
Abstract
Background
The global incidence of dementia is increasing, establishing it as a significant cause of disability and diminished quality of life. The World Health Organization underscores the necessity of enhancing the well-being of individuals with dementia and their caregivers. Research has indicated that art-based interventions can improve cognitive functions and overall quality of life. This pilot study aimed to evaluate the impact of a museum-based intervention program on the well-being (quality of life, depression, and mood) of individuals with mild-to-moderate cognitive impairment (MCI-moderate), which may indicate early to moderate stages of dementia that was not formally diagnosed.
Methods
We recruited 29 participants with MCI-moderate (median MoCA score: 22). The intervention group consisted of 16 individuals (11 females, 5 males; mean age 83.5 years) who attended sessions at an art museum in Israel every once a week from March to April 2023. Thirteen age-matched individuals formed the control group, which did not participate in the museum program. Measures of well-being were assessed before and after the intervention, along with collecting participants’ feedback. Well-being changes within and between-groups were analyzed using mixed model analysis of variance. Effect sizes were also calculated.
Results
The intervention group showed significant improvements in quality of life with large effect sizes in all domains, and a significant reduction in depression symptoms; the control group experienced non-significant changes. Additionally, mood significantly improved following museum activities. Most participants positively reviewed the program, with a significant majority reporting enhanced mood (81.2%) and a strong intention to recommend it (93.7%); 62.5% expressed a desire for future participation.
Conclusions
Our findings suggest that art interventions, such as museum programs, can significantly boost well-being in people with MCI-moderate, suggesting further exploration of the specific elements of such programs and their long-lasting effects.
Introduction
Dementia, a neurodegenerative condition characterized by a decline in cognitive abilities, including attention, memory, and social cognition, poses a significant global health challenge (Livingston et al., 2017). Dementia predominantly affects individuals over the age of 65 (Chen et al., 2023; Livingston et al., 2017). With global dementia cases expected to increase from 47 million in 2015 to 139 million by 2050, dementia is becoming a leading cause of disability that also incurs substantial economic costs (World Health Organization, 2017). In Israel, dementia estimates range from 106,650 to 150,000 and are projected to reach 270,000 by 2050, highlighting the critical need for effective care and support strategies for patients and their families (Bentur & Sternberg, 2019).
With no cure for dementia and current treatments only slowing its progression (Raina et al., 2008), it is vital to move beyond narratives of despair, exploring new perspectives to better understand and address the disease (Zeilig, 2014). Focusing on the social and psychological well-being of those with dementia is crucial (Beard, 2012). The WHO’s 2017–2025 Global Action Plan emphasizes enhancing well-being and developing person-centered, cost-effective care strategies for individuals with dementia, their families, and caregivers (World Health Organization, 2017, 2021). Research underscores the positive impact of creative support on mental health across patient populations, advocating for their integration into health and social care (Fancourt & Finn, 2019; Regev & Cohen-Yatziv, 2018; Reynolds et al., 2000; Slayton et al., 2010; World Health Organization, 2019).
By drawing on the existing cultural capital of older adults and enriching it through participation in museum programs, these activities have the potential to significantly enhance the well-being of the elderly (Bourdieu, 2011). Art galleries and museums are increasingly recognized for their mental health programs (Letrondo et al., 2023; Shaer et al., 2008), offering significant benefits for dementia patients, whose aesthetic appreciation remains intact despite neurological decline (Halpern et al., 2008; Stewart, 2004). Such engagement not only supports patient and caregiver social and psychological well-being by boosting confidence and social interaction (Kinney & Rentz, 2005; MacPherson et al., 2009) but also positively impacts health outcomes over time (Gordon-Nesbitt, 2015). Research has consistently demonstrated the efficacy of art interventions in enhancing well-being, cognitive function, and communication among those with dementia (De Medeiros & Basting, 2014; Letrondo et al., 2023; Salisbury et al., 2011; Young et al., 2016; Zeilig et al., 2014).
Camic et al. (2014) examined an 8-week art viewing and making program for individuals with mild to moderate dementia and their caregivers using a mixed-methods pre-post design. While quantitative well-being metrics showed no significant changes, qualitative feedback revealed enhanced social interaction, enjoyment, confidence, and cognitive engagement, with some participants reporting improved memory and learning. MacPherson et al. (2009) studied a six-week art program at the National Gallery of Australia with 15 dementia patients. Behavioral observations showed that 84.4% of participants were engaged during the sessions, while qualitative findings highlighted improved social interaction, enjoyment, and new learning. Staff also noted enhanced communication and liveliness among withdrawn participants after visits. (Camic et al., 2014; MacPherson et al., 2009).
In additional studies, Eekelaar et al. (2012) and Young et al. (2016) have highlighted the importance of integrating thematic art content with interactive strategies, enriching learning, fostering meaningful discussions, and enhancing cognitive and emotional well-being in individuals with dementia (Eekelaar et al., 2012; Young et al., 2016).
The “Meet Me” program, initiated in 2006 at the Museum of Modern Art in New York, was a pioneering effort to engage individuals with dementia in art, offering monthly themed tours to discuss artwork. This program has achieved notable improvements in participants’ self-esteem, mood, and well-being (Rosenberg, 2009). Inspired by The Alzheimer’s Association of Israel which created a similar museum program and introduced “In the Armchair with Picasso” for home-based art activities, although the effectiveness of these initiatives remains to be evaluated (Alzheimer’s Disease, 2012).
This pilot study used a pre-post intervention-control design to evaluate a museum-based program in Israel for older adults with mild to moderate cognitive impairment. Aiming to fill a gap in dementia care, the study seeks to provide evidence for expanding the program and improving the quality of life for individuals with cognitive impairments.
The initiative, the first of its kind in Israel, involved sessions in a museum tailored to Holocaust survivors from a Russian-speaking community, emphasizing the participants’ cultural background. This unique focus highlights the importance and feasibility of implementing diverse forms of support for older adults from various demographic and cultural groups living in Israel. The study underscores how culturally sensitive interventions can enhance well-being across different populations, offering a model for inclusive dementia care.
This study tested five hypotheses: (H1) the museum program improves quality of life; (H2) it reduces depressive symptoms; (H3) age and cognitive performance (via Montreal Cognitive Assessment [MoCA] correlate with post-intervention quality of life; (H4) participants experience mood enhancement; and (H5) linguistic or communication skills improve after participation.
Materials and methods
Participants
The participants were Russian-speaking members of a support community for Holocaust survivors (‘Matav’) with mild to moderate cognitive impairment, living in the city of Ariel. They were recruited by Matav with the support of the Ariel municipality, through direct invitations during community events for Holocaust survivors. The inclusion criterion was the presence of mild to moderate cognitive impairment, based on the results of a screening using the Russian-language version of the MoCA test (Freud et al., 2020), which differentiates stages of cognitive impairment and can indicate early signs of dementia. In this pilot study, we use the term ‘mild to moderate cognitive impairment’ rather than a definitive diagnosis of dementia, as we did not have access to participants’ medical records. Recruitment was based on the MoCA screening.
