
Abstract
Introduction
Person-centred care is a philosophy of care rather than a method ready for implementation and utilisation in daily work. Internationally, few methods for the implementation of person-centred care have been widely adopted in clinical and care practice. In Norway, the VIPS practice model is a commonly used model for person-centred care implementation.
Method
Qualitative manifest content analysis was used. Managers and leaders in the municipalities, care institutions and domestic nursing care services were eligible for inclusion if their workplace had implemented the VIPS practice model and conducted the consensus meeting regularly for a minimum of 12 months. Seventeen respondents were included. Individual interviews were conducted either via FaceTime, Skype or telephone.
Results
Three global categories emerged describing the implementation process: (1) factors that impact the decision made at municipal level to implement person-centred care; (2) requirements for a good start at unit level and (3) factors that help to support the new routines in the unit. The categories were entwined; the results of one affected the results of the others. The informants from both domestic nursing care and institutions described the same factors as important for the implementation of the VIPS practice model.
Conclusion
To implement person-centred care by use of the VIPS practice model, the frontline staff need sufficient information about the rationale for implementing the model. The management’s vision and ethos of person-centred care must be followed by time set aside for staff training and regularly scheduled VIPS practice model consensus meetings. Head nurses are key to getting the new routines established and maintained and should be supported by the management.
Keywords
Introduction
The perception of dementia as a slow living death that destroys a person as human being is on the wane in clinical practice, which the person-centred care philosophy developed by British social psychologist Kitwood (1997) may take much of the credit for. This care philosophy has since the 1990s become the most widely recognised person-centred care (PCC) approach. It is referred to in the British National Institute for Health and Care Excellence (NICE) (2006) as well as in the Norwegian (Norwegian Directorate of Health, 2017) and Swedish (Socialstyrelsen, 2017) dementia guidelines, which all state that dementia care must be based on person-centred care. The tenets of Kitwood’s care philosophy have been summarised in what is called the VIPS framework (Brooker, 2007), which has 4 main elements and 24 indicators. The letters of the acronym stand for (V)
Person-centred care is a philosophy of care rather than a method ready for implementation and utilisation in daily work. Few methods for the implementation of PCC have been developed, and the most known methods are all from the United Kingdom. One of the best known and most tested (Griffiths et al., 2019; Surr et al., 2018) is dementia care mapping (DCM), developed by Kitwood & Bredin (1992), an observational tool that can be used to improve the quality of care (Brooker & Surr, 2005). Brooker’s Enriched Opportunities Programme (EOP) for people with dementia is a multilevel intervention that focuses on improving their quality of life (Brooker et al., 2007). The Well-being and Health for People with Dementia (WHELD) intervention (Ballard et al., 2018) focuses on person-centred care training for champions in the staff group, in addition to promoting tailored, person-centred activities and social interactions.
Person-centred care and non-pharmacological interventions have been considered time-consuming and not cost-effective (Kales et al., 2014, 2015) but have been found to increase the quality of life among nursing home residents (Ballard et al., 2018; Rokstad et al., 2013) and to reduce neuropsychiatric symptoms, such as agitation, and the need to use psychotropic drugs (Ballard et al., 2018; Fossey et al., 2006; Rokstad et al., 2013; Testad et al., 2014). Still, few evidence-based interventions promoting PCC have been widely adopted in clinical and care practice. Cost-effective interventions that use a champion model and are less dependent on supervision from external therapists have been suggested to remedy this (Ballard et al., 2018; Kales et al., 2014). In addition, studies have found that personalised care provision, like person-centred care, is associated with the general job satisfaction of staff and affects staff attitudes towards people with dementia (Jeon et al., 2012; Moyle et al., 2011; Stein-Parbury et al., 2012; Wallin et al., 2012).
The implementation of any method in healthcare settings is a complex undertaking because it is a social process delivered through the actions of individuals as well as organisations. A method or innovation may be based on evidence and have excellent feasibility, but its results still depend on the effectiveness of its implementation. Implementation has been defined as the process of putting into use or integrating an evidence-based intervention within a setting (Rabin et al., 2008), and there are numerous frameworks for implementation in general (Damschroder et al., 2009; Greenhalgh et al., 2004; Kitson et al., 1998; Harvey, & McCormack, 1998; Villalobos Dintranset al., 2019) as well as several for person-centred care interventions in particular (Banaszak-Holl et al., 2015; Gilster et al., 2018; McCormack & McCance, 2006). There is, however, limited evidence about the requirements for the successful implementation of PCC methods (Surr et al., 2018), although known facilitating factors include preparation of frontline staff prior to implementation, managerial support during implementation and sufficient time to implement the method. A lack of leadership and resistance to change among staff have been found to hinder implementation (Backman et al., 2020; Kelley et al., 2020; Griffiths et al., 2019; McCormack et al., 2010; Surr et al., 2018).
