
Abstract
A most crucial aspect in dementia care is recognising and maintaining the person behind the dementia condition. Yet, it has been found that caring for people living with advanced dementia risk becoming mere techniques and undervaluing the significance of inter-embodied relationships. This can lead to that the unique person of those receiving the care becomes overlooked and undermined. Research suggests how the care recipients’ unique person fruitfully can be recognised via identifying humanising caring relations in their everyday lives. Thus, it is necessary to explore how formal caregivers engage in care that support people living with advanced dementia as human beings, which is the aim of this study. Following Galvin and Todres’ existential lifeworld-led approach to care, the lived experience of formal caregivers’ humanisation of their care recipients were explored through participant observations and semi-structured interviews at two nursing homes specialised in advanced dementia; both methods were granted ethical approval from a research ethics committee. Based on the lifeworld-led theory we found four ways within formal caregivers’ experience to be able to humanise care recipients living with advanced dementia, which can be described as: The continuity of self, The touch of the world, The kindred understanding, and The invisible bond. We argue that it is not enough just replicating such caring ways in order to deliver humanisation in advanced dementia care, but require of the caregiver to engage in a genuine human relation with those for whom they care. Such engagement in recognising and supporting the intrinsic humanness of the care recipient can guide a more humanly sensitive care practice that recognises and maintains the unique person behind the advanced dementia condition.
Keywords
Introduction
Dementia is a syndrome characterised by symptoms of cognitive decline that commonly affect memory, communication skills, judgement, and awareness. Over time, cognitive decline becomes more severe (referred to in this paper as ‘advanced dementia’) potentially disrupting many aspects of a person’s life (Christopher, 2023). The behaviour and communication of people living with advanced dementia can become incomprehensible, irregular, and unpredictable, which can make it difficult for formal caregivers (i.e. professional care workers) to see and recognise the person they still are and continue to be (Martin et al., 2020; Post, 2016). This is problematic, as recognising and maintaining care recipients’ status as a person behind the dementia condition is a crucial aspect of dementia care (Kitwood, 2019; Norberg, 2019).
According to Sabat (2006), people living with dementia risk being perceived by formal caregivers through a lens that solely sees their behaviour and communication as evidence of pathology and cognitive loss. This perspective overlooks other explanations; for example, that a person might act or express themself in response to social interactions or the environment (de Medeiros & Sabat, 2016). Ultimately, this can create a perception among formal caregivers that the person living with advanced dementia is no more than a collection of dementia symptoms (Kontos et al., 2020; Martin et al., 2020). Research shows that this type of misperception is, unfortunately, quite common in contemporary dementia care practice. Formal caregivers risk misinterpreting what could be regarded normal actions and expressions as disturbing, worrying, or even dangerous signs of cognitive decline (Featherstone & Northcott, 2021; Grigorovich et al., 2019; Lopez, 2014).
As dementia is a progressive condition, many people will eventually move into long-term care (Brück et al., 2025; Bøgmose & Martinsen, 2019). Care in nursing homes is usually nowadays founded on Kitwood’s approach to person-centred care (Caspar et al., 2020; Krøier et al., 2022). This places the focus upon the person, not just as a human being, but someone who figuratively represents humanity and how we live as humans (Rokstad, 2021). Thus, it requires caregivers to recognise their care recipients in their full humanity as the persons they are, regardless of the dementia condition (Kitwood, 2019). However, aspects of person-centred care may be criticised; for example, despite being “designed to counter the erasure of the person, ‘recognizing the person’ is being turned into a ‘technique’”, undermining the humanistic ideal on which it is based (Macdonald, 2018, p. 294). Even care techniques aimed to individualise the care recipients living with dementia, such as life history or detailed descriptions of family relations and hobbies, can become vehicles of dehumanisation by potentially ignoring the humanising relation with the unique person (Macdonald, 2018; Tieu et al., 2022). This tendency has been described as a ‘McDonaldization’ of caring practices, with profound focus on efficiency, formalised social control, and predictable routines (Johnson & Dietrich, 2021; Norlyk et al., 2017). This entails a risk of residents living with advanced dementia experiencing poor quality care characterised by containment (Nybakken et al., 2018), lack of empathic understanding (Miron et al., 2017), and excessive use of antipsychotics (Harrison et al., 2021).
