
Abstract
Young-onset dementia presents unique challenges, including employment disruption, financial strain, and stigma, which affect various aspects of social health, such as social frailty and social isolation. However, little is known about the experiences of people living with young-onset dementia regarding social frailty and social isolation, and support needs to improve their social health. This study aimed to explore the lived experiences and support needs on social frailty and social isolation of people living with young-onset dementia, to inform strategies and interventions to improve social health in this population. A descriptive qualitative design was employed. Semi-structured interviews were conducted with 12 community-dwelling individuals living with young-onset dementia in Ireland and the United Kingdom. Participants had been identified as socially frail, socially pre-frail, or socially isolated in a prior survey. Data were collected from December 2024 to March 2025 and analysed thematically. Five themes were identified: (1) Persevering in independence and voice, highlighting autonomy and being heard; (2) Challenges to stability: employment, finance, and family, describing disruptions and need for family-oriented support; (3) Impact on support: living with young-onset dementia and finding hope, disclosing the social and psychological barriers, and the importance of early and empowering information; (4) Exclusion from inclusion: building a dementia-friendly environment, bridging the need for addressing stigma and advocacy for public awareness; and (5) Gaps: Limited support and challenges, demonstrating age-related and geographic inequalities and sustainability challenges in dementia support access for people living with young-onset dementia. People living with young-onset dementia face significant, distinct and complex social health challenges often not addressed by existing dementia services. Their voices must guide the development of age-appropriate dementia care, with inclusive and empowering support systems. Tailored interventions and policies are needed to address social health needs and promote equity in dementia care for younger populations.
Keywords
Introduction
Any form of dementia diagnosed or with symptom onset before the age 65 is called Young-onset dementia, sometimes referred to as early-onset dementia (Rossor et al., 2010). Globally, approximately 3.9 million individuals aged between 30-60 live with young-onset dementia, accounting for 5-7% of dementia cases (Loi et al., 2023; Prince et al., 2013). Around half a million European residents have young-onset dementia (Hendriks et al., 2021) and over 4,300 Irish residents are estimated to live with young-onset dementia (Pierse, E, & Carney, 2019). People living with young-onset dementia face unique challenges beyond cognitive decline (Millenaar et al., 2017; Oliver et al., 2020), including employment loss (Sakata & Okumura, 2017), financial stress (Sakata & Okumura, 2017) and altered family dynamics (Wiggins et al., 2023), significantly impacting their social health (Vernooij-Dassen & Jeon, 2016).
Social health, reconfigured by Huber et al. (2011), encompasses three dimensions: (1) an individual’s capacity to fulfil their potential and obligations, (2) the ability to maintain some independence despite a medical condition, and (3) the capability to engage in social activities, including work. These dimensions are particularly relevant to dementia and young-onset dementia populations’ daily challenges (Dröes et al., 2017). Social health, viewed as an umbrella concept in the context of dementia (Vernooij-Dassen et al., 2022), includes markers of social frailty (Makizako et al., 2015) and social isolation (Vernooij-Dassen et al., 2022). A recent simultaneous concept analysis comparing social frailty and social isolation in dementia concluded that both involve being alone and limited social activities, engagement, or interactions (Wang et al., 2025). Although there might be a relationship between social frailty and social isolation, social frailty distinctly involves financial difficulty and absence of social resources while social isolation relates to a lack of social networks or social relationships (Wang et al., 2025). For the purposes of this study, social frailty was considered to relate to vulnerability to social isolation (Bunt et al., 2017), whereas social isolation related to actual deficits.
Individuals living with young-onset dementia have different social frailty and social isolation challenges than those living with late-onset dementia. For example, many leave their employment within one year of diagnosis due to impaired performance (Chaplin & Davidson, 2016), resulting in early retirement rates double those of individuals without young-onset dementia (Sakata & Okumura, 2017). Early disconnection from work frequently causes financial stress (Sakata & Okumura, 2017) owing to income loss (Kilty et al., 2023), contributing to social frailty (Li et al., 2023) and affecting social relationships (Ikeuchi et al., 2022). Recent research on dementia and leisure has highlighted how everyday activities can foster social inclusion, belonging, and citizenship among people living with dementia (Fortune & McKeown, 2016; Gray et al., 2023; Motta-Ochoa et al., 2021; Robertson et al., 2020). Leisure can offer individuals opportunities for self-expression and participation beyond medical therapeutic benefits, against stigma and social withdrawal (Gray et al., 2023). For example, community-based initiatives such as the Memory Boosters social club (Fortune & McKeown, 2016), inclusive leisure programmes (Motta-Ochoa et al., 2021), and dementia-friendly walking groups (Robertson et al., 2020) demonstrate how engagement in shared, meaningful activities can strengthen social connections and promote social health. Additionally, younger individuals diagnosed with the condition face more misunderstanding and stigma from peers who believe dementia only affects older adults (Cui et al., 2024a). This can lead to social isolation as friends or colleagues may lack the knowledge and awareness to interact with them (Kohl et al., 2024). People living with young-onset dementia might be less likely to go out, contact people, or use dementia services due to a lack of understanding (Nwadiugwu, 2021) and ineffective support from people around (Sullivan et al., 2022), which can significantly contribute to social frailty and social isolation. In families, individuals living with young-onset dementia move from caregivers or earners to requiring support (Bannon et al., 2021). This role change can challenge their social identity, contributing to social frailty and social isolation (Bannon et al., 2021). Moreover, social frailty and social isolation are associated with an increasing risk of developing and exacerbating dementia (Livingston et al., 2024; Ma et al., 2018) and worsening psychological issues such as depression and anxiety (Ma et al., 2018; Spreadbury & Kipps, 2019).
