more recently, a growing recognition of the importance of the social determinants of mental health has been seen both in England and elsewhere (e.g. Royal College of Psychiatry, 2014; World Health Organisation and Calouste Gulbenkian Foundation, 2014) with recommendations in England for the social model to be implemented more widely (All Party Parliamentary Group on Social Work (APPG), 2016). Whether this represents renewed support for social workers as core CMHT members is less clear. Some evidence exists to support this aim, in particular demonstrating that where social workers are present within CMHTs, the quality of care is improved (Abendstern et al., 2014; Huxley et al., 2011; Wilberforce et al., 2016). However, evidence remains limited (Moriarty and Manthorpe, 2016) with voices from within the profession expressing concern that an evidence base is required to demonstrate the relevance of social factors and social interventions to mental health recovery (Tew et al., 2012; Woodbridge-Dodd, 2018).
A complicating factor in evaluating the role of social workers in integrated CMHTs has been the rise of generic roles within these teams in England (Brown et al., 2000) which may have attenuated the social worker role (Rapaport, 2005) and increased its susceptibility to being undermined as a specialism (Bailey and Liyanage, 2012). Policy reforms that challenged traditional ways of working in CMHTs largely ignored the social work contribution (Department of Health (DH), 2007). More recent reports, however, have noted that social workers were often used generically, their skills wasted, to the detriment of service users (e.g. Lilo and Vose, 2016). Whilst some evidence suggested that professionals were more concerned to do what needed to be done rather than stick to their professional role (Hannigan and Allen, 2011), genericism was usually reported to result in professional entrenchment rather than the desired outcome of a boundary-spanning workforce (Oliver, 2013). Their perceived misuse as generalists rather than specialists in CMHTs has led to role conflict among social workers (Carpenter et al., 2003) and, in England, to their local government employers questioning their position as CMHT members. Anecdotal evidence of social workers being removed from CMHTs in England to relocate within local government Social Service Departments is growing (Gilburt et al., 2014; Moriarty et al., 2015).
It is within this context of limited role clarity and value that the current study is located. The aim of this paper is to identify and explicate the contribution of social workers to CMHTs and their perceived impact on service users.
Method
This qualitative paper forms part of a larger-mixed methods study that aimed to identify the social work contribution to CMHTs drawing on the characteristics, opinions and experiences of managers, practitioners and service users (Boland et al., 2019; Wilberforce et al., 2019). The views of social workers and their team colleagues were collected via focus groups and analysed using Braun and Clarke’s organic thematic analysis method (2016). The study was supported by a Lay Reference Group of seven people who were either carers of people with mental health difficulties or were mental health service users themselves. The group met regularly throughout the study and assisted in the conduct of the research, the interpretation of the findings and their presentation. They played a key role in the orientation of the focus group discussions to incorporate a service user perspective. Participants took part in a sense-making exercise where initial findings were presented in terms of key issues raised by groups. Participants were asked to consider whether findings resonated with their experiences. The outcome of this process was used by the research team in further analysis to refine and construct the final themes.
Sample
Participants were drawn from four NHS Trusts in England. Two served inner city populations and two described themselves as serving a mixture of urban and rural communities. At the time of data collection, one trust included age inclusive teams for people with functional ill health. In three Trusts, social workers were team members, and in the fourth, social workers had been removed within the previous year into separate social care pathway teams. Participants were contacted and invited to take part via their Trust’s Research and Development team. All team members, including support workers, were eligible. Whilst the presence of managers might have inhibited more junior staff, we did not exclude the possibility of team manager involvement, as the issue under discussion did not relate directly to management issues. Team managers were consequently regarded as experienced practitioners of relevant professions. Prospective participants were sent an information sheet, and informed consent was obtained in writing from individuals prior to each focus group.
