
Abstract
Objectives
This study aims to explore the journey to dementia diagnosis and reaction to the diagnosis from the perspective of people with young-onset dementia living in the community from diverse areas in Australia (metropolitan, regional, rural) and their family caregivers.
Methods
Semi-structured interviews were conducted with community-dwelling people with early to moderate young-onset Alzheimer’s disease (n = 8) or frontotemporal dementia (n = 5) and one person with both Alzheimer’s disease and frontotemporal dementia, and family caregivers of community-dwelling people with young-onset Alzheimer’s disease and/or frontotemporal dementia (n = 28). This study employed interpretive description. Thematic analysis was conducted for emergent themes, comparisons and interplay between themes.
Findings
The journey to the diagnosis is characterised as involving an extensive period of the gradual worsening of symptoms, drawn out investigations, and difficulties facing the prospect of a diagnosis of young-onset dementia. Participants with young-onset dementia struggled to manage their symptoms and the process of seeking a diagnosis was often slow due to difficulties during the course of their medical investigations and feeling reluctance to face the possibility of having dementia. Once participants finally received the diagnosis of young-onset dementia, participants with young-onset dementia and their family caregivers experienced feelings of devastation and shock, in some cases denial and avoidance, and even, confirmation and relief at having received a diagnosis. In some instances, participants experienced more than one of these reactions. There was a profound realisation by participants that a diagnosis of young-onset dementia had serious implications on their life and future.
Conclusion
The journey to diagnosis was found to be a drawn-out process and receiving the diagnosis was a shock for both people with young-onset dementia and their family caregivers. The findings highlight the significance of the role healthcare professionals play in both the diagnostic and post-diagnostic journey, particularly in terms of supporting patients with young-onset dementia and their family caregivers.
Introduction
Young-onset dementia is the onset of symptoms of dementia before the age of 65 years. Internationally, young-onset dementia accounts for up to 9% of all dementia cases (World Health Organisation, 2020). A recent systematic review of 95 studies determined the global prevalence of young-onset dementia to be 119.0 per 100,000 population in the age range of 30–64 years, which equates to 3.9 million people aged 30–64 years living with young-onset dementia across the world (Hendriks et al., 2021). Approximately one person in every 1000 below the age of 65 develops dementia (Alzheimer’s Disease International, 2020). Common types of young-onset dementia include Alzheimer’s disease, frontotemporal dementia, dementia with Lewy bodies, alcohol-related dementia, vascular dementia and medical disorders such as Huntington’s disease and Parkinson’s disease (Rossor et al., 2010).
Young-onset dementia has received growing attention in recent years, particularly in the areas of diagnosis, including timely diagnosis and diagnostic accuracy, and post-diagnostic support (Cations, Loi, et al., 2021; O'Malley et al., 2021a). Timely and accurate diagnose of young-onset dementia is particularly difficult as there is a lack of guidelines available on diagnosing young-onset dementia, there is heterogeneity in its presentation, and it is often misdiagnosed as a psychiatric condition, all of which leads to delays in diagnosis (O'Malley et al., 2019; Ottoboni et al., 2021). It has been found that time to young-onset dementia diagnosis is longer (1) the younger a person is, (2) when more services and specialists are consulted, and (3) for rarer types of dementia (Draper et al., 2016; Loi et al., 2020).
Another key issue faced by those with young-onset dementia is finding post-diagnostic support. People with young-onset dementia often struggle to find appropriate services for their needs as these services primarily cater for those aged 65 years or older (Withall, 2013). A systematic review of age-appropriate services for people with young-onset dementia found that services available for this group are variable, lack structure, and are often offered on a short-term basis due to a lack of longer-term funding (Mayrhofer et al., 2018). Encounters with existing services which are designed for those with late-onset dementia often prompt negative psychological reactions in those with young-onset dementia (Cations et al., 2017). A recent survey of 151 people with young-onset dementia and caregivers of people with young-onset dementia in Australia found that a majority of respondents were against young-onset dementia services being provided by the aged care system and should remain in the disability system (Cations, Day, et al., 2022).
Internationally, there have been multiple qualitative research studies exploring the experience of living with young-onset dementia in the community (Bannon et al., 2022; Busted et al., 2020; Greenwood & Smith, 2016; Rostad & Hellzen, 2013; Thorsen et al., 2020) and the experiences of family members caring for a person with young-onset dementia (Bannon et al., 2022). However, fewer qualitative studies have explored the journey to young-onset dementia diagnosis and reaction to the diagnosis by people with young-onset dementia and their family caregivers (Bruinsma et al., 2020; Thorsen & Johannessen, 2021). Bruinsma et al. (2020) explored the lived experiences and needs of 24 family caregivers of people with young-onset frontotemporal dementia in the Netherlands. The authors investigated the diagnostic process and found that participants experienced delays in seeking help and that healthcare professionals encountered difficulties diagnosing young-onset dementia. Thorsen and Johannessen (2021) explored the experiences of 16 spouses of people with young-onset frontotemporal dementia in Norway in relation to their needs for care and support and characterised receiving a diagnosis of young-onset dementia as a decisive moment involving feeling relief, confirmation, or catastrophic. A limitation of both papers is that they only focus on the experience of family caregivers. In Australia, to date, no study has qualitatively examined the experiences of both people with young-onset dementia and their family caregivers in the community leading up to and following their young-onset dementia diagnosis.
