
Abstract
People with dementia from culturally and linguistically diverse backgrounds often face poor health and social outcomes such as stigma, depression, and reduced help seeking behaviours. Dementia friendly communities have been shown to reduce stigma, and the gap in health and social outcomes for people impacted by dementia. Despite the large presence of established dementia friendly communities, their functioning in multicultural communities remains underexplored. The aim of this review was to identify the barriers and facilitators of cultural inclusivity to inform the development of a multicultural dementia friendly community. We systematically searched for academic and grey literature regarding existing and prospective age or dementia-friendly communities that engaged with culturally and linguistically diverse communities. Using the matrix method, data on the barriers and facilitators to engagement were extracted. Papers were analysed for common themes and findings were integrated in a narrative format. A total of 3,164 papers were identified, 11 of which met inclusion criteria. There were 6 dementia friendly communities in North America, 3 in Europe, 1 in Australia and 1 in Asia. Analyses revealed that barriers to cultural inclusivity were centered around the accessibility of services, sociocultural factors, and the environment, including issues such as low awareness of dementia and stigma, language barriers, isolation, and the inaccessibility of transport and buildings. Leveraging existing cultural leaders and social structures to target culturally and linguistically diverse populations and develop tailored dementia friendly initiatives were key facilitators. To foster cultural inclusivity in dementia friendly communities, a culturally specific lens that addresses these barriers and utilises facilitators must be applied from the design stage through to implementation and evaluation.
Introduction
Dementia is a syndrome associated with more than 100 different diseases and characterised by cognitive decline that impacts on functioning beyond what is expected from the normal process of ageing. Typically, dementia is associated with impairments in cognition and behaviour including memory, learning, language, judgement, and activities of daily living (Chertkow et al., 2013). People living with dementia often face social stigma leading to increased rates of loneliness and depression (Lion et al., 2015). Due to the common misconceptions surrounding dementia, a diagnosis can affect how friends, family and the community interact with the person diagnosed, often in a negative context (Herrmann et al., 2018). Social stigma around dementia often leads to perceptions and behaviours that the person is helpless and unable to make decisions or participate in the activities they were involved in previously (Lion et al., 2015; Rewerska-Juśko & Rejdak, 2020).
A practical initiative that seeks to support people with dementia and overcome misconceptions by building understanding, awareness and acceptance of dementia is a dementia friendly community. Dementia friendly communities were established with the aim of enabling people with dementia and their caregivers to feel empowered, supported and included in society (Lin, 2017; Lin & Lewis, 2015). The main characteristics of a dementia friendly community are to create a safe place where people with dementia can participate in community daily life, are able to access services and businesses, and feel valued and safe (Lin, 2017). The process of developing a dementia friendly community is enshrined in policy and planning that actively adopts a rights-based approach, recognising that people with dementia have a disability and are entitled to disability support (Shannon et al., 2019).
One objective of this initiative is to empower minorities within the dementia population such as individuals from culturally and linguistically diverse backgrounds. This is important given the rich cultural diversity in many countries, such as Australia, where 28% of people living with dementia were born in a non-English speaking country (Australian Institute of Health and Welfare, 2022). Culturally and linguistically diverse people with dementia remain a vulnerable and underserved cohort due to language barriers in dementia care, health literacy, and service delivery (Chang et al., 2019; Hohenberg et al., 2021; Sagbakken et al., 2018; Steiner et al., 2020). This is further complicated by the phenomenon where people with dementia from linguistically diverse backgrounds lose their ability to speak English and revert back to their first language (Tipping & Whiteside, 2015).
Stigma around mental health and dementia is also a common theme in this demographic, with carers and family members concealing and denying the diagnosis due to feelings of shame and embarrassment (Antelius & Kiwi, 2015; Cheung et al., 2019). Reluctance to acknowledge dementia as a neurological illness may lead to dementia being normalised as the natural progression of ageing (Adamson, 2001; Berisic & Nesvadba, 2008), which consequentially decreases diagnostic and treatment seeking behaviour (Lee et al., 2011; Mukadam et al., 2011).