Data collection
To move beyond a discussion of what social workers do and to elicit from participants the perceived effect on service users of their presence or absence, they were asked to consider the impact of social workers on service users and any potential loss to teams if they were no longer included. The question posed to each group was therefore: What would be lost to service users if social workers were not team members? The broad scope of this question lent itself to the focus group method, recommended where a group process can ‘illuminate’ a research issue and where members can work together to consider the topic and share their views (Lewis and Nicholls, 2014: 56). A strength of this method is that, in contrast with individual interviews, interaction between group members can generate a richer data set with individuals responding to and building on themes initiated by each other (Finch et al., 2014). Conversations are not rehearsed, and although their occurrence is constructed, interaction is naturalistic, as in everyday conversation where people are influenced by those who they are talking to (Krueger and Casey, 2009). Interactions within groups can also be challenging, for example, when faced with dominant voices and inter-group conflicts or due to the tendency towards normative arguments. It is important that facilitators are alert to these issues and able to manage them constructively within the data collection and during analysis processes (Smithson, 2000).
The optimal composition of groups to promote open discussion is between six and eight plus a facilitator (Finch et al., 2014). Some diversity is thought to be beneficial to stimulate discussion alongside a level of commonality to create trust within the group. For the current study, six groups were undertaken across three of the four trusts. Groups were divided into two types: social worker only and other CMHT professionals. Members of individual groups worked within the same NHS Trust. Some worked in the same teams. All knew at least one other member of their group. The fourth Trust (one of those with social workers in their CMHTs) was unable to bring a group of social workers together due to staff shortages whilst only one person turned up to take part on the allotted day of the other professionals group. The facilitator was a member of the research team (MA). A second member of the research team (SB/RP) was present to act as timekeeper and to support the process through attending to late comers and collecting consent forms. Ground rules about confidentiality were set at the start of each group and a summary of the process described. Groups lasted between 35 and 55 minutes.
Data analysis
A thematic analysis was undertaken, using Braun and Clarke’s (2016) ‘organic’ approach, whereby themes are ‘crafted’ (740) by the researcher through reflection and interpretation of the data, forming a representation of the researchers’ understanding of the data. Analysis was inductive, being data rather than theoretically driven. Codes, concepts and themes were developed throughout the analysis process, moving from semantic description to interpretation with the aim of conceptualising ‘the significance of the patterns and their broader meaning and implications’ (Braun and Clarke, 2006: 84). Subjective understanding is acknowledged within this method. Frequency of views is of less significance than relevance within this approach meaning that minority views that express issues closely related to research questions are just as important as identifying consensus within the data. The practice is iterative, rather than linear, with refinement of ideas throughout the analysis process. Braun and Clarke’s (2006) six-stage process of familiarisation, initial coding, searching, reviewing and defining themes, and producing the report was used. This process was undertaken by the lead author in the first instance with periodic discussion to challenge, modify, develop and reach consensus, with other co-authors who were familiar with the data through their presence during data collection or through their reading of transcripts. The coding system can be seen in a supplementary document (available from the journal).
Ethical approval for this study was granted by the North of Scotland (2) Research Ethics Committee: grant number: 17/NS/0127. All participants provided written informed consent.
Findings
Thirty-five staff participated in the focus groups of whom 20 were social workers. The non-social worker groups (from here on referred to as CMHT colleagues) comprised a mix of largely mental health nurses and occupational therapists with a smaller number of psychologists and support workers. Two of the three social worker groups included a team manager who was also a social worker. Team managers were also present in two of the CMHT colleague groups (representing occupational therapy and mental health nursing) with two present in one group. Most participants were female (ratio of 28:7). A breakdown of group membership which protects anonymity is presented in Figure 1.