Furthermore, more theoretically directed research raises concern about the person-centred approach in advanced dementia, for undervaluing formal caregivers’ responsibility to engage with people living with advanced dementia in ways that preserve their status as persons through interpersonal relationships (Jenkins, 2014; Macdonald, 2018; Petherbridge, 2019; Smebye & Kirkevold, 2013; Tieu et al., 2022). These strands of research emphasise relationality in advanced dementia and how we as persons continue - through all stages of dementia - to be embedded and active in relations with other people and the world. This is consistent with Zieler (2014), who stresses that human beings stimulate one another through inter-embodied relationships; that is, true mutuality and recognition of bodily expressions are essential to keep people living with dementia connected to who they are as persons.
So, there exists a need to guard against a technification of person-centred care in nursing homes, and to acknowledge formal caregivers’ inter-embodied responsible role in such care, if we genuinely are to recognise and maintain the person behind the advanced dementia condition. Attention to an ethics of care perspectives can avert a standardisation of a ‘one best way’ care, thus “preventing a practice of ‘McNursing’ in health care” (Norlyk et al., 2017, p. 6). Galvin and Todres’ (2014) existential lifeworld-led approach to care offers an appropriate ethical framework (Andersen et al., 2024). It describes how care recipients’ unique person can be approached through their existential sense of feeling as being humans, and how formal caregivers recognise and support the intrinsic humanness of those for whom they are responsible - despite severe cognitive deficit - is essential in caring relations. Such existential approach can guide a more humanly sensitive person-centred care.
To improve recognising and maintaining care recipients’ status as being persons in advanced dementia, it is necessary to explore how formal caregivers engage in humanly sensitive caring relations in nursing home settings. We need to describe what these caregivers do, not as trained techniques, but as their day-to-day lived experiences of supporting humanisation of the other. Thus, we ask in this paper: “how do formal caregivers’ experience providing care that support humanisation of nursing home residents living with advanced dementia?”
Method
Theoretical Underpinning
In our study we approach formal caregivers’ lifeworld, which concerns the world we live in, both as it immediately appears to us and also imperceptibly forms the background of all our everyday experience of what it is to live as a human being (Herholdt-Lomholdt, 2022). Thus, any descriptions of the significance of the lifeworld mediate knowledge of meaningful existential interconnectedness within a world that is humanly lived (Galvin, 2010). And such existential lifeworld-led knowledge is a kind of knowledge that is essential for caring relations and significant for humanly sensitive care (Galvin & Todres, 2014).
Therefore, our theoretical background for this study was provided by Galvin and Todres’ (2014) lifeworld-led conceptual framework of the dimensions of humanisation. Individually and together the dimensions refers to the ever-present universal themes of every human life, which involves: (i) living a life from the inside (insiderness), (ii) being accountable for one’s actions (sense of agency), (iii) being individually unique (sense of uniqueness), (iv) existing in relation with others (togetherness), (v) caring for the meaning of one’s personal life (sense-making), (vi) having lived and continuously live a unique life (personal journey), (vii) belonging to a familiar place (sense of place), and (viii) being bodily connected to the surrounding world (embodiment). This framework provided an evaluative basis from where existential dimensions of humanisation in caring relations can be assessed in our data collection and analysis (Galvin & Todres, 2014).
A key aspect of phenomenological research is the requirement for researchers to set aside their prior expectations, understanding, and experience of the phenomenon under study (van Manen, 2023). In order to adopt an attitude of openness and wonder, the first author (responsible for collecting and analysing data) repeatedly reflected on and discussed with the other authors about his preconceptions as well as his use of the lifeworld-led framework for identifying and interpreting humanisation in caring relations.
Setting and Design
The study was conducted in 2024 at two Danish nursing home institutions, where people living with advanced dementia reside and receive 24-hour care. The data included two parts: interviews with care staff members and participant observations of caring relations between care staff and residents.