Despite dementia friendly communities being a global initiative and present in many developed countries (Alzheimer’s Disease International, 2020), culturally or racially diverse groups are often misrepresented or excluded in the literature and in the operating models of current dementia friendly communities (Shannon et al., 2019). Therefore, to successfully develop a dementia friendly community that caters for a multicultural community, inclusive measures are needed to effectively tackle the barriers faced by culturally and linguistically diverse populations. The aim of this review was to explore global research on culturally and linguistically diverse participation in dementia friendly communities, and to identify facilitators and barriers for developing a culturally inclusive dementia friendly community intervention. The objective of this review was to generate practical insights for academics, policy makers, community organisations and health care professionals involved in the development and implementation of dementia friendly communities in multicultural contexts.
Positionality statement
Putting this research into context, our team works and resides across a highly multicultural region in Australia where a dementia friendly community is being established through the Canterbury Bankstown Dementia Alliance – a multisectoral collaboration involving diverse representatives from academia, industry, and the community. We position ourselves as advocates and allies for diversity, inclusion, and equity efforts particularly for the culturally and linguistically diverse members of our community who remain under-represented and under-serviced in this region. This is especially important to the lead researcher (DK), who was born into a non-English speaking immigrant family and has been supporting her grandmother (баба) through her dementia diagnosis and care for over 10 years. These personal experiences drive efforts to address the literacy gaps, inequities, and social impacts that many people living with, or at-risk of, dementia from diverse backgrounds face.
Methods
A systematic integrative literature review incorporating academic and grey literature was conducted to help conceptualise and evaluate the emerging topic of culturally inclusive dementia friendly communities. Integrative reviews involve summarising both experimental and non-experimental literature using a comprehensive method such as a matrix to build a cohesive understanding of a topic area (Whittemore & Knafl, 2005). Torraco's (2016) rigorous review process was used to develop a defined search strategy and appraisal of the identified articles, followed by an analysis and qualitative synthesis of the findings.
Terminology
The two major search terms used for this study were Dementia Friendly Community and Culturally and Linguistically Diverse populations/people. The definition for dementia friendly communities was taken from Dementia Australia (2020), defined as “a place where people with dementia are supported to live a high quality of life, with meaning, purpose and value” and Alzheimer’s Disease International (2011) “a social and physical environment that fosters community participation and promotes the autonomy of people with dementia ultimately improving their quality of life.” The definition of culturally and linguistically diverse was taken from the Australian Bureau of Statistics and is used to refer to “populations that originate from countries in which English is not the mainstream language and/or cultural norms and values differ from mainstream populations” (Australian Bureau of Statistics, 1999). Other commonly used terms to describe ethnically diverse groups were used in the search. These were Black, Asian, and Minority Ethnic (BAME) and Black and Indigenous People of Colour (BIPOC). BAME is commonly used in the UK research context “referring to people in the UK who do not consider themselves to be White” (Office for National Statistics UK, 2021). We recognise that the UK government recommended discontinuing the term’s use in March 2021, however, it was retained in our search of the literature to capture articles published prior to this date. BIPOC is commonly used in North American research to refer to Black and Indigenous People of colour (Andrasik et al., 2021).
Search strategy
An extensive search in PubMed and EBSCO (indexing CINAHL with Medline, PsychInfo, Health Source Nursing/Academic Edition, APA PsycArticles, Open Dissertations) was conducted from 20 August to 5 September 2021. The Population Intervention Context Outcome framework was used to identify relevant studies (Schardt et al., 2007); with the outcome term omitted as the integrative review was inclusive of both prospective and established dementia friendly communities. The following key words were included in the search strategy:
Population:
• Culturally and Linguistically Diverse (CALD) • Migrants • Ethnic Minorities • Multilingual • Bilingual • Ethnicity • Diversity • Black, Asian, and Minority Ethnic (BAME) • Black and Indigenous Person of Colour (BIPOC)
Intervention:
• Dementia friendly community (DFC) • Dementia-Friendly City • Dementia-Friendly Community • Dementia Action • Dementia-Capable Community • Dementia-Friendliness • Dementia AND Social Inclusion • Age Friendly Community
Context:
Prospective or existing dementia friendly communities
A grey literature search of the keywords was also conducted in Google, Google Scholar, and Grey Matters. Grey literature is defined as information published at all levels of government, academia, business and industry in formats that are not controlled by commercial publishing avenues and organisations where publishing is not the primary activity (Adams et al., 2016). Examples of grey literature include conference proceedings, technical reports, government documents, patents, white papers etc.