Procedure
In February 2023, during an Ariel municipality event for older adults, we introduced the planned museum program. From 38 attendees, 29 with mild to moderate cognitive impairments (per MoCA testing) were identified. Twenty-nine participants were randomly assigned to the pilot’s intervention (n = 16) or control (n = 13) groups using a single-blinded process, while the remaining individuals were placed on a waiting list for future sessions. Figure 1 outlines the screening process and study stages. Summary of methods used at different intervention stages.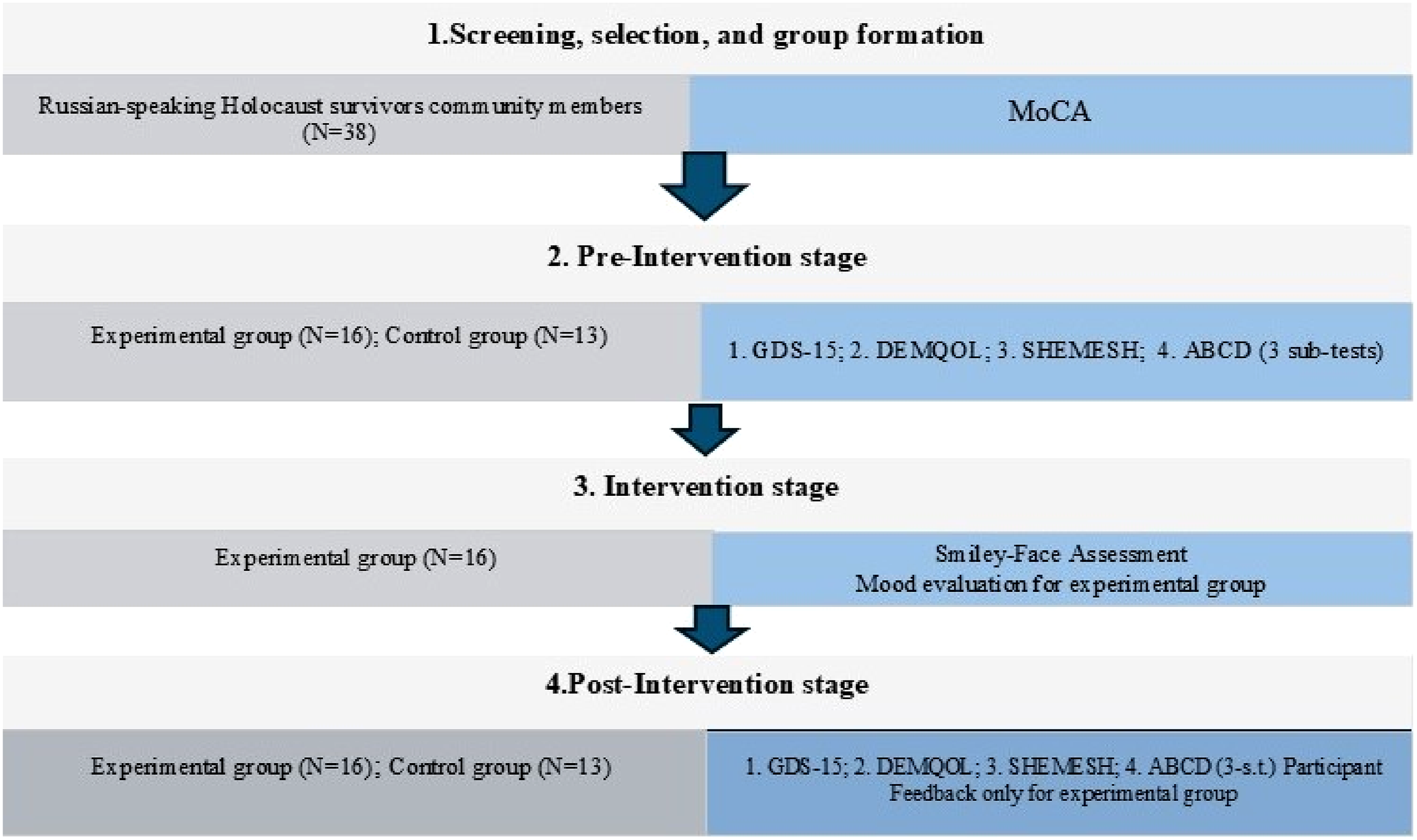
We arranged home visits for pre-intervention assessments for both groups, prioritizing participants’ comfort to ensure more accurate responses and considering their needs and preferences. In March and April 2023, participants in the experimental group attended three scheduled museum visits at the Ralli Museum in Caesarea, which took place once a week. They were greeted by staff and organizers and given time to rest after their journey, which took approximately an hour and a half, depending on traffic conditions. For convenience, the bus made several stops in the city to pick up participants, taking an additional 15 minutes. All sessions began at 11:00 AM, and participants were asked to rate their mood using the Smiley-Face Assessment Scale before and after each visit. All experimental group members attended every meeting. Post-intervention, we conducted home visits for both groups to evaluate outcomes using consistent assessment methods.
Intervention
We developed the project in collaboration with the Ralli Museum in Caesarea and the Ariel Municipality, focusing on: (1) Training with a professional museum guide; (2) Designing program content and structure; (3) Optimizing scheduling, routes, and logistics for accessibility and safety; (4) Organizing transportation from Ariel to the museum; and (5) Procuring necessary materials and equipment. The program, which consisted of three sessions, was co-designed with a museum educator and informed by international practices and guidelines for engaging older adults with dementia (Belver & Hernández, 2019; MacPherson et al., 2009; Rosenberg, 2009; Schall et al., 2017; WHO, 2019).
In this pilot study, the intervention took place at the Ralli Museum, known for its collection of classical and contemporary art, including paintings and sculptures. The criteria for selecting this museum included its accessibility; the suitability of the environment for older adults; the supportive atmosphere; and convenient logistics, ensuring a relatively quick and comfortable journey for participants. Additionally, the museum’s management demonstrated strong interest in supporting the project, which facilitated the organization of the sessions. The museum’s collection, featuring visual art and sculptures, was particularly well-suited to the themes of the intervention, providing an ideal setting for participants to engage with art in a culturally rich environment.
