
Abstract
Dementia-friendly communities can increase community participation and social wellbeing for people impacted by dementia. However, culturally and linguistically diverse people have typically been excluded or underrepresented from dementia-friendly community design processes. This study aimed to establish the factors that affect community engagement for culturally and linguistically diverse people impacted by dementia, and their suggestions for a dementia-friendly community in Canterbury-Bankstown, Australia. Bilingual researchers conducted semi-structured interviews (N = 17) in three languages: seven were in English (dyads n = 6; former carer n = 1); five were in Arabic (person with dementia n = 1; dyads n = 3; former carer n = 1) and five were in Vietnamese (dyads n = 4; former carer n = 1). These interviews explored barriers and facilitators to community engagement and design considerations for a culturally inclusive dementia-friendly community. Interview transcripts were thematically analysed, inductively. Factors that affected participation included community perceptions of dementia, family support, and the accessibility of transport and public environments. Members of the Arabic and Vietnamese groups faced language barriers and cultural stigma, which increased a sense of exclusion and isolation. In response, they emphasised the need for accessible transport, inclusive social groups, and community-wide dementia education to create a more dementia-friendly environment. Their suggestions aligned with traditional dementia-friendly community principles and were subsequently adopted by the local dementia alliance in designing a more inclusive and culturally responsive dementia-friendly community.
Introduction
Globally, dementia rates are rising, with culturally and linguistically diverse (CALD) communities facing unique challenges in accessing appropriate support (Chejor et al., 2022; Gilbert et al., 2022). By 2051, dementia cases within culturally and linguistically diverse communities in Australia are projected to increase by up to 600% (Temple et al., 2022). However, research within these communities – particularly regarding the social wellbeing of those affected - remains under-explored (Low et al., 2019). This gap in understanding makes it difficult to develop informed and inclusive practices, potentially reducing the effectiveness of interventions such as dementia-friendly communities in multicultural settings. Different cultural groups experience dementia differently due to the stigma in their communities, their perception of dementia and caring duties, and their social practices (Allam et al., 2023; Boughtwood et al., 2011; Kane et al., 2021; Xiao et al., 2015). Nuanced experiences and perceptions of dementia that differ from the main population in a particular geographical area are more prominent in cultural groups living in the diaspora, which refers to the spread of people from their original homeland, often in Western contexts (Chejor et al., 2022; Grossman, 2019; Nguyen et al., 2021). Culturally and linguistically diverse people living with dementia, and their families, often have low engagement rates within these communities due to pre-existing obstacles, such as stigma, language barriers, lower levels of education, as well as limited access to appropriate resources and transport (Cheung et al., 2019; Gilbert et al., 2022; Shatnawi et al., 2023). To build effective interventions or to conduct research involving diverse cultural groups, there needs to be direct inclusion of their voices when developing these interventions.
Within Canterbury-Bankstown, Australia, where this study is set, an estimated 8,000 people live with dementia; and this figure is predicted to double by 2050 (Dementia Australia, 2014). Canterbury-Bankstown is one of the most multicultural regions in Sydney, with nearly 60% of the population speaking a language other than English at home; the two most common being Arabic and Vietnamese (Australian Bureau of Statistics, 2016). These two language groups share some cultural factors that can impact their experiences of dementia. For example, stigma and discrimination are contextualised in a similar way. First, the idea of ‘losing face’ can lead to social isolation for the person living with dementia and their families, as some prefer to not experience or perceive diminished social standing in their community (Allam et al., 2023; Chejor et al., 2022; Gilbert et al., 2022). Second, caring duties are similarly emphasised within the family unit and considered an ingrained aspect of being a spouse or child (Kane et al., 2021; Nguyen et al., 2021). Vietnamese cultural concepts, such as Tình thương (compassion), nhân quả (karma), and sự hy sinh (sacrifice), also shape these cultural kinship structures (Xiao et al., 2015). Thus, some people who care for people living with dementia hesitate accessing carer supports and feel overburdened by these responsibilities (Hammad et al., 2022).
The aforesaid factors can impact people from culturally and linguistically diverse communities in accessing the community and/or adequate care in general. However, much of the data from previous studies were gathered from carers’ perspectives with people living with dementia not being present during the interview process. To inform the development of a dementia-friendly community intervention, the involvement of culturally and linguistically diverse people living with dementia is needed. This study addresses this by establishing how English, Arabic, and Vietnamese speaking people living with dementia and their care-partners engaged with the community before and after a dementia diagnosis, and how to support their ongoing engagement.
