
Abstract
Older adults with dementia, when hospitalised, frequently experience responsive behaviours. Staff struggle to manage responsive behaviours without specific education. We aimed to enhance staff knowledge and confidence with care for older adults with dementia and responsive behaviours on medicine units at a Canadian hospital. An online dementia education program was disseminated to staff as part of a broader quality improvement project. Gentle Persuasive Approaches (GPA) encourages staff to reframe responsive behaviours as self-protective expressions of unmet needs and learn to assess their meaning. Participants completed online quantitative and qualitative measures of self-efficacy, competence and knowledge in dementia care at three times: immediate pre-, immediate post- and six to eight weeks post-GPA eLearning. Immediately post-GPA, participants showed significant increases relative to baseline in dementia care self-efficacy, competence and knowledge. Self-efficacy scores increased further eight weeks post-GPA. Before GPA, few participants described dementia-specific strategies for de-escalating a patient’s agitation. Eight weeks post-GPA, participants described application of tailored, person-centred, non-pharmacological interventions and successful application of GPA strategies. GPA eLearning strengthened staff preparedness to interact with older adults experiencing responsive behaviours, thus enhancing their care.
Introduction
Older adults with dementia are admitted to acute care hospitals at a higher rate than those without dementia, primarily due to increased frailty and comorbid conditions (Prince et al., 2016). Moreover, a significant portion of older adults admitted to hospital are likely to have undiagnosed dementia (Briggs et al., 2017). However, acute care is a complex environment and hospital admission is associated with several negative consequences for people living with dementia, including delirium, falls, inappropriate prescription of medications, long lengths of stay (Briggs et al., 2017; Butcher, 2018), functional decline and emotional distress (Tay et al., 2017). Quality of hospital care affects the likelihood of these outcomes (Fogg et al., 2018).
People living with dementia and their families report stressful and unpleasant experiences in hospital (Naef et al., 2018). Hospital staff focus on tasks required to treat the patients’ comorbid conditions, prioritising routines and safety regulations as opposed to meeting individual needs (Dewing & Dijk, 2016; Jensen et al., 2018; Scerri et al., 2018). A fast-paced, treatment-focussed mindset triggers resistance if a procedure does not match patient needs or emotional state (Featherstone et al., 2019). When unprepared staff interpret resistive behaviours as a component of the dementia diagnosis rather than attempts to communicate personal needs, they often do not investigate underlying reasons for distress. Even when staff do identify needs and preferences of the person, this information is often not effectively communicated to new staff members after shift changes (Jensen et al., 2017). The complex physical, social and emotional needs of people living with dementia are beyond the scope of many acute hospitals.
Patients living with dementia express confusion, sadness, boredom, and frustration when not understood by caregiving staff (Hung et al., 2017; Jensen et al., 2018). When patients react to treatment with fear and confusion, staff frequently persist, despite apparent lack of understanding and consent (Jensen et al., 2018). When a distressed person’s behaviour is not defused, escalation leads to physical self-protection. Traditionally labelled from a diagnostic perspective as behavioural and psychological symptoms of dementia (BPSD), the term responsive behaviour has been identified as the preferred term amongst direct caregivers, since these behaviours generally occur in response to a person’s unmet needs and there is a movement to discourage pathologizing of human behaviour (Alzheimer Society of Canada, 2019; Behavioural Supports Ontario, 2020; Bourgeois & Hickey, 2009; Cohen-Mansfield et al., 2015; Dupuis et al., 2012; Dupuis & Luh, 2005). Up to 45% of older adults living with dementia admitted to hospital exhibit responsive behaviours (Dewing & Dijk, 2016; Keenan et al., 2011; Nayton et al., 2014), risking injury for both patients and caregivers.
When educational background is limited, staff witnessing responsive behaviours may not address the emotional needs of their patients, leading to moral distress in staff (Bryon et al., 2012; Livingston et al., 2014; Sourial et al., 2001; Zwijsen et al., 2014). Quality of hospitalisation for patients with dementia is influenced by staff valuing the person and their family through actions and communication skills (Prato et al., 2018). Despite a growing body of knowledge about best practices supporting patients with responsive behaviours (Legere et al., 2017; Livingston et al., 2014), few hospital staff receive formal education on aetiologies of and strategies for responding to responsive behaviours (Doherty & Collier, 2009; Fessey, 2007; Turner et al., 2017). Consequently, when patients experience responsive behaviours, staff provide a limited set of effective supports (Yous, Ploeg et al., 2020a; Yous, Schindel Martin et al., 2020b).
Staff perceptions of their own preparedness confirm the need for dementia education (Yous et al., 2019). Nurses feel uncertainty and fear about caring for patients with dementia, particularly because of variable behavioural presentations (Pinkert et al., 2018). Patients are required to follow strict routines because staff are pressured to maintain existing schedules. Adapting care to meet individual need is not encouraged. Physicians also report uncertainty about addressing food refusal, pain assessment and behavioural symptoms related to dementia (Helm et al., 2018).
The impetus for dementia education in acute care reflects culture change in hospitals (Brooker, 2007; Dewing & Dijk, 2016; McCormack, 2003; Talerico & Evans, 2000; Thompson, 2015) implementing patient-centred care delivery models that emphasise communication, partnership, and health promotion (Borbasi et al., 2006; Nilsson et al., 2012). Safety preparedness standards also drive education to mitigate risk of staff and patient injury (Human Resources and Skills Development Canada, 2009). Several dementia education interventions have therefore been developed and implemented within acute care hospitals.