Despite increasing recognition of the unique challenges facing people living with young-onset dementia, more research is needed concerning their social health experiences and support needs (Aspö et al., 2024). A recent scoping review focusing on the needs of people living with young-onset dementia highlighted that most studies focused on physical and cognitive aspects of young-onset dementia, with limited qualitative studies exploring how social frailty and social isolation affect their social life (Kim et al., 2024). Few countries offer specialised care and support for young-onset dementia, leading to challenges in accessing appropriate dementia services in many health and social care systems (Arvanitakis et al., 2019; Bakker et al., 2022; Cations et al., 2022; (Cui et al., 2024b); (Stamou et al., 2021); Sullivan et al., 2022). For example, while the Netherlands has a well-established care model for people living with young-onset dementia, coordinated by a national centre for knowledge development and dissemination and its regional centres, it does not currently mention the social health component (Bakker et al., 2022). Since 2021, the United Kingdom (UK) has developed young-onset dementia online support service guidelines (Loseto-Gerritzen et al., 2024). In Ireland, until recently, no model of care for dementia (Begley et al., 2023) comprehensively included young-onset dementia support services, and the research was limited to healthcare utilisation (Tan et al., 2019) and employment (Kilty et al., 2023). To meet the specific social health needs of people living with young-onset dementia, universal and equitable access to services is essential (Stamou et al., 2021).
Dedicated care and support services for people living with young-onset dementia are urgently needed, yet remain largely unavailable (Cations et al., 2022). Healthcare services for young-onset dementia population must be carefully considered. However, a significant gap in understanding social health experiences and identifying the support needs of people living with young-onset dementia exists due to limited qualitative research on this (Kim et al., 2024). This gap can hinder the development of tailored interventions, polices, and practices to effectively address young-onset dementia population’s unique social challenges. Moreover, understanding their experiences can help healthcare professionals, caregivers and other stakeholders to better understand and meet the needs of people living with young-onset dementia. This qualitative study aimed to explore social health experiences and support needs of people living with young-onset dementia to improve their social health by listening to the voices and lived experiences from their perspectives. Specifically, the objectives are to (1) explore experiences of social frailty and social isolation of people living with young-onset dementia, (2) identify their social health support needs, and (3) explore barriers and potential strategies to inform development of services tailored to improve social health of people living with young-onset dementia. This study specifically focus on both social frailty and social isolation as they reflect different related dimensions of social health, which can encompass individuals’ capacity and social connectedness.
Method
Study Design
This study adopted a qualitative descriptive design, which aimed to provide a detailed and clear summary of participants’ experiences in their own words (Neergaard et al., 2009; Sandelowski, 2000). Qualitative description is particularly suited to research questions focusing on what people experience and how they describe those experiences, without moving into deep interpretive or theoretical analysis (Colorafi & Evans, 2016). This approach was chosen because the study sought to capture the lived experiences and perceived social health support needs of people living with young-onset dementia in a manner that remains close to their everyday language and realities. The conceptualisation of social health, as defined by Huber et al. (2011), guided all stages of the study, from framing the research questions and developing the interview guide to coding, theme generation, and interpreting findings. The semi-structured interviews (Neergaard et al., 2009) were used to obtain rich, descriptive narration to address the following research questions: (1) What are social health experiences of people living with young-onset dementia? (2) What barriers and facilitators influence their social health? (3) What are their perceived needs of people living with young-onset dementia to improve social health? The reporting was guided by the Consolidated Criteria for Reporting Qualitative Research 32-item checklist (Tong et al., 2007).
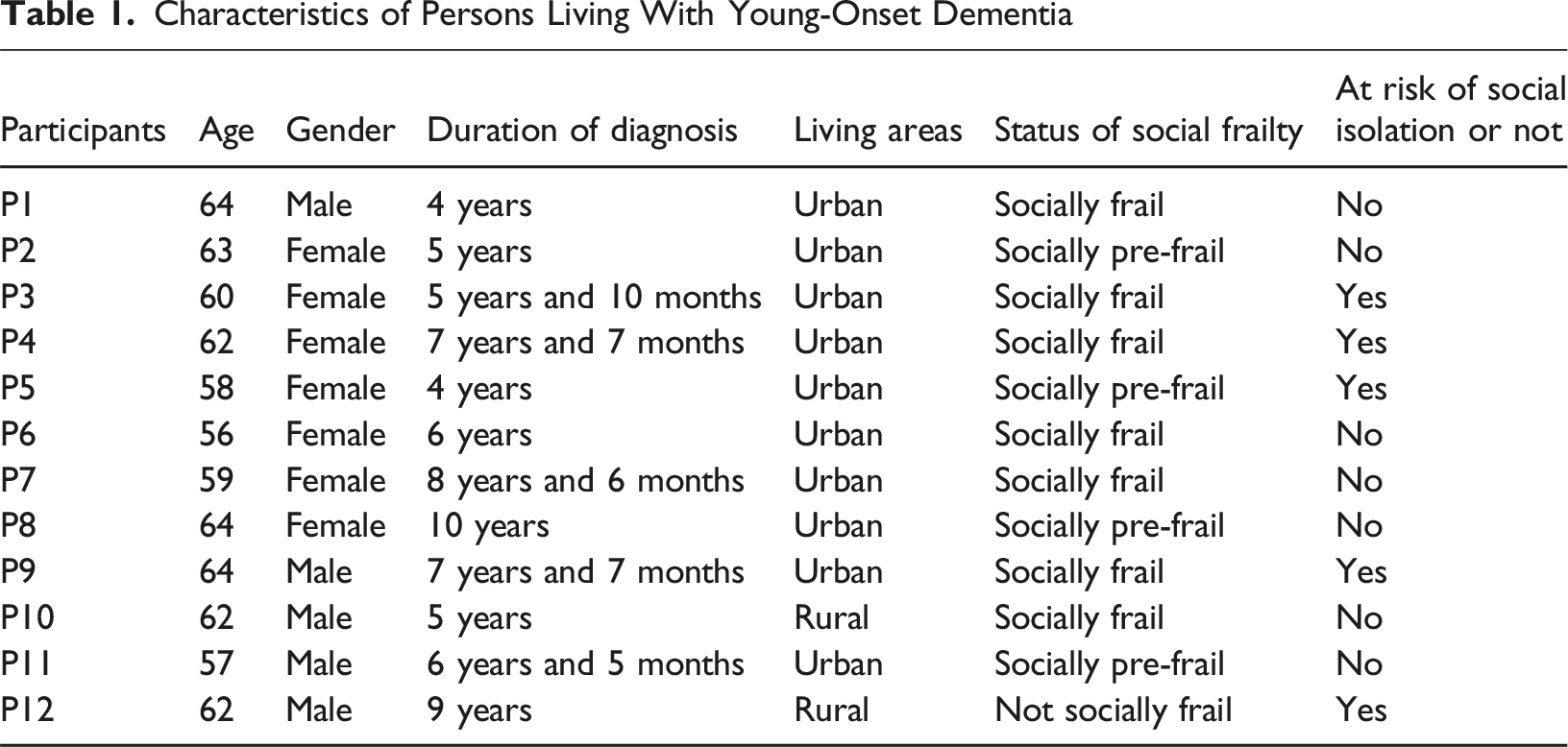
This qualitative study builds on the findings of a cross-sectional study that screened individuals for their social frailty and social isolation status. Socially frail or socially pre-frail persons with young-onset dementia were identified by using a 5-item social frailty questionnaire developed by Makizako et al. (2015), of which, a score of ≥2 indicate social frailty and a score of 1 indicate social pre-frailty. Social isolation screening was conducted by using the Lubben Social Network Scale-6 (Lubben et al., 2006), where participants scoring below 12 were considered as socially isolated. Participants were then invited to further discuss their social health experiences and needs in this qualitative study.