Overview of Interviewee Characteristics (Number of Participants in Parentheses)
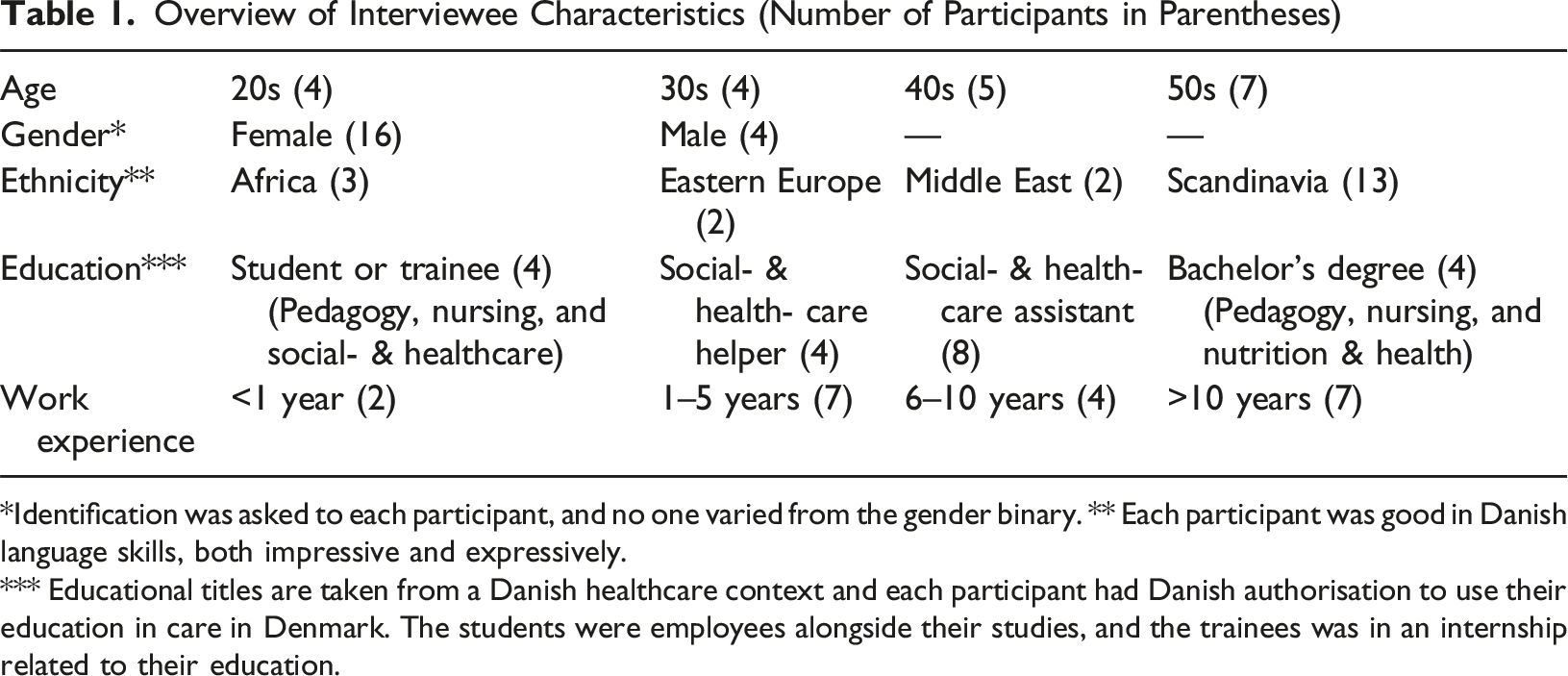
*Identification was asked to each participant, and no one varied from the gender binary. ** Each participant was good in Danish language skills, both impressive and expressively.
*** Educational titles are taken from a Danish healthcare context and each participant had Danish authorisation to use their education in care in Denmark. The students were employees alongside their studies, and the trainees was in an internship related to their education.
Additionally, observations were made of caring relations (not only concerning those interviewed) with the nursing home residents. Observations took place during daily three to six-hour visits across different days and shifts of the week during a four-month period. Here the lifeworld-led dimensions of humanisation (Galvin & Todres, 2014) implicitly steered the ‘grand tour observations’, which focused upon the general features of caregivers’ lived experience of providing humanly sensitive care. Gradually, observations were focused on more specific elements of their lived experience, changing them to ‘mini tour observations’ (Spradley, 2016). During the observations, the observer (the first author) at times actively participated in the daily care routines, meals, conversations, and activities, while at other times he simply observed the caring relations as they occurred.
In observing caring relations involving people with limited or no verbal language or activity, close attention was paid not just to what was said, but also to their behavioural patterns, non-verbal communication (e.g. appearance and grooming), body language (e.g. gestures and posture), and facial expressions (e.g. mimicry and signals). This was to acknowledge that even in the absence of speech, other actions and expressions do communicate something about the person in the caring relation (Ellingson, 2017). All observations were recorded, anonymised, and transcribed daily, and complemented with descriptive and reflective field notes (Emerson et al., 2011). Some of these observations were also used to inform questions used in the interviews with the care staff.
