
Abstract
Summary
Social workers are positioned to respond to clients with a history of trauma by practicing bio-psycho-social, trauma, and violence-informed care but frequently encounter systemic barriers to providing holistic care. The research presented in this article was initiated by a College of Social Work in Canada in response to concerns raised by social work providers that their practice was constrained by ideological, structural, and system limitations within publicly funded mental health and addiction services. Ideologically trauma-based social work care is defined by five principles of safety, trust, collaboration, choice, and empowerment and recognizes that what has happened to individuals, including early adversity, can influence their bio-psycho-social functioning across the lifespan. Structurally, trauma-based care recognizes the corrosive impact of poverty, systemic discrimination, and exclusion.
Findings
Our research included a literature review, an online survey (n = 115 completed surveys), individual interviews (n = 50), and three focus groups (n = 15). The findings consistently highlighted a dissonance between dominant bio-medical approaches and reliance on the Diagnostic Statistical Manual of Disorders and social justice–based practice. Primary themes included a recognition by social workers of the pervasive presence of trauma and its effects, including mental health and addiction challenges; intergenerational impacts of trauma; the limitations of the medical model; and the need to reposition social work practice.
Applications
Repositioning the role of social work within mental health and addiction settings to center social justice responses to trauma presents transformative opportunities to better meet the needs of service users and increase workplace satisfaction.
This article presents findings from a provincial study that explored how social workers perceive their role within mental health and addiction services. This study was initiated as a response to concerns raised by social workers across the province of Nova Scotia, Canada to the College of Social Work. These concerns acknowledged limitations to their practice imposed by ideological and system constraints that resulted in a dissonance between the dominant bio-medical model that relies on the Diagnostic Statistical Manual of Mental Health (DSM-5) (American Psychiatric Association, 2013) and their preferred approach to practice; a bio-psycho-social, justice-based approach that is trauma-based (Healy, 2016; Levenson, 2017; Nathan & Webber, 2010; Yip, 2004). We argue social work responses to trauma, for the past one hundred years, have incorporated an understanding that the relational injury associated with experiences of violence and trauma often harm a person's sense of agency, safety, negatively impacts upon self-esteem, and creates difficulties in regulating emotions and navigating trusting relationships. Principles of trauma-based care include providing approaches that enable safety, trust, choice, empowerment, and collaboration, and the recognition that trauma often impacts individuals across their lifespan (Herman, 2015; Levenson, 2017; Substance Abuse and Mental Health Services Administration, 2014). While these principles constitute what is commonly referred to as trauma-informed care we expand upon this term to use “trauma and violence-informed” to underscore the connections between trauma and cultural, structural, and direct forms of violence (Galtung, 1990; Government of Canada, 2021). The exponential rise in acceptance of the term “trauma-informed” has been critiqued as resulting in standardized practices that are often depoliticized, degendered, medicalized, and individualized within systems subject to neoliberal constraints (Johnstone et al., 2022; Tseris, 2019). In choosing to use the term “trauma and violence-informed,” we locate the source of distress within structural, cultural, and systemic inequity, including experiences of racism and colonization; not within individuals (Clark, 2016). In this way, tendencies toward biomedical and pathologizing responses to trauma can be resisted as it is the violences experienced within social contexts that must be acknowledged and contested. This emphasis on social context is aligned with social work's emphasis on the need for critical reflection and a bio-psycho-social model of practice that is particularly helpful in acknowledging the ways children's behavior and development can be understood as cumulative responses to violence and abuse that occurred within stressed environments (Burstow, 2003; Ellis & Dietz, 2017; Herman, 2015; Lafrance & Stoppard, 2007; Larkin et al., 2014; Tseris, 2013).
Long after traumatic events have ended individuals can continue to feel shame, helplessness, and fear (Herman, 1992, 2015). While a bio-psycho-social approach is important when holistically addressing the concurrence of these issues, too often the social aspects are left out when the focus is primarily biomedical. We present research findings that describe concerns about constraints to practice noted by social workers; particularly related to responding to trauma, and employ the principles of social work trauma and violence-informed care as a framework of analysis (Levenson, 2017; Substance Abuse and Mental Health Services Administration, 2014).
Literature review
The history of social work practice is rooted in responses to trauma with individuals, families, and communities. Social work emerged as a distinct profession in the late nineteenth century when the Settlement House and Charity Organization Society movements merged to provide community services to new immigrants, women and children and families in need as early as 1889; many of whom had prior experiences of trauma (Knight, 2010). Adequate housing, food security, and non-violent relationships were recognized as central to safety, the first principle of trauma-based care (Herman, 2015; Hick & Stokes, 2017; Levenson, 2017). Prioritizing safety included a recognition that circumstances in one's social context can contribute to their vulnerability to harm and that access to the social determinants of health, including employment, housing, and income assistance are necessary to feel secure (Harris & Fallot, 2001).