Dementia education described in the literature (e.g. Edwards et al., 2015; Elvish et al., 2018; Hobday et al., 2017; Jack-Waugh et al., 2018; Karlin et al., 2017; Kinderman et al., 2018; Pfeifer et al., 2018; Pleasant et al., 2017; Scerri et al., 2017; Spector et al., 2013) primarily deals with the aetiology of cognitive impairment, the concept of personhood, communication skills, recreational and diversional activities, behavioural assessment formats and broad behavioural management skills. Education has enhanced staff capacity to provide dementia care in a variety of contexts. However, there is a need for specialised dementia education that fosters the skills necessary to manage more intensely escalated responsive behaviours with risk of injury for patients, staff and others. Without such staff knowledge, it is likely that patients with these behaviours will ultimately be pharmacologically sedated, with high rate of complications (Dyer et al., 2018; Kales et al., 2019; Simpkins et al., 2016).
Gentle Persuasive ApproachesR (GPA) in Dementia Care is an established curriculum initially designed for staff in long-term care responding to responsive behaviours. It was developed beginning in 2004 by an interdisciplinary group of educators and clinicians from Hamilton, Halton and Niagara, Ontario in collaboration with the Continuing Gerontological Education Cooperative (CGEC) and with the assistance of a research grant from the Regional Geriatric Program (Central). GPA has been introduced into over 2000 long-term care facilities, adult day centres, and complex continuing care and acute care hospitals across Canada. GPA Basics day-long sessions are conducted face-to-face, while more recently, a 2–3 h eLearning version of GPA was developed, comprised of the core content from the GPA Basics curriculum. GPA eLearning allows efficient implementation to larger groups of participants. To date, GPA eLearning has only been provided to students and not to acute care staff.
GPA educates staff on how to use a person-centred and compassionate approach to respond respectfully, with confidence and skill, to responsive behaviours. GPA encourages staff to reframe behaviour traditionally viewed as ‘aggressive’ to be interpreted as self-protective behaviour reflecting unmet physical, psychological, spiritual or cultural needs. Staff learn to assess the meaning behind behaviour and work with the patient and family to meet the patient’s needs. A unique component of GPA is that it includes respectful and gentle physical body containment techniques. These are invaluable in some instances of escalating physical behaviours for momentarily redirecting the patient with dementia away from an altercation or situation involving risk of personal injury.
The GPA program is divided into 4 interactive modules with content on person-centred care principles (module 1), brain changes common in dementia, and how these changes are manifested in responsive behaviours (module 2), communication and interpersonal strategies that can either trigger or defuse behavioural escalation (module 3), and staff-specific physical self-protective skills and team/patient/family debriefing and reassurance techniques (module 4) that are effective, safe and respectful to use when interacting with people living with dementia. GPA eLearning pedagogical strategies include narrated, standardised slides with white board animations, video clips and tile-matching exercises that review core principles, as well as instructional videos that demonstrate the correct application of body containment strategies to safely de-escalate responsive behaviours.
First iterations of GPA significantly enhanced knowledge and confidence of long-term care staff regarding responsive behaviours and strengthened verbal communication skills during a simulated episode of behavioural escalation (Schindel Martin & Dupuis, 2005; Schindel Martin et al., 2003). In acute care, findings from an in-patient geriatric psychiatry program for older adults with dementia showed that incidents of patients’ aggressive behaviour declined by 50% after staff completed GPA, a decline sustained at three months post-GPA (Speziale et al., 2009). Another study in an orthopaedic surgery unit showed that relative to baseline, participants had significantly improved self-efficacy with responsive behaviour immediately after attending a GPA session (Pizzacalla et al., 2015). A mixed-methods non-randomised controlled trial at a large academic teaching hospital in Ontario evaluated the impact of GPA sessions in acute care staff (Schindel Martin et al., 2016). In the intervention group, staff self-efficacy for responsive behaviour was significantly increased immediately after GPA and sustained for eight weeks post-intervention. In contrast, control group scores were unchanged. Finally, a qualitative study (Hung et al., 2018) showed clear changes in hospital staff interpretations of patient behaviours after GPA. Staff learnt to adopt a positive attitude towards dementia care and look for the meaning behind the patients’ behaviours they had previously perceived as challenging or aggressive. Qualitative findings of all these studies indicated GPA-educated staff made efforts to get to know each person living with dementia, investigated modifiable reasons for responsive behaviours, and began to adapt the hospital routines to address unmet needs.
Staff in the current evaluation, who worked on five medicine in-patient units caring for patients aged >65 years at a hospital in Ontario, had historically received training in various dementia-specific educational interventions as well as general educational in-services. However, no standardised, sustainable process existed to operationalise the education. A quality improvement project was initiated with the aim of establishing such a process and to enhance existing resources. Specifically, the goal was to enhance the staff’s knowledge, confidence and skill to effectively practice a non-pharmacological approach to prevent and de-escalate responsive behaviours on the participating units. A portion of the quality improvement project funding was designated for implementing and evaluating staff training in GPA eLearning. It was predicted that GPA eLearning would significantly improve staff scores on measures of self-efficacy, competence and knowledge in supporting people experiencing responsive behaviours, relative to baseline scores. Moreover, it was expected that after GPA eLearning, participants would provide qualitative descriptions of how they had used GPA strategies in their clinical practice.