In Norway, the political incentive to implement person-centred care in dementia care was communicated through two national dementia plans (Ministry of Health and Care Services, 2015, 2018). This led to municipalities including person-centred care in their local dementia care strategy plans. The VIPS practice model (VPM) was developed in Norway to provide a feasible method for implementing PCC in municipal dementia care settings (Rokstad et al., 2013; Rosvik et al., 2014, 2011). Approximately 30% of Norwegian municipalities have chosen to use the VPM to implement person-centred care in both domestic nursing and care institutions since the launch in 2011. The model is described below, in the Procedure section. In the VPM, it is the responsibility of the organisation’s management to facilitate the implementation process. Hence, the aim of this study is to explore managers’ and leaders’ experiences in order to identify factors that facilitate or impede implementation and use of the VIPS practice model in domestic nursing care and long-term care institutions.
Method
Setting
In Norway, health care is public and financed by the tax system; hence, most primary-care services are publicly owned and operated. Approximately 9% of these services are run by private non-profit or for-profit healthcare providers (Statistics Norway, https://www.ssb.no/pleie, 2020). There is a strong political incentive that people should live in their own home for as long as possible; hence, a person can receive visits from the domestic nursing care unit several times a day, depending on the care need. The municipalities also provide day-care activity centres for home-dwelling people with dementia, various types of short-time stay in rehabilitation and relief units and long-term institutional care (not hospital care). More than 83% of residents in nursing homes have dementia (Røen et al., 2017), and mean survival in nursing home is 2 years (Mjørud, et al. 2020). The units in the nursing homes have approximately 30% registered nurses (RN) working in the frontline in addition to auxiliary nurses (50%) and unskilled workers (20%) (Gautun & Hermansen, 2011). In special care units for people with dementia, a regular staff-resident ratio at the day shift is 3 residents to 1 staff. Many workplaces have a RN with a master’s degree in geriatrics, dementia or similar who is responsible for the professional development training of staff in the organisation. All counties have publicly funded centres for the development of institutional and domestic care services (Centre for Development of Institutional and Domestic Services, 2020) that provide professional supervision to the primary-care services in their municipalities.
Procedure – the VIPS practice model
The VPM (Rosvik et al., 2011; Røsvik et al., 2013) is used in long-term care, in day-care service for home-dwelling people with dementia and in domestic nursing. The model is based on three factors that Kitwood (1997) described as central to creating a person-centred care culture: structured teamwork, training and supervision, and supportive leadership (Kitwood, 1997, p. 110).
The hub of the VPM is the weekly consensus meeting in the unit, where frontline staff discuss a care situation, for example, that a person with dementia resists morning care or does not participate in any activities he or she finds meaningful during the day. The consensus meeting adheres to a fixed structure. The frontline staff are assigned central roles and functions in the consensus meeting to ensure that they are engaged in the process of implementing person-centred care in their clinical practice (see Text Box 1). The VPM resource person (RP), a representative of the largest professional group in the frontline staff, chairs the meeting with support from the leader (preferably the head nurse). The resource person starts by explaining the situation to be discussed during the meeting. The situation must be delineated in time and space. Then, the primary contact (usually an auxiliary nurse) describes how she/he believes the situation is experienced by the person with dementia (see Text Box 1). Before the meeting, the primary contact should have (a) observed the situation; (b) talked to the person with dementia and, when relevant, his or her next of kin and (c) assessed the situation with the use of observational tools, for instance, the Cornell Scale for Depression in Dementia (CSDD) (Alexopoulos et al., 1998) or the MOBID-2 Pain Scale (Husebo et al., 2014, 2007). Information from frontline staff who are not present at the meeting should have been collected. Then, the rest of the staff give their views on the situation. The VIPS framework (Brooker, 2007) is used to analyse the situation to make sure all aspects of person-centred care are assessed, and interventions are agreed upon, documented, implemented and evaluated at a set date.
The aim of using the VPM is to learn what person-centred care is for each person with dementia in various situations and to build a foundation of competence of person-centred care and dementia within the staff group. The function of the head nurse is to supervise the competence-building process; this involves being vigilant and alert to staff needs for guidance and knowledge and ensuring that they arrive at professionally sound conclusions in the meeting.
A randomised controlled trial (RCT) (Rokstad & Rosvik et al., 2013) showed that people with dementia living in nursing home units using the VPM had significantly lower levels of depression as measured by the Cornell Scale (CSDD) (Alexopoulos et al., 1998) and fewer neuropsychiatric symptoms as measured by the Neuropsychiatric Inventory (NPI) (Cummings, 1997) than the control group.
To use the VPM, the staff in a unit must be trained in a two-day VPM basic course. Staff who must be trained are those who will have roles in the meeting, namely, the RP, the head nurse and the registered nurse who is responsible for professional development in the workplace. However, many workplaces train the whole staff. Those who do not participate in the two-day course must attend a three-hour introduction to person-centred care and the VPM.
After attending the basic course, the head nurse and frontline staff receive written VPM materials. For the leaders, this includes a manual describing the implementation of person-centred care, the VPM, the consensus meeting structure and the roles and functions of staff. For frontline staff, there is a manual describing person-centred care, the VIPS framework and various non-pharmacological interventions. There is a manual for institutions and another one for domestic care. In addition, there are support materials to be used in the consensus meeting. These include two posters displaying the VIPS framework indicators, one for domestic care and one for institutions, and a poster illustrating the consensus meeting structure and the questions the primary contact is asked when he or she tries to describe the perspective of the person with dementia (see Text Box 1).