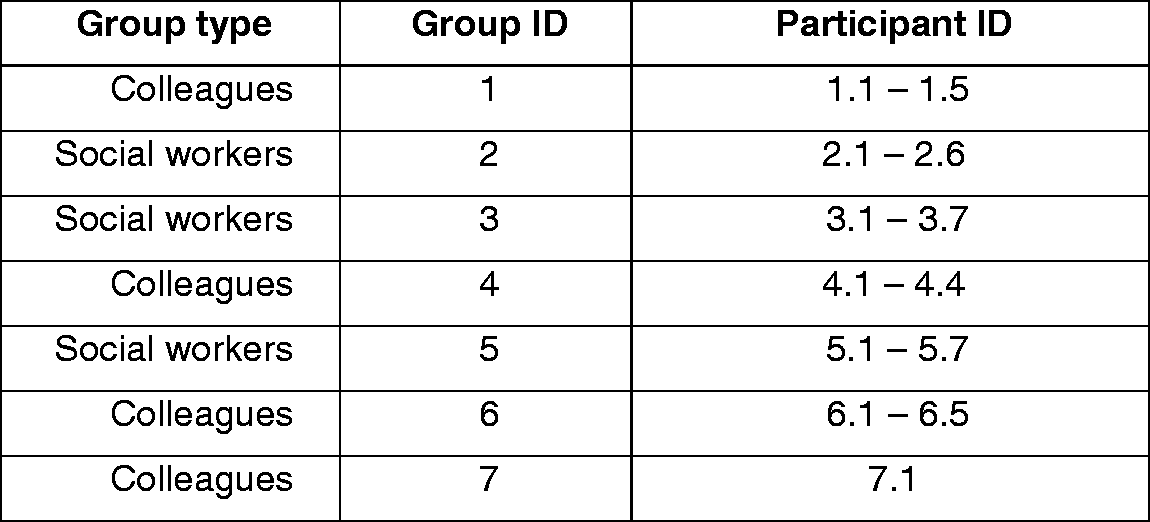
Group and participant type and ID.
Data analysis resulted in the construction of three major themes: (i) social workers’ self-conception of their contribution, including distinctive underpinning principles and values; (ii) CMHT colleagues’ understanding and valuing of the social worker role and (iii) the perceived implications of the loss of the social worker contribution to CMHTs for service users. Each theme contained subthemes, summarised in Figure 2.
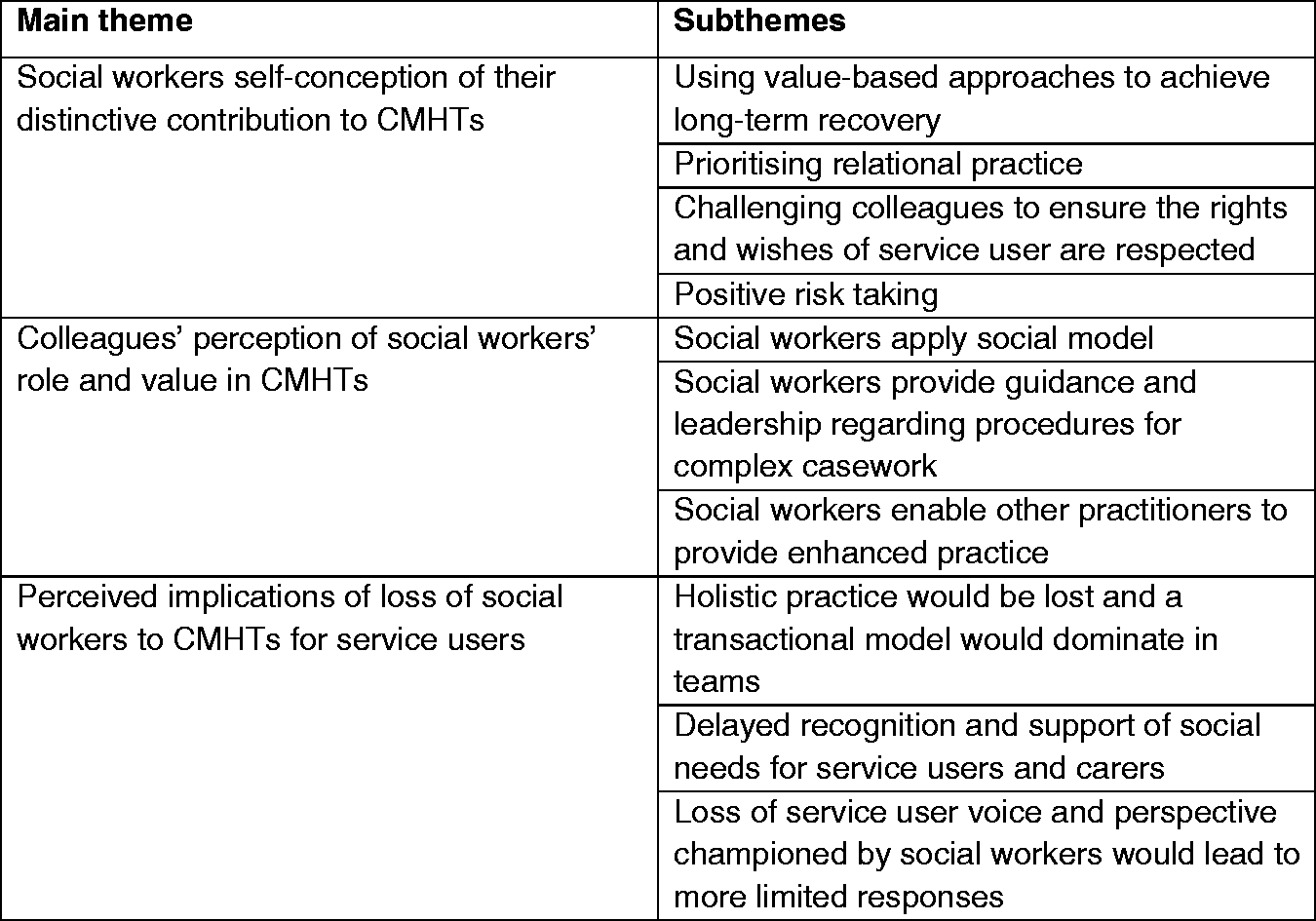
Themes and subthemes.
Social workers self-conception of their distinctive contribution
Social workers perceived themselves as making a distinctive contribution to the work of CMHTs, ensuring service users were seen ‘in the round’, accessed support and were enabled to achieve long-term recovery. They distinguished themselves from their team colleagues in terms of their understanding of the social determinants of mental ill health and their approaches to overcoming these. This was explained as bringing to their role an understanding of how, for example, poverty and discrimination affected mental health (e.g. leading to social isolation) and the skills and knowledge to work with people to ameliorate negative impacts. The example below illustrates this emphasising the differences between the social worker approach and other professionals who employ a medical model: We work in a long-term model of empowerment, so we’re building strength and resilience, and we’re working to long term recovery. So if you’re looking at the medical model, it’s very short term isn’t it … [Social work is] about the long term stuff, increasing choice and control … you get all of those social factors in place and people are more resilient … it can’t just be contained in a hospital admission, medication. (Social worker participant 2.3) There’s something about communication skills that comes into our role that’s quite complex … Sometimes it can just be a normal visit and there’s lots that’s thrown up at you and you have to think about in reflective practice … that’s just your day to day kind of care planning with your service users. (Social worker participant 2.2) We’re … less willing to give up on somebody … The medical model is much more ‘two shouts and … you’re out’. [We’ll] work with the person and we can see all the pressures because we’re going to their home environment and we can see what they’re under. (Social worker participant 3.4) Part of our role is obviously to promote their rights and give them the information and advocate on their behalf … and I think we’re really good at that. (Social worker participant 3.4)
CMHT colleagues’ perceptions of the value of social workers to the wider team
CMHT colleagues recognised the centrality of the social model to the social work role. They spoke of social workers having a ‘wider perspective’ (CMHT colleague participant 1.4) than other CMHT members, involving going ‘back to the causes … the things that the medical model just don’t realise’ (CMHT colleague participant 4.2) and looking at ‘what might have happened to that person that might have led to the situation that they’re in’ (CMHT colleague participant 1.4). This perspective was valued by them as helping to enhance their thinking and practice beyond the immediate medical issues. They also valued what they described as social workers broad knowledge and skills that could lead to improvements in their own practice in terms of: timeliness, person-centred and holistic approaches.