Existing Australian studies on the diagnostic journey of those with young-onset dementia have involved retrospective reviews of clinical data (Draper et al., 2016; Loi et al., 2020, 2021; Withall et al., 2014). For example, one retrospective cohort study examined the predictors of delay to a diagnosis of young-onset dementia and the impact of a specialist young-onset dementia diagnostic service on time to diagnosis for inpatients of a tertiary neuropsychiatry service in one state in Australia. The authors found that the introduction of a specialist young-onset dementia service led to a 12 months decrease in time to diagnosis; factors that contributed to delay in diagnosis were younger age at onset, type of dementia (other than Alzheimer’s disease or behavioural variant frontotemporal dementia), and number of services consulted by the patient (Loi et al., 2020). Another 10-years retrospective cohort study explored demographic and diagnostic characteristics of inpatients admitted to a tertiary neuropsychiatry service in one state in Australia and found that there was a 36% frequency of young-onset dementia over 10 years, with Alzheimer’s disease and frontotemporal dementia being the most common causes of dementia (Loi et al., 2021). Draper et al. (2016) examined the time to young-onset dementia diagnosis by mapping the clinical pathways of 88 patients with young-onset dementia using information from medical record reviews and interviews with patients and their carer. They found that factors that influence time to diagnosis vary depending on the stage of diagnosis. Longer time to dementia diagnosis occurred for those younger at symptom onset, when mild cognitive impairment or depression was present, and in dementias other than Alzheimer’s disease and frontotemporal dementia (Draper et al., 2016). Withall et al. (2014) examined the prevalence and causes of young-onset dementia in one catchment area in eastern Sydney. The limitations of these existing Australian studies are that (1) the participants were recruited from metropolitan memory clinics or hospitals in only one state of Australia (Loi et al.’s two studies were conducted in Victoria; Draper et al. and Withall et al. conducted their studies in New South Wales), (2) all studies employed retrospective examinations of clinical records, and (3) none conducted qualitative explorations enabling rich descriptions of participants’ experiences of their journeys to diagnosis and their reactions to the diagnosis.
The study reported in this paper is part of a larger project that qualitatively explored how people with young-onset dementia who live in the community in Australia, and their families, experienced the diagnosis and made decisions and plans for the future. The focus in this paper is on the journey to diagnosis and subsequent reactions to that diagnosis in order to provide an in-depth understanding of the experience of people with young-onset dementia prior to and soon after their diagnosis that often impacts on the way they interact with their family, care services and others in the community. This paper adds to what is currently known and provides a rich, cohesive account that combines the experiences of both people with young-onset dementia and their family caregivers on the journey to diagnosis and their subsequent reactions. An in-depth understanding of the experience and perception of people living with young-onset dementia and their family caregivers before, during, and soon after the diagnosis of dementia is critical to addressing known gaps in support and services. This includes people living in regional and rural areas who experience lack of access to services; 72% of Australia’s population live in a major city and the remainder live in either regional or rural Australia (Australian Institute of Health and Welfare, 2021). Australians living in such areas are more likely to experience lack of access to healthcare services which delays diagnosis, as well as a lack of access to information on dementia (Dementia Australia, 2020). Therefore, it is imperative to include the experiences of those living in regional and rural areas.
Material and Methods
Study Design
Interpretive description was employed in this study as it is a qualitative inductive analytic approach used in health and applied disciplines to understand clinical phenomena and yield practice implications (Thorne, 2016).
Participants
People with dementia were eligible for inclusion if they lived in community settings in Australia, including in metropolitan, regional and rural locations, and had a diagnosis of Alzheimer’s disease or frontotemporal dementia prior to 65 years of age who, at the time of the recruitment, were in the early to moderate stages of dementia (self-reported). Current family caregivers, aged 16 years and older, of people with early to moderate stage young onset alzheimer’s disease or frontotemporal dementia who live in the community in Australia were also invited to participate. Family caregivers were family members who self-reported that they undertook caregiving activities to assist a person with young-onset dementia. Participants were recruited Australia-wide via community-based young-onset dementia support groups and Dementia Australia (the peak national organisation for dementia in Australia). With some families, more than one family caregiver was interviewed at their request as more than one member of the family was often involved in care for the person with young-onset dementia.
Maximum variation sampling was employed in order to recruit a diverse range of participants and ascertain a broad range of views and experiences. Variations included gender, geographical location and relationship of supporter to the person with young-onset dementia (e.g. spouse/partner, child).
Ethical Considerations
Ethical approval was obtained from the [University of Sydney] Human Research Ethics committee (2017/845). This study followed the guidelines outlined in the National Statement on Ethical Conduct in Human Research (The National Health and Medical Research Council Australian Research Council Universities Australia, 2007), particularly for participants with a cognitive impairment, such as dementia. All participants provided written consent.
Data Collection
The main source of data collection was telephone or in-person semi-structured interviews which commenced in November, 2017 and concluded in December 2018. In line with the aims of the broader research study, the interview guide primarily explored how participants made decisions and plans for the future. However, the interview questions firstly explored, in-depth, each participant’s journey to the diagnosis, reaction to the diagnosis, and their experiences of living with young-onset dementia or caring for someone with young-onset dementia.
Most interviews were conducted with one participant at a time. Five of the interviews with participants with young-onset dementia were conducted in the presence of a family caregiver at the request of the person with young-onset dementia. The family caregiver acted as a support person and only provided prompts and reassurance to the participant with young-onset dementia. The average duration for interviews with participants with young-onset dementia was approximately 50 minutes, and the average duration for interviews with family caregivers was approximately 1 hour and 20 minutes.