The basic course is taught by a VPM course conductor. Healthcare personnel with a bachelor’s degree or more are eligible to attend a VPM conductor course. Typically, workplaces have their own VPM course conductor, usually a manager, head nurse or registered nurse responsible for professional development at the workplace. To standardise the course and ensure that it is taught the same way everywhere, the course conductors receive all course materials, including pretaped lectures, a booklet describing the course and a list of questions to be asked and discussed during the course. The Norwegian National Advisory Unit on Ageing and Health is responsible for the VPM conductor courses.
Participants
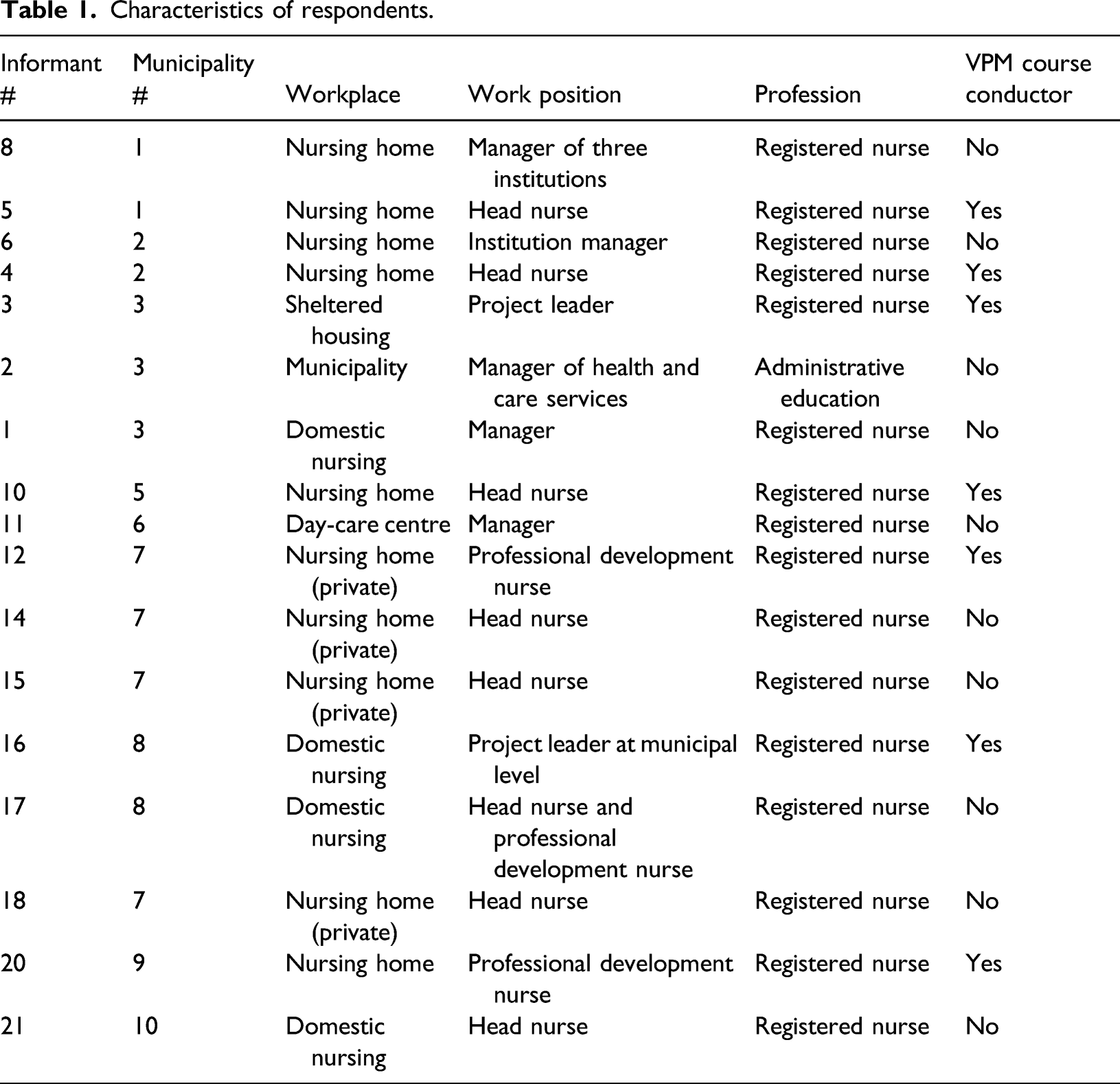
Characteristics of respondents.
Inclusion process
Initially, the dementia resource centres and the Centre for the Development of Institutional and Domestic Services in all counties were contacted by email and asked to provide a list of workplaces that had used the VPM for more than 1 year. Management at one nursing home was contacted directly because the authors had information about how long they had used the model. Managers at all levels were then invited by email by the authors to participate in the study. This resulted in the inclusion of seven leaders from three workplaces. To increase the inclusion rate, all those who had attended a VPM conductor course were contacted by email and invited to participate. The course conductors were also asked to forward the invitation to workplaces they knew were using the VPM but did not have their own course conductor as these workplaces had not received the invitation. This resulted in the inclusion of 10 respondents. When the interviews started, a total of 17 respondents were included representing 10 workplaces. Additional three leaders replied by e-mail that they were willing to be interviewed, and their names were added to a waiting list. However, after 17 interviews, no new information emerged, and saturation was reached; therefore, the leaders on the waiting list were not included.