Methods
Setting and sample
Staff employed on five medicine units at a Canadian hospital were invited to participate. This hospital has two main sites; the north site has a 60-bed medicine unit while the south site has several 12-bed medicine pods, including an Acute Care of the Elderly unit. A sample of 100 interdisciplinary full-time, regular part-time and casual staff enrolled in GPA eLearning, and 94 staff members completed it. Of those 94 participants, 86 volunteered to complete the program evaluation measures.
Design
A longitudinal pre-post design was used, and GPA eLearning was implemented over two months via its online platform to eligible staff. The effects of GPA were assessed using online quantitative and qualitative questionnaires at three time points: (1) immediately pre-GPA, (2) immediately post-GPA and (3) 6–8 weeks post-GPA training.
All eligible staff were invited to attend a subsequent four-hour workshop about the overall program evaluation, including one hour for supervised practice of GPA body containment strategies with in-house GPA certified coaches. Finally, a subset of participants who had attended the workshop voluntarily attended a face-to-face focus group after the workshop, describing their experiences in practical application of GPA principles. Because this program evaluation was not designated as research by the associated institutional research ethics board, ethical approval was not required. Nevertheless, all the principles from the Tri-Council Policy Statement (TCPS) on the Ethical Conduct for Research Involving Humans (Canadian Institutes of Health Research et al., 2018) were followed. Participation in the program was mandatory, reflecting organisational expectation; however, completion of the evaluation was voluntary. All participants who completed the program evaluation measures provided electronic informed consent and understood that their identity would not be linked to their evaluation responses, their personal information would remain anonymous to the project team members, and the evaluation data would be stored securely.
GPA eLearning program implementation
Participants accessed GPA eLearning through a standardised email recruitment message and URL. Staff could access the course for six weeks. GPA eLearning takes 2–3 h to complete, but participants could complete it at their own pace. After completing it, the content could be reviewed at any time during the six-week period. Participants could also download an accompanying eManual and a certificate of completion.
Measurement instruments
1. The Self-Perceived Behavioural Management Self-Efficacy Profile (SBMSEP) measures confidence in the clinical behaviours and tasks necessary for responding respectfully to responsive behaviours (Schindel Martin & Dupuis, 2005; Schindel Martin et al., 2016). This 10-item, 7-point Likert-type scale (1 = not very confident ranging to 7 = very confident) measure was completed at all three time points, followed by several open-ended questions. The SMBSEP was developed using Bandura’s (1977) principles of self-efficacy and subjected to review by clinical experts in behavioural symptoms associated with dementia to establish its content validity, internal consistency, and reliability (Cronbach alpha = 0.93). Three open-ended questions were asked at the end of the SBMSEP at three time points, immediate pre- and post-GPA and again at 6–8 weeks post-GPA. The questions were: (1) If I were to describe the way I usually react when older people living with dementia are aggressive, agitated and upset, I would say; (2) If I were to change anything about my ability to respond to older people living with dementia who are aggressive, agitated and upset, I would; and (3) The best practice approaches to use when responding to older people living with dementia who are aggressive, agitated and upset are. 2. The Sense of Confidence in Dementia Care Staff scale (SCIDS, Schepers et al., 2012), completed at all three time points, is a 17-item measure with 4-point Likert-type scales (Cronbach alpha = 0.91). assessing the confidence staff have in their ability to interact with and care for older people with cognitive impairments (participants rated how well they could do each item and responses ranged from 1 = not at all to 4 = very much) Scores on this measure are positively associated with work experience, job satisfaction, and person-centred approaches to dementia care (Schepers et al., 2012). 3. The Knowledge Test was developed to assess understanding of the GPA curriculum and consisted of multiple-choice questions (MCQs) reflecting the content of the course, evaluating knowledge of dementia and person-centred care strategies. Stem questions included short scenarios describing responsive behaviours, and participants were asked to select the most adept intervention from 4 options. Eight questions were drawn randomly for each participant from a larger bank of 40 questions, 2 questions per module, with the same set of 8 given across all three time points. 4. The participant satisfaction questionnaire assessed how well various components of GPA eLearning met participant expectations. Participants were asked if they would recommend GPA eLearning to their colleagues and rated their satisfaction on a 7-item 7-point Likert-type questionnaire (1 = not very satisfied ranging to 7 = very satisfied) with GPA eLearning overall, the length of the program, its practical application, the white board animations, the learning activities, the embedded video clips and the self-protection demonstration video clips. Lastly, they provided open-ended qualitative suggestions for improvement.
Focus group
The 25-min post-intervention focus group was conducted by two facilitators with a volunteer sub-group of eight participants who completed the GPA eLearning program prior to attending the follow-up workshop. Participants provided written consent, and no members of the program evaluation implementation team or workshop facilitators attended the focus group. The primary facilitator asked three main questions from a semi-directed interview guide based upon the core competencies embedded within the GPA eLearning content and which has been a standard component of our GPA program evaluations from the inception of the curriculum (Schindel Martin et al., 2003). The questions prompted participants to (1) describe what they had learnt from GPA that was significant for the successful management of responsive behaviour in their practice, (2) provide specific scenarios in which they had implemented GPA strategies on their units and (3) explain if, how and why they thought the strategies had any impact on patient outcomes or job satisfaction.