Feminist social workers and survivors of interpersonal trauma further influenced the importance of prioritizing safety as the gender-based anti-violence field emerged in the 1970s to contribute to the development of services to respond to domestic violence, sexual assault and incest (Armstrong, 1983; Bass & Davis, 1994; Brown, 2013, 2018, 2020; Brownmiller, 1975; Burgess & Holmstrom, 1974; Burstow, 2003; Forward & Buck, 1988; Herman, 1992, 2015; Ross & Morrison, 2020; Tseris, 2013). Smith and David's (1975) text titled Women look at psychiatry: I’m not mad, I’m angry emphasized the importance of recognizing how experiences of injustice and trauma can result in symptoms that are pathologized as mental illness. Similarly, in 1972 Phyllis Chesler critiqued “psychiatric imperialism” and the diagnosis of women in her definitive work Women and madness. She noted that oppression itself was traumatizing. As such, these texts serve as an early call to consider what has happened to individuals as opposed to what is wrong with them. This approach is now a hallmark of current trauma and violence-informed approaches that emphasize empowerment as a principle of trauma and violence-informed care. Empowerment, a ubiquitous term in social work practice, has come to represent a strengths-based, social justice approach that both celebrates survival and coping skills and recognizes “power” as a political and economic force that can fuel injustice, limit choices and access to care (Lemke, 2001; Marecek, 2006; Morrow & Malcoe, 2017). The ability to choose is extinguished by oppressive experiences and abuse of power and therefore choice is an essential principle of trauma and violence-informed care and an important component of self-determination and healing processes (Levenson, 2017).
Feminist research and practice led the way in recognizing the serious impacts of sexual assault, domestic violence, and childhood physical and sexual abuse that are associated with a loss of confidence, depression, anxiety, and substance use which are then often pathologized (Brown & Stewart, 2008; Burstow, 2003; Butler, 1978; Herman 1992, 2015; Herman et al., 1989; McKenzie-Mohr & Lafrance, 2011; Ross & Morrison, 2020). Nowhere has this process been established as clearly as in the growth of individuals diagnosed with “borderline personality disorder” a diagnosis overwhelmingly applied to women with a history of trauma and abuse (Becker & Lamb, 1994; Brown, 1992, 2020; Cermele et al., 2001; Herman, 1992; Marecek & Gavey, 2013; Tseris, 2013). Feminists examining the context of women's lives and the impact on their mental health struggles have argued that women's misery has often been medicalized (Lafrance & McKenzie-Mohr, 2013; Ussher, 2010).
The links between prior adverse childhood experiences and trauma and the development of a substance abuse problem and/or addictive behaviors among girls and women is significant and profound (Brown, 2020; Najavits, 2002; Ross et al., 2015; Ross & Morrison, 2020). These connections are also increasingly recognized among men (Augusta-Scott, 2020; Lew, 1988) and trans-women and men (Cochran & Mays, 2007; Cox, 2014). In the late 1980s, Lew (1988) authored a book specifically about steps men could take to recover from incest and other sexual child abuse in which he made connections to mental health and substance use challenges.
Following the earlier work of Herman in 1992, Felitti et al. (1998) and his team published the results of a landmark study describing the relationship of trauma and adverse childhood experiences (childhood abuse and neglect, and household dysfunction) to many of the leading causes of illness and death in adults. A global systematic review and meta-analysis of the effect of trauma and multiple adverse childhood experiences on physical health and mental wellbeing found that individuals who have experienced four or more adverse childhood experiences were more than twice as likely to be current smokers or heavy drinkers, almost six times as likely to drink problematically, about four times more likely to experience anxiety and depression, about eight times more likely to be a victim and/or perpetrator of violence, and thirty times more likely to attempt suicide than those who had no adverse childhood experiences (Hughes et al., 2017). Working with individuals who have substance abuse issues, mental health challenges, and prior experiences of violence is central to social work practice. Research related to adverse childhood experiences signals the urgent need to provide care and advocate for prevention of all forms of abuse and violence. Since many survivors of adverse childhood experiences were betrayed by those who were supposed to protect and care for them, they are often vulnerable to abuse of power by those in authority positions, including helping professionals. As a principle of trauma and violence-informed care social work practitioners recognize the development of trust as a relational process that can take time to be established. In their practice, social workers recognize this process is necessary to permit risk-taking by service users and self-paced disclosure to model healthy relational processes (Levenson, 2017). Collaboration, another principle of trauma and violence-informed care, emphasizes a social worker's professional knowledge is combined with the service users’ expertise about their life narrative (Levenson, 2017). Recognition of this expertise encourages service users’ engagement in determining their goals and together defining what is necessary for their healing.