Data collection
An interview guide was developed based on the aim of the study and sent by email to the respondents a week in advance of the interview (see Text Box 2). Individual interviews were conducted either via FaceTime, Skype or telephone. Both authors participated in the interviews, which were tape-recorded and lasted approximately 30 minutes; the shortest lasted 16 minutes and the longest 49 minutes, with a mean of 27 minutes. One respondent had a hearing impairment and replied to the questions in the interview guide in writing by e-mail.
Transcription was done verbatim by the firm Totaltekst AS. The audio files and transcribed files were stored in a research server accessible only by the two authors.
Analysis
NVivo version 12 PRO was used to support the analysis. Qualitative manifest content analysis was chosen because it implies staying close to the text and describing the visible and obvious (Elo & Kyngas, 2008; Graneheim & Lundman, 2004). This was found to be a useful approach as the aim was to identify barriers and facilitators. Open coding was applied because predetermined categories were not considered to appropriately reflect the respondents’ experiences of the implementation process. Coding categories were derived directly from the text data (Hsieh & Shannon, 2005).
To extract the content, meaning units (e.g. sentences and paragraphs) were labelled with codes. Based on the codes, categories and sub-categories were developed describing the manifest content of the transcripts (Graneheim & Lundman, 2004). The categories were used to further analyse the interviews and were modified when appropriate. In the interpretation of the data, the two researchers discussed and reflected upon the categories and sub-categories (Graneheim & Lundman, 2004). The interviews were read again to see if any new understanding of the material emerged from the meaning units. The final categories and sub-categories were discussed in light of the research question and the context of the study, and global categories were developed after reviewing the structure of the categories. The credibility of the interpretation was established by grounding the meaning units in the text using quotations from the respondents.
Both authors participated in the analysis. If the authors disagreed about an interpretation, they discussed it until consensus was reached. A third party, Knut Engedal, professor emeritus of geriatric psychiatry, could be consulted in the event that the authors failed to reach an agreement, but this did not happen.
Results
In all, 16 women and 1 man from 10 municipalities were included; their ages ranged from 30 to 65 years. There were from 1 to 4 respondents from each workplace or municipality talking about each workplace.
In the transcribed interviews, three global categories emerged describing the implementation process: (1) factors that impact the decision made at municipal level to implement person-centred care; (2) requirements for a good start at unit level and (3) factors that help to support the new routines in the unit. The three categories were entwined; the results of one affected the results of the others. Respondents from both domestic nursing care and institutions described the same factors as important for the implementation of the VPM. In the following, the term ‘manager’ refers to the municipal (administrative) level, while the term ‘leader’ refers to organisational (clinical) level.
In line with national guidelines: Factors that impact the decision made at municipal level to implement person-centred care
The first category had two sub-categories: (a) the management’s ethos and rationale and (b) champions outside and inside the organisation. This category highlights the decision-making process prior to the implementation in the unit.
The management’s ethos and rationale
Management at both municipal and organisational levels saw the implementation of the VPM as a way to comply with the Norwegian dementia guideline, national strategy and quality documents and local dementia care action plans. An informant who was the VPM project leader in a municipality referred to the incentives and guidelines from national health authorities: The VPM is a very good tool; it is quite in line with all that [the national dementia guidelines and the quality regulations]‘A full life – all your life’ and [its motto] ‘What is important to you’ (#5). Person-centred care was described as the organisation’s ethos, and improving the quality of care was the most important incentive for implementing person-centred care for the leaders irrespective of management level. In addition, at the municipality level, good results regarding both human resources and economy were envisioned, as described by a municipal manager for health and social care: The goal is to reduce sick-leave and increase the quality of care (#2). Another respondent referred to the rationale conveyed by leaders at the municipality level this way: (. . .) person-centred care and VPM, and having consensus meetings, if it helps, if it saves resources in regard to the staff (. . .) and [leads to] thriving both for employees and residents and more inclusion of next of kin [in the care for the residents] (#3).
Champions outside and inside the organisation
The respondents described that having champions, both outside and inside the organisation, was important in reaching the decision to implement PCC. A supportive champion could be found at any level of an organisation and among all staff groups at both domestic nursing agencies and long-term care institutions, including at the specialist healthcare service level, the municipality management level and among registered nurses and frontline staff. One informant said: We had a psychiatrist here who is very interested in person-centred care (…). When I signed up for the [VPM conductor] course, I told him, and he was very enthusiastic. It made it easier for me to go for it (#10).
Leaders on all three levels, that is, the municipality management level, the organisation management level and the unit level, sought the endorsement of the frontline staff for the decision to implement the VPM. They underlined the importance of preparing the frontline staff before the implementation process began by providing sufficient information about the VPM and the rationale for implementing it: We [the leader and staff] talked about it a lot for a while before starting, so they were ready and aware that we were about to start (#10). Another manager said: What is VIPS, and what are we trying to achieve? I think that is important [to talk about] (#2).