There was a recognition from all participants that a working knowledge of a range of ‘generic’ tasks was required of all care coordinators working in CMHTs. However, such work was reported to be undertaken with more confidence and efficiency where there was access to specialists (in this case social workers) for advice and support relating to social care. I’m trained as a CPN, and my focus mainly is … on the effects and side-effects of medication … I still have to deal with housing issues … I feel confident when I have a specialist in the team that I can ask, and validate whatever I’m doing. (CMHT colleague participant 6.2) It was so helpful having them there … knowing which other agencies around domestic abuse I could contact and what forms I had to fill out to carry that process forward …It was great having someone in my office who sits next to me who’s so knowledgeable … It’s kind of time sensitive because the person’s abuser is coming out of prison. (CMHT colleague participant 1.2) If they’re already within the team … they’ll know what’s going on, on a regular basis … they would have already had all the background … It makes it so much easier than meeting up with them for a meeting, because the CTO is about to occur, ‘cause that seems to be what happens now. (Participant 4.3) That is massively valuable to me to have these brief discussions with them … it can throw the case in a whole different direction and usually a much more positive direction by having that discussion with them. (CMHT colleague participant 1.3) I’m always checking my responses when I’m working with somebody…. why have I got that team involved? … Am I dis-enabling the service user by trying to put more care in? How do I work … to best empower that service user … ? (CMHT colleague participant 7.1) Most of the individuals can do a lot of things for themselves but mental health services are doing a babysitting role … and I think the way services should be set up is to get people to … live more independently. You can’t do that if you have a service that keeps people drawing back in (Participant 6.4)
Perceived implications for service users of losing social workers from the CMHT
The contribution of the social worker to the CMHT has been positively identified in the two preceding sections. Participants also directly discussed the impact they perceived that the absence of social workers in the teams would have on service users. Concerns focused on three areas: the replacement of relational with transactional support, delay in recognition of social needs leading to less timely service delivery and a diminished service user voice and consequent adoption of more restrictive practices with a loss of social justice.
There was one alternative voice who took a critical stance regarded social work as one of many professions or agencies, like GPs and the police, to be called upon when needed. This person argued that where an issue required social worker input, a referral could be made and, consequently, there would be no loss to the service user. Whether you are … contacting the GP or police or safeguarding team or whatever, a lot of it is these different teams working in different hubs, and when they need to get involved, they get involved and … life goes on. I think it might make more efficient use of services if people are simply completing the piece of work they have to do for that particular case. (CMHT colleague participant 6.4) If we were to lose [social workers from the team] … we actually regress as a paradigm in terms of recovery model because we’re going back into management of medical model type reduction strategies for treating mental wellbeing, rather than seeing the whole picture. (CMHT colleague participant 6.2) I think we perhaps wait, and then a bit further down the line, we might think, oh yeah, this person might benefit from a Social Care Act assessment, and then things might have deteriorated … further than perhaps would have done had [social workers] been sitting in our meetings. (CMHT colleague participant 4.4) It’s not about they can’t get that service, you can still refer them, but how long is it going to take you to do that? When you’ve got your colleague actually in the system, I feel that it actually speeds everything up, and it’s very beneficial to the service user. (CMHT colleague participant 6.2) A medic might say, well our option is, are you going to take the medication, no? So you’re going to need to be in hospital then. A social worker might have different considerations … from a different angle. (CMHT colleague participant 4.2). So he was telling the doctor … I don’t want to take it any more … And the doctor and the nurse were saying, well … he’s older, he’s not married, why does it matter? I said, but it does … he’s telling you it’s important to him. (Social worker participant 5.3)
Discussion
The findings from this study provide detailed evidence of social workers’ unique contribution to CMHTs, identifying a distinctive value for services users and team colleagues. Their role was expressed in terms of both what they do in enabling service users’ recovery and social inclusion, and how they do it by prioritising the relational element of working with service users. It was demonstrated that they undertake value-based practice that supports the whole team to adopt more holistic, person-centred approaches that assures added-value to both service users and team members alike (Penhale and Young, 2015). The findings are important in adding empirical evidence to the calls from within the profession and from both local and central government to preserve, enhance and support the social work role within CMHTs (e.g. Association of the Directors of Adult Social Services, 2017; DH, 2016). There was an alternative opinion suggesting that uncertainty about the social workers’ role in integrated teams may exist among other professionals. Three key findings, summarised in Figure 3, are discussed below.