While safety, trust, choice, empowerment, and collaboration are central to trauma and violence-informed care, the recognition of intergenerational effects also guide social work practice. A growing amount of research notes that safe, stable, and nurturing relationships between intimate partners and between mothers and children can break intergenerational cycles of abuse (Bethell et al., 2017; Bombay et al., 2014; Jaffee et al., 2013). This research validates the importance of helping people develop skills necessary to have healthy relationships with both their partners and children. These efforts have been central to trauma and violence-informed social work care. This direction supports a move from system-centered services to care that is human-centered and relational; prioritizing parental skill development and the need to have adequate resources to be able to provide safe and nurturing care to children. The profession of social work's commitment to social justice also promotes a critical analysis of the profound ways in which structural and cultural inequities compound experiences of childhood adversity, oppression, and can result in interpersonal violence and poor health throughout the lifespan. This analysis positions the profession to lead responses to adverse childhood and traumatic experiences by integrating biomedical insights within the ongoing development of holistic trauma and violence-informed care, and in defining social policy measures and prevention strategies. This article underscores the history of critical engagement with trauma, violence, and adverse childhood experiences by the profession of social work and proposes this work is central to social work practice in mental health and addiction settings. Centering responses to trauma experienced by individuals, families, and communities requires innovation and coordination.
Methods
In response to a call from the Nova Scotia College of Social Workers to explore the concerns raised by social workers within mental health and addiction settings, the authors jointly conducted a consultation across the province. These concerns included excessive wait times and system constraints that limited their full scope of practice and resulted in their dissatisfaction in the workplace and among service users. This research explored the experiences of adult service users, service providers, and service supervisors of social work in mental health and addiction public funded care by conducting individual interviews, focus groups and an online survey to gather evidence that reflects the experience of those on the front lines of mental health and addiction services in Nova Scotia. Our aim was to explore their perceptions of strengths and limitations of services in individual interviews and focus groups. Our questions explored areas related to barriers, equity, access, funding, infrastructure, dominant mental health discourses and the impact of marginalization and discrimination on mental health and mental health services. All participants were over the age of eighteen. The three methods of data collection, alongside a literature review, provided consistent data and data saturation.
Data collection
Opinio survey: Service providers/supervisors
We conducted an online survey that explored the experience related to mental health and addiction care by using the Opinio survey platform through Dalhousie University to reach as many participants as possible. This survey was promoted by the Nova Scotia College of Social Workers on the social media platform Facebook, their online magazine and newsletter which is emailed to over 2000 members. The survey results which permitted an initial sense of social worker's perspectives of the provision of mental health and addiction care, were followed with in-depth individual interviews and focus groups. Recruitment criteria was membership in the provincial College of Social Work which is a requirement for practice. To maintain anonymity, participants were asked not to provide their contact information. The introduction to the survey provided information related to anonymity, confidentiality, and a list of services available should participants find their participation unsettling and require therapeutic follow up support. This information also informed participants that if, at any time, they chose to end their participation and withdraw from the survey, there would be no negative repercussions. The decision by participants to participate in the survey implied their informed consent. In total, 115 participants completed the survey online (166 people contributed to the survey with 51 not fully completing it).
Individual interviews and focus groups
We conducted fifty individual interviews in total, thirty with mental health service providers, ten with supervisors, and ten with service users. In addition to the College of Social Work newsletter and word of mouth (snowball sampling), participants were recruited through posters distributed in the community and a service user Facebook site. We intended to interview 50 people and our recruitment process resulted in this ratio of interview participants. Interviews took place in person or by telephone to allow for greater representation across the province and were approximately 90 min in length. We offered $50 honorarium to service users who were interviewed to compensate for childcare and/or transportation costs incurred. Each participant was provided written information prior to the interview so they could make an informed consent regarding their participation as outlined above. These measures followed the standards established by Dalhousie University Research Ethics Board.
Focus groups took approximately 90 minutes each with a total of 15 participants. We conducted three focus groups among service providers, one urban area (n = 5) and two in rural areas (n = 6) and (n = 4). The first two focus groups were conducted in person by the research team, with the final rural focus group conducted through Zoom due to provincial requirements of social distancing during the COVID-19 pandemic. The research team chose three different areas of the province that they felt were representative of both rural and urban areas and recruited participants in these areas by emails sent out by the College of Social Work. Individual and focus group interviews were audio recorded and later transcribed verbatim with identifiers removed as part of the data collection and research findings. The results of this study were shared by request with participants for member-check upon the completion of the project.