Method
Design
This observational qualitative study was conducted with a multicultural community advocacy group called the Canterbury Bankstown Dementia Alliance using community-based participatory action research methods (Wallerstein, 2021). The study was designed with Alliance members to ensure the findings would inform their action plans and advocacy efforts (see Supplemental Materials for more details). This study was reported as per the consolidated criteria for reporting qualitative research framework (Tong et al., 2007). Ethics approval for the study was received from the South Western Sydney Local Health District Human Research Ethics Committee (Reference: 2021/STE02281). All volunteers provided written informed consent to participate.
Recruitment and Consent
A purposive sampling strategy was used to recruit people living with dementia and care-partners residing in Canterbury-Bankstown, Australia, using in-language newspaper articles, emails, and flyers circulated through the alliance’s networks. A AU$30 gift card was offered to each participant for their expertise and time. Participant materials (including the promotional material, information sheet, consent form, and interview schedule) were translated from English into Arabic and Vietnamese using an accredited translation and proof-reading service.
Eligible participants were: aged 18 years or over; resided in Canterbury-Bankstown, spoke English, Arabic or Vietnamese; and self-reported as living with cognitive decline or dementia. If required, the person living with dementia was accompanied by an informal/family carer with appropriate proxy consent obtained. Former informal care-partners of a person who had dementia and passed away within the past 5 years of the study were also eligible to participate to capture the experiences of the community.
Participation was determined through a screening phone call, where the researchers discussed the project, their eligibility, addressed questions or concerns, and asked about decision-making capacity and whether they had vision, hearing or speech accessibility requirements that may impact their ability to consent. Potential participants were not excluded based on the severity of their dementia to obtain a broad range of experiences from the community (refer to Supplemental Materials for more details). Informed consent involved detailed verbal and written provisions at the appropriate level of comprehension for each person, about the purpose, methods, demands, risks, inconveniences, discomforts, benefits, and possible outcomes of the research. The volunteers received a participant information sheet via post or email and their written informed consent was obtained before the interview.
Bilingual researchers (two female, one male) communicated with Arabic and Vietnamese participants, while two researchers (both female) communicated with English-speaking participants. Researchers held at least a Bachelor’s degree with Honours level qualification and were currently working in academia. These researchers completed Dementia Australia’s Dementia Friends training, and the senior researchers provided project-specific training on the conduct and transcribing of interviews. There were no established relationships between the data collectors and participants.
Data Collection
Semi-structured interviews of 30 to 60 minutes were conducted between October 2021 and September 2022, inclusive. The interview schedule contained two parts. Part one pertained to: age; gender; country of birth; languages spoken at home; year of arrival to Australia (if applicable); employment status; education level; the nature of relationship with participant; their dementia diagnosis type and stage; and their living situation. Part two of the interview pertained to community engagement before and after the dementia diagnosis. The interview questions were sourced from Dementia Australia’s dementia-friendly community survey (Dementia Australia, 2018) and referred to participation in activities like shopping, eating out, physical activity, social activities, entertainment and sporting events, and visits to galleries, libraries, and community groups. Participants were also interviewed about the factors that helped and hindered community participation, as well as forecasting what their participation in these activities might involve as the disease progressed. Participants were asked about future strategies and initiatives to make Canterbury-Bankstown a dementia-friendly community (see Supplemental Materials for the full interview guide).
The Alliance reviewed and refined the interview guide with the researchers. To be sensitive to the cultural stigmas of dementia, the use of the word ‘dementia’ was minimised and where possible referred to ‘Alzheimer’s disease’ or ‘memory changes’. Participants were asked when they started to notice memory changes rather than directly probing about the diagnosis. Participants were given the option to be interviewed over the phone or in person at a public place of their choosing or in their home (following COVID-19 pandemic precautions at the time). All interviews were audio-recorded and transcribed into English by the bilingual researchers for efficient analysis.
Data Analysis
Thematic analysis was conducted inductively, as per Braun and Clarke (2006), using NVivo (1.7.1). Interview transcripts were (re)read to construct and refine themes from the data. Transcript text was initially coded to a descriptive theme. Saturation was achieved when there were no new codes or themes constructed from the data, ceasing the need for further recruitment. Two senior researchers reviewed the codebook. Preliminary themes were constructed using two overarching topics discussed in the interview: involvement in the community, before and after diagnosis; and suggestions for a dementia-friendly community intervention.