The entire cycle of meetings was united by a cross-cutting theme related to health promotion and a healthy lifestyle. In this regard, each of the three meetings had its own theme and a corresponding set of exhibits. Each meeting lasted an hour and a half and consisted of several elements: • Storytelling and Discussion: Facilitators introduced each piece of art, sharing its history and key features, and encouraged participants to inquire further. Discussions were sparked by prepared questions tailored to each exhibit, aiming to deepen cognitive engagement and emotional insight. • Animating Exhibits: In this interactive segment, participants engaged in two activities. First, they physically replicated poses of sculptures, bringing the artwork to life. Participants and observers added imaginative elements and expanded the meaning of the sculptures through active discussion and embodiment. The second activity involved easels with prepared paintings similar to museum exhibits. These duplicates had movable key elements, allowing participants to rearrange them and discuss the artwork’s composition. Both methods aimed to make interaction with the artwork active, imaginative, and dynamic. Evidence has shown that active engagement with the arts, including embodied participation and creative reinterpretation, can significantly enhance well-being by fostering emotional involvement, social interaction, and cognitive engagement, ultimately improving the quality of life for older adults (Groot et al., 2021; World Health Organization, 2019). • Drawing: Participants were given the freedom to use tablets, paper, pastels, and charcoal to draw images inspired by the session’s themes or specific prompts from the facilitator. This activity was designed as a creative outlet for personal expression and as a method to reinforce the learning experience, helping participants to consolidate their cognitive gains and reflections on the discussed themes.
The following themes were selected for each museum meeting: (1) Bounty and nourishment: Healthy nutrition; (2) Shadow and light: Sleep and wakefulness; and (3) Motion and movement: Physical activity. The incorporation of these selected themes into the museum meetings, rooted in an analysis of the most popular topics for discussion and used in organizing events for members of the targeted community, crafted an integrated educational journey. The intervention was designed to integrate art and health in a supportive, engaging environment for older adults. By leveraging the strengths of visual and participatory learning, we aimed to cultivate a profound comprehension of and connection to behaviors conducive to health. Our choice of themes related to healthy living—nutrition, sleep, and physical activity—was intentionally aligned with the interests and experiences of our participants, thereby ensuring the program’s relevance and impact.
Although participants did not report any special vision problems when selecting paintings, we paid attention to the fact that they were large enough, high-contrast, and properly positioned on the wall or floor. When selecting exhibits for the program, we avoided disturbing images with themes of war and violence.
Design and outcome measures
We analyzed data from older adults with mild to moderate cognitive impairment in a randomized study. Standardized tests and questionnaires were used to assess outcomes immediately before the intervention started and soon after it concluded.
We screened participants for cognitive impairment using the Russian version of the Montreal Cognitive Assessment (MoCA, 0–30). Scores of 26–30 indicate normal cognition, 18–25 indicate mild cognitive impairment, 10–17 indicate moderate cognitive impairment, and a score below 10 indicates severe impairment. Validated for Russian speakers (Freud et al., 2020), the MoCA ensures reliability in this context. (Freud et al., 2020; Nasreddine et al., 2005).
Depressive symptoms were measured using the 15-item Geriatric Depression Scale (GDS-15, Yesavage & Sheikh, 1986), with scores of 0–5 indicating normal mood, 6–10 indicating mild depression, and 11–15 indicating moderate to severe depression. The validated Russian-language version ensured cultural and linguistic appropriateness for our analysis (Yesavage & Sheikh, 1986).
The quality of life of the participants was evaluated using the Russian adaptation of the 29-item DEMQOL questionnaire (Gavrilova et al., 2009; Smith et al., 2005), which assesses aspects of feelings, memory, and everyday life. Using a four-point Likert scale (1 = ‘a lot' to 4 = ‘not at all'), the overall score range of this tool extends from 28 to 112, with detailed subscale scores ranging from 13 to 52 for feelings, from 6 to 24 for memory, and from 9 to 36 for everyday life.
In our research, we utilized the Smiley-Face Assessment Scale to quantify participants’ mood changes, employing a 1-5 scale: 1 for very sad, 2 for a little sad, 3 for neutral, 4 for a little happy, and 5 for joyful. This assessment was administered before and after museum visits to gauge the emotional impact, with higher scores indicating improved mood (Rosenberg et al., 2009).
Participants’ primary communication abilities were assessed during the screening meeting using the immediate and delayed story recall sub-test and object description sub-test from The Arizona Battery for Communication Disorders of Dementia (Bayles & Tomoeda, 1993; Biran & Friedmann, 2005).
Verbal retrieval abilities were assessed pre- and post-intervention using the SHEMESH naming test (Biran & Friedmann, 2004). To avoid fatigue and potential learning effects when using all the pictures pre- and post- intervention, we divided the pictures into two parts: part A included items 1 to 50 of the original test, and part B included items 51 to 100 of the original test. We divided the participants randomly so that half of them completed part A pre-intervention and part B post-intervention. The other half of the participants completed the SHEMESH test in the opposite order (part B pre-intervention and part A post-intervention).
One week after the three total sessions, experimental group participants completed a feedback questionnaire with quantitative and qualitative assessments. They rated the program’s usefulness, impact on quality of life, mood, relationships, likelihood of recommending, and interest in future museum programs on a 1-5 scale (1 = “not at all” to 5 = “very much”).
Data analysis
Normality assumption
Normality was evaluated using the Shapiro-Wilk test. The analysis revealed that the clinical variables, MoCA scores, and language (immediate story recall, delayed story recall, naming) scores were not normally distributed. However, the emotional health status variables (quality of life and depression) were all normally distributed. Therefore, both parametric and non-parametric statistics were used to analyze the data.
Sociodemographic and clinical characteristics of the study participants
Sociodemographic and clinical characteristics of the participants are separately presented for each study group using descriptive statistics, including the median, sample size (n), and percentage. To assess differences between the two study groups, various statistical tests were employed. Categorical variables were compared using the chi-squared test, while continuous variables were analyzed using the Mann-Whitney U test.
Changes from pre- to post-test in quality of life scores and depression symptoms
A mixed-model analysis of variance was performed to evaluate changes in quality of life and depression scores over time between the intervention and control groups. The analysis examined the total score of quality of life, three quality of life sub-domains (feelings, memory, everyday life) and depression. The Bonferroni Post-hoc tests were used.
Since the sample size in each study group was small and may account for the null results (p > .05), we also reported the effect sizes (ES). One of the advantages of the ES is that it is independent of certain details of the experiment, such as the sizes of the samples used. ESs for the ANOVA were quantified using partial eta squared, with interpretations classified as follows: values less than 0.01 were considered negligible, values between 0.01 and 0.06 indicated a small effect, values between 0.06 and 0.14 signified a moderate effect, and values greater than 0.14 represented a large ES (Richardson, 2011).
Variables associated with post-test quality of life scores and depression symptoms
Associations between age and clinical characteristics (cognition and language level) and between post-test quality of life scores and depression were evaluated using Spearman rank correlation coefficients. In addition, an ANCOVA test was conducted to evaluate changes in quality of life and depression between the control and intervention groups, with age, cognition (MoCA), immediate language recall, delayed language recall, and naming as covariates. Levene’s test for equality of variances was performed. The Levene test was negative (p > .05), suggesting that the variances in the groups were similar, and therefore the assumptions for ANCOVA were met. The assumption of homogeneous regression slopes for the various groups was also examined, with the assumption being met (p > .05).