Analysis
The survey explored questions related to scope of practice and employment satisfaction with primarily closed ended questions. The Opinio survey software providing initial analysis of the data. The small number of open-ended questions in the survey were thematically analyzed and these results were integrated and further explored in the semi-structured interview schedule.
The interview narrations were thematically coded and integrated with the survey data. The thematic analysis approach of Braun and Clarke (2006) begins with identification of themes before progressing to a discursive analysis that encourages the contextualization of participant narratives and the recognition of dominant cultural discourses influencing service delivery that include neoliberalism, professionalism, and biomedicalism (Braun & Clarke, 2006; Clandinin & Connelly, 2000; Wells, 2011).
Our data analysis situated participants’ stories about mental health and mental health services within dominant social discourses and within the context of their lives to enable the participants’ narratives to be contextualized within the broader social constructs and dominant discourse of mental health (Brown, 2018; Ross & Morrison, 2020; White, 2007). The three methods of data collection, alongside a literature review, provided consistent data and data saturation.
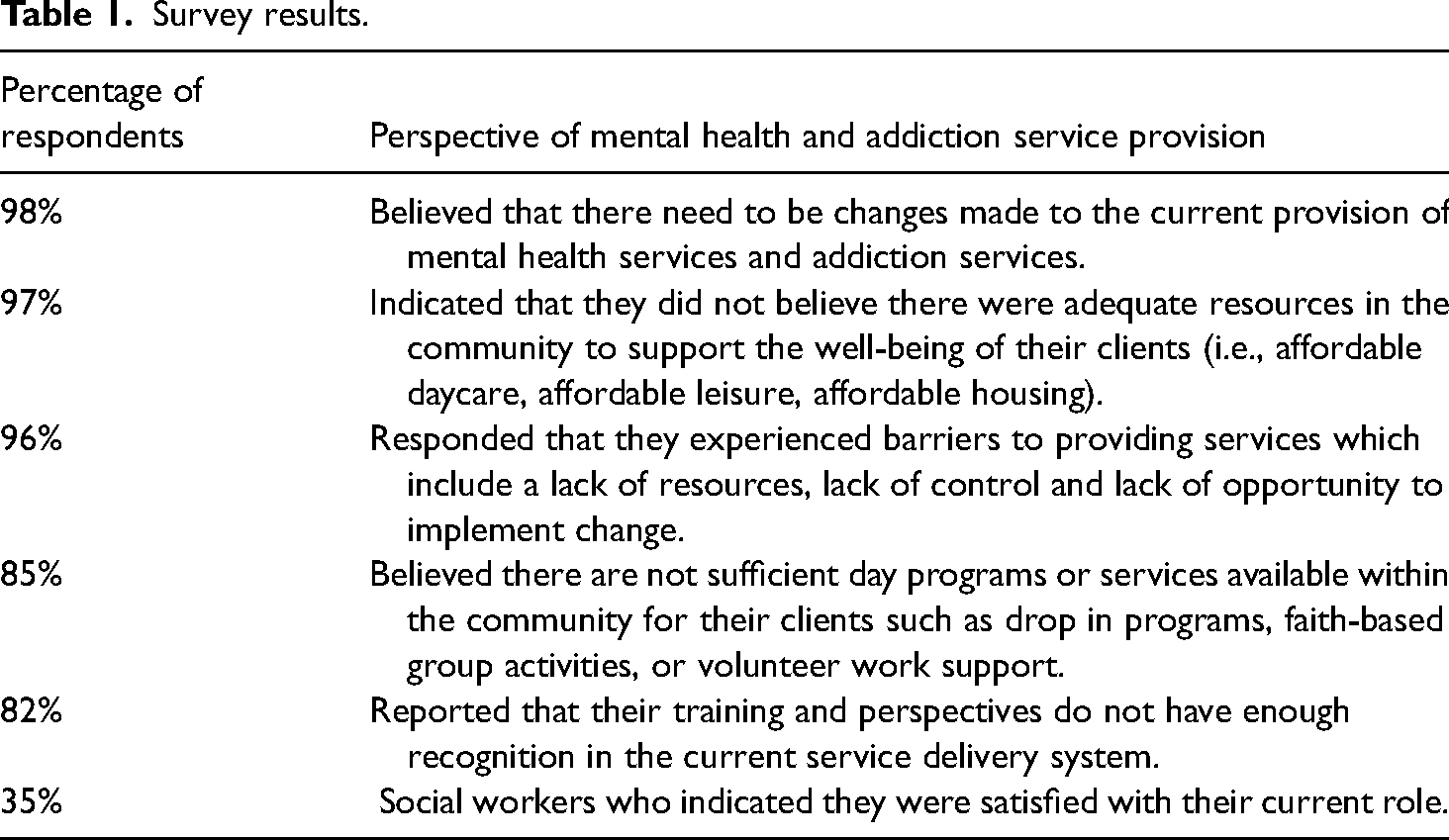
The following sections describe a) socio-demographic information of the research participants, b) findings that emerged from the Opinio Survey in Table 1, and c) five central themes that emerged from this study specific to trauma within social work practice and mental health care. These themes included: the need to respond to pervasive trauma experiences, mental health, and addiction issues as a result of trauma, intergenerational trauma, the limitations of the medical model, and the need to reposition and empower social work practice to better respond to trauma.