Three researchers reviewed the preliminary codes and themes regarding the first topic (community involvement). This process was repeated until consensus was reached. The thematic analysis served to construct themes pertaining to the barriers and facilitators of social engagement and community mobility for each language group and the data were narratively synthesised across and, where relevant, between-groups.
Transcript data regarding the second topic (suggestions for a dementia-friendly community intervention) were collated, discussed between three researchers, and narratively summarised into categories. This involved synthesising the suggestions provided by participants, across all language groups, into actionable recommendations for presentation to the Alliance. Individual participants did not provide feedback on the themes; however, the findings were communicated to the Canterbury Bankstown Dementia Alliance through two hybrid meetings for comment and consideration in their dementia-friendly community action planning process. The presentation of the results for the Alliance was anonymised with demographic information removed to prevent the possible identification of participants, as per the protocol approved by the human research ethics committee.
Results
Participant Characteristics
One participant withdrew their consent after completing the interview process, stating that they were uncomfortable with their data being used in the study. Their data were excluded, and the final sample comprised of 30 individuals from 17 interviews: six English speaking dyads (or pairs of a person living with dementia and their care-partner) and one former care-partner; three Arabic speaking dyads, one former care-partner, and one person with dementia; and four Vietnamese dyads and one former care-partner (see Supplemental Materials).
Community Engagement
Title of Each Theme and Definition Regarding Community Involvement
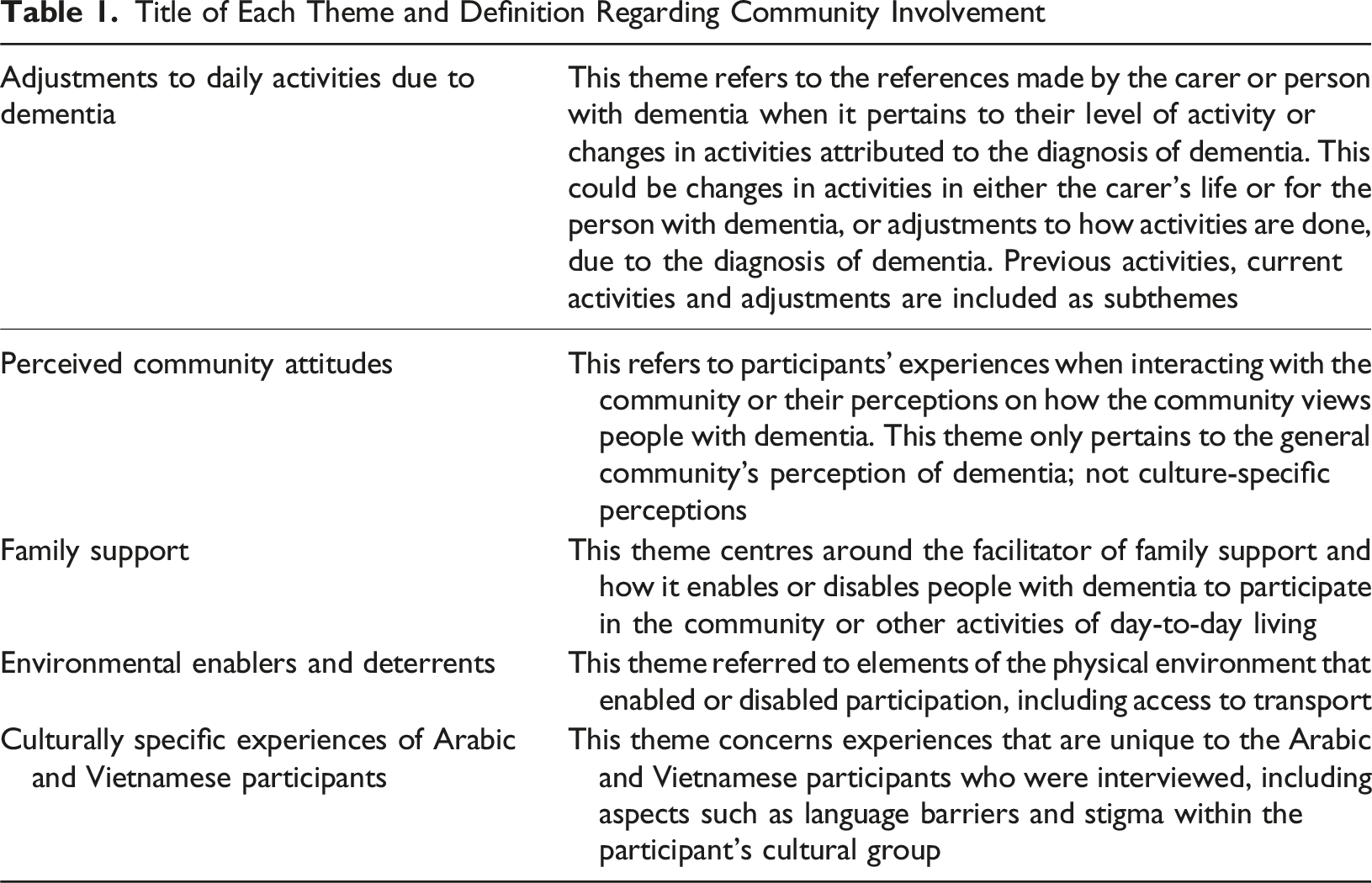
Adjustments to Daily Activities due to Dementia
Prior Activities
All three groups discussed having a broad range of activities before the diagnosis that were limited or adjusted after diagnosis. This included going to the park, walking, shopping, visiting museums, cafés, friends, libraries, and concerts, as well as driving: Everything, we went cinemas, we went shopping, we went picnics, yeah, Ramadan festivals and other events (Arabic carer 1, age 60 years).