Due to a resource limitation, interviews were only conducted in-person if the participant chose a location for the interview to be held within a 25 km radius of the Sydney Central Business District. All interviews outside of this radius were conducted via a video conferencing facility (Zoom, Skype) or telephone. Overall, six interviews were conducted face-to-face, and the remainder over telephone (n = 30) or using an online video conferencing facility (n = 6). Five out of the six interviews conducted face-to-face were conducted at the participant’s home and one was conducted on the university campus.
Participants completed a demographic questionnaire which captured characteristics including age, gender, type and duration of dementia for the person with young-onset dementia and employment status. Family caregiver participants were asked an additional question on how long they had been supporting the person with young-onset dementia.
Data Analysis
Interview transcripts (transcribed verbatim) were uploaded into NVivo (Version 11) for coding and data management (QSR International Pty Ltd, 2018). Thematic analysis was conducted on the interviews for emergent themes and comparisons as well as interplays between the themes (Braun & Clarke, 2006). Initially, an inductive approach was adopted, and codes were created. These codes were then allocated into two main categories that addressed the main objectives: “journey to the diagnosis” and “reaction to the diagnosis”. As part of the analysis process, codes were shifted around and/or merged or separated in order to conceptualise the data, make connections, identify patterns and ultimately develop themes. Simple descriptive statistical analysis was conducted on the demographic characteristic data using Microsoft Excel (Microsoft Corporation, 2018).
Findings
Descriptive Characteristics of the Participants.
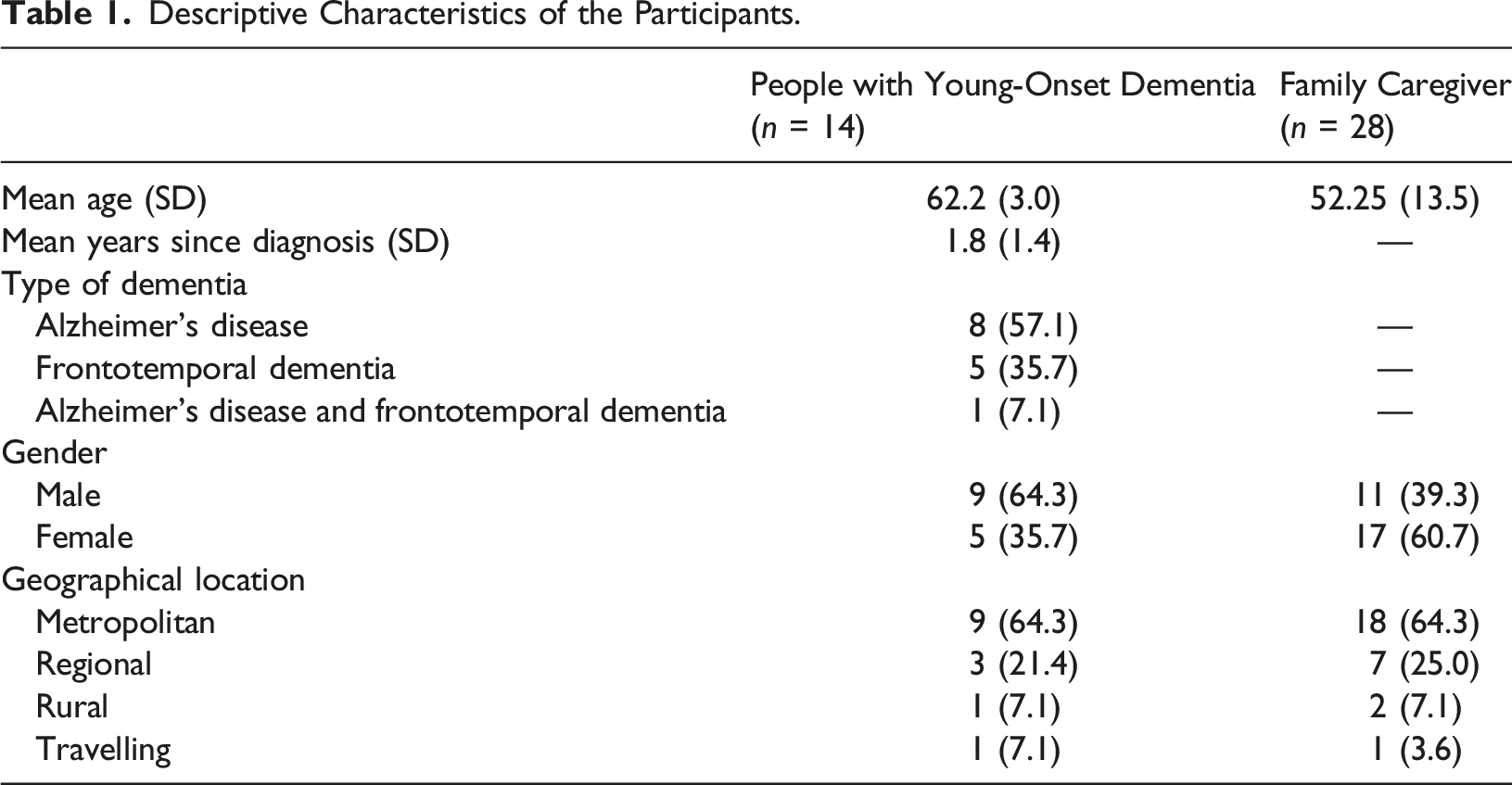
Participants with young-onset dementia ranged from 56 to 65 years old at the time of interview. The mean self-reported age of onset of dementia was 61 years (SD = 3.05 years). All but one lived at home with their family. At the time of interview, none were in paid employment; in fact, all but three participants with young-onset dementia retired after receiving their diagnosis. Family caregivers, at the time of their interview, had been supporting the person with young-onset dementia for an average of 3 years (SD = 1.6 years). Their ages ranged from 19 to 71 years old. An equal number of family caregivers worked full-time or were not in paid employment (n = 10 each), five worked in casual employment, and three worked part-time.