Eligibility
Selection was a three-stage process with titles being assessed first for relevance, followed by abstracts, and full text readings of identified articles by two authors. No limitations were placed on study design, quality, or location. To meet the aims of this review, articles were assessed on the following eligibility criteria:
Inclusion criteria:
• Refer to an existing or prospective dementia friendly communities • Include people from culturally and linguistically diverse and/or multilingual backgrounds.
Exclusion criteria:
• Theoretical, editorial, or discussion papers • Secondary analyses • Articles not published in English • No demographic information pertaining to participants’ cultural or ethnic background provided.
Data analysis
The matrix method described by Garrard (2020) was used to extract, summarise and analyse the data. After screening, articles were condensed into a review matrix where the following data were extracted: author, title, year and country, type of document, study aims, prospective or existing dementia friendly community, data collection design, and participant characteristics including representation of people affected by dementia, their cultural backgrounds and age range. The barriers, facilitators, and/or implications were also extracted in paraphrased format (see Table 1).
The authors identified barriers as issues or existing phenomena in place that prevented or made it difficult for culturally and linguistically diverse people to engage with a dementia friendly community (either prospectively during the design phase or retrospectively within an existing initiative). The barriers can be experienced by culturally and linguistically diverse people with dementia, caregivers, stakeholders and/or service providers, community members, and researchers. An example of this would be a dementia friendly community only utilising materials in English whilst operating within a multilingual community. Facilitators were identified as any recommendations or strategies that would increase engagement with the community and address the barriers identified. Strategies that were reported to have been implemented by a dementia friendly community were considered facilitators, whilst any recommendations for strategies were considered implications. An example of this could be a recommendation that language specific resources be created and distributed to increase engagement with their service.
The extraction process was conducted by two authors and any disagreements were resolved through discussion. Barriers and facilitators/implications were thematically analysed in an iterative format. Overarching themes from the barriers and facilitators were extracted and the occurrence of each theme in each article was recorded and collated (see Tables 2 and 3).
Results
Search outcome
The search process and selection of articles was guided by the preferred reporting standards for systematic reviews framework (Page et al., 2021), as shown in Figure 1. PRISMA flow diagram of search and selection process.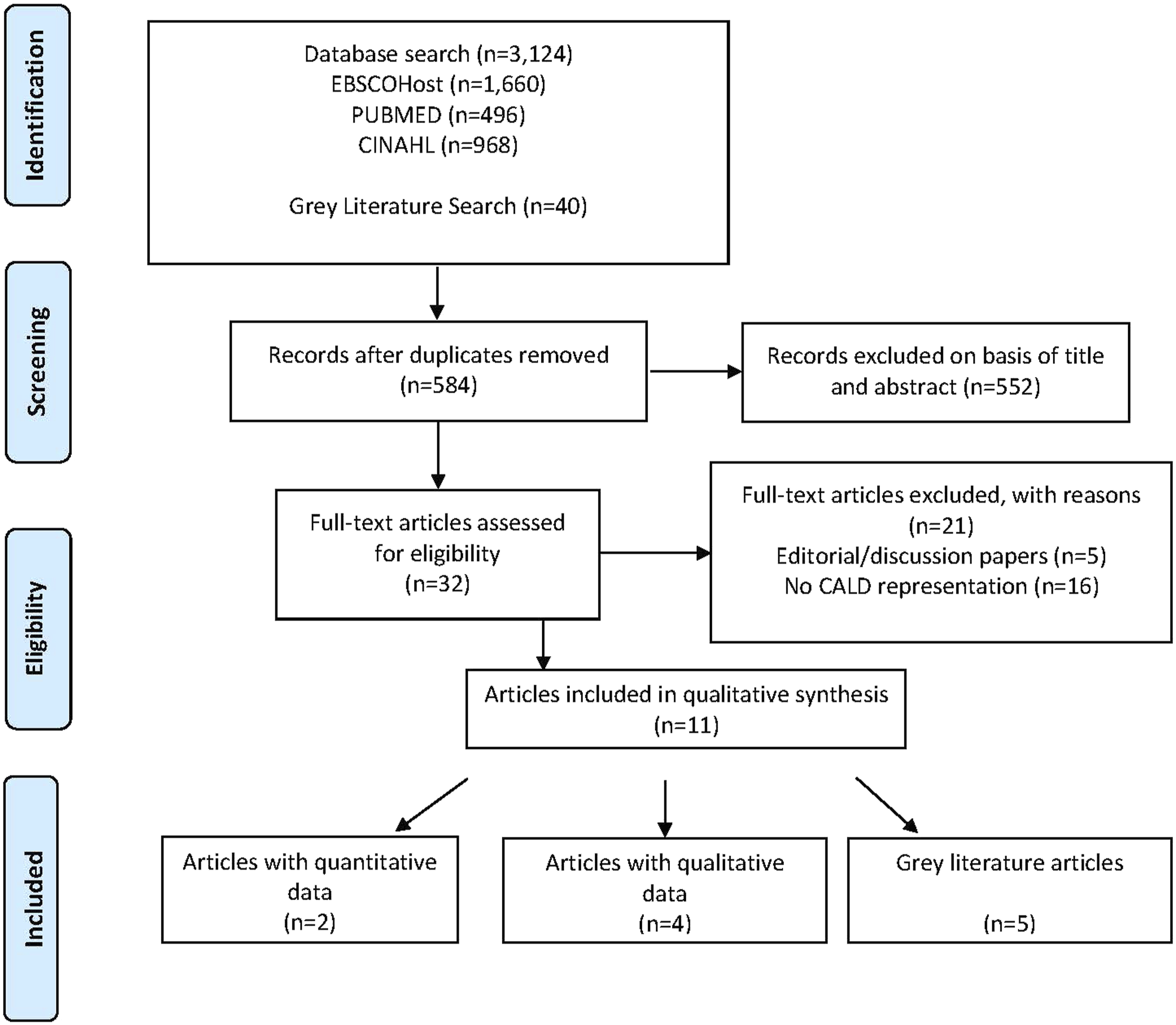
Study characteristics
Dementia friendly community study characteristics and the barriers and facilitators to cultural inclusivity within each study.
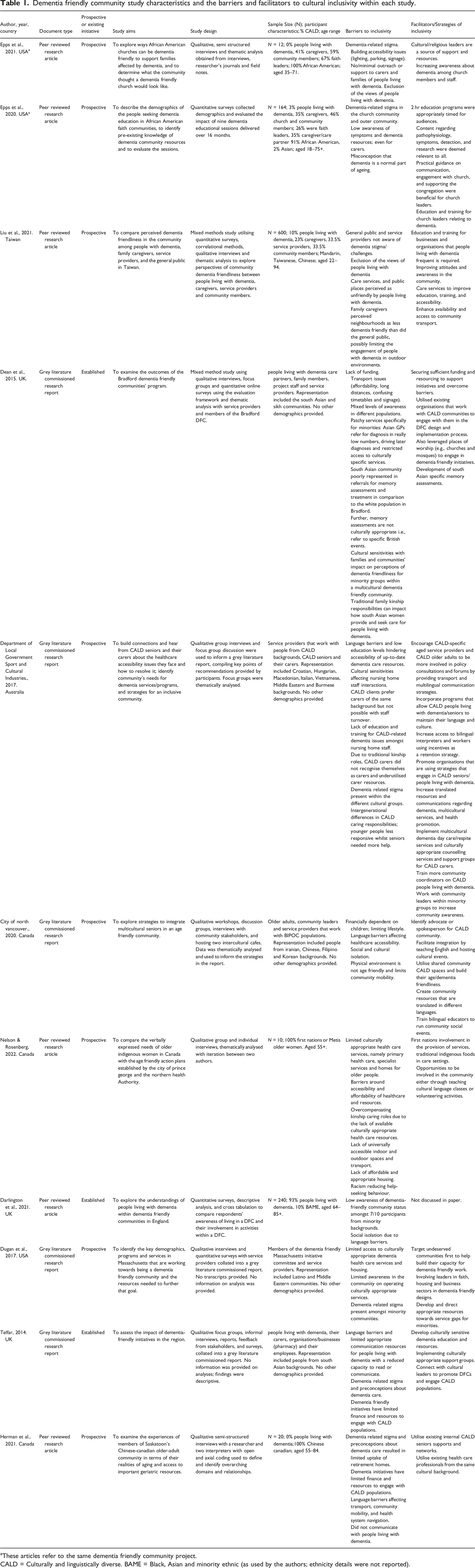
aThese articles refer to the same dementia friendly community project.