Current Activities and Adjustments
Participants faced significant changes or adjustments to their daily activities after the diagnosis of dementia, with common activities such as errands, going to the gym, and attending medical appointments, having to be paused or conducted with greater difficulty and planning than before diagnosis: A few times per month (Community activities). Going to my GP, or going out, eating out. But now everything stops as [person living with dementia] is too weak now (Vietnamese carer 3, age 61 years).
Major activities that required greater planning, such as holidays, were also impacted: [Person living with dementia] used to go shopping and did all the errands independently, used to go to the movies uh, used to go to the gym, used to play tennis, used to walk quite a lot. Probably wanted to go to more museums but uh, used to go away on girls’ weekends away. We used to go on extended holidays overseas. What else? Go out for dinner on a regular basis (English carer 3, age 56 years).
Participants who reported less of an impact on current activities attributed this to the person with dementia being able to have someone who accompanied them on these activities or to other adjustments put into place: I think we’re still doing all the same things it’s just that 80% of time I will accompany [person living with dementia] and 20% of the time other people are accompanying [person living with dementia] (English carer 3, age 56 years). I can’t leave him on my own anymore, we have a support worker we are very lucky on NDIS
1
, but the support worker isn’t trained so I have to train them, and I have to wait and support him, so it takes longer so by the time he is showered and dressed. He always goes out every day for a coffee, a walk, some fresh air, whilst he is out with support worker (Arabic carer 1, age 60 years). Doing errands and shopping for 2–3 times per week. Another carer will come and drive us to the shops. We also go out for a walk after breakfast, if the weather is nice and we feel good. Additionally, we need to go to GPs or pharmacy. Sometimes, my husband (person living with dementia) needs to stay inside the carer’s car, and I will try to do a quick shop. Otherwise, we walk to the shops or restaurants then take a cab home. My husband is unable to walk a round trip (Vietnamese carer 5, age 62 years).
Community Perceptions
While all the participants reported experiencing issues surrounding the community’s perceptions of dementia, the impact on their community activities differed among the groups. In the English and Arabic groups, participants described feeling unwelcome in community settings and public spaces, such as shopping malls and cafes. Some cited the community’s understandings of dementia as people who are “lesser” or “loony” as the reason they avoided public spaces: 200,000% they do not understand dementia, you look at him and he seems normal, he opens his mouth, and they start rolling their eyes around like loony loony (Arabic carer 1, age 60 years). Because of their perception of my mother was, she was now less, and I don't know how you get that out of our society. That people who are disabled, elderly or frail are less. Because they're not! They’re just different and they need an equal amount of support. And not everyone was like that I don't mean that. But my radar was on. Now we're not coming into this shop again. Now we weren't coming to this cafe again. You know, they’re going to be that rude. Forget it. And, you know, we'll go somewhere else. We'll try somewhere else. (English former carer, age 67 years).
However, the Vietnamese participants cited a different experience, often stating that people were friendly and helpful: They are all good and supportive. For example, they gave me the way when I crossed the street with my mom (Vietnamese carer 2, age 72 years).