Intervention group – mood before and after the activity
Mood before and after the activity were evaluated in each of the three activity sessions. Mood changes from before to after the activity were compared using repeated measures analysis of variance (Bonferroni corrected). This analysis was conducted only for the intervention group. The results are displayed graphically using box and whisker plots.
Participants’ feedback on the program
Participants were asked six questions regarding the activities conducted at the museum. Each question was ranked from 1 (not at all; negative feedback on the activity) to 5 (very much/likely; positive feedback on the activity). The percentage of participants reporting each of the five ranking categories was calculated and presented graphically using histograms.
In all analyses, the level of significance was set to p < .05 (two-tailed) using IBM SPSS Statistics (version 23.0).
Results
Study participants
Sociodemographic and clinical characteristics of the study participants.
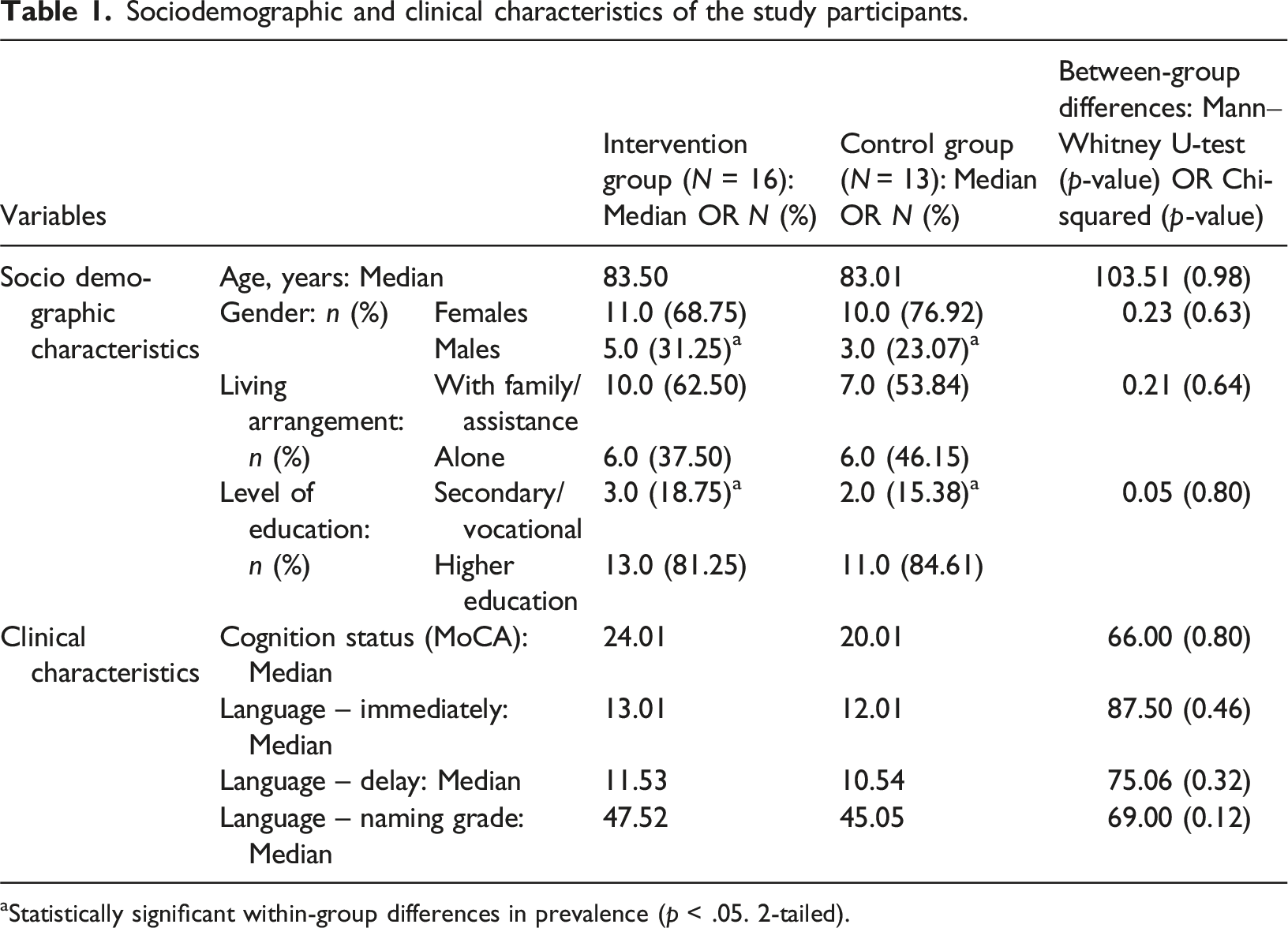
aStatistically significant within-group differences in prevalence (p < .05. 2-tailed).
Pre- and post-test changes in quality of life scores and depression symptoms
Mixed model analysis of variance for the intervention group and measurement time.
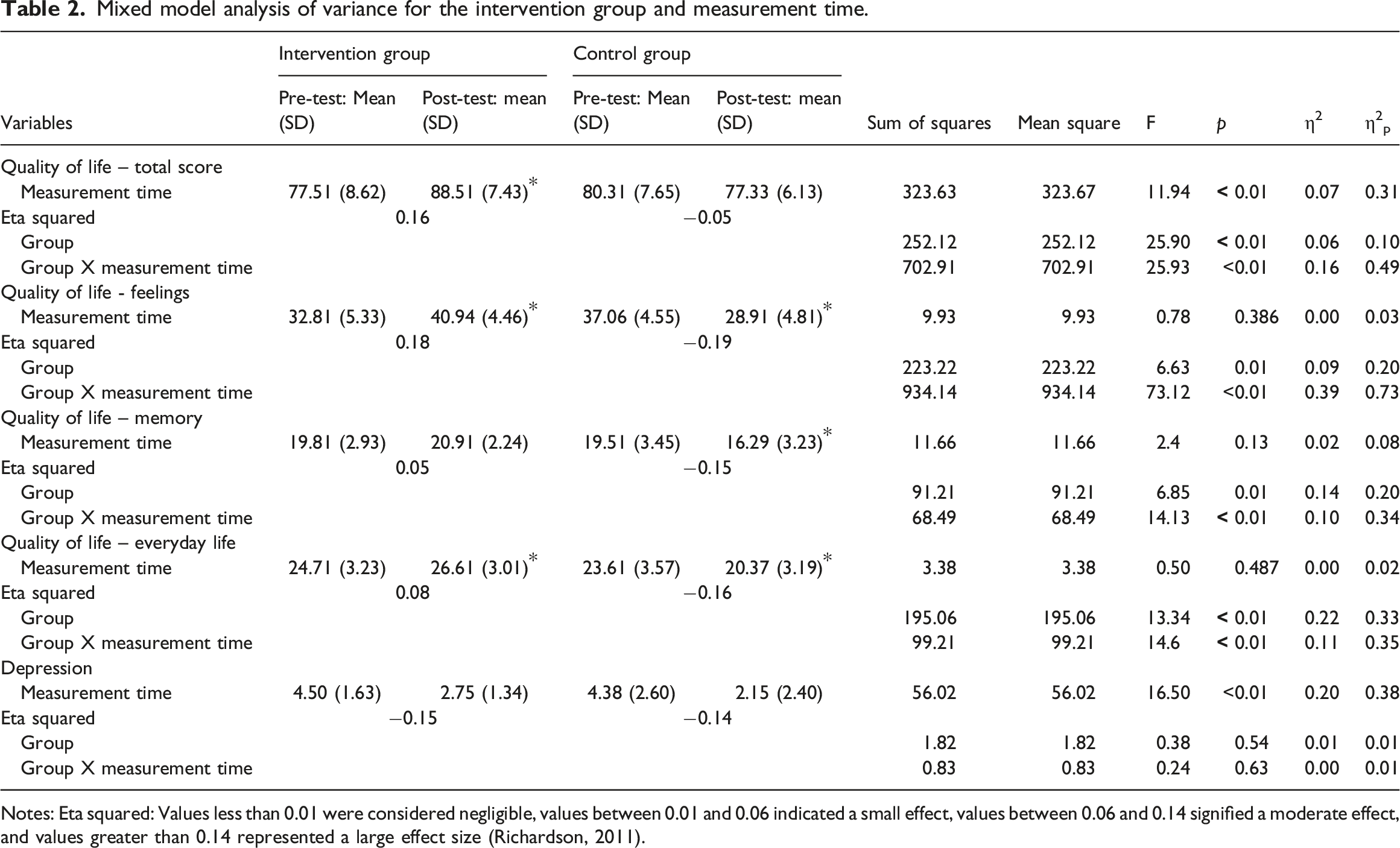
Notes: Eta squared: Values less than 0.01 were considered negligible, values between 0.01 and 0.06 indicated a small effect, values between 0.06 and 0.14 signified a moderate effect, and values greater than 0.14 represented a large effect size (Richardson, 2011).