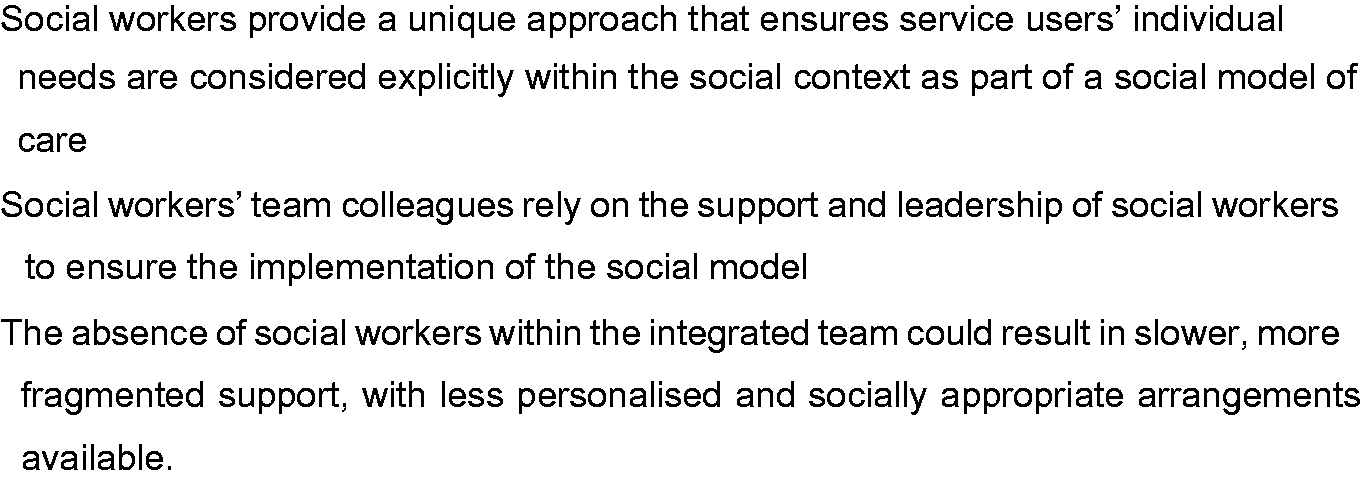
Key study findings.
The social workers’ unique approach
The findings demonstrated a sophisticated articulation of the social work contribution by social workers and their colleagues, rationalising their role according to strong underpinning principles which oriented their contribution to a social model. Previous research into CMHTs for older people found that non-social work staff valued social work team membership for their specific skills, knowledge and values and in improving communication pathways within and beyond the team (Abendstern et al., 2014). Earlier studies also pointed to differences in social worker attitudes’ compared with their colleagues that could influence CMHT service delivery. For example, social workers (and psychologists) were significantly less likely to support compulsory treatment compared with psychiatrists or nurses (Steinert et al., 2005), were more able to accurately identify complex social needs than nurses (Cestari et al., 2006), to be the ones to defend the rights of people with the most complex needs (Roysum, 2017) and to have the ability to recognise issues beyond the immediate (Morriss, 2017). The current findings concur with these earlier reports, emphasising that social workers undertook distinct roles and tasks contingent upon specific social work knowledge, skills and values that encouraged more person-centred support.