Family Support
All carers interviewed were direct family members. Many carers discussed their sacrifices or adjustments to enable the person they cared for to remain in the community. They reported times when they prioritised the needs and wellbeing of the person living with dementia over their own. For instance, they missed social events or hobbies, lest something happen to the person living with dementia while they were gone; they did not access timely healthcare for their own needs; and they limited their community participation: We have hardly gone to the city since the pandemic and transport issues with [person living with dementia] I am the one who also feel trapped and broken down, not only mom – much stress (Vietnamese carer 1, age 59 years).
This also included examples of carers being personally impacted by a stressful experience, for example an injury and having their first thought being what would happen to the person that they care for: She had a fall a few years ago and she rang me and she goes ‘oh I split my head open, what's gonna happen to dad? I’m like you need to call the ambulance and get yourself to hospital first. So, she was more worried about what was going to happen to him (English carer 1, age 73 years).
In Arabic and Vietnamese communities, cultural perceptions of caring suggested that more extreme examples of care-partner needs were undervalued: I was living here on and off, but now post-diagnosis I can’t leave her, she is highly functional. I don’t want her to get unwell. She is extremely healthy mashallah
2
, but sometimes she gets viruses. I don’t know, sometimes, it’s pretty rare. Like I had covid for a week and I had to leave and when I came back, she was really unwell. She kept falling over and couldn’t get up, it took two weeks to get on her feet. So, otherwise she is quite fine. But there is definitely not enough support (Arabic carer 4, age 54 years). Actually, I think I am in the early stage of dementia as well. I usually forget when to take my mom to the GP for injections. That’s really not good for her (Vietnamese carer, aged 72 years). Yes, absolutely. Regularly feel tired. Keep forgetting things. Like I am having heart attacks (Vietnamese carer, age 62 years).
Carers also reported having to advocate for the person living with dementia to access or maintain care, maintain their ability to participate in the community, and ensure positive social, emotional and health outcomes: It's all about respect. It’s been 3 and a half years since my husband (person living with dementia) has had a heart attack… He was unwell then, they wanted me to leave to go home without him, and it was the early days when he was really anxious, and I said well, I’m not leaving, and because I had good English skills and was able to communicate I could stay overnight. It was 11pm at night and his procedure was at 6 am so I could stay with him, just don’t tell anyone, and stayed at night (Arabic carer 1, age 60 years). Let me tell you about specialists, the ones who got it and the ones who were just completely blank. One of the nurses used to talk to me and ignore mum. So, with my hands and signals behind my mother's head to attract his eyes to get him to talk to mum (English former carer, age 67 years).
Environmental Enablers and Deterrents
Participants reported how the environment enabled or deterred activity in the community. The Arabic and Vietnamese groups often cited public transport issues, stating that buses were not regular and hard to navigate for people living with dementia: There is no transport, she used to drive up to 2 years ago, but she fell and broke her pelvis. I mean her dementia - she is still highly functional, but she has short term memory problems. So, I don’t want her driving, so she stopped driving two and a half years ago. But she had dementia before that, and public transport is too difficult for her. The girl that takes them out, the two girls they have cars, and they drive her. Sometimes they catch a ferry from manly and go to Cabrita from there (Arabic carer 4, age 54 years). My husband really loves it. The info sessions were used to be in Bankstown Library. When we came there, people spoke with us showed us some simple work out exercises then they gave us lunch. We really love it. But now they stop. No more funding. They ask me to go to Villawood. It’s too far for me. Also, there is no lift in Villawood station. How can we come there? Even I cannot go there, how can my husband come there? We cannot even go to the dentist. I asked them (service provider) to help me come there. They said they could not as they have only two hours. Bad service (Vietnamese carer 5, age 62 years).
Conversely, the English-speaking participants cited issues with the lack of disability parking: suppose it could be more like for instance, (to be able to do more activities) the place has got a bus that people can go out and do things on but it’s not catered for mum (English carer 5, age 63 years). Yeah, because the parking and the access for us so … you have to think about how we pick a physio or a pathology place. How we can drive over there and drop her off. She does have the disability sticker but it's, you know, with our mum, we could park close sometimes disability parking wasn't always free. At least there was a lift for access (English carer 6, age 63 years).