The informants described how they teamed up with engaged and interested frontline staff before initiating this intervention, which would affect the way the staff worked: They [the auxiliary nurses] felt important, that was a good thing. I asked them how they wanted it to be, and let it be their thing. That was wise, I think. They got ownership of it [the VPM]. Then it was the employees’ peers who recommended it, not just me (#14).
One head nurse allowed frontline staff who were interested in person-centred care to attend the VPM basic course before the rest of the staff group. Their enthusiasm influenced the other staff: They came back, all fired up, and told the others about this fun and useful thing we would start doing. So, then the others were positively attuned [to the VPM] as well when they attended the course (#4).
This is the way we work: Requirements for a good start at unit level
Category 2 had three sub-categories: (a) leadership commitment, (b) stability among the staff group and (c) staff training. This category highlights requirements for a successful start in the unit.
Leadership commitment
The respondents underlined that leaders at all levels in the organisation had to be committed for the ethos of person-centred care to become a reality: We were very clear that this was not just another project; this should be the way we work, how we do things (#8). Without this commitment, it was very difficult to find the time and the resources necessary to do it. Having motivated – and motivating – leaders at the organisational level who were well-informed about the content of the training and its significance for the successful implementation of PCC facilitated initiating PCC at the unit level. Two informants, an administrator and a project leader, commented about this. The first stated: When you are about to start, it is important to have someone who makes an effort and is engaged (#2). The other said: It’s a good thing the leader attended the course. She helped us get the two days set aside for the [basic] course (#20).
In several municipality meetings, a block of time was designated for reporting on the progression of the implementation process in the units: . . . to keep up the steam on the VPM, we have this reporting going on; the leader has to report (#5). A respondent said: I ask, “What have you discussed? Have you used the manuals?” I am this concrete about using the manuals because I think that is wise; it helps us maintain the way of thinking (#8). Some managers demanded structured plans; one head nurse said: Every term we give the manager a schedule for the [VIPS] consensus meetings. I have heard her say to the other head nurses [that] it’s a good way to see that it is being done (#11).
Stability among the staff group
Having stable personnel, regarding leaders as well as frontline staff, was described as a decisive factor for the successful implementation of PCC. One of the informants, a manager of domestic services, said this about the successful units: They have had a very stable leadership, with both a coordinator and a professional development nurse in place and engaged. In the other units, there has been more sick leave, resignations and dismissals (#16). Stability in the unit was necessary in order to develop the competence and skills required to execute the functions of the VPM: [It is important] that the turnover is low, that people know what the primary tasks are, that they can document things, simply a well-driven unit. You need to sort out any chaos before you can implement something that requires professionalism and structure because you need structure to make it work (#14).
Staff training
All the informants talked about the importance of providing the two-day basic course for as many of the staff as possible before starting to conduct the consensus meetings in the unit: I think it is part of the key when you are starting up – to have people who understand it and know it [the VPM]. And it helps that many others in the staff group and colleagues have attended the course and have an understanding about it (#21). According to the informants, the more staff attending the basic course, the better: First, we prioritized the full-time employees, but in health care there are lots of temporary workers, so you should give the course to everyone (#3). Attempting to save time and resources by minimising training proved futile; implementing the consensus meeting was very difficult if the staff had not undergone the training. A manager said: I think we made a mistake first. So, we went back to the start, and she [the project leader] used a lot of time to teach the VPM to the staff. And then it was much easier (#2). In order to provide new employees with a smooth transition into the staff group and the PCC way of working, several of the informants described making the course mandatory to the staff if they wanted to work in the unit: So now we conduct the course regularly once a year for all the newly employed (#6). Allowing for time to learn the structure of the consensus meeting ensured good results: It is a very high attendance; they have learned the meeting culture and say, now, after a year, it is automatic, they have high-quality professional discussions (#2).
There was some difference of opinion regarding who should be trained to carry out the roles and functions of the VPM. Most of the informants underlined the importance of choosing the right person to be the RP who chairs the meeting: You need a good chair (#16), and another described being . . . very picky about who I choose as RP (#8). These informants stressed that the RP must have a genuine professional commitment and the ability to engage the rest of the staff group: Find an RP who is enthusiastic about care for the elderly and is concerned about everyone having a good time at work (#1), and: They need professional engagement and [to] be able to bring people along. You have to be a bit…. you must be a driving force, giving people a push, and selling it (#8). Some leaders had decided to train the entire frontline staff group to master the RP’s functions in order not to be dependent on the presence of one particular member of staff: Most are RPs. The RP is the chair. It says right there what you are supposed to do. They’re all trained (#10).
Personnel who did not attend the two-day basic course received an introduction to person-centred care and the VPM in order to include them in the process of change in the unit and provide knowledge about dementia and person-centred care: . . . And we had the shorter course [3 hours] for other staff groups, the occupational therapist, the physiotherapist, the physicians, the chaplain, people in the administration. They were frustrated because there was so much talk about the VIPS [VPM], and they didn’t know what it was (#6) and: I had a 3-hour teaching for the unskilled workers and those in the kitchen and in service [janitor, etc]. They really liked learning about dementia, so now they understand why the residents talk and act as they do, and they meet them [the residents] the way they should (#12).