For the dyad and triads who participated, the approach of creating one cohesive account was adopted as the data from their interviews indicated a strong interconnection of experiences. Therefore, the findings in this paper are presented as one cohesive narrative that is not separated by participant type (i.e., person with young-onset dementia and family member).
The journey to the diagnosis is characterised by the overarching theme “A painful and prolonged journey to diagnosis”, which consists of the sub-themes: (1) Dementia: a difficult word to face and (2) Challenges with a first point of contact and waiting time. The reaction to the diagnosis is characterised by the overarching theme “The life that I have known is changed forever”, which consists of the sub-themes (1) Devastation and shock, (2) Denial, avoidance and self-stigmatisation, and (3) Confirmation and relief.
A Painful and Prolonged Journey to Diagnosis
Many participants reported that the person with young-onset dementia struggled to live with the symptoms of dementia and seeking help for the symptoms was often a slow process due to reluctance to face the possibility of having dementia and encountering difficulties investigating the symptoms.
‘Dementia’: a Difficult Word to Face
In this study, the journey to the diagnosis for many began with the person with young-onset dementia experiencing symptoms of dementia in daily living, in particular, at their workplace and when driving. The most common symptoms experienced by participants with young-onset dementia, as reported by the participants, were memory problems such as forgetfulness, decreased comprehension ability, difficulty speaking and/or writing, and self-perceived changes in personality. All 25 participants with young-onset dementia featured in this study experienced at least two or more of these symptoms. Work performance was also often compromised by these symptoms, for example, an inability to process information or to plan and execute actions, as well as struggling with tasks previously completed with ease. Participants reported that these symptoms gradually worsened and increasingly affected the daily lives of the participants until the symptoms could no longer be ignored, explained away, or hidden. Participants said that this prompted them to seek medical help.
One person with young-onset dementia spoke of his struggle to carry out his work duties as a handyman (Box 1, Quote 1); another participant, who worked as a legal professional, was making noticeable mistakes at work (Box 1, Quote 2). Some family caregivers recounted how, when driving, their relative with young-onset dementia made poor driving decisions, drove erratically or were unable to recall usual driving routes. Other symptoms included loss of motivation, social disengagement, and trouble speaking and articulating.
Some family caregivers reported the person with young-onset dementia responded slowly to the symptoms and tried to justify, deny, hide, or disguise the changes (Box 1, Quote 3 and 4). They said many with young-onset dementia were reluctant to seek help or did not want to give up hope that the problems were caused by something less serious or attributed them to events in their personal life or other conditions such as stress or depression. A number of family caregivers talked about their struggle to convince the person with young-onset dementia to see a doctor to investigate their symptoms as some people with young-onset dementia reacted defensively. One spouse/partner compared raising their concerns with the person with young-onset dementia with “standing in front of a firing squad” (FYOD7) as the person with young-onset dementia would react with anger and denial. One person with young-onset dementia suspected their symptoms related to dementia but resisted confirming this diagnosis as their mother also had young-onset dementia, which was an experience they associated with sorrow and pain. Seven family caregivers of seven people with young-onset dementia reported that the person with young-onset dementia was reluctant to investigate or seek help for their symptoms.
Many participants with young-onset dementia and their family caregivers confessed that the difficulties in daily living they faced were often a source of frustration and even fear. They feared that the person with young-onset dementia’s personality and behaviour would change. One spouse/partner described it as a “fear that you’re going to lose the person that you knew that you loved, that have supported, and to change into a whole completely different person” (FYOD8). Some family caregivers reflected that they did not want to face the possibility of bad news about the person with young-onset dementia and be confronted with their worst fears. One spouse/partner said that he had sensed that the cause was serious but was not ready to “toss the towel in or see that it was perhaps what it turned out to be” (FYOD5).