Audio-recorded focus group data were transcribed verbatim and the transcript was de-identified. The focus group facilitators reviewed and analysed the data independent of the implementation team. It was agreed that the implementation team would only see data in the form of illustrative quotes supporting the emergent themes, to protect the anonymity of the participants.
Data analysis
Quantitative data analysis
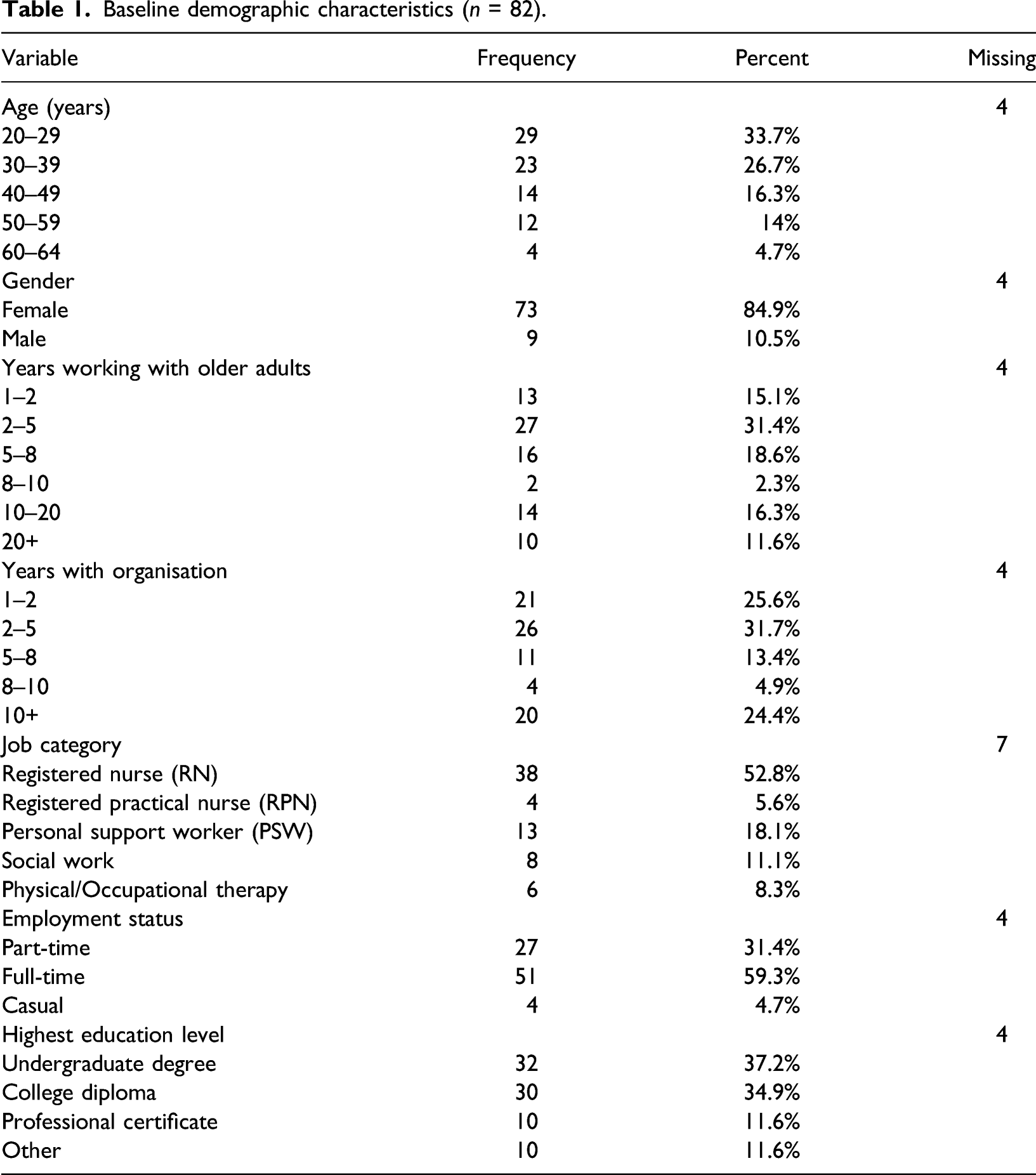
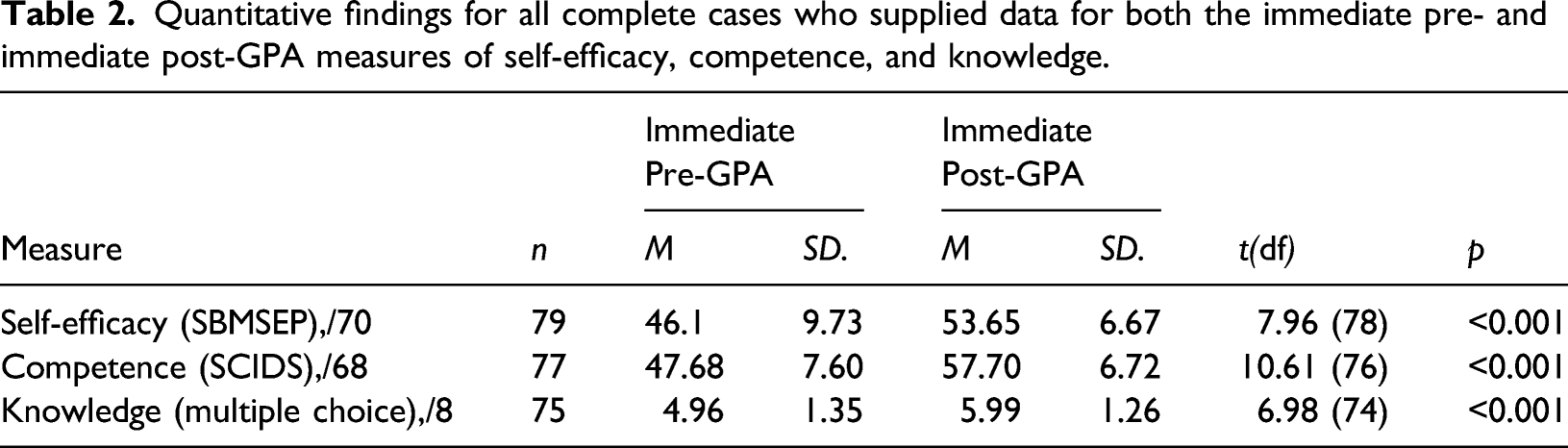
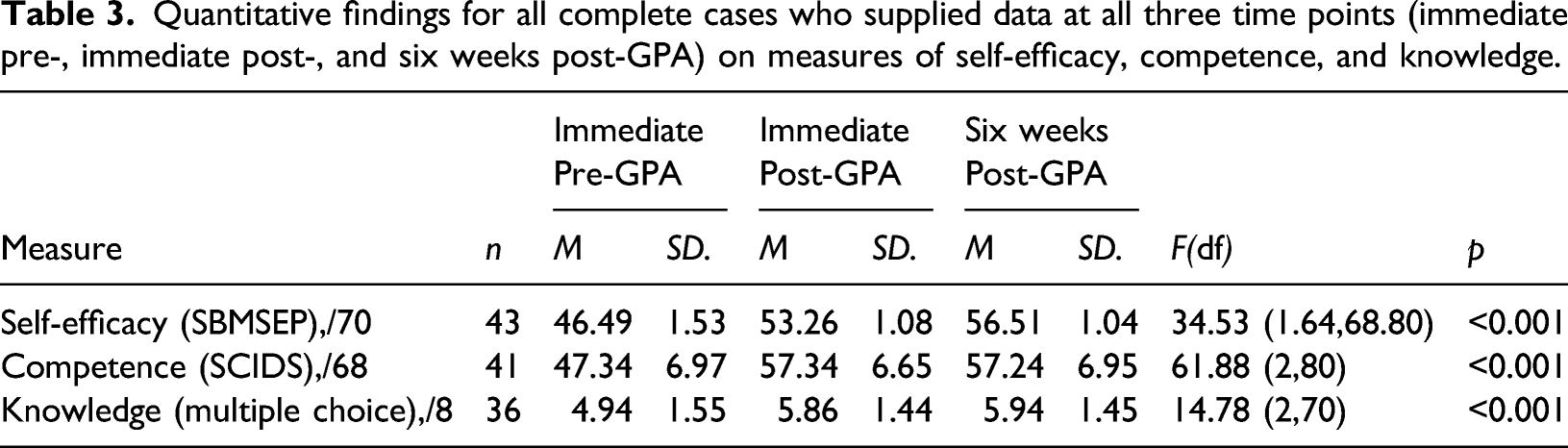
Descriptive statistics were summarised for the participants’ demographic characteristics (age, sex, number of years working with older adults and at their organisation, job role, employment status, shifts worked and education), and these categorical variables were reported as frequencies and percentages. Next, paired samples t-tests contrasting the immediate pre- and post-intervention measures of self-efficacy, competence and knowledge in dementia care were conducted to determine whether there were significant improvements in each of these three measures after GPA eLearning. Finally, one-way repeated measures ANOVAs were applied to the smaller set of all complete cases across the three time points (immediately pre-, immediately post- and six to eight weeks post-GPA eLearning) to assess the changes in participants’ self-reported self-efficacy, competence and knowledge in dementia care. For both of these latter analyses, in order to avoid biases in estimates of total self-efficacy, where participants had completed the self-efficacy measure at a given time point but missed responding to one or two individual items, the missing value was replaced with the mean of the other items on that measure (Downey & King, 1998). For all tests, a statistical threshold of p < 0.05 was considered significant.
Qualitative data analysis
The self-efficacy measure included three open-ended questions inviting participants to provide written responses at all three time points about their approaches to caring for patients with responsive behaviours. Similarly, during the post-intervention focus group, participants provided verbal responses to semi-structured interview questions about how GPA eLearning influenced their practice. All these data were subjected to thematic content analysis completed by two individuals of the team who were familiar with the curriculum content, but not involved in the delivery of the workshop and had no prior relationship with the professional healthcare team or participants. The qualitative data were analysed using a step-by-step inductive approach to arrive at the final thematic categories (Braun & Clarke, 2006). Categorical themes were refined and described according to GPA best practice competencies and discussed with the members of the implementation team during a review of the project précis report.