Keep the wheels turning: Factors that help uphold the new routines in the unit
The third category had four sub-categories labelled as follows: (a) a determined head nurse, (b) leaders who establish structure, (c) mastery and positive results and (d) supervising the staff.
Implementing person-centred care and the VPM is not a one-time operation. It requires determination, organisation and improvisation when unforeseen events occur. Both in domestic nursing and in the nursing homes, enthusiastic, engaged and supportive leaders and head nurses worked to organise and facilitate the consensus meetings: She [the nurse responsible for professional development] has been very able and a driving force regarding this. And she really has structure and order. She maintains the structure firmly in her unit. That is necessary if you want to accomplish anything. You need to stick to the plan and the structure you have set up (#16).
A determined head nurse
Upholding the new routines for the consensus meeting was highly dependent on the head nurses. In fact, their engagement was described as pivotal: It is the head nurse who makes the difference . . . a leader who schedules the meetings and organizes the time to hold them (#10). A commitment to conducting the consensus meetings meant determination and organisation as it was difficult to find time for a meeting when the entire day shift was present: In our workplace, it is important not to have this type of attitude: ‘There is staff calling in sick today; we can’t have the meeting; we have to get out [of the nurses’ station] and work’. We [try to] avoid that, you just must find solutions when there is sick leave [among the staff group] (#17). Residents could have appointments outside of the unit that required staff resources, making it difficult to convene the staff, and unexpected events could interfere with the meeting schedule: And if someone [staff] has to leave [the unit] and four [members of staff] shall sit around a table and talk [about] VIPS, there is no one in the unit [with the residents]. That is a huge challenge (#5). Still, the head nurse found it worthwhile to prioritise the consensus meetings: We have so little time. But I wish we could have more meetings because they are very useful (#21). In the VPM, the head nurse is expected to attend each consensus meeting, supervise the staff, ensure the professional standards of the decisions and provide recognition to the frontline staff. Doing all of this was described as difficult to accomplish but necessary: It is difficult for her [the head nurse] to attend every Thursday. She has been to some meetings, but sometimes we use the team nurse*. She is responsible for the team. But it is not the same (#20). (*The team nurse is the leading registered nurse in a smaller group of residents and staff.)
The new routines required the staff to be prepared for the professional discussion in the consensus meetings, something they were not accustomed to. The head nurse, therefore, had to remind the staff to do the preparatory work: They used to meet up without cases to discuss, and then suggested something at the meeting, but then you do not get the required professional level: no assessments, no observations, haven’t talked to the next of kin, just very ad hoc. So we have become stricter (#1). The VPM requires members of staff to voice professional assessments and deliberations, for instance, when attempting to take the perspective of the person with dementia when presenting a situation that is up for discussion (see Text Box 1 on how to take the person’s perspective). Some staff needed support from the head nurse to do this, and one head nurse said she encouraged them by stating: This is your job, and I know you can do it (#15). To ensure the legitimacy needed to install loyalty to and compliance with the decisions made in the consensus meeting, it was important that all staff took part in the decision-making process. To support quieter members of staff so they did not just agree with the more talkative ones in the discussion, one head nurse handed out sheets of paper and asked the participants at the meeting to write down their thoughts before the discussion started.
The informants described the impact that the roles and structure of the VPM consensus meeting had on the staff: The engagement has increased. Everyone is being heard. They can’t just sit and not say anything. The different roles are really smart (#15).
One head nurse reminded the staff that they were responsible for their decisions at the end of the meetings: Ok, it is good that you agree about this; this decision is yours (#1). The head nurse was also vigilant regarding the frontline staff’s daily work and held them accountable for the implementation of the interventions they had agreed upon in the meeting: It has to do with trust. I must teach them to tell me when someone does not follow our plan [the interventions set in the consensus meeting]. I need someone to tell me about the Saturdays and Sundays when I am not here (#15). The new systematic way of working also meant that interventions should be adjusted if necessary. The head nurse reminded the staff to be alert and make observations: I tell the frontline staff ‘You need to document it [how the interventions work], then we can discuss it. You need to observe it and look into it before the consensus meeting when we are evaluating it’ (#12).
The head nurse who establishes structure
The head nurses described how they worked to keep the VPM alive in the unit: When no one watched over it, it just faded (#14). To manage to conduct the consensus meetings regularly in the units, the meetings were all planned ahead regarding time and participants: For things to work, you need leaders who create structure, structure with fixed meeting times and full-time employees [present] (#16). They made schedules, so staff could be prepared for the meetings: We planned the next meeting early on; they [the frontline staff] knew 14 days in advance. It gives them time to process it in their heads (#21). The head nurses also ensured that the meeting was conducted and that staff attended it: I remind them in the morning: At noon we are having the VIPS meeting. So, someone must look after the residents, and the rest join the meeting. There is always someone who does not come, so then we must go and get them (#14).