Quote 1: It was more about forgetting and getting instructions mixed up - even simple instructions that I knew... Not all the time but mostly just situations where you would be asked to do a task... In the first instance after being told, I used to get the wrong message and I would get - that had probably been going on for about 3 or more years and it got to the point where it was getting embarrassing. So I would just walk off and if I worked it out, I worked it out. If I didn’t, I would make a phone call and get away with it. That was the main sort of start of it. (PYOD10, male, late 50s) Quote 2: I started to sense that I was forgetting things or missing out on things or not fully following some things and a couple of my clients mentioned things to me and it was more other people mentioning than me personally realising. Then, I thought I’ll go and investigate it. (PYOD14, male, mid 60s) Quote 3: I found a copy of piece of paper of her practising how to spell simple words like “girl”. And she couldn’t get it right. All the letters were the wrong way around. And writing numbers, like “21”. She couldn’t put the 2 and 1 together... I really got behind the 8 ball and said “we’ve got to go and see the GP [general practitioner].” And that’s when I found out at the interview - the GP looked at his computer and he said “you haven’t been back to see the neurologist to complete your testing.” And I didn’t know that she’d been to see the neurologist. She kept it quiet. What actually happened was that during the process of the testing with the neurologist, she realised she was failing cognitive assessment 101 and it didn’t sit very well with her so she didn’t go back. We lost about 18 months altogether. (FYOD21, spouse/partner, male, late 60s) Quote 4: He was having issues remembering to do things and he didn’t tell me about it. He kept that to himself. He didn’t tell me about it. So that’s when he first noticed it but he didn’t say anything to me for a couple of years after that. I was just thinking that he was a little bit forgetful at times. (FYOD6, spouse/partner, female, mid 50s)Box 1. Exemplars for ‘Dementia’: a Difficult Word to Face
Challenges With a First Point of Contact and Waiting Time
All participants reported that the diagnostic process involved a series of investigations and consultations with healthcare professionals and was often a long process. In Quote 1 of Box 2, a spouse recalled her difficult experience obtaining her husband’s diagnosis whilst managing her husband’s increasingly difficult behaviour, including some physical violence towards her. She recounted that healthcare professionals attributed her husband’s symptoms to other conditions or issues in the couple’s relationship which delayed the diagnosis. Her overall experience at the time was so distressing that she fell seriously ill and reached out for help to her general practitioner when at breaking point.
Participants reported that the general practitioner was the first point of contact for a majority of participants in their investigations (n = 16 cases of young-onset dementia) and they conducted basic diagnostic testing, such as administering the Mini Mental State Examination (MMSE) or ordering imaging tests. Two participants, one person with young-onset dementia and one family caregiver, explained that their general practitioner was instrumental in moving the diagnosis process along. Some family caregivers, through their own persistence, said they were able to facilitate the diagnosis process with the general practitioner. However, several participants recounted difficulty trying to convince their general practitioner that the symptoms warranted investigation. For example, a daughter of a person with young-onset dementia said that their mother’s general practitioner reportedly attributed her memory issues to the normal ageing process (Box 2, Quote 2). She expressed her shock and dismay that her concerns regarding her mother’s condition were being dismissed by her mother’s general practitioner despite pleas from herself and her sister. In another example, a spouse/partner described how her husband’s general practitioner was flippant about his memory loss and normalised it as part of ageing (Box 2, Quote 3).
After first contact with the general practitioner was made, participants said they were often referred to a specialist, particularly a neurologist, for further investigation and diagnosis. It was not uncommon for participants to report encountering multiple healthcare professionals in the journey to the diagnosis. According to participants, many general practitioners often referred the person with young-onset dementia onto memory clinics, psychologists, neurologists, mental health services, psychiatrists, and geriatricians.
The journey to diagnosis was experienced by participants to be prolonged for some due to being misdiagnosed with other conditions, only for later testing to reveal dementia. Most participants reported that the investigations lasted at least a year, with an average length of approximately 21.5 months (n = 16 cases of young-onset dementia). Many participants from rural and regional areas faced lengthy intervals in between appointments to access specialists, with some also making trips into metropolitan areas. The waiting in-between appointments was a source of anxiety for all participants. One person with young-onset dementia, a former public servant with Alzheimer’s disease, who lived in a regional area, required medication to cope with his feelings of anxiety (Box 2, Quote 4). It was also not uncommon for the person with young-onset dementia to develop further symptoms or for their existing symptoms to worsen during the process of diagnosis, which further inflamed feelings of anxiety, frustration and desperation (Box 2, Quote 5).
Quote 1: So we went to a doctor and the doctor did the little test. “Oh yeah, no, nothing really.” Then we went back again and they said “depression.”... So then we went to a neurologist at *Hospital. She said he was an alcoholic and I was in denial... I went to my doctor and she wasn’t there and I saw another one and she said “how’s your life?” and I just started crying. She said “maybe he’s got alcoholic dementia.” So I read up on it and there was a number you could ring and I went and spoke to someone at Dementia Australia for an hour. She said to me “go back to your doctor and get a referral to *Dementia Clinic.” That took 8 months and he was diagnosed with behavioural FTD [frontotemporal dementia]. They gave us a letter, told us “you’ve got 5–10 years to live, go to your GP.” (FYOD10, spouse/partner, female, late 50s). Quote 2: My sister and I went to the doctor ourselves - to mum’s normal doctor to talk to him about what we should do and what he thought what process we should follow because of her reluctance to actually attend the doctor… He dismissed our concerns…We were very upset and told him what we thought it…just being on the internet, you have all the information at your fingertips and using reliable sources like Dementia Australia and sources like that. We had kind of almost thought at the time that it was probably the one cause - frontotemporal. He was very dismissive of our thoughts. Georgie went back again and demanded and asked for an MRI. (FYOD14, daughter, mid 30s) Quote 3: He had been complaining and concerned about his memory for a couple of years prior to - and he had been to the GP and I think he had been so far as to have a MRI on his brain and the GP was quite flippant, initially saying “as we get older, we all can’t remember people’s names.” (FYOD27, spouse/partner, female, early 50s) Quote 4: It seemed to be a longwinded process…But you had to basically be very patient... I mean, I guess when you know that something’s wrong and you want to find out what it is, you get a bit anxious about it. Well, I did. And I think most people would in my situation… It just seemed to take a long time to get rolling…I knew that I had to do a number of tests before they made their final diagnosis. At one level I thought “yeah yeah OK, that’s the way it is.” But the other part of me, the scared part of me, thought “oh you know, this seems to be taking so long.” And I did have to take - it got to the stage where I did have to take some medication for anxiety because it was really stressing me out because of long gaps between appointments. (PYOD3, male, mid 50s) Quote 5: He [neurologist] went through and did a very intense kind of testing and judging how he reacted and did things. He said at the time that he thought it was probably frontotemporal lobe dementia but equally possibly could be something else. He suggested we could go back in 12 months and he would reassess, which we did. There was a decline. So his ability to speak was less – a lot of the testing was no longer carried out when he returned to the neurologist. He just wasn’t able to do a lot of the speaking answers or the mental... pointing and completing any of the requests. (FYOD23, spouse/partner, female, late 50s)Box 2. Exemplars for Challenges with a First Point of Contact and Waiting Time
“The Life that I have Known is Changed Forever”
The reaction to the diagnosis of young-onset dementia by participants is captured by the theme “The life that I have known is changed forever” which is characterised by the sub-themes (1) Devastation and shock, (2) Denial, avoidance and self-stigmatisation, and (3) Confirmation and relief. In some instances, participants experienced more than one of these reactions.