Quantitative results
Baseline demographic characteristics (n = 82).
Quantitative findings for all complete cases who supplied data for both the immediate pre- and immediate post-GPA measures of self-efficacy, competence, and knowledge.
Quantitative findings for all complete cases who supplied data at all three time points (immediate pre-, immediate post-, and six weeks post-GPA) on measures of self-efficacy, competence, and knowledge.
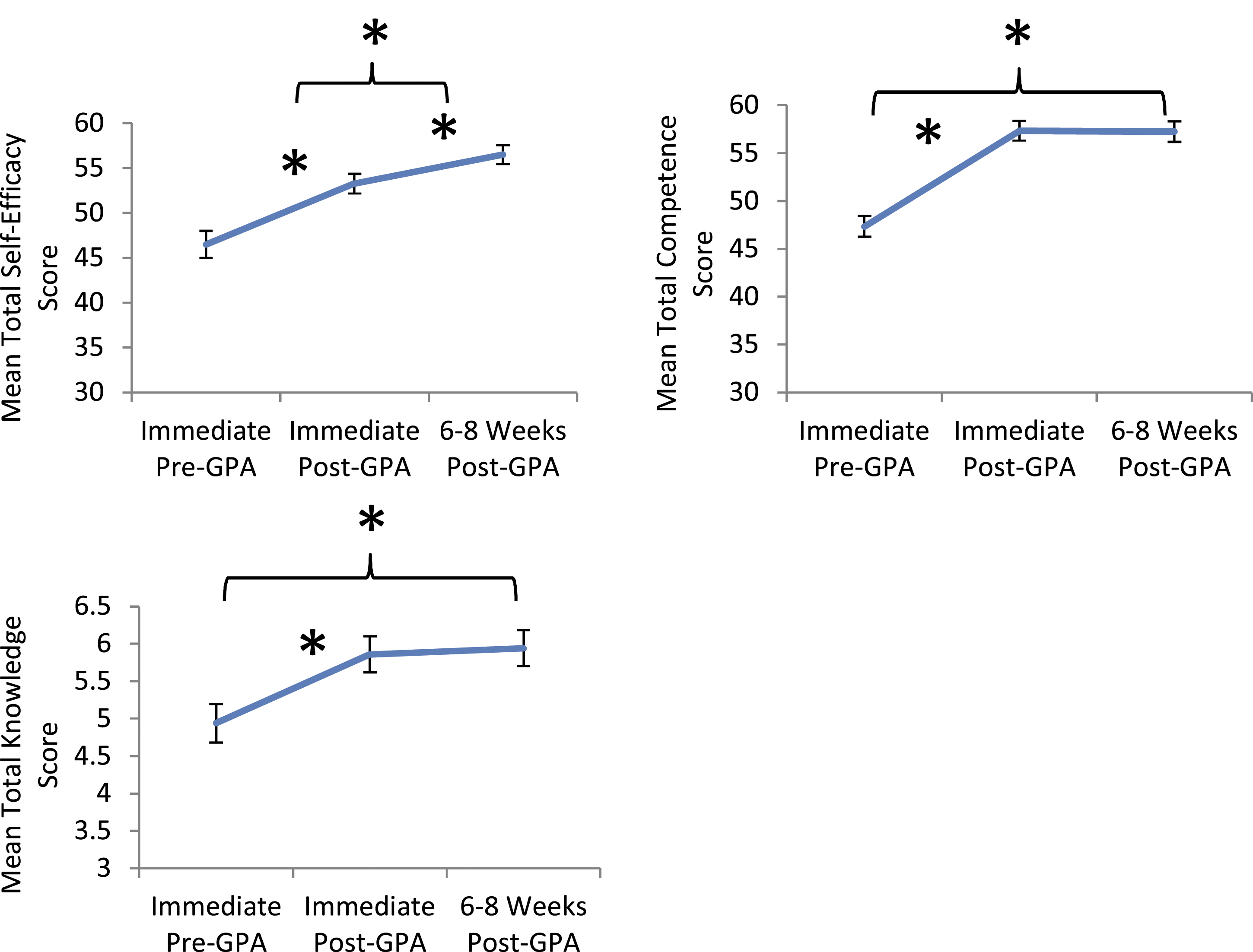
Mean total self-efficacy, competence and knowledge in dementia care at three time points: immediately prior to GPA eLearning, immediately post-intervention, and six to eight weeks post-intervention. Stars denote a significant difference (p < 0.05), error bars depict standard error of the mean.
Before GPA eLearning, participants had moderate levels of self-efficacy, competence, and knowledge, indicating use of basic best practices for patients with responsive behaviours. However, after completing GPA eLearning, participants’ mean scores on all three measures significantly increased. Large increases in competence and knowledge scores occurred immediately after GPA eLearning and were sustained up to eight weeks afterwards, while maximum increases in self-efficacy were not achieved until eight weeks post-GPA eLearning, suggesting that having opportunities to put learnt techniques into clinical practice contributed to improving self-efficacy (see Figure 1). Overall, findings suggest that at baseline, there were gaps in participants’ confidence and knowledge that were addressed through participation in GPA eLearning.