Ethical Considerations
The study respected the Helsinki Declaration and the guidelines for nursing research in the Nordic countries (Northern Nurses’ Federation, 2003) and received ethical approval journal number 2024-2 from an acknowledged research ethics committee (Roskilde University, 2025). All participants - including both residents and care staff - were giving written and oral information about study purpose, voluntary consent, and opportunity to end participation at any time with no consequences (Northern Nurses’ Federation, 2003; The Ministry of the Interior and Health of Denmark, 2017). None of the participants in the interviews or observations made use of this. Yet, the observer understood participants with cognitive limitations were not necessarily able to do this directly and, therefore, had distinct focus on this during the study.
People living with advanced dementia may lack the capacity to give informed consent in the usual manner. Hence, ‘process consent’ was used to ascertain residents’ willingness to take part (Dewing, 2007). As such, prior to the observations an extra initial effort was made to learn the resident’s general well-being and assess their ability to make an informed, voluntary choice. Time was spent informing the residents and their relatives through posters, handouts, nursing home-visits, and informal conversations about what the research entailed and that they could voluntarily choose to participate or not as well as withdraw their participation anytime if preferred. During the observations their agreed voluntary consent was approached as a process with continuous review as to whether their participation still was voluntary and informed (Dewing, 2007). Therefore, the observer made himself physically visible, so the residents took notice of him and asked him about his presence and purpose for being in the nursing home. This led to conversations with them about the study as well as their participation. Residents who did not or could not show direct interest in the study were informed about its purpose and the possibility of their voluntary participation at each new meeting. Only one resident slowly expressed reluctance to participate and was withdrawn from the study, after this was discussed with himself, his relatives, and regular caregivers.
In addition, the observer used his knowledge and years of experience in dementia care, both as a nurse and nursing educator, to consider the health of the residents and pay further attention to signs of discomfort in their bodily expressions and behaviours. This was to ensure that the vulnerable participants were not adversely affected by participating in the research (Liamputtong, 2007). Two residents experienced a deterioration in their health. Although this seemed not directly related to their participation, it was collaboratively decided with care staff and the manager of the nursing home to omit these residents from the remainder of the observational study.
Data Analysis
Interview and observation data were analysed in unison using van Manen’s (2023) phenomenological method as a guide for thematic reflection. This meant the data were analysed first through a holistic reading, to identify and capture the main significance of caregivers’ lived experience of humanisation in caring relations. Then, the data were read repeatedly focusing on certain sections, phrases, or statements essential or revealing in describing caregivers’ lived experience of humanisation in caring relations. Finally, the data were read with focus on each single sentence or sentence cluster and what they each revealed about caregivers’ lived experience of humanisation in caring relations. This three-step analysis process yielded general themes representing caregivers’ experience of providing care that support an humanisation of people living with advanced dementia.
Through a persistent, iterative, and reflective process of reading, identifying, and comparing meaningful descriptions and patterns the general themes were slowly allowed to evolve. Furthermore, to aid the analysis, the lifeworld-led framework to dimensions of humanisation served as a guide and structure in identifying and capturing instances of humanisation in which the care recipients have an existential sense as being humans (Galvin & Todres, 2014). However, the framework was only used in the initial part of the analysis and there was no attempt to force the findings into the particular dimensions.
van Manen (2023) emphasises the importance of presenting general phenomenological themes in ways that evoke wonder, embodied feelings, and empathy in the reader. Thus, inspired by a lifeworld-led approach, our general themes were analysed in a further step, transforming them into ‘embodied interpretations’. These can function as more aesthetical and evocative ways of representing others’ lived experiences that can strengthen the reader’s empathic imagining and understanding of such experiences (Amos, 2016; Galvin & Todres, 2014). In this way, each general theme was read several times while permitting an interpretative felt sense of empathically understanding these themes. Then, we focused on how this felt sense resonated and confirmed with the more detailed descriptions of caregivers’ lived experience or whether it required us to rework our interpretations. By moving back and forth between our felt sense and the detailed descriptions we identified possible words, phrases, and images capable of capturing the aliveness of the meaning of the general themes (Amos, 2016; Galvin & Todres, 2014). This allowed us to develop overall embodied interpretations, representing caregivers experience of humanisation in advanced dementia care as well as subsidiary interpretations of the more specific ways they do it.