Social work support to colleagues
The findings also indicated that the presence of social workers is important in supporting colleagues and enhancing the work of the whole team. Whilst others support the ethos and approaches taken by social workers, these are not necessarily central to their own work, and they were perceived to rely on social workers to keep the social determinants of health, the holistic approach and the rights and voice of the user central to practice. Peck and Norman (1999a) noted that social workers were the only CMHT members reportedly challenging medics with nurses questioning whether they got tired of this role. Twenty years on it appears that they are still in this position. The implication is that if mental health services are to deliver social wellbeing and tackle the social determinants of mental ill health and social trauma, social workers need to be at the heart of integrated team practice. Recent legislative guidance in England has stressed the importance of integration between health and social care in mental health, citing social workers as playing a vital role in achieving this goal as leaders ‘both in their teams and across professional boundaries’ (Care Act, 2014: 1.30). The detailed evidence from social workers and their colleagues working in CMHTs in this study supports these statements.
Potential service user loss
The significance of the social worker role within mental health teams was emphasised in England by an APPG (2016). Their report stressed the importance of social workers in enabling people with mental health difficulties to achieve essential outcomes, such as protecting people’s rights and using solution-focused approaches to practical, emotional, health and legal issues. It stressed the lack of recognition and attention given to these crucial roles in policy or legislation, despite being ‘the things that people using services say are most important to their recovery’ (APPG, 2016: 3). The findings of this study add to weight to these statements. They demonstrated that without social workers in the CMHTs , users would be likely to receive a more restricted and transactional-based service which paid less attention to their rights and wishes and that access to appropriate support could be delayed with negative consequences for mental health. The question of whether social workers’ CMHT colleagues should incorporate a more holistic approach into their practice is also raised by this research. The vital but separate roles played by nurses, occupational therapists and other CMHT members was noted by participants in this and earlier research (e.g. Peck and Norman, 1999a, 1999b). Overall, the findings emphasise the need for CMHTs to have a range of skills and expertise available to service users that cannot be expected to be the domain of any single professional group.
Study limitations
First, the focus group approach has some strengths described in the method, but there are also limitations, which in the current study relate to the voices within the groups of CMHT colleagues. Although these contained some variety, the voices of nurses and occupational therapists dominated the discussions, possibly reducing the perspectives captured. Second, whilst our aim was to consider social work, the lack of discussion of the AMHP role is a potential weakness and should be addressed in future research. Third, the service-user voice is also absent from this study despite the question posed aiming to understand their experiences. Other elements of the larger study of which this paper forms a part have addressed service users directly, examining their preferences with findings supporting those reported above, particularly in relation to the social workers’ holistic perspective (Wilberforce et al., 2019). Future studies might also consider the implications of the social work role on carers as well as service users. Finally, although the statutory and organisational arrangements specific to England framed the focus group discussions, the findings relating to social work practices and approaches in relation to their direct work with service users and their support to colleagues are of international relevance.
Conclusion
The range of voices within this study offer an insight into the level of understanding and support for the social work role in this context. The critical voice alerts us to the challenges that may exist for social workers when their role is obscured and highlights the importance of nurturing and building its profile, protecting its specialist contribution within integrated settings. The findings provide strong evidence to support the continued presence of social workers in CMHTs as specialists, whose unique value-based approaches promote whole team practices that are valued by service users and team members alike.
Supplemental Material
sj-pdf-1-qsw-10.1177_1473325020924085 - Supplemental material for Perceptions of the social worker role in adult community mental health teams in England
Supplemental material, sj-pdf-1-qsw-10.1177_1473325020924085 for Perceptions of the social worker role in adult community mental health teams in England by Michele Abendstern, Jane Hughes, Mark Wilberforce, Karen Davies, Rosa Pitts, Saqba Batool, Catherine Robinson and David Challis in Qualitative Social Work
Footnotes
Acknowledgements
The views expressed are those of the authors and not necessarily those of the NIHR SSCR, the National Institute for Health Research or the Department of Health and Social Care.
Declaration of conflicting of interests
The author(s) have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by the NIHR School for Social Care Research.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.