CALD = Culturally and linguistically diverse. BAME = Black, Asian and minority ethnic (as used by the authors; ethnicity details were not reported).
Barriers to cultural inclusivity
Barriers to CALD engagement within dementia friendly communities.
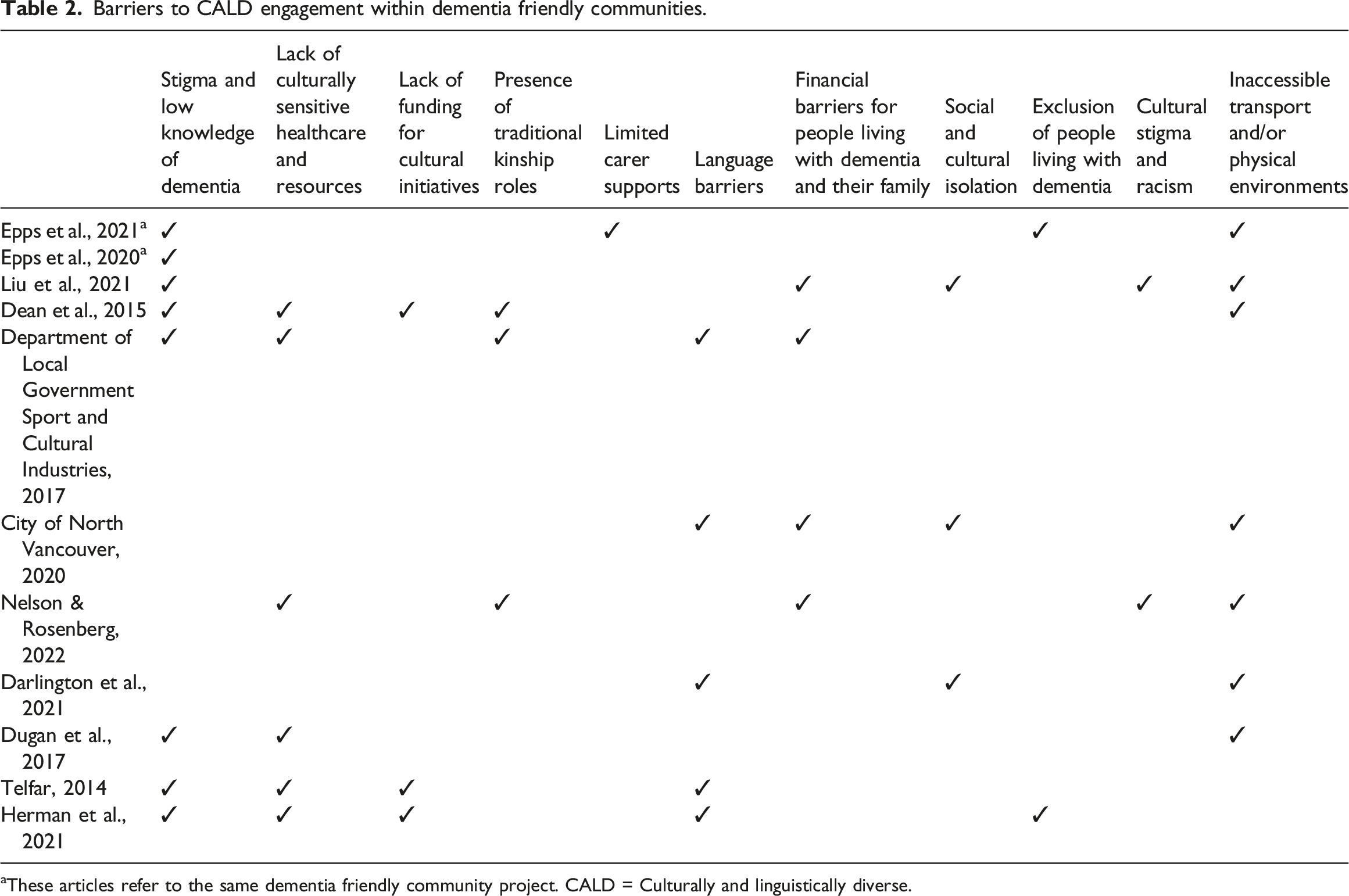
These articles refer to the same dementia friendly community project. CALD = Culturally and linguistically diverse.