All three groups mentioned how: pavements were often uneven and unsafe to use for people living with dementia; lighting in buildings was typically insufficient; public spaces were, at times, excessively noisy; and places of interest were sometimes difficult to safely navigate. This theme was a source of stress for care-partners, as they had safety concerns for themselves and the person they cared for. Some care-partners cited that they themselves had fallen on uneven ground and were worried that the person they cared for would be injured: [Person living with dementia] is not that physical so it’s really, really important to have well laid paths. But it was a slow, slow, slow process. And I guess it was more than medical and locals and paramedics thoughtful people in the community. It became more and more important to bring the world into the house. But we in many ways lost touch (English former carer, age 67 years). so we go to the art museum in the city or the art museum. He likes to sit and watch but there aren’t many museums, he loves playing golf, things like that. Bowling is too noisy, it's not for him. Canterbury Bankstown is too noisy; they say they need to stimulate but it’s the other way around we need to do – de stimulate (Arabic carer 1, age 60 years). No, they (pavements) are not good. I and my mom bumped into the walking pavements many times. Luckily, I put seatbelts on for both, otherwise we would be badly injured (Vietnamese carer 2, age 72 years).
Culturally Specific Experiences of Arabic and Vietnamese Participants
This theme relates to the presence of culturally specific barriers and facilitators for Arabic and Vietnamese participants accessing social supports and the community. These included the sub-themes of language barriers and cultural understandings of dementia. Participants noted difficulties when navigating the community due to language and assimilation barriers, and this made connecting with community members more difficult. However, they did engage with groups that exclusively worked with their language group.
Language Barriers
Language barriers were stated as a hinderance for community engagement, with participants citing difficulties with translation and cultural assimilation: I can’t speak English well. For example, during the Covid pandemic, I wanted to buy groceries, but I could not do that. I don’t know how to use the internet. I lost my Woolworths loyalty card, but I could not have them issue a new card for me. They asked me to do it online…Businesses should provide more supports for people like me, especially the ones who cannot speak good English (Vietnamese carer 2, age 72 years). She hasn't known any road or street for the last seven years. She does not speak English, nothing. She depends on (me) completely. When shopping, she doesn’t know where to go. She can’t even cross the road (Vietnamese carer 1, age 59 years).
Community participation was aided by attending events or organisations that were culturally appropriate for the carer and the person living with dementia: I still try my best to join the Vietnamese group once a week, so mom also join the group once a week, same group. I take mom with me in the morning, and she comes home with me in the afternoon. I don’t leave her alone (Vietnamese carer 1, age 59 years).
Participants also described how cultural organisations can facilitate community engagement and the associated effects for people living with dementia: yeah. [Person living with dementia] will go shopping, they will go to the park, picnics, she goes organisation twice a week, coffee, zoo, shopping she does recreation as well... plus they would do Quran classes, and she used to go to Quran classes and then she fell, and she couldn’t go up the stairs. But she learnt to read the Quran (Arabic carer 4, age 54 years).
Cultural Communities’ Understandings of Dementia
Arabic and Vietnamese participants recounted instances of stigma within their own cultural community and its impact on community engagement.
Within the Arabic community, participants cited avoiding public spaces that specifically were populated by people from the same cultural background such as the local fruit shop, due to the scrutiny they might face: yeah, I was born in Brisbane and raised in Campsie and lived in Burwood my whole life, I know everybody, so I can’t walk outside on the street, I know everybody they know my husband, you know? Shopping centres, like everyone knows me and I can’t go with him because they roll his eyes, and I can’t send him out with the support worker, I can’t even send him out to Lakemba, I have to send them out to Miranda (Arabic carer 1, age 60 years). To me, Canterbury-Bankstown is a dementia village everyone knows each other except the fact no one is receptive, it’s an ideal situation (if people were receptive from the community) to be amongst Arabic community (Arabic carer 1, age 60 years).
Among some Vietnamese participants, community understandings of dementia impacted how they approached cultural participation. Participants recounted advocating for people with dementia within culturally specific social groups, and having to emphasise how the carer’s role is valuable in their cultural structure, and for the happiness of the person living with dementia. A lady in the… [Vietnamese] group is not too old but forgot a lot. Just say it, but she forgot right away. She only remembers the past. Her husband passed away a long, long time ago, (she) only talks about her husband. If you tell her something, she will forget it straight away. Few members got angry with her. I have to tell them, please understand, she has dementia. Otherwise, people get angry and shout loudly. We all need to understand and support each other. I do my work but also do community education. I feel for her. So here, in these activities, we need sympathy from surrounding people (Vietnamese carer 1, age 59 years).