In all quality of life sub-domains, there was no significant main effect of measurement time (p > .05). However, in all three sub-domains a significant main effect of group was found, suggesting that the intervention group had consistently higher scores than the control group. The significant interaction effect indicates a differential change between groups, with the intervention group showing a large positive improvement in the three quality of life measures: feelings (eta squared = 0.18), small positive improvement in memory (eta squared = 0.05), and medium positive improvement in everyday life (eta squared = 0.08). The control group showed a large negative change in feelings (eta squared = 0.19), a large negative change in memory (eta squared = 0.15), and a large negative change in everyday life (eta squared = −0.16).
The analysis of depression scores revealed a significant main effect of measurement time (F = 16.50; p < .001) with no significant main effect of group (F = 0.83, p = .544). The interaction effect between group and measurement time was also not significant (F = 0.24; p = .62), with both intervention and control groups showing large changes in depression scores (eta squared = 0.15 and 0.14, respectively ; Table 2).
Associations with post-test quality of life scores
Associations between post-test quality of life scores and depression symptoms.
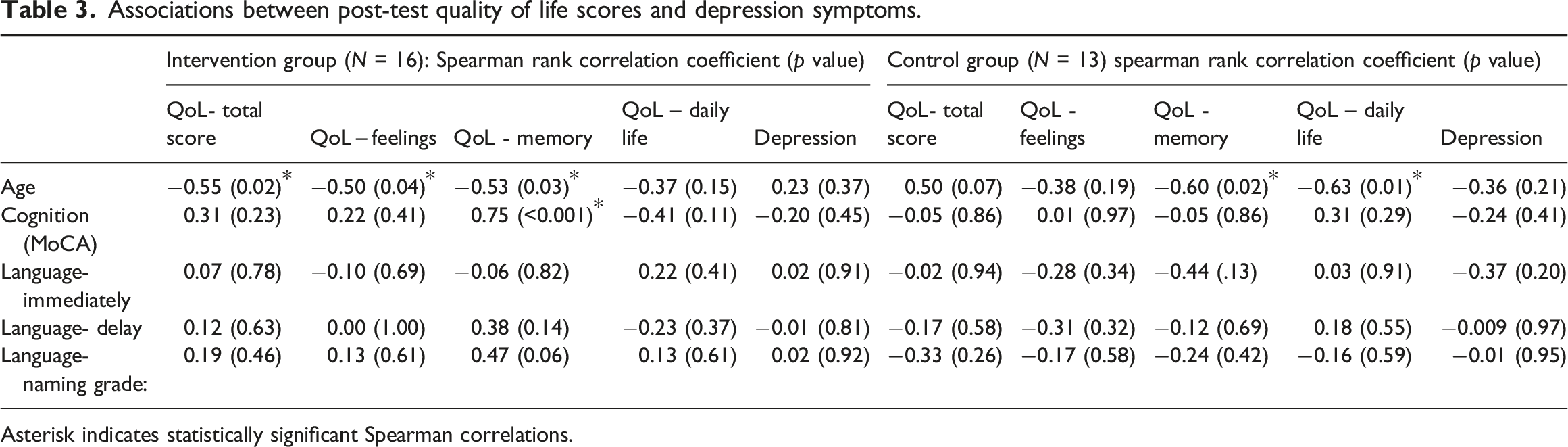
Asterisk indicates statistically significant Spearman correlations.
Analysis of covariance for changes in quality of life and depression.