Mastery and positive results
Some resistance towards change from frontline staff was registered at the beginning: Yet another thing? Yet another meeting to attend every week? (#14). However, most resistance towards the consensus meetings evaporated after staff experienced what could be achieved: They had a situation with much aggression [from a resident] at every morning care. Even coercion was used sometimes. Then they had a consensus meeting which made them think: What is the resident’s experience? And they employed interventions with a completely different approach, and then suddenly, the problems were solved. Of course, when you have had an experience like this, you want to do it again (#5).
Experiencing that the consensus meeting helped them to identify interventions that made a difference for the resident motivated the staff: They told me they detested the VPM at first; it was so much [to learn], but really it isn’t that much. Now they appreciate that they have it [the consensus meeting] once a week to discuss things like this, find interventions. They see that it is useful (#3). The professional discussions that led to interventions that staff could see benefitted the person with dementia motivated them: We see the purpose. We want to succeed, and it gives a sense of mastery to us who are involved. It leads to a good dialogue and good care plans (#17). Another informant said: You see that the interventions you discuss and put into action really work (#17). One informant described how one of the older frontline workers changed her attitude: In the beginning, she was sceptical and said: ‘What kind of nonsense is this’, but then she attended the VIPS meeting, and we found some really good interventions. And she saw how this turned the resident’s day around. So [she said], ‘We must have a new VIPS meeting soon!’ She became the keenest one, right, and [now] initiates meetings (#16).
Supervising the staff
In the start-up phase, the head nurses were often supervised either by a member of the municipality’s dementia team or the project leader responsible for implementing the VPM in the municipality. Frontline staff were usually supervised by the VPM course conductor or a registered nurse responsible for professional development in the workplace. Several of the informants described having supervision for larger groups of staff members: We share experiences, talk about how we are doing, what we manage and what the challenges are. Share the good stories from the VIPS meetings, it is important because it inspires, and then someone has some good advice to share (#6).
Discussion
This is the first study to explore managers’ and leaders’ experiences and identify factors that facilitate or impede the implementation and use of the VIPS practice model in domestic nursing care and long-term care institutions. Several facilitators and barriers were described within three overarching categories: (1) factors that impact the decision made at municipal level to implement person-centred care, (2) requirements for a good start at unit level and (3) factors that help to support the new routines in the unit. Central facilitators were leadership commitment, a committed head nurse, sufficient training of frontline staff and champions among frontline staff. Central barriers were resistance to change among frontline staff, lack of training of frontline staff, difficulties finding time to conduct the consensus meetings and high staff turnover.
Factors that impact the decision to implement person-centred care
Few evidence-based methods for implementing person-centred care have been widely adopted in clinical practice (Ballard et al., 2018; Kales et al., 2014). The respondents in the present study stated that the reasons for implementing the VPM were to comply with national guidelines regarding PCC in dementia care and to increase the quality of care. Lack of cost-effectiveness (Ballard et al., 2018) has been an argument for not implementing methods for PCC, but the managers in the present study had expectations of reduced sick leave among staff as a result of enhanced job satisfaction when the VPM was implemented. Such expectations are supported by research that has shown that person-centred care is associated with increased job satisfaction (Moyle et al., 2011; Wallin et al., 2012) and a decrease in staff’s emotional exhaustion (Jeon et al., 2012). Without commenting on economic benefits, Kitwood (1997), p. 104 stated that the ethos of person-centred care includes the well-being of staff as well as that of people with dementia. With regard to cost-effectiveness, the fact that the head nurses in the present study prioritised the consensus meetings despite sick leave and planned ahead and changed the timing of events that would disrupt the meeting schedule indicates that the VPM was found to be a manageable model. It could readily be implemented because the benefits to people with dementia as well as staff made up for the time required for meetings.
Previous studies have found that a lack of leadership and resistance to change among the staff impede implementation, while organisational characteristics like communicating with staff and an absence of hierarchies are favourable conditions for implementation (Griffiths et al., 2019; McCormack et al., 2010). The respondents in the present study described how they worked to obtain staff endorsement of the decision to implement the VPM. They talked with staff about what the VPM entails and the rationale for the decision to implement it, and they asked staff’s opinions about the VPM before the implementation started. This supports the assumption that involving staff in decisions that affect their work is favourable for successful implementation.
Requirements for a good start
The finding that the management’s commitment was decisive for successful implementation of the intervention at the ground level in the organisation is well-documented in previous research. Without it, it would be difficult to secure the economic resources to conduct the necessary training of the frontline staff and set aside the time required for the procedures the intervention entails (Griffiths et al., 2019; Stein-Parbury et al., 2012; Surr et al., 2018). Griffiths and colleagues, in their study of the implementation of another person-centred care method (dementia care mapping), described that managers who were unaware of the resources required for a PCC approach represented a barrier to its implementation because they were reluctant to make the necessary priorities (Griffiths et al., 2019).
In the VPM, the function of the head nurse is to encourage, coach and supervise. This type of support was reported to increase staff’s work engagement and aligns well with what has been described regarding the importance of teamwork in other studies on the implementation of PCC (Backman et al., 2020; McCormack et al., 2010).