Vietnamese Kinship Roles
Relative to the participants who were part of other cultural groups, some Vietnamese participants emphasised the carer role, viewing it as central to their identity. This impacted their access to the community as they valued full-time caring over their own need to engage with the community. This limited their activities to those that focused on the person living with dementia: A person with dementia should stay with family if they have one. The family must sacrifice so the patient can be comfortable and healthy. They can be healthy until they die… In caring for a person with dementia, a carer is the most important. The carer has to sacrifice so that the patient will be happy. The patient was happy till he died. So that is the most important thing. If we don't love and don't care, the patient will feel sad. Or if the patient lives with their children, they will never get this care. But if they live with someone who always cares and loves them, that is what makes them happy till they die. That is the most important thing, making the patient feel they are not our burden (Vietnamese carer 2, age 72 years).
A Culturally Inclusive Dementia Friendly Canterbury Bankstown
Participants were also asked for their suggestions for a dementia-friendly community intervention that would enable social participation. Suggestions were consistent across all groups and were compiled into seven separate categories and expanded on below.
More Accessible Transport Options
Suggestions included making public transport more accessible by increasing bus frequency and stop locations, and making train stations accessible with lifts. Transport officers should also be trained on dementia communication competencies.
Improving the Physical Environment to be Safe and Accessible
Suggestions included having smoother outdoor pavement, ramps in buildings that people with dementia may use, establishing quiet areas for rest, improving signage to assist with navigation, and making bathroom facilities safe and easy to use.
Local Dementia Support Groups that Cater to Diverse Care Needs
Participants expressed a need for more support groups operating in the area that catered to diverse care needs, such as groups that catered to younger participants and those in the later stages of dementia, had language support, and were culturally competent (e.g., gender matched groups).
Inclusive Social Groups and Activities
Participants recommended having recurring activities in the region for people with dementia and their carers to be able to socialise like crafts, gardening, picnics, and sensory walks. Existing social groups could be trained to be inclusive of people with dementia and advertised as such. Participants from the cultural groups emphasised having in-language activities too.
Dementia-Friendly Shopping Experiences
Suggestions around shopping centres included having noise free areas and a sensory time (or quiet hour) where people with dementia and their carers could get their shopping done without being overstimulated. Shopping staff should receive dementia and/or disability competency training; and there should be more disability parking spots.
Dementia Education and Training to Anybody that May Interact with People Impacted by Dementia
Education is needed to improve stigma and community interactions. Suggestions included training stakeholders that people with dementia and their carers come across in the community (e.g., support workers, allied health professionals, transport workers, shopkeepers, librarians, and the public).
Simplifying Access to Care Services
People impacted by dementia and their carers need help navigating the system and identifying appropriate support services. Having a checklist of supports that are typically used by people impacted by dementia, or a designated care navigator, could ease this process.
Discussion
This qualitative study established how community participation was hindered and facilitated among English, Arabic, and Vietnamese speaking people living with dementia and care-partners. The three groups experienced reduced community engagement after a dementia diagnosis, reflecting previous research (Hackett et al., 2019). This was influenced by community perceptions of dementia, family support (particularly through care-partners), transport availability, and environmental accessibility. The suggestions for a dementia-friendly community intervention aligned with established principles that aim to reduce stigma, promote social participation, and improve quality of life through education and environmental modifications (Hung et al., 2021; Shannon et al., 2019). However, as outlined by participants, these principles need to be used in a way that is inclusive and sensitive to diversity with respect to culture, language, age of onset, and disease stage i.e. not assuming everyone involved is at the same level.
Reduced social participation was worsened by negative perceptions of dementia in the general community and within their cultural groups – a recurring issue documented in prior research (Allam et al., 2023; Cheung et al., 2019). Culturally specific factors, such as language barriers and stigma, suggests that different cultural groups can experience dementia differently (Boughtwood et al., 2011). Care-partners described the need to shield their loved ones from social harm, often at the cost of reduced community participation. This finding mirrors previous studies highlighting isolation as a means of protecting reputation (Allam et al., 2023; Chejor et al., 2022; Gilbert et al., 2022; Nguyen et al., 2021).
Carers were also found to have a major role in enabling community participation for people living with dementia – this finding highlights the important role they have in maintaining activities and socialisation. People from culturally and linguistically diverse backgrounds prioritise their roles as carers and this was especially witnessed in the Vietnamese group (Nguyen et al., 2021; Xiao et al., 2015). Families offer a built-in support network for carers and people living with dementia to lean on for emotional support and enhance social wellbeing (Bressan et al., 2020).