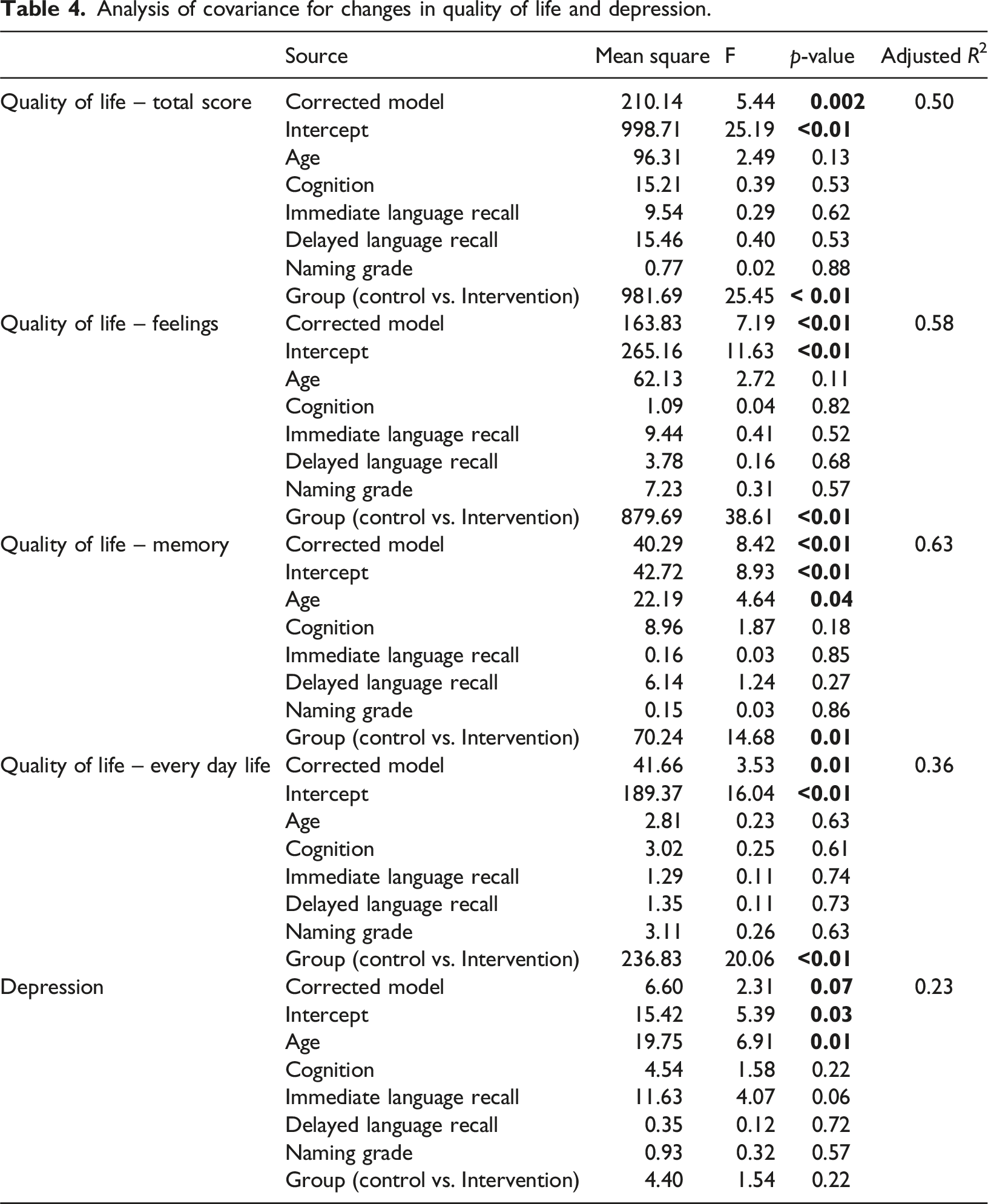
Regrading quality of life – memory (adjusted R2 = 0.63) and depression (adjusted R2 = 0.23), there was also a significant effect for the intercept (p < .05). However, the covariate significantly influenced quality of life – memory and depression scores (p < .05). In addition, in quality of life – daily life the intervention group score was better than this in the control group. However, there was no statistically significant difference in depression scores between the control and intervention groups after adjusting for the covariates (F = 1.54, p = .23; Table 4).
Intervention group – mood before and after the activity
Across the three museum sessions, participants’ mood scores showed a significant improvement from pre- to post-session. The mean pre-session mood scores for sessions 1, 2, and 3 were 3.75 ± 0.21, 3.43 ± 0.15, and 3.37 ± 0.20, respectively. These increased to 4.68 ± 0.11, 4.56 ± 0.12, and 4.56 ± 0.10 at post-session, respectively (F = 16.85, p < .01; see Figure 2). Intervention group – mood before and after the activity (Notes. (a), statistically significant different