Facilitators of cultural inclusivity
Facilitators to CALD engagement with dementia friendly communities.
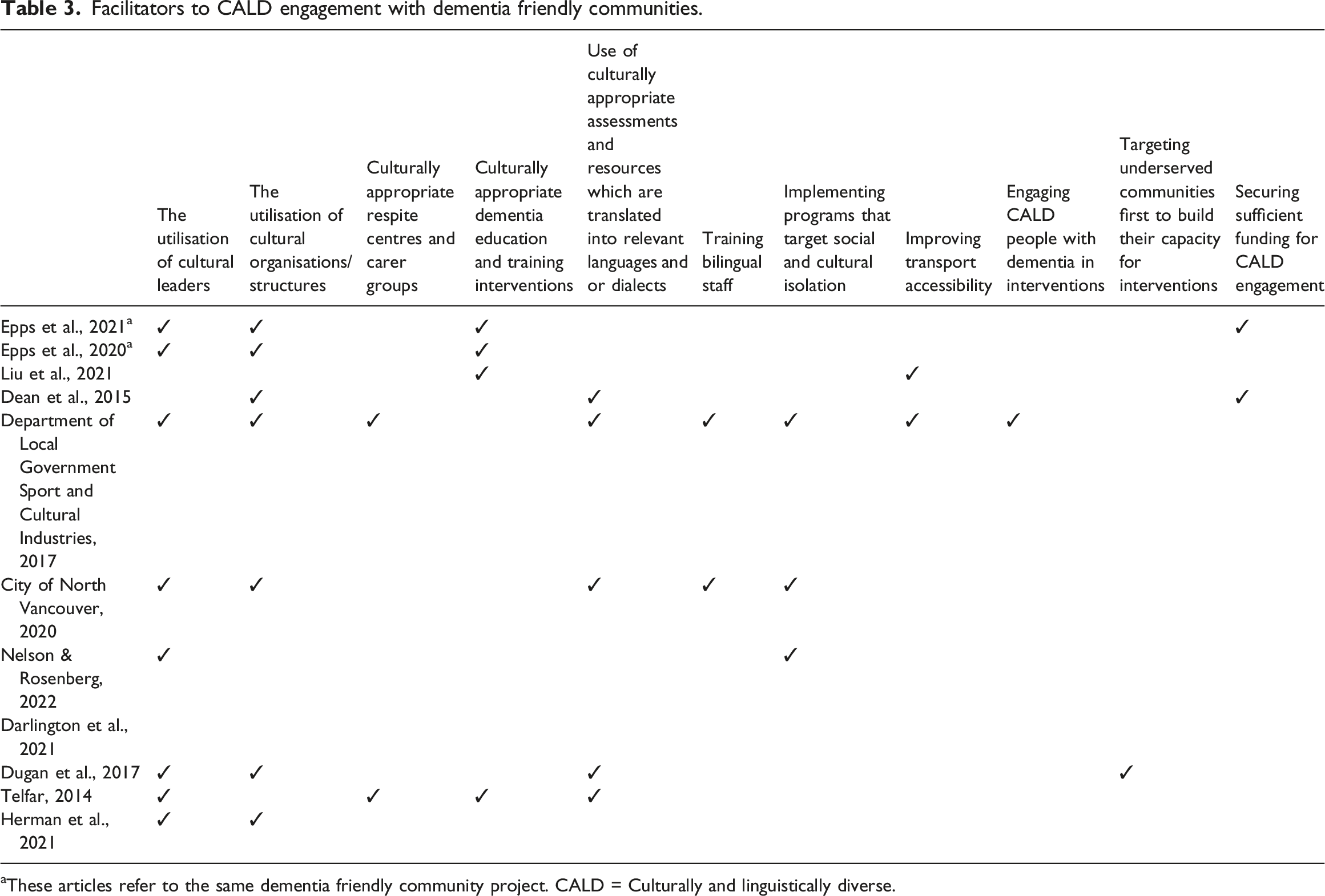
aThese articles refer to the same dementia friendly community project. CALD = Culturally and linguistically diverse.