Settings, Participants, and Recruitment
People living with young-onset dementia included in the study were from Ireland and the UK. Eligible participants included those who (1) were socially frail, socially pre-frail, or socially isolated, (2) were younger than 65, (3) had young-onset dementia symptoms or a diagnosis, (4) lived at home, and (5) were able to give informed consent on their own. Those having severe hearing or visual impairment, not socially (pre) frail or isolated, aged 65 or over, not living with young-onset dementia symptoms or diagnosis, not a community-dweller (such as living in a residential care), or unable to give consent were excluded.
The recruitment approach followed purposive sampling (Palinkas et al., 2015), including criterion sampling (Patton, 2002) and snowball sampling (Green & Aarons, 2011). Eligible participants who provided their contact information were invited for in-depth follow-up interviews from the former cross-sectional study (Patton, 2002). The snowball sampling (Green & Aarons, 2011) was employed to recruit participants by asking participants to share this study with others within their social network (Ikeuchi et al., 2022), as it was difficult to find people living with young-onset dementia and few were interested in the research. The participants recruited through snowball sampling also completed the cross-sectional survey phase first. Only eligible participants were included in this qualitative descriptive study.
The Alzheimer Society of Ireland’s research participant recruitment support service, TeamUp for Dementia Research, advocators from Dementia Ireland and community healthcare professionals introduced the study to potentially eligible people living with young-onset dementia. Those interested in participating were informed by the researcher (ZW) about the study through a plain language statement.
Characteristics of Persons Living With Young-Onset Dementia
Data Collection
Data were collected from December 2024 to March 2025 by the first author (ZW). One-to-one interviews with persons living with young-onset dementia were mainly conducted online via Microsoft Teams or by phone considering long travel distances required and participants’ preferences. For those interviewed online, participants and their families received prior instructions on how to join the online call. During interviews, participants could bring a companion person to provide comfort. The interviewer (ZW) had prior experience conducting qualitative interview studies but had no relationship with the participants before the study. Participants were informed that the interviewer is a PhD student conducting the study for an academic qualification. A semi-structured interview guide was developed by the research team (ZW, AH, CG, DS), (Supplemental Material 1). The interviews were piloted by ZW with dementia experts to refine the interview guide before interviewing participants. The pilot data was not analysed. No interviews were repeated. Each interview took approximately 30-60 minutes and was audio-recorded using Microsoft Teams. Notes were also taken to support data analysis. Data collection was finalised when no new ideas emerged in subsequent interviews, indicating that sufficient data had been collected to meet the study’s objectives (Saunders et al., 2018). Interviews were automatically transcribed using a University-licensed Microsoft Teams platform, which complied with institutional and European Union’s General Data Protection Regulation (Regulation, 2016) standards for secure data handling.
Data Analysis
Data analysis was conducted by the research team (ZW, AH, DS). An inductive thematic analysis was conducted in six steps (Braun & Clarke, 2006, 2021). Step 1. Familiarising with the data - Audio recordings were transcribed by Microsoft Teams and then checked by ZW to ensure transcription accuracy. The data were read in detail and re-read as needed to familiarise the researchers with the data. Step 2. Generating initial codes - The data were openly and independently coded using NVivo 20 and MS Word by ZW, AH, and DS, guided by the research questions. All researchers’ codes were compared, and a coding tree was developed. For example, “I’m still me, I’m still capable of taking most information.” was initially coded as “Maintain independence despite the challenges of young-onset dementia”, while “would love some independence” was initially coded as “Valuing/Needs independence in young-onset dementia”. Step 3. Searching for themes - The codes were collated and categorised to form initial themes and then the relevant sub-themes were identified by ZW. They were reviewed, discussed, revised, and agreed by the research team. For instance, initial codes such as “Maintain independence despite challenges of young-onset dementia”, “Needs for flexibility in the young-onset dementia support group”, and “Valuing/Needs independence in young-onset dementia” were merged into the subtheme “Fighting for independence”. Similarly, other initial codes “Cover of young-onset dementia voices due to more focus on carers” and “Value voice form people living with young-onset dementia” were merged into the subtheme “Hear me: speaking for ourselves”. These two subthemes were then merged into the theme as “Holding independence and voice”. Step 4. Reviewing potential themes - Each theme and subtheme were carefully reviewed by the researchers to confirm it appeared in a coherent pattern, reflected the data, and was relevant to the research questions. For example, data coded under the subtheme “Fighting for independence” were checked against the content and description of the subtheme to ensure it reflected the participants’ intended meaning. This code was refined to “Maintain independence” subtheme following discussions by the research team. A thematic map was developed by ZW, which was reviewed by the researchers to ensure the themes’ validity and that they accurately reflected the meaning of the data. Step 5. Defining and naming themes - The themes were further refined, defined, and named through discussion of ZW, AH, CG, and DS. For instance, the quotations and codes in the theme “Holding independence and voice” were then checked and discussed by ZW, AH, CG, and DS. The authors all agreed on naming of “Persevering in independence and voice”. Step 6. Producing the report - The finalised data were ready for reporting, following peer-review.