from post-test session 1 (p < .05); (b), statistically significant different from post-test session 1 (p < .05); (c), statistically significant different from post-test session 1 (p < .05); The central box represents the values from the lower to upper quartile (25th–75th percentiles); the vertical line extends from the minimum to the maximum value. The middle line represents the median).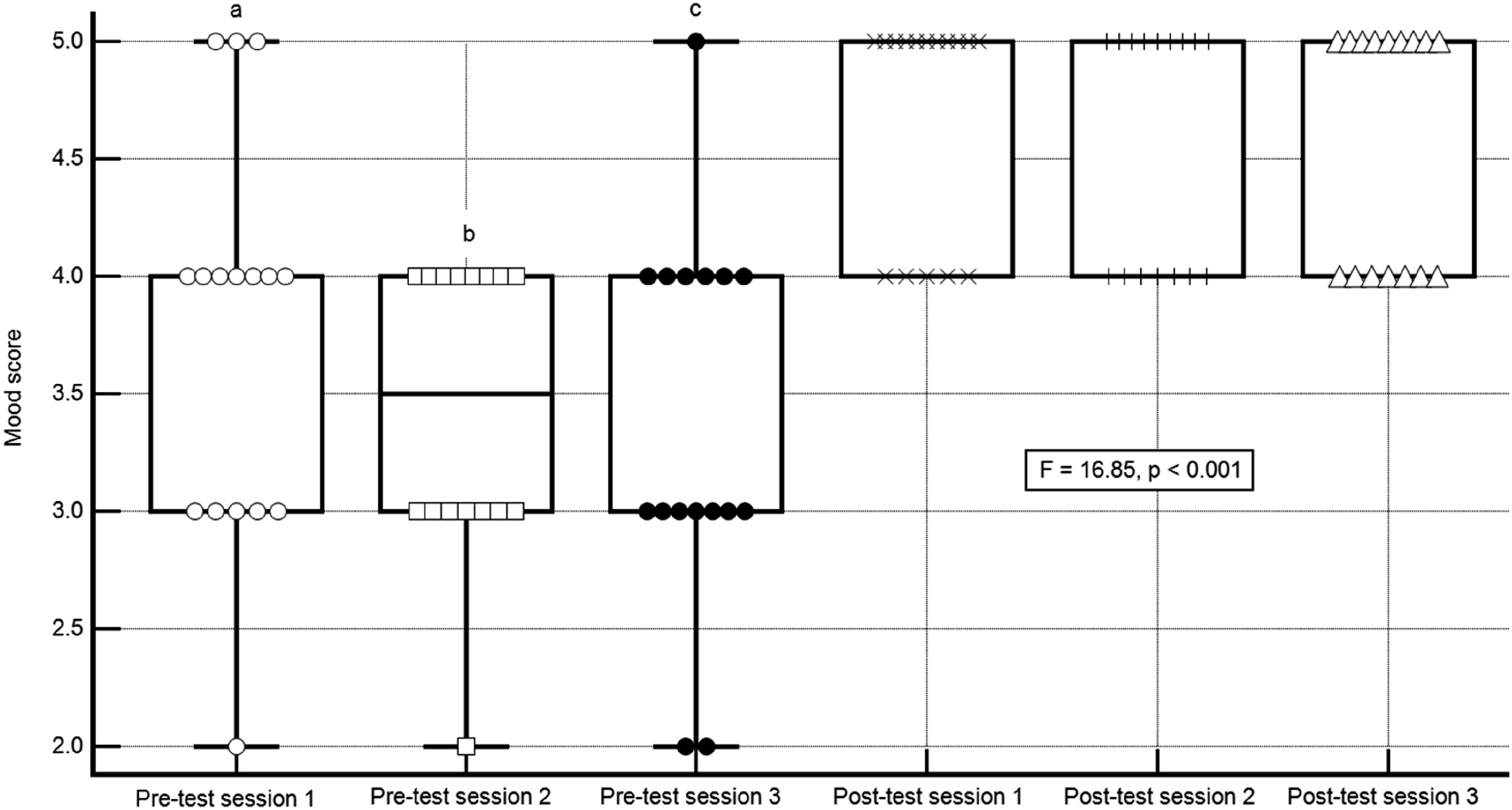
Participant feedback on the program
Overall, 81.2% of the participants who reported that the program helped them improve their mood “very much” were very positive, 93.7% reported that they were “very likely” to recommend the program, and 62.5% indicated that they were “very likely” to return to the program (Figure 3). Participants’ feedback on the program. Note. No participant reported scores of 1 or 2 on any of the questions.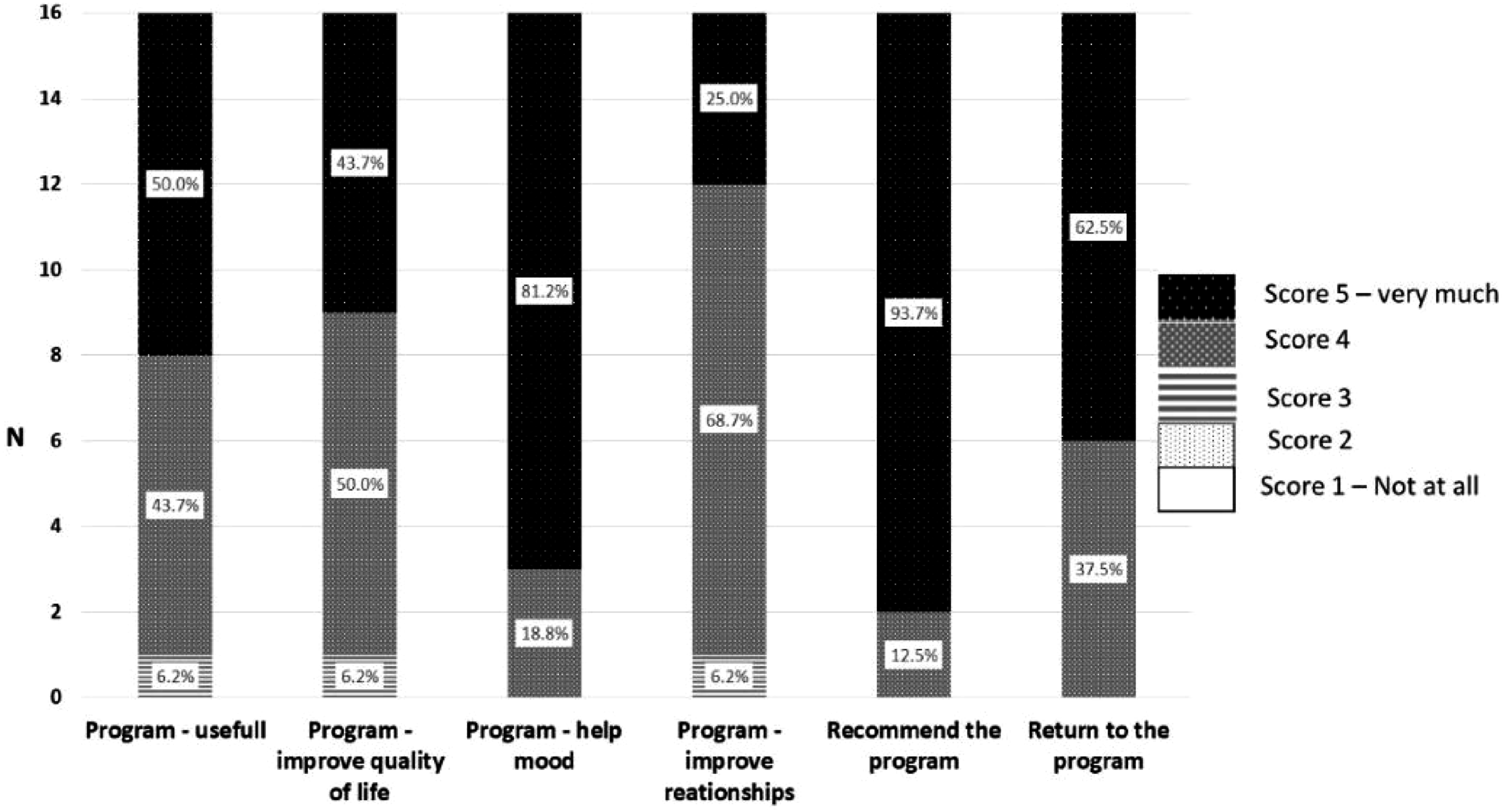
Linguistic and communication abilities pre- and post-intervention
Means and standard deviations of the language tests pre and post-intervention.
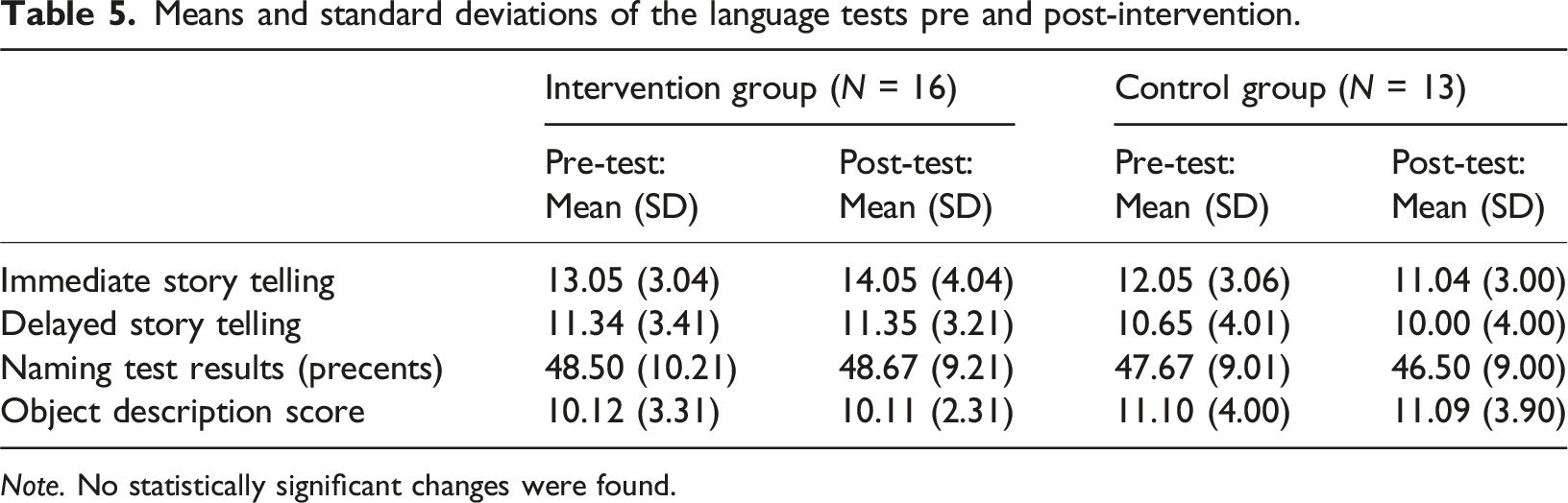
Note. No statistically significant changes were found.