Satisfaction results
Participants were generally highly satisfied with GPA eLearning, making mean ratings of greater than 5.5 out of a maximum of 7 on all course components, and of the 81 participants who responded to the question, 100% reported that they would recommend GPA to their colleagues. Some participants thought the program could be shorter and would have liked more time devoted to practicing techniques for specific scenarios.
Qualitative results
Pre-GPA eLearning open-ended questions: Baseline approaches to responsive behaviours
Seventy participants answered the three open-ended questions at baseline asking about their current approaches, perceived need for practice change and knowledge of best practice expectations when caring for older people living with dementia and responsive behaviours. Baseline responses to these questions are presented here grouped under three main themes: Rudimentary Self-Confidence, Best Basic Approaches to Responsive Behaviours and Need for Additional Responsive Behaviour Techniques.
Rudimentary self-confidence
At baseline, only a few participants stated that they felt confident and successful when responding to episodes of responsive behaviour in the hospital setting. Several participants were nervous or frightened when caring for older patients experiencing responsive behaviours. Caring for such patients was identified as ‘difficult’ (#2), ‘annoying’ (#82) or ‘scary’ (#68) and episodes of responsive behaviour were ‘startling’ (#12) when encountered. One participant wanted to complete GPA eLearning to learn more about how to ‘control my own emotions’ (#12) during episodes of responsive behaviour. Several participants emphasised that it was important to be ‘wary and very cautious’ (#93) of individuals with dementia who displayed responsive behaviours during hospital admission. Many participants felt unprepared to interact with patients during episodes of responsive behaviour and identified that they needed to gain more knowledge and skill in communication, safety techniques and non-pharmacological interventions overall. During episodes of physical responsive behaviour, a frequent strategy was to ‘back off and let someone else handle it’ (#102) or leave the patient to de-escalate on their own, then return to assess if the patient was calmer. This simplistic strategy assumes staff presence evoked the behaviour and the person could de-escalate independently with no emotional support, which is often not the case.
Some participants discussed awareness of safety of self and others, including the identification of a potential exit route to avoid injury. A few participants mentioned awareness of the distance between themselves and the patient to mitigate responsive behaviours: ‘Do not approach patient from the back. Ensure that the patient knows I am there and I do not invade the patient’s space’ (#96). Few participants indicated that teamwork enhances safety during routine care of patients displaying responsive behaviours, which may reflect discomfort with requesting assistance.
Participants wanted to become more confident in their ability to care for patients during episodes of responsive behaviour, aiming to become ‘more assertive’ (#70), ‘purposeful’ (#18) or ‘firmer’ (#68) in their interpersonal approach. Participants wanted to learn more about how to respond to responsive behaviour that was not easily mitigated and find out about effective de-escalation techniques. Most participants used positive, hopeful language when identifying their learning goals. In the words of one participant: I would like to improve my ability to endure challenging behaviours over many days. It does become frustrating repeating oneself over and over, trying each technique only to have to start all over again. I am hoping to learn new ideas and concepts that I can apply to my practice and teach others. (#124)
Current basic approaches to responsive behaviour
At baseline, approaches to mitigate responsive behaviours in hospitalised patients with dementia were mundane, relying on basic verbal de-escalation strategies such as a quiet voice and conversational distraction. ‘I speak slowly, softly and clearly’ (#41). Several participants were aware that the quality of the interpersonal relationship with a patient with dementia was important, and that they routinely and purposefully offered empathic care by being ‘understanding, respectful and friendly’ (#127), ‘patient’ (#97), ‘kind and gentle’ (#77). These are all general communication strategies taught in first year training courses, rather than dementia-specific competencies. A small number of participants realised it was important to repeat requests more than once, use short and simple phrases, and offer explanations, offer choice, and involve the patient directly in care activities, as explicated in dementia communication and activity guidelines published for many years but have become part of professional vernacular to the degree that these terms are meaningless and indiscernible in practice (Nissenboim & Vroman, 1998; Rau, 1993; Yous, Ploeg et al., 2020a; Yous, Schindel Martin et al., 2020b; Zgola, 1999).
Participants identified that a core approach to responsive behaviour was to control their own emotional responses, rather than focus on patient-centred need. Overall, it was important to ‘
At baseline, participants mentioned a small number of person-centred interventions such as ‘offering tea, taking a patient for a walk, using music’ (#71), ‘engaging in distracting conversation’ (#121), ‘providing washcloths to fold and showing movies’ (#40), or ‘offering food’ (#52). With great insight, one respondent stated that it would be helpful if there were more activities available on the unit to help with distraction, for example, puzzles, colouring books, magazines and newspapers (#42). A handful of participants described specific purposeful distraction techniques such as massage or reminiscence, supported by evidence as reasonable best practices in guidelines for assessment and care of older adults with delirium, dementia and depression (Legere et al., 2017; Registered Nurses' Association of Ontario, 2016). Notably, at baseline, few respondents identified validation as a purposeful communication strategy to promote de-escalation when a patient is displaying responsive behaviours.