Discussion
This paper explored factors negatively and positively affecting cultural inclusivity in dementia friendly communities and associated initiatives. The most common barriers included low dementia literacy, stigma, lack of culturally sensitive healthcare and resources, language barriers, environmental inaccessibility and traditional kinship roles. Leveraging existing cultural leaders and social structures to target culturally and linguistically diverse populations and develop tailored initiatives were key facilitators. These barriers and facilitators to inclusivity align with typical dementia friendly community designs, principles, and outcomes set out by Alzheimer’s Disease International (2011): increasing dementia literacy in community and care settings, promoting social engagement for people with dementia, and increasing community participation. In the context of dementia in multicultural communities, facilitators need to be designed and implemented with a culturally appropriate lens.
Combating dementia illiteracy, stigma, and isolation requires culturally appropriate education programs for the wider community, people impacted by dementia, and service providers. Engaging with local community hubs frequented by culturally and linguistically diverse populations, such as churches and community centres, enabled this (see Epps et al., 2020 for an example). This strategy has been found to be effective in other community-based health education interventions, as people from culturally and linguistically diverse backgrounds tend to build their own enclaves and community spaces that are deemed safe and accessible to members of that cultural group (Forrest et al., 2006; Ndwiga, 2021).
Embedding culturally relevant support groups for people impacted by dementia within existing sociocultural structures offers opportunities for social and civic engagement (Bank et al., 2006; Chien et al., 2011; Department of Local Government, Sport & Cultural Industries, 2017; Mason et al., 2005; Telfar, 2014). Culturally relevant groups are a natural way for people with dementia to still engage with their culture, have culturally appropriate food and activities, and interact with people from the same cultural background. This combination of factors can help a person with dementia feel more integrated with their community, engage with their culture in a meaningful way, and participate in social interactions that they might have missed out on due to cultural barriers, helping to mitigate potential social isolation and loneliness (Heward et al., 2016; Napoles et al., 2010; Shanley et al., 2012). In terms of dementia friendly communities, a culturally specific support group can potentially serve as an impromptu focus group to allow people affected by dementia to voice their opinions on the development of a dementia friendly community and ensure it meets their needs.
Increasing the capabilities of health and care services to provide culturally specific care is necessary as language barriers, lack of bilingual staff, and staff spending less time with people who did not speak the same language were barriers for culturally and linguistically diverse people living with dementia (City of North Vancouver, 2020; Darlington et al., 2021; Department of Local Government, Sport and Cultural Industries, 2017; Herman et al., 2021; Telfar 2014). Traditional kinship and caregiving roles within families also impacted engagement with support services (Dean et al., 2015; Department of Local; Government, Sport and Cultural Industries, 2017; Nelson & Rosenberg, 2022). As evidenced in the Bradford, United Kingdom dementia friendly community, cultural roles that emphasise the need for women to take on traditional caregiving roles for someone with dementia can impact when and how they seek help (Dean et al., 2015), which can perpetuate reduced help-seeking and isolation (Fanany et al., 2013). Further compounding this issue, staff training for issues faced by culturally and linguistically diverse people living with dementia has been reported as scarce in mainstream health and social services in multicultural locations (Dean et al., 2015; Department of Local Government, Sport and Cultural Industries, 2017). There is a clear need for training bilingual staff, developing culturally appropriate assessments, and securing funding, specifically for cultural health initiatives (Epps et al., 2021; Liu et al., 2021; Telfar, 2014).
Cultural competency has been established as a key strategy in reducing health care inequities and improving the quality of care for culturally and linguistically diverse populations (Steiner et al., 2021). For cultural competence to be effective, it needs to be more than just raising cultural awareness for existing services. It should be embedded in the operations, knowledge, awareness, behaviour, skills, and attitudes at all levels of service delivery (Harrison et al., 2019). Active community participation through consultation with key community leaders, culturally and linguistically diverse people with dementia, and bilingual health care workers was key to fostering cultural inclusivity in dementia friendly communities as it facilitated knowledge exchange and awareness raising between peers rather than service-based information from professionals (City of North Vancouver, 2020; Dean et al., 2015; Epps et al., 2020). Engagement and participation with culturally and linguistically diverse groups, particularly in the design of services and initiatives, can promote and build cultural competencies across multiple layers of the community.