Discussion
We reported on a pilot museum-based program developed to address a noticeable gap in available social services in Israel, particularly regarding the enhancement of well-being among individuals with mild to moderate cognitive impairment. This groundbreaking initiative resulted from a collaborative effort between experts, academics, and practitioners in the fields of aging and museum practice, uniting professionals from Ariel University, Ariel Municipality, and the Ralli Museum in Caesarea. Moreover, a comprehensive experimental study was designed to rigorously assess the impact and efficacy of this intervention program.
Our study was grounded in a set of hypotheses, the first of which posited that museum interventions could improve the quality of life for older adults with mild to moderate dementia. Initial data showed similar quality of life scores across intervention and control groups, though controls had slightly higher feelings subscale scores. Following the intervention, the intervention group experienced significant improvements in quality of life across all domains, despite a decline in the control group’s memory performance—a reflection of dementia progression (Livingston et al., 2017; World Health Organization, 2017). These outcomes highlight the value of ongoing interventions, supporting the WHO’s guidelines on enhancing the well-being of those with dementia (World Health Organization, 2021). The positive impact of museum programs on the quality of life of cognitively impaired older adults is supported by existing studies (Camic et al., 2014; De Medeiros & Basting, 2014; Rosenberg, 2009; Schall et al., 2017; Young et al., 2016; Zeilig et al., 2014), confirming the vital role of cultural activities in dementia care.
We hypothesized that the museum intervention program would reduce depressive symptoms in older adults with mild to moderate dementia. While no significant between-group differences were found, the intervention group showed a positive shift with a large effect size, unlike the control group. These findings align with an Australian study on art-viewing sessions, which also reported reduced depressive symptoms post-intervention (D’Cunha et al., 2019).
Our third hypothesis was that age and cognitive score (MoCA) would be associated with post-test quality of life. In the control group, only older age was associated with reduced quality of life. In the intervention group, older age was also significantly associated with reduced post-test quality of life (feelings, memory, and total score). However, in the intervention group, the cognitive score (MoCA) was also significantly correlated with post-test memory, with higher MoCA scores associated with increased memory. These findings confirm our hypotheses related to age and cognitive scores affecting post-test quality of life.
We hypothesized that museum activities would positively affect participants’ mood, a hypothesis supported by the observed increase in mood scores from before to after the activity. This aligns with Rosenberg’s study, which found a positive effect of museum programs on the mood of older adults with cognitive impairment (Rosenberg, 2009). Furthermore, participants' positive feedback emphasized enhanced mood and a keen willingness to recommend and return to the program. Unlike previous studies, such as Johnson et al. (2017), which highlighted participants’ enjoyment in feedback, our research explores participants’ readiness for repeat visits and to recommend the program to others, thereby reinforcing its effectiveness.
No significant changes in linguistic or communication measures were observed, likely due to high baseline naming test scores, indicating a ceiling effect. Additionally, the test materials were general rather than tied to museum content, suggesting that using art-specific items could yield different results.
Our findings affirm the value of art interventions in dementia care, highlighting the ‘effect' as significant improvements in well-being, cognitive abilities, and communication. This broad definition of ‘effect' aligns with established research (Camic et al., 2014, 2016; De Medeiros & Basting, 2014; Rosenberg, 2009; Salisbury et al., 2011; Schall et al., 2017; Young et al., 2016; Zeilig et al., 2014), emphasizing the wide-ranging benefits of these programs.
Limitations
This study has several limitations. First, the small sample size, inherent to its exploratory and pilot nature, limits the generalizability of the findings. Despite this, the substantial effect sizes observed in the intervention group suggest meaningful improvements, warranting further investigation.
As we focused on a specific population (Russian-speaking Holocaust survivors), it is important to highlight the need for broader participant diversity and the inclusion of various dementia types in future research. The use of the MoCA without medical records also restricted our findings into specific dementia conditions (Livingston et al., 2017; World Health Organization, 2017, 2021). Additionally, the social component of the intervention may have influenced the outcomes, suggesting the need for a control group with purely social activities in future studies.
Further, the reliance on self-reported measures and the single museum setting limited the study’s scope. Future research should explore broader methodologies, including pictographic scales for dementia patients and the effects of both passive and active arts interventions (Alzheimer’s Disease, 2012; Shaer et al., 2008; Zeilig et al., 2014). Long-term follow-up is also needed to assess sustained impacts.
Digital platforms, including virtual reality, offer potential for scaling art interventions, providing accessible and cost-effective solutions for enhancing cognitive and emotional well-being (Flynn et al., 2003; Manera et al., 2016; Oliveira et al., 2021).
Lastly, sensory impairments were not formally assessed, which may influence the interpretation of the results. While no discomfort was reported, unaddressed hearing or vision issues could have affected engagement and outcomes. Organizers mitigated these factors by optimizing room acoustics, using a microphone, and reminding participants to bring glasses for viewing exhibits or drawing.
Beyond its empirical findings, this study contributes to the theoretical understanding of non-pharmacological interventions, such as museum-based programs, in improving cognitive and emotional well-being.
Conclusions
The study highlighted the significant benefits of museum programs on mood and quality of life in older adults with cognitive impairments. Recognized by local and national authorities, these findings call for further exploration of long-term impacts and scalable implementation within social support systems to enhance dementia care.
Footnotes
Acknowledgements
We extend our heartfelt thanks to the Ariel Municipality staff and the Matav organization for their unwavering support. We also appreciate Judith Tlebel, the museum educator and art therapist, for her invaluable contributions in designing and conducting the museum sessions. Special recognition of the dedicated team at the Ralli Museum, with a sincere acknowledgment of Lily Tzohar, the museum’s director, for her pivotal role in coordinating the meetings. Finally, we express our profound gratitude to the study participants for their enthusiastic participation and the wonderful atmosphere they fostered throughout the project.
Author contributions
S.Z., A.B.L., S.B., S.L., Y.M. and R.T. conceptualized the study and performed the data analysis and interpretation. S.Z., A.B.L., S.B., S.L., I.K.S., Y.M., S.S. and R.T. contributed to the writing. S.Z., A.B.L., S.B., S.L., I.K.S., Y.M., S.S., and R.T. critically reviewed the final version. All the authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.