Survey results.
Findings
Socio-demographic information
Data collection began with a separate author-compiled socio-demographic questionnaire with all participants in the study. The aim of the socio-demographic questionnaire was to provide insight on the social determinants that impact participants’ realities, such as income, employment, ethnicity, sexual orientation, gender expression, and education. The age categories representative of most participants were between the ages of 30 and 44 (n = 51) and 45 and 59 (n = 47). Most of the participants, (n = 119), identified their gender as female, 22 as male, one participant identified as Male (cis) Two Spirit and another as gender diverse. Twenty-one participants are 2SLGBTQIA + with identities that include: queer, gay, lesbian, bisexual, bisexual Two-Spirit, and pansexual. One hundred and nine participants identified as White and other racial/ethnic identities included Indigenous, African Nova Scotian, African Canadian, and Sinhalese. Most participants speak English as a first language; other languages of note are French and Sinhalese. Most participants were in relationships and 83 participants had children. Almost all (117) participants were employed full time, 17 part-time, two retired. Most participants had a master's degree in social work (93) with 42 participants educated at a bachelor level and three people with PhDs. Of those employed, the majority work in the public sector, primarily the Nova Scotia Health Authority and the IWK. Fifteen providers identified as working in private practice, and 5 in both private and public systems. Most noted their individual income category between $60,000-$79,999, while those with a combined income primarily indicate their income as between $100,000-$149,999. Thirty-one participants are living with a chronic illness or (dis)Ability.
Survey results
As highlighted in Table 1 below, the survey explored the perspectives of mental health and addiction service providers with primarily closed questions that resulted in “yes” or “no” responses that were tabulated and presented as an aggregate final total by the Opinio software. The meaning of these initial results was explored in greater depth in the individual interviews and focus groups. The results from the Opinio survey indicated that most participants believed there were not enough available resources for their clients and that they experienced barriers in offering mental health and addiction service care. The survey results also indicated that most participants were not satisfied with their current role and believed that change needed to occur within the delivery of mental health and addiction services to broaden the scope of practice of social workers. Additionally, the survey results pointed to a social justice mandate to advocate for adequate resources within communities to support their client's wellbeing.
Thematic analysis
The need to respond to pervasive trauma experiences
The results of our research indicated that the need to respond to experiences of trauma was central to social work practice. One participant reported, sexual abuse…. That's the majority of my caseload right now…… we all have children who have been impacted…most of them have been impacted by trauma. (Rural 1 Focus Group Participant, Sue)
Given that recent studies confirm that over one billion children between the ages of 3 and 17 worldwide experience a severe form of childhood abuse this is not surprising (Hillis et al., 2016; Knaul et al., 2020). Another social worker, Alexandria, who worked in crisis intervention services said when patients were asked questions about what had precipitated their admission to hospital it was very common for them to share their experience of past trauma and/or sexual assault. Service provider Jess also identified the prevalence of an underlying history of trauma in her social work practice and, consequently, the need for more training in this area. A consistent theme in our research was the overwhelming presence of trauma in the lives of individuals accessing mental health and addiction services and the concurrent need for ongoing related professional education.
Interviewee Sara referred to the growing body of knowledge about the prevalence and physical and psychosocial impacts of adverse childhood experiences as helpful for people to make the connections between these experiences and health challenges. She said: So right now my trauma therapy looks like using the …… adverse childhood experiences to build like a context for people to understand that they’re not alone in that experience. So we do….. sensory kind of things ….to learn different skills to help with disassociation, or different calming techniques that they can use if they are experiencing a highly anxious moment or something's triggered their childhood response. (Social Work Provider, Sara)
Interviewee Peter also made the connection between adverse childhood experiences, stress, and subsequent health issues. These stress reactions are normal responses to trauma and often reflect a predictable “fight or flight” response (Herman, 1992). Prioritizing the relationship between the client and therapist, a principle of trauma-based care, involves assisting the client to understand how they have coped through exploring the meaning of trauma experiences.