Our review found that community participation by culturally and linguistically diverse people with dementia was impeded by linguistic, financial, and environmental barriers (City of North Vancouver, 2020; Department of Local Government, Sport and Cultural Industries, 2017; Liu et al., 2021; Nelson & Rosenberg, 2022). Many culturally and linguistically diverse people living in dementia friendly communities were not aware of such initiatives due to information not being translated (Darlington et al., 2021). Language barriers, unaffordability, and dementia unfriendliness also contribute to inaccessible transport and cultural/social isolation in the community (City of North Vancouver, 2020; Dean et al., 2015; Giebel et al., 2015; Hauger et al., 2019; Nelson & Rosenberg, 2022; Risser et al., 2015; Telfar, 2014). However, it is important to note that access was complicated by unique financial issues and language barriers reported by culturally and linguistically diverse populations, and not specifically stemming from a diagnosis of dementia as caregivers also struggled to access resources due to previously held barriers (Hauger et al., 2019; Khatri & Assefa, 2022; Risser et al., 2015; Shanley et al., 2012). Facilitators to improving accessibility and community participation included recommendations to design transport initiatives targeting isolation, using resources that were language and culturally appropriate, and ensuring funding for transport use (Dean et al., 2015; Department of Local Government, Sport and Cultural Industries, 2017; Liu et al., 2021; Nelson & Rosenberg, 2022). It should be noted that although this strategy, amongst others, was recommended in several prospective studies, it appears that it has not yet been implemented, or at least disseminated through publication.
Considering the increased barriers that culturally and linguistically diverse people face when accessing dementia care, interventions with diverse populations should consider additional strategies that act as facilitators to the common barriers. This can include having the option to engage in intervention activities with a bilingual worker or interpreter and through telephone and online video conferencing for people who are limited by financial and transport barriers and/or creating audio-visual advertising material, resources, and science communications that do not rely solely on reading skills for populations that face literacy issues both in English and their main language (Boughtwood et al., 2012). Lastly, it is important to consider the cultural appropriateness of the material being distributed, for example by reflecting on whether the use of the word dementia is stigmatising in the population being targeted, which can result in materials being confronting rather than engaging (Boughtwood et al., 2012).
Limitations
Despite a systematic and comprehensive search strategy for academic and grey literature, there is the potential that not all the literature was identified. Restricting publications to the English language may have excluded relevant articles from other languages. Having said this, cultural inclusivity in dementia friendly communities is an emerging area of interest, with all included articles published within the last 8 years. Barriers and facilitators were spread out across the studies, with some factors repeated and some standing alone. Further research exploring the implementation of facilitators is needed to determine their impact and value. We acknowledge that our definition of facilitators also included strategies or recommendations for engagement that were proposed by authors but had not been implemented or evaluated. It remains unknown to what extent these facilitators would help (or possibly hinder) this process. Ideally, an inclusive dementia friendly community addresses as many barriers as possible to facilitate the effective engagement of people living with dementia from culturally and linguistically diverse backgrounds. The quality of studies was also not assessable here due to the limited and varied reporting of methods. As the literature base continues to develop, more thorough reviews will be possible.
Conclusion
The barriers and facilitators to cultural inclusivity in dementia initiatives align with internationally recognised dementia friendly community design and outcome principles. Diversity and equity considerations are often an afterthought in mainstream dementia initiatives. It is important for interventions, researchers, and/or organisations to adopt an ‘inclusivity-first’ approach from the outset and throughout. This does require greater funding, time, and resourcing particularly from granting bodies, dementia charities, advocacy groups, and academic institutes. Facilitators need to be designed and implemented with a culturally appropriate, competent, and inclusive lens. A culturally inclusive dementia friendly community would ideally incorporate principles of cultural competency from the initial planning stages all the way to outcome and implementation, and actively involve culturally and linguistically diverse community stakeholders, people living with dementia, their caregivers, and health care professionals/service providers in all stages of the initiative (Wu et al., 2019). These multisectoral partnerships leverage the unique experiences, resources, personnel, networks, and skills of all involved, which can bolster funding applications, implementation success, and advocacy efforts. Together, this would activate, enable, and empower the culturally and linguistically diverse person living with dementia to fully realise their constructive and meaningful participation in the community.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Maridulu Budyari Gumal, National Health and Medical Research Council, APP1195709.