Ethics Considerations
Ethical approval was obtained from the Research Ethics Committee at the University of Galway (REC ID: 2023.11.023; 2024.08.021). The study’s aims and procedures were explained to all participants in a plain language statement. They were aware that the interviews would be audio-recorded and gave consent before recording. The recordings were destroyed once they had been transcribed and analysed.
All data were anonymised to prevent identification of individuals. To protect the participants from harm or upset on potentially sensitive topics, a distress protocol was developed (Draucker et al., 2009), though it was not needed during the interviews.
Rigour and Reflexivity
Reflexivity is crucial in addressing research bias. The research team had regular reflexivity and review sessions to examine the researcher’s assumptions or potential influences on interpreting findings. A detailed audit trail documented all decisions during data collection and analysis for replication and transparency (Wolf, 2003). For credibility, participants were recruited through gate persons who are healthcare professionals, representatives from Alzheimer organisations, and memory service advisors (Elo & Kyngäs, 2008). Additionally, two Public and Patient Involvement contributors reviewed all processes and the interpretation of the study. Another group of Public and Patient Involvement contributors supported reviewing interview questions and the process prior to the interviews. The researchers accurately reported the viewpoints of persons living with young-onset dementia by closely following the original data. Codes were generated directly from the data, and findings were supported with direct quotations (Naeem et al., 2023). Transferability was addressed by supplying details about the participants, the study context, and findings’ implications. This detailed reporting enables a degree of applicability to similar settings or cultural contexts (Elo & Kyngäs, 2008).
Findings
Five themes with subthemes were identified, presenting the experiences of people living with young-onset dementia on social frailty and social isolation, and their perceived needs. (Figure 1). Collectively, the themes uncovered that people living with young-onset dementia made efforts to maintain independence and identity despite substantial disruptions to their employment, finances, and family life. Participants described significant emotional and social impacts of diagnosis and symptoms, experiences of stigma and exclusion, and unequal access to suitable services. Additionally, they expressed resilience and a strong desire for age-appropriate, inclusive, and sustainable support, as well as a need for improved connection between medical settings, social care and accessible services. These themes and subthemes are detailed below with quotations. All themes and subthemes were supported by data from multiple participants; however, selected quotations were presented to represent the range and depth of perspectives. The map of main themes and subthemes
Theme 1 - Persevering in Independence and Voice
This theme has two subthemes: “Maintaining independence” and “Hear me: speaking for ourselves”. The theme describes key aspects of social health, including how participants wished to maintain their independence and autonomy, and be recognised in their daily lives. They stressed the importance of speaking for themselves and being included in conversations about their care and daily experiences, not being hidden by families or carers. These subthemes reflected a strong sense of autonomy and desire to retain control over one’s life despite cognitive decline and other challenges of living with young-onset dementia.
Maintaining Independence
Despite cognitive or physical challenges, the participants described that they still had the capability to manage daily tasks and make decisions, though some activities became more difficult than before. They stated that they took active efforts to continue their daily routines and highlighted their desire to maintain independence, such as participating in community activities and managing their own affairs, which are essential for social health. Several participants associated autonomy with being able to choose, act, and contribute, rather than being defined by their diagnosis. Maintaining independence allowed them the ability to perform tasks but also as an affirmation of self-reliance and a sense of purpose. “I can still go and walk. I can still be on my own.” (P10) “I'm still me, I'm still capable of taking most information.” (P11)
Hear me: Speaking for Ourselves
Another social health concern presented was how family caregivers’ perspectives often covered the voices and experiences of individuals living with young-onset dementia. Most participants shared that service providers often communicated with their carers instead of them directly. However, participants emphasised the significance of direct interactions with individuals living with young-onset dementia, rather than carers or families, when discussing their experiences, needs, and services. Being listened to and recognised by others symbolised respect and social inclusion, which might be the core components of social health for people living with young-onset dementia. When professionals bypassed them, participants felt invisible and disempowered, which undermined their confidence. Having their voices heard can restore their ability and reinforce their place as active contributors to their care rather than passive care recipients. “They really talk to my wife, not me.” (P11) “Very much listen to our voice. And don't presume what I need or want. Ask me.” (P8)
Theme 2 - Challenges to Stability: Employment, Finance, and Family
This theme has two subthemes: “Employment and associated financial issues” and “Calling for support: employment, financial, and family”. The theme covered participants’ employment disruptions and financial instability, and family role changes. These experiences showed how financial insecurity and shifting family roles can destabilise multiple dimensions of social health, influencing confidence, belonging, and participation. Participants reported a strong need for workplace accommodations, financial assistance, and support for their families, especially for parents with young children.
Employment and Associated Financial Issues
Many participants discussed that they had to leave their jobs or shift their career paths due to the diagnosis, or the cognitive and physical demands of their roles that became unmanageable with the onset of dementia. The early forced exit from employment often led to feelings of frustration, loss of self-worth, and social disconnection. “I changed my work, so I got kind of retired from the work that I was doing.” (P1) “Because you don't work. You've lost all your work colleagues.” (P7)
They, consequently, experienced financial burdens and barriers, including not having access to their pension. Another difficulty presented was managing their limited funds carefully due to living on benefits without income. They highlighted these financial challenges severely restrict their ability to engage in social activities and access necessary services. “So financially, there’re huge issues because I don't have access to the state pension.” (P10) “It costs me 10 pounds or more just to go on that single journey so it can cost 20 pounds or more for me to go into town and back.” (P4)
Calling for Support: Employment, Financial, and Family
They needed structured support on employment challenges post-diagnosis, including guidance on workplace adaptations, legal protections, and potential working positions. In addition to employment-related concerns, financial assistance was needed to access essential care and resources. These needs reflected a desire for security and stability in a period of uncertainty. Without clear advice or a coordinated system of support, participants felt unprepared to plan their lives, which can add their feelings of stress. “more formal advice about being able to keep working or what it's like to have dementia at an early age.” (P10) “Financial support is very important at the beginning for a good circle.” (P4) “We need somebody to step in. Whether it's just some money.” (P7)
Family members, especially partners and young children, were also deeply affected by young-onset dementia and sought support for essential care needs and social health. Participants noted that families require relief and recognition, and parents with young-onset dementia need guidance on communicating with their children about what dementia is, how it might affect the family, and whether it could be inherited. Participants often described these conversations as emotionally complex but necessary for maintaining openness and mutual understanding within the family. Addressing such needs could reduce their anxiety, promote family resilience, and sustain social connectedness. “I had a younger family with children who were of school age. I would have wanted to have some advice about how to have those types of conversations with them.” (P10) “Your family needs to be supported in order that if you have any family then they can continue supporting you.” (P4) “It has taken a load off her shoulders that she actually can go outside for a few moments or to the shop or something without work and worrying about the husband being not all.” (P5)
Theme 3 - Impact on Support: Living with Young-Onset Dementia and Finding Hope
This theme has three subthemes: “Experiencing the impact: social health and psychological challenges”, “Loss to hope: promoting positive information and connection”, and “Left behind: early information and support needed”. The theme highlighted the social and psychological impact of living with young-onset dementia symptoms and diagnosis, from fear and hopelessness to long-term psychological distress, worsened by unmet needs. Participants also described that clear care pathways and early information and support, which could have provided feelings of hope to them, were lacking. The absence of such support often left individuals living with young-onset dementia feeling isolated and uncertain about their future, underscoring how unmet social and information needs can compound psychological distress.