Mental health and addiction problems: Responses to trauma and violence
A second theme pervasive in the data implied an understanding that many of the problems individuals described when accessing mental health and addiction services could be understood as a response to trauma. For example, one social work provider indicated that many of the women who accessed her services initially expressed symptoms of anxiety and depression that were often the result of violent experiences. But that's usually made quite invisible unless you actually name it. And then you can say to women, “did you know that there's a big connection between mental health issues, substance use, violence against women, financial dependency, all of those gendered factors?” And they go, “Oh my god, yes.” And then they’ll say, “Now I know I’m not crazy.” Or if you talk about the social, political context in which sexual assault, sexual violence takes place, and they say, “Oh my god, I knew I wasn't crazy.” But they could be crazy depending on who they go to, right? You know, it depends who's looking. (Social Work Provider, Karen)
Karen indicates that the impact of violence and trauma can be assessed differently depending on the theoretical framework that is applied. She describes situating trauma and experiences of violence within a political and social context moves away from pathologizing the individual to a recognition of the impact of oppressive factors on their life that are often gendered. Empowerment, a central theme of trauma and violence-informed care incorporates a social justice framework that recognizes individuals who have experienced trauma can feel powerless and that this is compounded by social inequity. Brown and Stewart (2008) argue that trauma often precedes the development of anxiety and/or depression, which is often addressed through substance use. For example, among girls and women, the links between substance use and sexual victimization are profound (Poole & Greaves, 2012; Ross et al., 2015).
A social work supervisor noted that the recognition that trauma could have negative impacts on both physical and mental wellbeing resulted in more holistic assessments. They said: It's actually one of the things that I really have to make a point to ask about when I’m doing assessments because as you probably know, the effects of trauma on health are becoming better understood all the time. And particularly in clinics like the diabetes management centre, for example, where folks are dealing with obesity or problems with eating, the chances of some of those folks having an underlying trauma are pretty great. People who are gender non-conforming or who are dealing with gender dysphoria, the chances of trauma are huge. (Social Work Supervisor, Miller)
In Canada, at least 20 percent of people with mental health problems have a co-occurring substance use problem (Rush et al., 2008). Research estimates a 7 to 45 percent overlap between alcohol dependence and depression and anxiety, a link which is commonly higher among women (Rush et al., 2008). In general, the research literature has established strong links among substance use, eating disorders, depression, anxiety, and posttraumatic stress with histories of trauma and violence among women (Brown, 2018; Herman, 2015). An emerging body of literature also points to the vulnerability of people who are gender non-conforming or who experience gender dysphoria to experiences of trauma and subsequent mental health challenges, particularly depression and suicidality (Cox, 2014; Bechard et al., 2017).
“Eroding the soul”: Intergenerational trauma
Many of the individuals who participated in this research addressed the topic of systemic and historic injustice which they associated with intergenerational trauma and the ways in which it could undermine hope and trust, a principle of trauma and violence-informed care. One social work supervisor, Kelly, stated that she did not believe all professionals understood the legacy of racism. She said, “I think intergenerational trauma. I think marginalized and systemic racism. These are all major issues in my practice that not everybody gets.” However, responses from several other social work service providers indicated they did understand how the insidious effects of trauma impacted the delivery of services. For example, in a rural focus group discussion, it was noted that intergenerational trauma underpinned the challenges in establishing a working relationship with Indigenous communities where distrust and suspicion were high. Difficult relationships with the Indigenous population that do reach out for services on reserve. A lot that don't. So, we get I guess a lot of intergenerational trauma and presenting trauma. That it's a population of the whole area of Cape Breton that don't really go out and reach out for services in their own communities for security…for trauma reasons, right. (Rural Focus Group 1, Rachel)
These comments underscore the need for social workers to be attune to historical and current influences of colonialism and the need for culturally responsive services. Research participants acknowledged the mental distress resulting from intergenerational trauma and the potential ripple effect on parenting that could result, in what one social worker provider Lori described as, “attachment wounds.” Research participants also indicated that often the initial reasons for intervention were later recognized by social workers as surface issues and that there were other issues, often connected to past trauma that were later disclosed. Inseparable from experiences of trauma, was often the lack of opportunities and resources that compounded a sense of oppression and marginalization. The complexity of addiction work was also noted in the findings as linked to histories of intergenerational trauma that could include experiences of childhood adversity and domestic violence that were compounded by the cumulative oppressive impacts of poverty and discrimination. Such information can sometimes precipitate feelings of powerlessness as social workers are provided a window to personal histories often threaded by intergenerational trauma and marginalization as noted by Elaine, a social work supervisor. A recognition of the cumulative impact of poverty, lack of access to resources and opportunities and social workers’ inability to fully meet the needs of individuals and families can contribute to their feelings of inadequacy. And so we kind of abandon people to these very complex cases. And even if you’re doing good work with them, they’re very eroding to the soul. You know what I mean? Some of these stories, it's like cycles of trauma, right. And even when it's not clearly that, it takes its toll on people. It's very hard, especially in smaller communities. You know, where my staff will say to me, “Oh, we saw their mom too when she was a kid.” Like the cycle is hard. (Social Work Supervisor, Elaine)
Interruption of these cycles must go beyond work with individuals as such stories should be linked to advocacy and community development efforts. Concern about social injustice is often the first motivation that motivates people to enter the profession of social work and it is perhaps the inability to link their professional work with a social justice mandate that “erodes the soul.”