Findings
Our analysis shows that caregivers’ experience of existential humanisation in advanced dementia care was expressed in four embodied interpretations: The continuity of self, The touch of the world, The kindred understanding, and The invisible bond. Within each of these, we identified three subsidiary interpretations expressing particular features emerging in the caregivers’ lived experience, indicated by (i), (ii), and (iii). In keeping with Galvin and Todres (2014), each embodied interpretation is presented creatively as a reconstituted, synthesised first-person narrative from the caregiver perspective and includes citation signs to indicate sentences or situations that were literally said and/or observed. This may help to make our embodied interpretations of caregivers’ lived experience more relevant to others at an existential level and “communicate them (…) not only in faithful and rigorous ways but in evocative ways that can awaken the aliveness of the meanings for the reader” (Galvin & Todres, 2014, p. 165). Not only can the use of first person in academic writing be favourable when appropriate (Webb, 1992), but it can be used in multiple ways to embody representations in qualitative research (Ellingson, 2017).
The Continuity of Self: Fragile Self-Recognition and Being Remembered
(i) I remember who they are. And I will help them to be who they want to be. Every day I have to remember carefully what each care recipient likes and how they formerly used to do things. I “serve an elderly man from the lovely island of Bornholm his morning coffee brewed in a particular Bornholm fashion” or ”aid an elderly woman with her make-up and getting dressed, putting on a nice hat, so she can feel like the fine lady she has always been and still wants to be”. But my point is not just about getting things done as each care recipient likes, such as their morning coffee, otherwise they could just order it in an automatic machine. Actually, my point is more that they’ll need me to show them that I remember who they were and still are, when struggling with awareness of this themselves. Both someone who remembers their unique person and shows them that they are a human who is not forgotten - me remembering a thing they like is sometimes more important than just the fact that they have the thing they like. So, I need to hold on to and not forget the person apparently lost in their dementia.
(ii) How I support them in recognising something of their self, a thing they might not be aware of or consider in that moment, is not just by following treasured outer things - coffee, clothes, or a local football team. It is also about their insiderness – being humorous, adventurous, or a romantic spirit. I recall helping an elderly gentleman who had always appreciated giving his wife small gifts by laying out things for him to collect and give him a loving feeling of having something for her and say “honey, look what I have for you”.
(iii)Yet sometimes it’s hard, when they don’t behave as they usually do or show no reaction to things they normally respond to, leaving me “questioning whether they are still the same person or even a person at all?”. Of course that’s not true! I know they are not just a collection of former circumstances, but keeps changing through their lives, as we all do. It’s not enough just relying on their past self, becoming ‘trapped in melancholy’, and keep looking at old pictures of their family or a ship they once sailed. I must be curious, concerned about, and committed to honestly learn who they are as the human being they always have been and continue to be. Learning to ‘truly know’ them allows me to become a ‘familiar caregiver’ who can aid in their self-recognition. “Imagine waking up not knowing where you are, not necessarily knowing the person in front of you, but slowly starting to recognise things in the situation that remind you of yourself”. They too as human beings have a special piece of music from their youth, a desirable way of being talked to, or something that suddenly have found its way back into their appreciation.
The Touch of the World: Embodied Belonging and Sensory Presence
(i) “Everyone needs a hug” as often words are not enough. I cannot keep talking or just performing my everyday routines. It’s not just about feeding, washing, nor managing a certain amount of sleep. The care residents need more than this, a feeling of “ahh, that feels nice” or when angry and chaotic “come have a hug, feel understood”. Something beyond what I can say, beyond what I can explain, but it makes them seem more relaxed, composed, uplifted - as if they find their footing on uncertain ground. To be honest what I think they need is to feel a ‘bodily sense of belonging’ in a lovely world surrounded by loving others. Of course, I know it is not just about going around touching people, merely pleasing people’s senses. There’s more to it, maybe a presence of closeness, maybe a heartwarming human feeling of having someone willing to do something nice for them. Many times, when we sit and enjoy the early spring sun, I see present in their bodies well-being and warmth - “I make sure that the sunrays touch their skin”. Or, when we sit and enjoy the silence of a peaceful ward, I sense in them a presence of comfort and intimacy that my closeness provides - “I make sure to hold and caress their hand”. By ‘sensorial touching’ them through their skin, but also their eyes, ears, nose, or mouth, it allows me to keep the person linked to a lovely world with their dementia.
(ii) But it’s more than just the presence of the actual sensory touch. I can see them becoming hopeful for the promise of sprouting life and light from the spring sun. Or that they are soothed by a feeling of unity with someone who calmly and steadily holds their hand. I like to think it gives them some sort of assurance of a more welcoming future, especially, in the days of feeling confused, insecure, or lonesome.