Medical specialists were cited by people with young-onset dementia and family caregivers as the most common source of diagnosis (20 cases of young-onset dementia). The most common type of specialists were neurologists, followed by geriatricians and psychiatrists. Very few general practitioners diagnosed the person with young-onset dementia.
Devastation and Shock
The primary reaction most participants reported having in response to the diagnosis was shock and devastation (Box 3, Quote 1). Their shock primarily stemmed from the person with young-onset dementia being diagnosed with a condition often seen in older people. To be diagnosed with dementia at a comparatively young age was unexpected for most participants (Box 3, Quote 2). Many believed that their symptoms would be attributed to issues in their life, due to the person with young-onset dementia’s relatively young age, such as depression, stress, and even alcoholism.
Shock was also experienced by most participants as they came to the realisation that their life would now change and they considered the implications of the diagnosis. The diagnosis was a catalyst for some participants with young-onset dementia to retire, ending decades long careers. In fact, all participants with young-onset dementia who were interviewed were no longer in employment at the time of their interview. One person with young-onset dementia was unable to cope with his diagnosis and in his despair attempted suicide in response to the news. The person with young-onset dementia’s distress at the diagnosis and the thought of his future with dementia was so great that he drove his car into a lake but changed his mind and swam out.
Some participants also reported feeling devastated by the diagnosis as they thought of the terminal nature of the disease, including thoughts of the end stage and what that would entail, as well as their future in a residential aged care home (Box 3, Quote 3). In a few cases, participants said they asked the diagnosing healthcare professional in the same consultation when receiving the diagnosis about how long the person with young-onset dementia had left to live (Box 3, Quote 4).
Quote 1: All I can think of is “well... the life that I have known is changed forever.” That’s a huge thing for anyone to contemplate. Most of us had to do something in our life at times when circumstances change. But this sort of came out of the left field really. (PYOD3, male, mid 50s) Quote 2: It was really suddenly, devastatingly horrible. We had no idea at all… No, I did not suspect that. Not at 58. Thought it might be a memory - oh no, not really memory. Stress-related. Depression. More something like that. Not dementia. (FYOD20, spouse/partner, female, early 60s) Quote 3: When she was first diagnosed, she said “I don’t want to be in an aged care home. I don’t want to be in a home.” [There were] two things - she said to the doctor “how long have I got to live?” and… she said just to me “I don’t want to be in a home.” (FYOD9, brother, early 70s) Quote 4: For me it was probably overwhelming because at that point I think I completely jumped to the end state - at his death…I’ve known people who have dementia and Alzheimer’s and that starts going in your mind. You basically jump to that and then I said to the neurologist, “what’s the worst-case scenario?” And she said “5–7 years” (FYOD3, spouse/partner, male, early 40s)Box 3. Exemplars for Devastation and Shock
Denial, Avoidance and Self-Stigmatisation
As well as shock, another common reaction to the diagnosis witnessed by family caregivers in their loved one with young-onset dementia was denial and avoidance. Seven family caregivers, all of whom participated as lone participants reported that their loved one’s denial of their diagnosis made it difficult to talk with them about any situation associated with dementia, even the invitation to participate in this study. Dementia was a taboo topic in such households (Box 4, Quote 1). In fact, these family caregivers participated in the study alone as the person with young-onset dementia did not want to be interviewed to talk about their diagnosis.
One reason cited by these family caregivers for people with young-onset dementia to avoid discussing their diagnosis, or for denying their diagnosis, included feeling stigmatised by having dementia which they perceived to be a mental illness and a degenerative condition. These family caregivers believed their loved one with young-onset dementia feared that their condition was deteriorating and that it would be too confronting to accept and/or to disclose to others (Box 4, Quote 2). These family caregivers reflected that the person with young-onset dementia found their dementia to be socially unacceptable.
Another reason, according to a few family caregivers, for people with young-onset dementia to deny their diagnosis was resistance to accepting that their life was changed forever and that they would now be dependent on others (Box 4, Quote 3). The prospect of the independence they enjoyed and valued diminishing over time was one too difficult to accept and confront. To cope with this, some participants with young-onset dementia ignored and refused to acknowledge their diagnosis.