Limitations of a medical model
Throughout the findings, social workers reported that they felt very constrained working within a medical model. The assessment shortcomings of the Diagnostic Statistical Manual (DSM-V) were identified in relation to trauma issues as was the need for additional advocacy for those who experienced marginalization. While there is a usefulness of the DSM …complete reliance on this has found clients needing mental health services coming into my counselling space due to rejection only to have referrals done over again by myself or in collaboration with their medical doctors (if they have one) due to our concerns which are then finally recognized as client-based needs and they are accepted for assistance. (Social Work Provider, Opinio Survey Participant)
The expectation that social workers practice within a bio-medical model often does not fit well with anti-oppressive training.
The research findings indicated some social work providers believed mental health and addiction settings were not client or trauma-based and that they were prevented from offering trauma therapies. These experiences contributed to a dissonance resulting from an inability to be responsive in ways aligned with social work training and practice.
Repositioning social work practice to lead responses to trauma
While social workers need to keep abreast of the ways in which trauma can negatively impact an individual's ability to cope, their profession dictates attention be paid to the “social.” As social work provider Karen noted, “the roots of trauma are in our society, are in our social organization.” This understanding has long been embedded in social work knowledge. Bessie Touzel (1904–1997) an influential social worker, feminist pioneer, and champion of universal rights advocated for a politicized approach to social work practice to recognize the structural implications of social problems with her key message to value the “social” in social work (Johnstone, 2015). Structural inequities were noted by social workers as contributing to a stressed environment with cumulative impacts on individuals and families. For example, an experience of physical violence can occur within a social and family context of physical neglect and poverty. The profession of social work resists a narrow interpretation of family “dysfunction” by understanding the interdependence between individual and society is such that chronic health problems, poor housing, under-employment or unemployment, lack of education, and inadequate childcare affects everyone and creates community problems (Johnstone, 2015). Social worker's knowledge of personal histories including traumatic experiences does not fit well within medical models. The following participant expressed a belief that the profession of social work is positioned to lead change. In order to do really effective trauma-informed care work, we’d have to deconstruct a lot of practices and policies that are going on, and personal values and team values, and organizational values. And that's going to take a long time. … I think social work is well aligned to shift because trauma-informed care aligns very well with social work. (Social Work Supervisor Ann)
The urgent need to reposition social work practice in mental health and addiction to better respond to trauma in community-based settings was noted by participants as a move toward a proactive focus on wellness-based care. One participant suggested if each patient attending a medical clinic was assigned a counselor similarly to the ways in which they were assigned a family doctor they would be able to provide support when needed before their situation escalated to more serious challenges. Such support could include attendance in social group work programs and perhaps contribute to a reduction in stigma experienced by those accessing mental health and addiction services.
Research participants expressed the need to work to their full potential and scope of practice and that the acknowledgment of their provision of trauma-informed care was the way to do that. The social workers we interviewed did not look away from experiences of trauma but instead, in noting its prevalence, discussed the importance of repositioning the profession to better respond.
Discussion
Safety, trust, choice, empowerment and collaboration, the principles of trauma and violence-informed care are supported by values aligned with the profession of social work. These values are rooted in social justice and relational approaches, and are enacted when responding to the question: “what has happened to you?” The biomedical perspective begins differently by exploring “what is wrong with you?”. The integration of a social justice paradigm with biomedical approaches is necessary to the provision of more holistic care. The broad gulf between the two approaches can be bridged by the profession of social work.