Common sense and evidence show that high staff turnover is a barrier to successful implementation (Griffiths et al., 2019). The managers in the present study stated that it was futile to start the implementation process if a unit did not have stable personnel. However, staff attrition may affect implementation differently, depending on the characteristics of the intervention. In the study by Griffiths and colleagues, the intervention required observation, coding, report writing and feedback sessions conducted by one or two trained individual members of staff. When the personnel trained to conduct the intervention procedures resigned or were absent, it was difficult to identify and train a suitable replacement (Griffiths et al., 2019). The VPM procedure of the consensus meeting provides a team-building structure that involves the whole care-staff group who all have central roles on a permanent or rotating basis. The head nurse or other members of staff can serve as substitutes until new personnel are trained if staff members trained for the permanent roles resign. This makes the VPM more sustainable.
Factors that uphold the new routines
Ballard and colleagues concluded that future work should consider how to facilitate sustainability of the person-centred care intervention in a nursing home setting (Ballard et al., 2018). A challenge that is described in most implementation studies is maintaining the new routines an intervention entails (Backman et al., 2020; Griffiths et al., 2019; Surr et al., 2018). If new routines and procedures are skipped repeatedly, regardless of well-justified reasons, the intervention is simply not implemented. If that is the case, it may be pertinent to ask whether the intervention is a good match for the setting. However, Ballard et al. (2018) and Kales et al. (2014) stated that many of the interventions described in studies that document this problem relied on external personnel, such as a researcher or project leader or non-medical personnel. As Ballard and colleagues contended, if the use of supervision from external therapists is limited in favour of internal supervision (Ballard et al., 2018), sustainability may be more likely to be attained. In the VPM, internal supervision in addition to training means that the competence remains within the organisation. The findings in the present study indicate that, in order to be sustainable, interventions should train the majority of the staff in person-centred care and teach them to be responsible for the routines and procedures required by the intervention.
Future research should focus on the competence the staff needs to work in a person-centred way. In addition, research should investigate resulting change in work culture and possible financial benefits of using a person-centred care model, both related to staff, for instance, sick-leave, and people with dementia, for instance, use of psychotropic medication.
Strengths and limitations
Purposive sampling was used in this study because the aim was to identify factors that contributed to overcoming barriers and facilitating a successful implementation that proved to be sustainable; hence, only service locations that had used the VPM for at least 1 year were included. The experiences from service locations that failed to implement person-centred care using the VPM were not obtained. This information could have provided knowledge and understanding about challenges and barriers that were not encountered among the respondents for this study. However, our focus was on implementation, and the respondents knew that barriers to implementation were of interest to the interviewers.
Contributing to the strength of the present study is the fact that leaders from all four health regions and from both larger urban and smaller rural municipalities in Norway were included and that leaders at ground level as well as administrative managers at municipal level were interviewed.
Primary contact: spokesperson for the person with dementia; presents the situation from the perspective of the person with dementia. Resource person: the chair of the meeting; a representative of the largest frontline staff group. Head nurse: provides support to the resource person and the primary contact if needed; ensures that interventions uphold the appropriate professional level by guiding and teaching frontline staff when needed. Questions to be answered by the primary contact In the VPM, the primary contact is responsible for presenting the perspective of the person with dementia. This can be done by answering the following questions: What do you think the person is reacting to? How do you think the person experiences the situation? 2. What information and observations do you have to indicate that this is how the situation is experienced by the person? 2.1 What does the person say? (For example, ‘I won't, I don't want to’, ‘come here’ and ‘ouch!’) 2.2 What does the person do with his or her body? (For example: turns his or her back, looks down and grabs the caregiver) 2.3 What do relatives say? 3. Which feelings do you recognise in the person in this situation? 3.1 Is the person angry, anxious, frustrated or scared? 3.2 Is the person trying to protest about something?
VIPS practice model Interview guide for physicians and leaders 1. Have you noticed any changes in the unit since you started using the VPM concerning The staff? The residents/users? The next of kin? 2. Looking back, are there differences in the care and treatment in the unit from before you started using the VPM and now? If you answered yes, what are those differences? What is the most important change that has happened? 3. For physicians especially Can you explain your conception of the VPM? Has use of the VPM affected your function in the unit? If you answered yes, how has your function been affected? For leaders especially What affected the implementation of the VPM both negatively and positively? Were there factors that had to be present in order to implement the VPM? Please provide examples. 4. Now that you have used the model for a while, is there something you would have done differently? Do you have any advice to those who are about to start using the model? What is important in order to be able to conduct the consensus meetings weekly and follow up on the interventions?
Conclusion
This study provides concrete guidance and recommendations for the implementation of person-centred care using the VPM from leaders of units that have succeeded in the implementation and use of the VPM for more than a year. The informants underlined the importance of preparing the frontline staff by providing sufficient information about the rationale for implementing this model. The management’s vision and ethos of person-centred care must be followed by time set aside for staff training and regularly scheduled VPM consensus meetings. As head nurses are key to getting the new routines established and maintained, they need support from the management and should be offered supervision in the start-up phase from professionals in the municipality with experience from implementing the VPM.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the Norwegian Centre for Research Data (NSD). All included respondents provided a signed consent form.