Carers also advocated for people living with dementia in various contexts (e.g., community education and healthcare provision). Advocacy can contribute to confidence, wellbeing, and healthier relationships for the families of people living with dementia (Fetherstonhaugh et al., 2021; Weetch et al., 2021). However, community participation among people living with dementia can depend on the wellbeing of the main carer and their ability to prioritise and advocate for their loved one. The dyadic nature of the care relationship when it comes to social connections for people living with dementia should not be overlooked (Bressan et al., 2020). These findings highlight the need for carers to be included in the planning of dementia-friendly community initiatives, particularly for culturally and linguistically diverse people living with dementia who rely on their carers to communicate their desires, navigate the community, and access support (Gilbert et al., 2022). Although, it is important to have this level of commitment from carers, it can add to the physical and emotional strain they experience. As evidenced in our interviews, carers are neglecting their own wellbeing to support the person they are caring for. The presence of carer-specific skill building, self-care, and support groups within dementia-friendly community models can lessen the impact of this strain and reduce the risk of burnout (Adelman et al., 2014; Brodaty & Donkin, 2009). Future research and interventions should explore how to develop advocacy skills among carers and create initiatives that recognise the dyadic nature of social engagement for people living with dementia and their carers (Shannon et al., 2019).
Strategies to improve community participation encompassed social, physical infrastructure and service domains, reflecting previous research and reinforcing the ongoing nature of unmet needs (Hung et al., 2021; Shannon et al., 2019). Accessible transport for culturally and linguistically diverse people living with dementia is needed to overcome navigational, financial, and language barriers (Liu et al., 2022; Nelson & Rosenberg, 2022; Shannon et al., 2019). However, dementia-friendly transport would require considerable investment to upgrade signage at transport stops, city maps be made disability friendly, and personnel undergoing dementia education. The social improvements identified in the current study, such as inclusive community groups and activities, dementia support groups that cater to diverse care needs, and educating the public on dementia competent interactions, are less intensive and can be actioned more efficiently. These recommendations reflect a greater need to collaborate with culturally specific service providers to develop and deliver culturally or language specific initiatives (Shannon et al., 2019).
Methodological Limitations
This study is one of the first to directly partner with culturally and linguistically diverse populations for a dementia-friendly community intervention and is not without its limitations. First, there were no comparative measures of social isolation or mood scales across the three groups, so it was not possible to contextualise these issues regarding wellbeing. This case study reflects a unique geographical and demographic profile that might not be transferable to other populations. However, the methods used for engaging linguistically diverse people could be adapted for other under-represented groups. We also recommend a rigorous evaluation of the different dementia-friendly strategies taken not just to overcome these barriers but the extent to which they are making a difference to the daily life of culturally and linguistically diverse individuals with dementia and their families.
Conclusion
This study has shown that, while community engagement declines after a diagnosis of dementia, the barriers to continuing participation are addressable. People living with dementia and their care-partners are important sources of knowledge that need to be used to build effective interventions. It is important for researchers, service providers, and government funding bodies to involve their community members to gain an understanding of the issues they face and the solutions that can be put into place. Through a culturally inclusive research process, we have mapped out the needs of this community and identified strategies to improve community mobility and social participation. Importantly, these recommendations informed the action plan of the Canterbury Bankstown Dementia Alliance and community planning efforts of the local government.
Supplemental Material
Supplemental Material - “It Became More and More Important to Bring the World Into the House”: Exploring the Barriers and Facilitators to a Culturally Inclusive Dementia-Friendly Community
Supplemental Material for “It Became More and More Important to Bring the World Into the House”: Exploring the Barriers and Facilitators to a Culturally Inclusive Dementia-Friendly Community by Eman Shatnawi, Genevieve Z. Steiner-Lim, Gabriela E. Caballero, Irena Stojcevska, Thi Hang Vu, Nhan Ho Trong Pham, Nicky Morrison, Michelle DiGiacomo, Ann Dadich, Diana Karamacoska, and Canterbury Bankstown Dementia Alliance in Dementia
Footnotes
Ethical Consideration
Ethics approval for the study was received from the South Western Sydney Local Health District Human Research Ethics Committee (Reference: 2021/STE02281).
Consent to Participate
All volunteers provided written informed consent to participate.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Maridulu Budyari Gumal (SPHERE), ClubGRANTS NSW, Western Sydney University, and National Health and Medical Research Council (APP1195709).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: As a medical research institute, NICM receives research grants and donations from foundations, universities, government agencies, individuals, and industry. Sponsors and donors provide untied funding for work to advance the vision and mission of the Institute. The project that is the subject of this article was not undertaken as part of a contractual relationship with any organisation other than the funding declared.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, DK, upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.