(iii) Yet sometimes I lose sight, when they don’t show me, seem to remember, or can’t describe how they experience our caring relation, which makes me “questioning whether their desires, needs, or feelings are not relevant or required?”. But that’s a flawed idea. It’s not enough just pacifying them with things to make living in our nursing home feel convenient and cosy. Making things just to be nice, does not really make them feel like a human. No, it tends to make them confused and uncomfortable, maybe even get them to wander around or stay passively alone. My physical touch must be more than massage, watching TV more than entertainment, smelling and tasting food more than nourishment, celebrating festive days more than distraction from everyday routines. “It needs to be meaningful to them, appealing for them to be held in connection to a world they know and cherish”. They too as human beings find ‘meaningful comfort’ in all sorts of things of the beautiful world we live in. Like listening to birdsong or children laughing in a nearby schoolyard. Smelling freshly brewed coffee in the morning or blooming lavenders. Or getting goosebumps from a cold winter breeze or the magical moment of reliving something pleasureful you had forgotten.
The Kindred Understanding: Empathic Envisioning and Human Curiosity
(i) “Put yourself in their shoes”. Is not always easy, I cannot always understand why they do what they do, and why it is always so easy to think of it as just cognitive symptoms. The other day one care recipient was screaming and hitting out at his own mirror image in a window, he does this occasionally - “maybe a symptom of his lost self-awareness”. Another one walks smiling up and down the ward to see when her late husband is coming to visit, she does this tirelessly every day - “maybe a symptom of her lost memory”. I can feel it tires me that I cannot recognise where their unusual behaviour comes from. But here is when I need to stop myself and think again, ‘look again’. To be frank this is what they need of me, that I try to look again and see the person behind their dementia.
(ii) Yet sometimes it occurs to me, when their ways of expressing themselves are not commonly expected from a human being, to “questioning whether their behaviours and communication are just meaningless and irrational carried out by someone less than human?”. Coming to think like this scares me and I discover how wrong I have been. Sometimes I thought that I actually saw them and understood their ways of acting, giving them what they wanted. No maybe even worse, I misunderstood their needs, thinking they sit there passively means they do not want anything. Just because they ‘can’t really express’ what they need or what they desire in ways I can grasp, that does not mean that they need or desire nothing. How mistaken I am in these moments. Of course, I know they are a human being just like me. No matter what, I need to remind myself “always to see them as the humans they are and always will be”.
(iii) I find it helps me to turn towards my own subjective self and be curious about imagining how I might as a human being have acted the same being in a similar situation. ‘Empathically envisioning’ how our caring relations could affect me and use this insight to find a kindred human rational and meaning of their actions. I will also get angry if I feel that I constantly say things and no one takes me seriously, or I will to be confused and defensive if someone I don’t know talked to me as if they have known me all my life and steadily wants me to do something I don’t want. By focussing “when would I react like that myself”, I can better envision how the world could look from their eyes, even when most apathetic, angry, or amnesic. They too as human beings may get unintentionally passive, aggressive, or repetitive when guarding themselves in unsure, unsafe, or unfamiliar situations.
The Invisible Bond: Honest Connection and Mutual Recognition
(i) Allowing yourself to be a person too. Striking this delicate balance between “leaving your shit at home”, but not completely. I cannot fake a smile or a look as if everything is positive and happy when I am not. I have to be hopeful for the care recipient’s sake, and even if I am having a bad day, I find in myself a place of home and joy to share, lift, and support. In fact, it is like they see through me - they look at me with a tender gaze when the days hurt, cheer me up when the hours exhaust, laugh with me when moments delight. Like they sense me - they react and adapt their spirit to my determined tone, my dreary mood, and my witty personality. And in this ‘honest connection’, they actually care for me. We “create an invisible bond between us” where I learn to recognise them as the person they are, because they try to learn recognising my person too. When things are light, we embrace the moment, we socialise in entertaining ways, we become adventurous of our beautiful world. When things are hard, we find ways to keep the mood up, we find things to laugh about, we make it cosy together.
(ii) Even though we can joke about quite serious things, they will not allow me to make fun of them, to infantilise them. They are grown-up persons, and they use humour and laughter as grown-up persons, not as kids trying to bring out a giggle. When talking to them as kids: “come here my little princess”, their eyes and mimic shows me signals of unease, embarrassment, or being on unworthy display. When treating them as kids: “who are in the mood for popcorn”, hints of humiliation and shrinking away become visible in their posture and reaction. I need to ‘respectfully acknowledge’ the person affected by their dementia and ‘curiously meet’ this person as my active partner in our shared caring relation.