Experiencing the Impact: Social Health and Psychological Challenges
Participants stressed significant challenges in maintaining social health and psychological health due to dementia symptoms, such as physical limitations and challenges with recalling information. Some participants emphasised that young-onset dementia symptoms or diagnosis forced them stop driving and abandon certain hobbies. Many described the psychological consequences of these challenges, including frustration, sadness, and a sense of disconnection from everyday life. Losing the ability to take part in previously valued activities meant losing part of their identity and sense of belonging. “So difficult to hear and difficult to keep up with the conversation (in a pub).” (P1) “I stop driving. Three years ago, my perception is dodgy. I think everything's closer to me, so I can't drive.” (P2) “I'd love to go horse riding. Because I've got an Alzheimer and vascular dementia. They think that I won't be able to remember their instructions and things like that. … the diagnosis has stopped me.” (P7)
Participants described various psychological effects of young-onset dementia. Several highlighted that they had to withdraw from general interactions due to dementia symptoms and a lack of accessible resources leading them to depression. Others reported losing confidence because they had to rely on others for basic activities like crossing the road or travelling. They expressed that dedicated dementia support for younger people was important, but left unaddressed, which made them feel neglected and upset. This declining confidence limited their willingness to engage with others, creating a cycle of withdrawal and social isolation. “When I got Lewy body I lost my confidence.” (P2) “I'm depressed. Thinking of all the things we've not got.” (P7)
Loss to Hope: Promoting Positive Information and Connection
Participants noted how young-onset dementia is typically framed – especially by healthcare professionals and the public – often increase fear and despair. Despite such negative framing and experiences, they stressed that they still tried to stay socially connected. Maintaining social contact was described as an active effort to resist social isolation in daily life. Several participants reflected that most public narratives about young-onset dementia often highlight their challenges rather than guiding them on how to keep living well. Trying to stay connected became an act of defiance and self-preservation, helping them sustain confidence and social identity. “All of those are negative. That it just implies, …, imminent death.” (P10) “We would visit neighbours more and socialise that way. With friends and neighbours, …, but I work hard at not at not getting isolated.” (P12)
Participants expressed that young-onset dementia does not immediately end their ability to live a fulfilling life. They also highlighted a strong desire for providing positive, hopeful and empowering information about living with young-onset dementia, focusing on post-diagnosis life management and adaptability. They viewed accurate and encouraging information as essential for helping newly diagnosed individuals see that a meaningful life remains possible. Promoting hopeful narratives was described as a way to challenge stigma and inspire others, while reaffirming their own sense of value. “To let them know that there’re people my age, I'm 57 now, people my age that have dementia that can live a normal life.” (P11) “It's no good bringing somebody in and said I'm sorry to tell you, but you've got dementia. And they're not sad. You should be - I'm sorry to tell you you've got dementia, but it's OK you can still carry on to other things.” (P9)
Left Behind: Early Information and Support Needed
Many participants described how healthcare professionals often lacked understanding of young-onset dementia and failed to provide basic next steps or connect them to support services, including social support. Several participants said that not receiving clear information immediately after diagnosis caused confusion and distress, making it difficult to plan their next steps or access appropriate services. They expressed they needed the right amount of information or guidance at diagnosis. “But still we have professionals who can't have real problems digesting the fact that you can be younger and have dementia.” (P4) “We left on a Friday evening with the diagnosis and with no information.” (P12)
Many participants reported that the lack of structured support during the diagnosis process or even earlier, when symptoms first appeared, left them feeling lost and unsupported at a hard time. They stated that they needed support and information from the onset of symptoms or diagnosis waiting period. Participants emphasised that receiving guidance earlier could have helped them maintain stability and hope, reducing the fear and uncertainty that often accompany early symptoms. Early information and support also meant they were not alone. “Nobody comes and says to you like, ‘What support do you need?’ Nobody's explaining it to you because you've never had a diagnosis.” (P9) “Early intervention. Early support. That's all it needs.” (P7)
Theme 4 - Exclusion from Inclusion: Building a Dementia-Friendly Environment
This theme has three subthemes: “Experiencing stigma and misunderstanding”, “Efforts for dementia-friendly spaces”, and “Advocacy and raising public awareness for understanding of young-onset dementia”. The theme reports experiences of stigma and misunderstanding from surroundings, contributing to social isolation and social frailty. Almost all participants emphasised that the public was unaware that dementia could affect working-age people. Alongside these challenges, they described their efforts to make the world more dementia-friendly and wanted more public awareness, education, and environmental adaptation to better support individuals living with young-onset dementia.