Quote 1: [Person with young-onset dementia’s] maybe just ignoring it … she’s never spoken about it [diagnosis] with me or with my sister. It’s almost like it’s a taboo topic. She knows she’s got a bad memory but she kind of fobs it off as if she kind of doesn’t like to talk to us about it. (FYOD24, daughter, mid 30s) Quote 2: She was, excuse my French, she was p***** off. She was floored. She never thought that he [doctor] would say she had dementia. I guess she had spent a lot of her time researching what possible - even though dementia is a physical illness - what possible physical illnesses that would be accepted by society that she may have to justify why she was having all these symptoms... she’s old school. Like dementia means you’ve lost your marbles, that you’re going crazy… In her era, it used to be called childlike or childish. That you reverted back to being a baby. It was never a good thing. It was seen more as a mental illness as opposed to a physical illness…It would be easier for her to say, “I’ve got a brain cancer” than “my brain’s dying, the cells are dying off.” (FYOD25, daughter, late 30s) Quote 3: She [person with young-onset dementia] didn’t like the fact that her life was being taken over by me or the family trying to assist her in this difficult road. There was a lot of angst and denial and to this day she’s still in denial that she has that disease or condition. (FYOD22, spouse/partner, male, early 60s)Box 4. Exemplars for Denial, Avoidance and Self-Stigmatisation
Confirmation and Relief
The diagnosis was a confirmation for some participants that their concerns, suspicions, and for some, fears, were well-founded. It was not uncommon for participants to admit in their interviews, particularly family caregivers, to searching online for the symptoms of the person with young-onset dementia and discuss them with other family caregivers and friends to try and identify the possible cause. Once they received the official diagnosis of young-onset dementia, it made sense to these participants, and it did not come as a surprise (Box 5, Quote 1).
For some participants, the diagnosis of young-onset dementia came as a relief as they had an explanation for the changes in the person with young-onset dementia (Box 5, Quote 2 and 3). Those participants had endured several years of living with the symptoms or caring for their loved one, as well as the subsequent longwinded process of investigating the symptoms without a diagnosis, and even not being taken seriously by healthcare professionals. Receiving a diagnosis came as a relief for these participants as it ended the suspense and uncertainty, and it enabled them to move forward and start planning for life with dementia or caring for their loved one with dementia.
Quote 1: It didn’t shock me 100% because I knew something was wrong… It just made so much sense, as much as it was a shock. It made so much sense. (PYOD10, male, late 50s) Quote 2: He was finally diagnosed with younger onset dementia, which to me was a relief in a way because I knew it wasn’t something else. It wasn’t depression or anything like that because he’s normally happy - he’s not the depressed sort of quiet person. So once we sort of knew it was coming - the diagnosis - it wasn’t a huge shock. (FYOD4, spouse/partner, female, late 50s) Quote 3: I was quite happy at the time because I had an explanation for what was going on which was better than not knowing... Having a definitive answer was a lot better than, you know, being told I was wasting people’s time. (PYOD8, male, early 60s)Box 5. Exemplars for Confirmation and Relief
Discussion
This is one of the first qualitative studies to explore the perspectives of both the person with young-onset dementia and their family caregivers on the journey to diagnosis and their subsequent reactions, thus creating a rich cohesive narrative of their – often shared – experiences. Overall, the journey to diagnosis was experienced as a slow, long and painful process. For many, it took years for their dementia to be diagnosed while their symptoms worsened. Some participants were reluctant to pursue investigations and attributed the symptoms to other conditions until they could no longer be ignored. When help was sought, investigations were often prolonged, and misdiagnosis was not uncommon. Participants were shocked by the diagnosis and the magnitude of the implications on their life and future. Some people with young-onset dementia were in denial and avoided discussing their diagnosis. Relief and feelings of confirmation were also felt as their suspicions were validated, and they were now able to plan their life with young-onset dementia or caring for their loved one with young-onset dementia.
The slow, troubling journey to diagnosis identified in this study has been commonly reported in the young-onset dementia literature (Draper et al., 2016; Kilty et al., 2019; O'Malley et al., 2021a; Spreadbury & Kipps, 2019; Wawrziczny et al., 2016). One study has found that, on average, people with young-onset dementia waited 4.4 years from symptom onset until diagnosis, compared with 1.3 years among people with late-onset dementia (Novek et al., 2016). Another study also found that their cohort of participants with young-onset dementia waited, on average, 4.4 years from symptom onset until diagnosis, whereas those with late-onset dementia waited, on average, 2.8 years to receive their diagnosis (Van Vliet et al., 2013).
One study of 242 patients with young-onset dementia in Australia found that the younger the person was, the longer it took for them to receive a diagnosis of young-onset dementia (Loi et al., 2020). Seeking a diagnosis is also made more difficult when the person with young-onset dementia is in denial about their decline or lacks insight into their decline or symptoms (Bruinsma et al., 2020; Rabanal et al., 2018). This leads to delays in seeking help whereby people with young-onset dementia and their family caregivers manage the symptoms until they can no longer cope, at which point they then seek advice. Furthermore, it has been found that those with frontotemporal dementia are reported to have increased time from symptom onset to obtaining their diagnosis, when compared with those with Alzheimer’s disease (Van Vliet et al., 2013).