(iii) Yet sometimes I find myself in moments, when the care recipients may become aggressive, or remain absolutely passive, or monotonously repeat themselves, of “questioning whether they live in a world of their own, detached from meaningful relations with other people?”. No! This idea has to be in my awareness, this idea has to be put aside. We are ‘mutual persons’ in our caring relation and as they sense me on a given day, I too must learn to sense them. Invest my time and focus exploring and find into their actual mood, desires, tempi, tone, and perception of things. This may help me to better act on their terms, alter my approach according to their feelings, and generally create a kind of ‘unity between us’. They too as human beings have good and bad days of gratefulness, longing, excitement, annoyance, joy, fatigue, indifference, vitality, and the like, and need to be met and treated accordingly.
Discussion
Our findings show that formal caregivers experience their care practices or at least elements of them as being able to existentially humanise their care recipients. We found that they do this by: helping the care recipient to be aware of their own unique person by being remembered by others, nurturing a sense of belonging through the care recipient’s sensed body, focusing to develop an envisioned understanding of being in the care recipient’s situation, and respecting and responding to the invisible bond that exists in the mutual relation with the care recipient.
Our findings also indicate how formal caregivers’ experience of humanisation in advanced dementia care demands of them to grant recognition to care recipients as persons. This recognition is often linked to identifying and affirming the person’s unique identity, to re-mind who they are. But importantly this recognition is not tied to continuously trying to revive the care recipient’s former identity. They have not only been human throughout their past but continue to change - and will do so in the future - as human beings in relation to their overall life situation, not solely as a result of their dementia condition. Granting recognition of their person should not be limited to a constant effort to ensure that they still remember who they were and who others are. This idea is being greatly expressed by Taylor (2008) in her renowned essay, emphasising that instead of always asking if her mother living with advanced dementia recognises those dearest to her, we should ask “Do you, do we, recognize her? Do we grant her recognition?”” (p. 315). And the way in which we can grant her mother recognition should be based on the mother’s present actions and expressions. This resonates with emerging ideas in scholarly dementia literature that accentuates changes in one’s unique person before (and during) dementia as signs of qualitative changes of still being the same person, while adapting to an ever-fluctuating world of living with progressive dementia (Käll, 2017; Post, 2016).
Our findings also show how humanisation in advanced dementia care is experienced by formal caregivers as a genuine engagement in the behaviour and communication of their care recipients, even when most subtle or apart, as signs of who they are as a person. This kind of caregiver engagement can be defined as a ‘participant’ attitude towards the other, in which this other is conceived of as a person and someone “who is the author of their own words and actions” (Brinkmann, 2025, p. 606). Similarly, Grøn (2022) describes how caregivers need to explore the ‘imagistic signatures’ of care recipients, which convey their particular ways of being embodied present in the world. Thus, one resident shows her personal boundaries towards another person by drawing a border around her napkin with her finger. Another resident screams mournfully whenever someone sitting closely to him gets up and tries to leave. Both can be seen as expressions of their person’s unique signatures. Also, Vermeulen (2021) depicts an elderly woman living with dementia who reacts to the silence around her by leaving her home and staying out in the community. “When you do nothing you die a little bit” as the woman tellingly says (p. 185). Yet, such sudden behaviour is often understood by caring others as evidence of irrational ‘wandering’. It is important, Vermeulen (2021) argues, that caregivers avoid such misconceptions and instead try to understand unfathomable behaviour of people living with dementia as a ‘honing responsive engagement’, which entails their unique sensitive way of responding to everyday life situations. In this case breaking the stillness of the home by moving outside.