Experiencing Stigma and Misunderstanding
The majority of participants stated significant stigma and distancing behaviours following their diagnosis among their families, friends, the wider community, and the public. They expressed their frustration and sadness due to others’ limited understanding of young-onset dementia, leading to dismissive attitudes and misconceptions about their condition and capabilities. Many described withdrawing from friends or social situations to avoid embarrassment, noting that these experiences made them feel isolated in turn. Stigma therefore functioned as both interpersonal challenge and a barrier to social participation and wellbeing. “One lady in particular. Had told her that I'd received my diagnosis of dementia, and as soon as I told her, every time she saw me, she used to run back in the house and shut the door.” (P3) “It's about the diagnosis, about kind of how I am or, it's how I feel. But it's also how other people see me.” (P1)
Efforts for Dementia-Friendly Spaces
Despite the barriers they experienced, participants discussed that they actively contributed to campaigns or research to make public environments more accessible and supportive for individuals living with young-onset dementia. They listed their successful efforts, such as adapting public transportation to announce stops clearly for dementia population, simplifying Automatic Teller Machine (ATMs) and supermarket self-service, and promoting the use of the symbols or marks to identify hidden disabilities. These actions reflected participants’ commitment to improving both their own lives and those of others living with young-onset dementia. “Advice or feedback on a service that they offer as to how to make it more dementia-friendly, or to be told it's totally dementia-friendly and how they can change it.” (P8) “I also was reasonably lucky to be involved in the start-up of (a transportation project). …, I spoke at certain things.” (P2)
Advocacy and Raising Public Awareness for Understanding of Young-Onset Dementia
Participants stated their strong needs for young-onset dementia public awareness. Some of them actively promoted young-onset dementia awareness and education through engaging in a wide range of advocacy activities, including public talks, webinars, social media shows, educational outreach, and research. Engaging in advocacy fostered a sense of inclusion and countering the exclusion might have been faced elsewhere. “I work with the University as well, occasionally with their department, chatting to students, just about how to deal with people with early-onset dementia.” (P11) “I'm actually one of the volunteers in it. That is called ‘pathways for young onset dementia’”. (P9) “I did like radio things, video things, just awareness, type things to make people aware of dementia.” (P2)
They stressed that community acceptance and inclusion of young-onset dementia required open conversations and increased visibility of young-onset dementia. Consequently, public education to improve understanding was needed. Participants saw open dialogue or discussion on the topic of young-onset dementia as a key step toward reducing fear and stigma and making communities more inclusive. By speaking out, they hoped to inspire others living with young-onset dementia and to influence how dementia is referenced in daily life. “The more people talk about it, the more people will be able to talk about it, and the more easier it will be for people to accept it. So, getting the word out, getting people talking about it. Not keeping it quiet.” (P2) “The realisation that this is the biggest killer, ..., dementia. We've got to make the general public aware. I want a national wide awareness of young-onset dementia.” (P7)
Theme 5 - Gaps: Limited Support and Challenges
This theme has three subthemes: “Current support is available, but challenging”, “Age and geographical inequalities for dementia services”, “Self-organisation young-onset dementia group and sustainability challenges”. The theme presented that participants often had significant difficulties in accessing and sustaining appropriate services to improve their social life, while some support was available.
Current Support is Available, but Challenging
Some participants reported positive experiences with dementia care and support providers, including dementia advisors, organisations or charities, and peer support groups. Particularly, they stated there were opportunities to share experiences, be understood, and gain practical advice when they were around people with similar diagnoses. For many, peer support was one of the few contexts where they could express themselves freely without fear of judgement. “(Dementia) groups are very helpful. I have other people who are in the same situation.” (P5) “Alzheimer programme, they are fantastic.” (P6) “The dementia advisor gave some support, and they're very supportive...” (P1)
Other participants expressed informal support from partners, friends, and neighbours. However, some lack knowledge of young-onset dementia, leading the informal support being inconsistent or decreasing, and reducing social networks or relationships of people living with young-onset dementia. This unsustained support highlighted how lack of awareness in the community increased social isolation even when goodwill exits around. This reflected a wider challenges of sustaining social health for young people living with dementia. “I lose friends because friends don't know how to deal with it.” (P8) “Families, they don't know how to deal with people with dementia.” (P7) “My next door neighbour, …, whom is absolutely brilliant. He helped me out. And he always stops and takes the time to speak to me.” (P3)
Age and Geographical Inequalities for Dementia Services
Most participants highlighted that dementia services were often designed primarily for older adults with dementia, leaving younger individuals with limited or no suitable support. Some participants described that their young age prevent them from joining dementia peer support groups. Others who could access such groups emphasised that they felt isolated in these settings because the activities were designed for older adults and not suitable for their age. The lack of age-appropriate environments also limited access to support. They expressed a strong desire for services tailored to the needs and social expectations of younger people living with dementia. “I tried joining groups here, but most of the groups around my area are for older people.” (P3) “You need to put people somewhere where they're the same age.” (P9)
Some participants stressed that geographical disparities further restricted access to appropriate dementia care and social support, with such services often available in big cities, not covering their locations. The geographical disparities created unequal opportunities for participation and increased the feeling of being left behind. Some participants reported that they accessed online peer groups. While online contact can provide some connections, the participants highlighted the need for local support and face-to-face events that can offer real-world connections, natural communication and physical expressions of support, such as hugs, which are absent in online interactions. “Mostly in (the capital city), so I don’t go there.” (P6) “If I could have more support, it would be face-to-face meetings with people of my own age.” (P3)
Self-Organisation Young-Onset Dementia Group and Sustainability Challenges
In the absence of formal structures, some participants shared that they run their own support groups to connect and engage people living with young-onset dementia. They expressed; however, that it was very difficult for them to maintain such groups due to challenges related to dementia symptoms. Additionally, lack of funding and withdrawal of national or regional organisations’ challenged these self-organised groups further. “I have tried to get a dementia garden going. But that's what we've had to do on our own. There's nothing out there to help us.” (P7) “They lost the (Alzheimer's Society’s) contract, so … that meant the group was supposed to be finished.” (P9)
Discussion
This qualitative study identified the lived experiences of social frailty and social isolation of people living with young-onset dementia, and their perceived need for social health support. These findings highlighted the distinct and complex nature of social health challenges for people living with young-onset dementia, many of whom were engaged in employment, parenting, and other social roles. Participants described how existing dementia care, which is largely designed for older adults, failed to accommodate their needs. Despite barriers, participants expressed resilience and a strong desire to remain socially connected, advocating for tailored, inclusive and age-appropriate support. Our study findings can inform strategies and interventions to improve the social health of people living with young-onset dementia.