Many people with young-onset dementia experience challenges when trying to obtain a formal diagnosis, particularly as they appear too young to have dementia and tend to appear physically well, which can contribute to healthcare professionals dismissing their concerns or misdiagnosing them (Harris, 2004; O'Malley et al., 2021b; Rabanal et al., 2018). They do not fit the typical image of what most people envision a person with dementia to be as they are relatively young (Clemerson et al., 2014). Instead, their symptoms are often attributed to stress, depression, or marital problems (Bruinsma et al., 2020), or as found by this study, alcoholism. Spreadbury & Kipps (2019) interviewed six healthcare professionals on their views of the issues they encountered along the young-onset dementia care pathway. They explained that they encountered much uncertainty when making a diagnosis of young-onset dementia, particularly the method of establishing a diagnosis including which tests or scans to order and how to manage inconclusive results.
This study suggests that many people with young-onset dementia may not be diagnosed in a timely manner. As participants explained, the diagnostic process is prolonged, involving consultations with a number of different healthcare professionals, numerous investigations and tests, and even, for some, misdiagnosis. Young-onset dementia is heterogeneous in its presentation, and is often misdiagnosed (O'Malley et al., 2019). Developing the professional understanding of young-onset dementia and establishing pathways to care for diagnosis will also contribute to ensuring timely diagnosis of young-onset dementia (Cations, Loi, et al., 2021). Key to this should be the establishment of guidelines on diagnosing young-onset dementia to guide healthcare professionals (O'Malley et al., 2019).
Reactions to the young-onset dementia diagnosis experienced by the participants in this study included shock, devastation, denial, avoidance, or relief. These have also been identified in the literature as common reactions in response to a diagnosis of young-onset dementia (Bannon et al., 2022; Spreadbury & Kipps, 2019; Thorsen & Johannessen, 2021; Wawrziczny et al., 2016). People with young-onset dementia have reported feeling that the diagnosis of young-onset dementia came as a shock as they believed they were too young to be diagnosed with dementia (Clemerson et al., 2014). Clemerson et al. (2014) interviewed eight people with young-onset dementia who reported that they found it difficult to accept their diagnosis as they perceived it to be threat to their self-identity and potentially affected how others viewed them. Feeling relieved and recognising that their concerns were justified has also been reported among family caregivers (Bruinsma et al., 2020; Ducharme et al., 2013). Receiving a diagnosis provided an explanation for the changes in behaviour and emotions of the person with young-onset dementia (Ducharme et al., 2013; Thorsen & Johannessen, 2021).
Accompanying reactions of shock, devastation, denial, avoidance, and relief is an overwhelming sense and realisation that the life people with young-onset dementia and family caregivers had known will be forever changed (Kilty et al., 2019). It is not uncommon for people with young-onset dementia to imagine their own premature ageing and death when they learn of their diagnosis, as well as think of what their future now holds and the loss of the future they had assumed would be theirs (Clemerson et al., 2014). The moment of diagnosis has been described in the literature as a “decisive moment” in their lives (Thorsen & Johannessen, 2021). Receiving a diagnosis of dementia is the beginning of a new path to living with young-onset dementia and has profound effects on the lives of those with young-onset dementia and their family caregivers, including how they plan for the future.
Post-diagnostic support for people with young-onset dementia and their family members has been identified as an area requiring significant improvement (Stamou et al., 2021a). Age-appropriate support and young-onset dementia specific services for both the person with young-onset dementia and their family are lacking and often they must access services that are designed to meet the needs of older people (Cations, Loi, et al., 2021). People with young-onset dementia and their family have distinctive needs in relation to their family, finances and employment (Mayrhofer et al., 2018). Furthermore, they require services that enable them to come to terms with the diagnosis, cope with resulting changes, and maintain a sense of connection with their family and age-appropriate social contexts (Stamou et al., 2022). It has been found when people with young-onset dementia and their family access young-onset dementia specific services post-diagnosis, which is designed to improve continuity of care and quality of care, this leads to the person with young-onset dementia having an enabling and protective support network and adapt to life with their diagnosis (Stamou et al., 2021b).
Limitations of this Study
Firstly, the study only explored two predominant types of young-onset dementia (Alzheimer’s disease and frontotemporal dementia), therefore, the findings do not encompass the experience and perceptions of those with other types of young-onset dementia such as vascular dementia. Secondly, all cases of young-onset dementia featured in the study concern people with young-onset dementia who have familial support and live with their family and may not reflect the journey that those with young-onset dementia who live alone or have no support experience.
However, strengths of this study include having diverse perspectives and population groups from purposively sampled participants, particularly geographical diversity and different types of family caregivers (spouse/partner, child); as well as presenting cohesive accounts from both person with young-onset dementia and their family that appreciates the journey to diagnosis and reaction to diagnosis to be a shared experience.
Conclusion
The road to diagnosis can be experienced as prolonged, painful, and sensitive for both those with young-onset dementia and their family caregivers. It is not uncommon to be misdiagnosed and to have to wait years to receive a diagnosis, further compounding the anxiety experienced. Receiving a diagnosis of young-onset dementia is experienced as life changing, fraught with feelings of shock, relief, and devastation. Greater awareness amongst healthcare professionals, and general practitioners in particular, about young-onset dementia and its presentations is likely to ensure timely diagnosis as well as post-diagnostic care. For example, assisting people with young-onset dementia and their family caregivers to access information that is tailored towards younger people, and provision of better-informed support and guidance overall, will assist them to make appropriate decisions in relation to their future planning.
Footnotes
Acknowledgements
We acknowledge the Royal Freemasons’ Benevolent Institution for providing a PhD scholarship to the first author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.