Formal caregivers’ participant attitude in caring relations, where they see, listen, and feel the uniqueness of their care recipient, is described as essential if they are to steer away from a technification and dehumanisation of care practice (Johnson & Dietrich, 2021; Macdonald, 2018; Norlyk et al., 2017; Tieu et al., 2022). Although such stereotyped care might create a system flexible enough to adapt to each individual care recipients’ particular desires and preferences, it can end up taking for granted or even eliminating the human relation between caregivers and the care recipient’s uniqueness (Johnson & Dietrich, 2021; Norlyk et al., 2017). In contrast, our findings reveal that formal caregivers experience a profound sense of humanisation in advanced dementia care, where recognising the individuality of care recipients forms the basis for genuine human relations, not merely a procedural response to personal desires or preferences. In all our findings this genuine human relation is clearly the main element ensuring a humanly sensitive care, taking precedence to any form of technique, method, or system organisation. A ‘logic of care’, as Mol (2008) terms it, where “defining ‘good’, ‘worse’ and ‘better’ [care] does not precede practice, but forms part of it” (p. 87). Therefore, it is crucial not to take our findings as knowledge of novel techniques that merely provides more choices of colour to the caregiver’s caring palette. Rather, they are to be taken as a kind of aesthetical knowledge that appeals to and touches the ‘heart’ of the caregiver (Galvin & Todres, 2014). In this way it can better support a more humanly sensitive care, where the status of people living with advanced dementia as being persons are maintained (Galvin, 2010).
Finally, though our findings help to identify more clearly what humanly sensitive care should entail, it is perhaps unremarkable that humanisation in caring relations demands among other things recognition of the other’s uniqueness, helping each other to create and enjoy beauty, enriching life with laughter and sharing our tears. However, when the formal caregivers act in these ways to recognise and engage the humanness of the residents, they are also calling forth and expressing their own humanness. This in the form of sensitively, purposefully, and meaningfully giving of themselves to the residents. As implied in one of our embodied interpretations, caregivers experience that, “Even if I am having a bad day, I find in myself a place of home and joy to share, lift, and support”. Thus, by giving to humanising the care recipient living with advanced dementia, the formal caregivers are also giving to humanising themselves.
Strengths and Limitations
Allowing ourselves to be bodily immersed in the analysis could be criticised by those who consider that researchers should operate at more distance from the lived experience of the participants. However, qualitative voices emphasise how “researchers do not merely use their bodies to access knowledge in their minds; our knowing is interwoven throughout our bodies” (Ellingson, 2017, p. 156) and how “attendance to the researcher’s bodily response to the research data is understood as enabling the production of ‘words that work’ for the participant, author, and reader alike” (Amos, 2016, p. 307). Thus, by becoming an ‘analysing body’ to our qualitative data, we can understand and represent the lived experiences of others in ways that better work aesthetically, promote wonder, and sensitise empathic understanding (Amos, 2016; Damsgaard et al., 2023; Ellingson, 2017). Certainly, this is also the intention with our embodied interpretations.
Furthermore, some doubts can be raised of the validity of our findings, as those receiving the care may be inhibited to explicitly confirm whether the care actually made them feel as being human. Thus, can we truly say that engaging as suggested in our embodied interpretations fosters humanisation among care recipients living with advanced dementia? In phenomenology, the intertwined relations between humans and their worlds can be described as intersubjectivity implying that as humans we are already situated in a context where we share environments, language, and meanings. This means that intersubjective experience allows for an empathic experience (Moran, 2017). Given this, we are able to understand other humans’ experience to some extent (Mortari, 2008). Researchers have shown how they validly interpreted the lived experiences of people with limited cognitive function by following their intersubjective experiences (Bakkenget & Våpenstad, 2023; Martinsen & Norlyk, 2012). The same reasonably applies to our findings.
Conclusion and Clinical Implications
Our study shows how formal caregivers are able to support the person status of residents in advanced dementia care through genuine human relations. Four embodied interpretations indicate what fosters such humanising caring relations. It stems from formal caregivers who constantly (deliberately or not) bear in mind that their care recipients living with advanced dementia are in increased risk of not being seen or met as a person and find ways to ensure their humanness, not just as an abstract ideal, but as a sensible reality in everyday care for those most vulnerable to be dehumanised. However, the attempt of just replicating such everyday ways will not deliver humanisation in advanced dementia care if the genuine human relation is absent. So, if person-centred care in nursing homes is to become less stereotyped and commodified and more of a recognition of the person behind their advanced dementia, our embodied interpretations can serve as a useful guide to support a more humanly sensitive person-centred care. Hopefully, our study may inspire future research in taking a more existential approach to understanding life and care in dementia, and show how a focus on the aesthetic and embodied can promote humanisation not only of those receiving care, but also of those providing it.
Footnotes
Ethical Consideration
The project received ethical approval from Roskilde University’s research ethics committee with journal number 2024-2.
Consent to Participate
To ensure voluntary consent of participation on an informed basis, the ‘process consent’ method was applied throughout the study. A method that is developed for use in research involving people living with advanced dementia.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of a PhD project supported by the Independent Research Fund Denmark (2061-00010B) and Aarhus University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.