The first theme emphasised the importance of autonomy and including people living with young-onset dementia in conversations about their care. This aligns with previous research on engaging people with dementia in decision-making (Fetherstonhaugh et al., 2013) and ensuring that their voices are heard (Ditton et al., 2025). The loss of independence earlier than necessary was also commonly reported in other studies (Kokorelias et al., 2024), such as having to rely on others for travelling after being diagnosed (Scott et al., 2024). According to Swaffer (2014), people with dementia often felt overlooked or treated as incapable, especially when professionals addressed family carers instead of them. The existing research related to young-onset dementia or dementia generally focused on caregivers’ experiences (Lew et al., 2025) and supporting informal carers (Moyle et al., 2025), rather than the experiences of people living with young-onset dementia (Oldfield, 2021). Our findings contributed to new insights by showing how people living with young-onset dementia desired for their capacities and abilities being recognised, and felt more respected when their views were included in conversations, not expressed by others (Gibson et al., 2024). Many people with dementia are able to actively participate in meaningful conversations, despite memory and communication challenges (Moore & Hollett, 2003). This suggests that healthcare professionals should promote inclusive communication practices and keep the person living with young-onset dementia central in clinical and social care settings. Previous studies have demonstrated that participation in everyday and leisure activities can foster inclusion (Fortune & McKeown, 2016; Gray et al., 2023; Motta-Ochoa et al., 2021; Robertson et al., 2020). However, the findings of our study suggests that social connection for younger people living with dementia requires more than simply having access to leisure. Inclusive support and leisure for people living with young-onset dementia depends on environments that recognise their autonomy and life stage, enabling them to contribute and interact meaningfully. In this sense, our study broadened the understanding of social engagement in dementia by illustrating that, for those living with young-onset dementia, sustaining independence and purpose is an active, often self-driven process rather than a structured recreational activity provided by others.
Consistent with previous research, the second theme highlighted the financial insecurity experienced by people living with young-onset dementia (Mayrhofer et al., 2021), followed by early retirement (Bagnasco et al., 2025; Sakata & Okumura, 2017), family support needs, and addressing changing family roles. Beyond income loss, these challenges affected their personal identity and social participation. Several participants reported ineligibility for pensions or age-related benefits, further increasing disadvantages. Work-related guidance and system navigation support were clearly expressed, mirroring a recent study that emphasises employment protections and social insurance needed to support people living with young-onset dementia (Bagnasco et al., 2025). For example, providing work opportunities suitable to their capabilities or part-time positions can help people living with young-onset dementia socially and financially. Addressing these needs requires action by governments at national policy levels. Families of people living with young-onset dementia are also affected by the consequences of the young-onset dementia diagnosis (Bannon et al., 2021), especially those with young children (Holdsworth & McCabe, 2018). Participants highlighted that existing interventions rarely addressed how to communicate with children about their dementia diagnosis. This suggests that family-oriented support should be included in post-diagnosis care pathways.
Consistent with earlier research reporting withdrawal from activities or interactions (Maters et al., 2025), and loss of confidence (Stamou et al., 2024), participants highlighted that young-onset dementia significantly affected their social health and had a psychological impact on them. Despite this, participants still desired a meaningful life with young-onset dementia. Several participants described receiving their diagnosis with limited or no information on what young-onset dementia meant, what to expect, or what support was available. This absence of guidance left people living with young-onset dementia with negative emotions, a fear of death (Maters et al., 2025) and unsupported. Participants also expressed that clinicians had limited knowledge of dementia (Faulkner et al., 2024) and young-onset dementia (Cations et al., 2022), consequently they had to look for information independently. However, they mostly found negative, stigmatising content or misinformation, not verified by experts. Despite this, our findings added that people living with young-onset dementia still actively sought connections to engage in more activities and desired positive and empowering information, suggesting a direction to reframe how young-onset dementia is perceived publicly. People living with young-onset dementia need the right amount of information and positive support in a timely manner, including at diagnosis and even much earlier when the symptoms first appear. Additionally, healthcare professionals should be specifically trained to provide clear pathways to young-onset dementia care and social support, helping young-onset dementia population to maintain their social health and wellbeing.
Stigma and misunderstanding, feeling dismissed or avoided by others were frequently reported by the participants, echoing previous studies (Maters et al., 2025). Younger people living with dementia might face greater stigma than older adults, partly due to widespread misconceptions that dementia is a disease of older people (Berner et al., 2024). Another challenge is that some countries offer young-onset dementia services as part of disability services (Cations et al., 2022). This approach may improve access but may also inadvertently cause misunderstanding or stigma associated with young-onset dementia. Dementia awareness campaigns, for example, Understand Together in Ireland (Foley & Guiry, 2019), often overlook younger people with dementia. Meanwhile, many participants of our study expressed that they actively advocated for change and awareness, both for improving dementia-friendly services and public education. This builds on previous research findings that people with dementia can engage in system level changes through active research involvement (Oliver et al., 2020). Our findings emphasised that young-onset dementia-targeted advocacy should be resourced and expanded, and that public awareness campaigns must include diverse age groups of people, not only focus on older adults with dementia.