Acting on the principles of trauma and violence-informed care the role of social workers could expand to acknowledge, assess, and respond to trauma in holistic ways that move beyond management of immediate symptoms to provide comprehensive healing responses and preventative programs. As the growth in science continues to assert the ways in which childhood adversity impacts our biology (Bethell et al., 2017; Burke Harris, 2018) we need to recognize that by itself brain science is only one component of a bio-psycho-social model pivotal to feminist and narrative therapeutic trauma-based social work practice and structural advocacy (Brown, 2020; Burstow 2003; Levenson, 2017; Tseris, 2013). Biological arguments do not guide existing therapeutic strategies to address the psychological and social pain, suffering, and relational injury that often result from trauma. The social work profession is well positioned to counterbalance connections between biomedical science with resistance to oppressive social and political contexts in responding to trauma. Social workers can assist in identifying and politicizing the vulnerability resulting from social and historical trauma by situating trauma and experiences of violence within a political and social context that moves away from pathologizing the individual to a recognition of the impact of oppressive factors.
As noted in our findings and in recent research, intergenerational trauma must be understood within a social and historical context. Such formulations as evidenced by the work of Bombay, Matheson & Anisman (2014), must include intergenerational impacts of colonialism and systemic racism. Hubl (2020) describes healing from collective trauma as a global responsibility to stop vicious cycles by ultimately integrating and reducing its effects in our global culture. Social workers grapple with these large concepts, recognizing that social injustice and histories of trauma have collective impacts that ripple out across generations and impact individuals, families, and communities.
According to Rush et al. (2008) social workers face unprecedented challenges in effectively responding to trauma-related experiences. They recommend “multifaceted” responses that emphasize the importance of community. This approach acknowledges the ripple effect of trauma on individuals through to communities on the one hand, and from communities back to individuals on the other hand, which necessitates a simultaneous focus on multifaceted interventions. These responses must align with core values of social work—a commitment to social justice and valuing the rights of all people (Baines et al., 2019; Morrow & Weisser, 2012; Pease et al., 2016).
Social justice holds a special place within social work practice, theory, and knowledge. Social work is the only profession with social justice as a central part of its code of ethics (Canadian Association of Social Work Educators, 2005). This code provides a set of foundational values that should inform every interaction, every relationship, every policy, and every aspect of the social work endeavor. However, social justice and “skills” are increasingly set up in opposition to each other, with a narrow instrumental definition of “clinical” social work practices viewed as the only skills needed and separated from a critical clinical approach which embraces social justice principles. However, this mode of practice does not always fit well in a constrained underfunded, neoliberal workplace (Brown, 2016; Baines, 2020). This serves to marginalize social justice social work practices as aspirational and largely unachievable and unaffordable, thereby, perhaps contributing to the internal dissonance experienced among the social workers we interviewed.
Limitations
The authors are committed to critical clinical practice and are registered social workers with “insider knowledge” regarding the breadth and scope of practice that was useful in framing this research. However, their views may not be representative of the views of all social workers in direct practice and this perspective may have influenced who chose to participate in the research. Therefore, the information shared by participants in this study may not be representative of all social workers.
Conclusion
Our findings noted the widespread prevalence of trauma among people accessing mental health and addiction settings and the subsequent need for these services to be trauma responsive. The practitioners we interviewed felt a responsibility to respond in ways aligned with the values of violence and trauma-informed social work practice and believed there were systemic barriers that prevented this type of care. A repositioning of the profession of social work within mental health and addiction settings could empower the full scope of social workers’ practice. Responding to trauma in ways that acknowledge the relational component of people's lives and the social determinants of health is essential as the growth in knowledge about the intergenerational nature of trauma confirms.
A willingness to listen, hear, and validate experiences of childhood adversity, gendered violence, and experiences of adult trauma is central to the relational component of social work practice and the ethical dictate to respect the inherent dignity and worth of persons. We argue that the ethical foundation of the social work profession, which includes the pursuit of social justice, service to humanity and integrity and competence in professional practice, dictates an individual, family, and community response to trauma. Optimal workplace satisfaction and competence is linked to alignment with professional and ethical standards of practice. In this study, social workers recognized the prevalence and importance of working with trauma and identified barriers that interfered with their ability to fully do this work. Repositioning the role of social work within mental health and addiction settings requires innovative change to maximize social work responses to trauma and mobilize prevention efforts. While more research is needed to explore ways in which centering social work responses to trauma will present transformative opportunities in mental health and addiction services, definitive healthcare policy and system change is required to address both prevention efforts and much needed service transformation.
Footnotes
Ethics
This study was approved by the Research Ethics Board at Dalhousie University (REB file # 1025277).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Nova Scotia College of Social Workers (no reference number provided).
Acknowledgments
The authors wish to acknowledge the assistance of Kaitrin Doll in coordination of this research project.
Authors contributions
All authors contributed to the development of the study, conducting focus groups and interviews, coding the texts, engaging in analysis of themes, and writing this article. Dr. Catrina Brown led the overall study.