Participants identified significant gaps between current dementia care and their needs, reflecting international research findings that young-onset dementia was often poorly integrated into existing dementia care systems (Arvanitakis et al., 2019; Bakker et al., 2022; Cations et al., 2022; Stamou et al., 2021; Sullivan et al., 2022). For example, in the United States (US) and Ireland, age-restrictions limited people living with young-onset dementia from accessing appropriate services (Arvanitakis et al., 2019; Kilty et al., 2023), forcing them to rely on dementia services intended for older adults (Tan et al., 2019). Our findings also noted geographical disparities in dementia care and support (Donath et al., 2025), with dementia care and support being more accesible in capital cities and urban areas, whereas non-capital citities and rural areas lacked face-to-face opportunities. Research from the UK reported similar resource inequalities, where 20% of people living with young-onset dementia received services from general practitioners and around 16% received no care services (Stamou et al., 2021). In Ireland, dementia care and support were included in the National Dementia Strategy (Hennelly & O'Shea, 2019), but it did not specify targeted services for people living with young-onset dementia. A recent Irish study reported that age restrictions and cognitive impairment prevent people living with young-onset dementia from appropriate healthcare services (Kilty et al., 2023). These age-inappropriate services limited daily and leisure activities that were valuable for maintaining social connection and were often aggravated by financial instability and stigma. Our findings also noted service discontinuity in current dementia care, including sustainability and loss of external organisational support (Cui et al., 2024a). In many cases, people living with young-onset dementia relied on self-organised support networks, but these were difficult to sustain due to dementia-related challenges, lack of structured coordination, and funding support. This suggested an urgent need for policy and system-level investment in sustainable, inclusive, and young-onset dementia-tailored services. To meet specific social health needs of people living young-onset dementia, priorities include age-appropriate peer support, expanded geographical coverage, and increased resources for more young-onset dementia-focused staff and organisations (Stamou et al., 2021).
This study has implications for future practice, policy, and research on young-onset dementia care and support. Interventions must address the unique social health needs of people living with young-onset dementia, including employment, family life, and identity. Additionally, care pathways should be redesigned to include timely, empowering, and the right amount of information, with respect for the autonomy and independence of people living with young-onset dementia. Public awareness and health education should explicitly include young-onset dementia and reflect more positive lived experiences. Future research should co-design interventions with people living with young-onset dementia and evaluate models that integrate social health into dementia care. Policies should prioritise targeted young-onset dementia services that are accessible, sustainable, and inclusive.
Limitations
This study may not fully represent the most socially frail and socially isolated people living with young-onset dementia, as they may have been less likely to participate in interviews. However, the sample was diverse in dementia subtypes, gender, and geographic locations (urban and rural), enriching the perspectives captured. Having participants from two European countries may increase the transferability of findings to other health and social care service contexts. Future studies could develop strategies to engage more socially frail or isolated people living with young-onset dementia in research, to better understand the barriers they face regarding their social health and to inform more inclusive and targeted support strategies for them. Another limitation is that all the participants were older than 50 and had young-onset dementia for several years. Future studies could include younger or newly diagnosed people living with young-onset dementia, and consider approaches to understand their changing experiences and needs over time. Finally, the use of an online communication platform for conducting interviews might be a limitation. While this approach enabled participation from geographically dispersed individuals and ensured convenience during data collection, it also presented some limitations. Online interviews limited the researcher’s ability to observe subtle non-verbal cues such as body language, which might have enriched further contextual understanding. Most participants had their cameras on throughout the interviews, which helped maintain engagement and rapport. Occasional connectivity or audio issues occurred, but were minor and did not affect the completeness of the data.
Conclusion
People living with young-onset dementia seek to maintain independence and get timely and accurate information, despite barriers, such as employment loss, financial strain, stigma, and lack of age-appropriate dementia care. Inadequate information on young-onset dementia and unclear support pathways affect their psychological and social health. People living with young-onset dementia seek connection, advocate for greater understanding, and demand age-appropriate care. They should have access to tailored and dedicated services across health and care systems. Interventions for people living with young-onset dementia should promote autonomy and independence, offer support for families affected by young-onset dementia, and provide timely, right amount of and positive information. Public awareness initiatives should aim to reduce stigma and enhance understanding, and policies must address age and location-based inequalities. Most importantly, the voices of people living with young-onset dementia must guide the development of services and strategies to ensure their rights, needs and experiences are fully recognised.
Supplemental Material
Supplemental Material - Social Health Experiences and Support Needs of People Living With Young-Onset Dementia: A Qualitative Study
Supplemental Material for Social Health Experiences and Support Needs of People Living With Young-Onset Dementia: A Qualitative Study by Ziyue Wang, Andrew Hunter, Carmel Geoghegan, Masood Ahmed Qureshi, Martina Davis, Hayleigh Kicks, Duygu Sezgin in Dementia
Footnotes
Acknowledgments
The authors would like to sincerely thank all the individuals living with young-onset dementia who generously shared their experiences and perspectives on perceived needs for social health in this qualitative study. We also acknowledge the support of the organisations and networks that assisted with participant recruitment in Ireland and the United Kingdom (UK). We are especially grateful for our Patient and Public Involvement (PPI) contributors, Alison McCarthy, member of the Dementia Research Advisory Team, supported by Research Project Officer Cíara O’Reilly from The Alzheimer Society of Ireland, and Martin Roberston, Martyn Colebourne, Tim Little and other members involved in the Alzheimer’s Society’s Young Dementia Thematic Group in the UK, for their openness, time and valuable insights. The study was co-designed with PPI perspectives. The study flyer, information sheet in plain language and interview questions were all reviewed by PPI contributors.
Ethical Consideration
Ethical approval of this study was obtained from the Research Ethics Committee at the University of Galway (REC ID: 2023.11.023; 2024.08.021).
Consent to Participate
All participants provided written informed consent with fully anonymous consent forms prior to participating. All participants provided verbal consent prior to recording during the interview process.
Author contributions
Ziyue Wang: Conceptualisation (lead), Funding Acquisition (lead), Methodology (lead), Project Administration (lead), Writing – Original Draft Preparation (lead), Writing – Review & Editing (equal).
Andrew Hunter: Conceptualisation (equal), Methodology (supporting), Supervision (supporting), Writing – Review & Editing (supporting).
Carmel Geoghegan: Methodology (supporting), Writing – Review & Editing (supporting).
Masood Ahmed Qureshi: Methodology (supporting).
Martina Davis: Methodology (supporting).
Hayleigh Kicks: Methodology (supporting).
Duygu Sezgin: Conceptualisation (equal), Funding Acquisition (supporting), Methodology (supporting), Supervision (lead), Writing – Original Draft Preparation (supporting), Writing – Review & Editing (equal).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by University of Galway - Chinese Scholarship Council Research Scholarship, grant number 202308300025.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
In the ethics application, the authors stated that all data will only be accessed by the data collector and data processors in the research team of this qualitative study. Therefore, the data will not be available unless approval of the amendment is obtained.
Supplemental Material
Supplemental material for this article is available online.