Some participants used very general statements that could be interpreted to infer an understanding of the importance of meeting unmet psychological, environmental, or physical needs. As one participant stated, ‘I try to make things right’ (#6), ‘I try to find out other ways to relax the patient; I try to respect their needs’ (#25), or ‘I try to do at least one thing they ask me to do’ (#31). Of the 70 respondents, only one participant provided more details with respect to their understanding of meeting unmet physical and psychological needs: Allow the patient to express their thoughts and try to work with what they are saying they need. Try to guess what they may need, by ruling out possible needs. Toileting, pain, hunger, thirst, loneliness, fear. (#120)
The responses provided at baseline were typical of studies conducted in acute care (Schindel Martin et al., 2016; Yous, Ploeg et al., 2020a; Yous, Schindel Martin et al., 2020b) whereby pre-learning descriptions of best practice surrounding responsive behaviours are general and lacking precise dementia-specific language or interventions. Baseline responses suggest verbal reassurance is frequently applied but there is limited use of tailored, person-centred interventions to mitigate patient distress.
Immediate post-GPA eLearning open-ended questions: New approaches to responsive behaviour
After GPA eLearning, 63 participants answered the same three open-ended questions as at baseline about their practice experiences, identified need for change and best practices for patients with dementia. Their responses revealed a newfound awareness of their personal reactions to responsive behaviour and a deeper understanding that responsive behaviours reflect unmet needs of both a psychological and physical nature. When asked about the best practices to use when responding to older people living with dementia who experience responsive behaviours, relative to baseline, participants more frequently mentioned validation as the preferred communication strategy (Feil, 1982, 1993), the importance of identifying psychological, emotional, physical and environmental triggers and providing for unmet needs (Cohen-Mansfield & Taylor, 1998), and noted the necessity to look for the meaning behind behaviours and entering the patient’s reality (Kitwood, 1997). Participants felt significantly more knowledgeable after completing GPA eLearning, but some stated that increases in confidence would come only with the experience of using new knowledge at the point-of-care. Responses are presented here under the themes of Enhanced Professional Insight and New Person-Centred Approaches to Responsive Behaviour.
Enhanced professional insight
Immediately after GPA eLearning, participants had developed more insight of how their own emotional response to responsive behaviour might impact the patient. ‘I would almost be confrontational towards them and now I see how that was the wrong approach’ (#4). A second participant wrote, ‘I reacted with confusion and a lack of understanding. I kinda took it personal. I didn't understand their limitations’ (#12). Another participant stated, ‘I learnt it is important to control my own body language better, I’m sure I look scared’ (#28). Yet another participant indicated, ‘I was quick to react before, now I will observe and reflect’ (#18). This growing professional insight into the reciprocal nature of behavioural escalation is critical for promoting reflection upon best practices and the confidence to deliver person-centred care to mitigate responsive behaviour, rather than scolding, setting limits or taking punitive action. As one participant admitted, ‘I used to say please don’t speak to me that way’ (#31). Conscious awareness of the way the professional caregiver might evoke or exacerbate responsive behaviour is personal knowledge necessary for best practice change (Carper, 1978). As one participant stated, ‘remember that what they are expressing is their reality and very real to them and not to persuade them differently’ (#11).
New person-centred approaches to responsive behaviours
Many respondents identified several new approaches they intended to use in combination, during interactions with hospital patients experiencing responsive behaviours. As one participant stated, I will take more time to know the patient, use open communication, de-escalation techniques, validation, distraction/redirection, attempt to find the underlying cause of the behaviours’ (#14). Others identified specific care techniques such as breaking the care task up into smaller units, using the GPA STOP & GO technique and applying the GPA hold releases as specific professional behaviours they would enact on their units (GPA eLearning, Module 4, Advanced Gerontological Education, 2014). As one participant wrote, ‘The education program was useful and informative. I have the ability to remove myself from holds without agitating the patient further’ (#92). Sixteen of the 63 immediate post-GPA respondents explicitly mentioned that the Stop & Go approach was a technique that could be used immediately to acknowledge the patient’s distress by purposefully pausing during a care interaction to promote behavioural de-escalation. With this strategy, the caregiver understands that 30-to 60-s breaks during a care routine will provide a small moment of interruption to a feeling of personal space invasion that will result in an immediate momentary relief of stress and upset for both patient and caregiver. This reduces the likelihood of responsive behaviour. As one participant wrote, ‘Use the STOP technique and realize that the task is not the priority, but rather the person’ (#24). In contrast, baseline responses included general statements that it was important for the caregiver to ‘re-approach’ the patient after leaving them alone for a period. The STOP & GO technique is a purposeful intervention that does not include leaving the patient, rather, it is a strategy whereby the patient is given a short break to de-escalate and the care provider remains to promote and support that de-escalation. The knowledge, strategies, and techniques that participants intended to apply as best practices on their units suggested they understood these new skills could be integrated into care delivery for positive outcomes. As one participant typed, I think this course is very well rounded. I tended to get flustered and wished to complete which ever task more quickly, so I could remove myself. Now I believe just the “take a moment” approach and understanding the responses are the need for the patient to protect themselves, and not intended to harm me as a nurse, these are useful tools for anyone who frequently works with someone suffering from dementia (#85).
Post-GPA eLearning focus group
During the focus group, participants provided specific, detailed examples of how they used the knowledge they acquired in the program to direct patient care, using GPA eLearning principles in an integrated, holistic fashion. Participants stated how the program provided them with new understanding and skills for both face-to-face interactions with patients and strengthening care culture. Responses are presented here under two themes, Competent Application of Person-Centred Approaches to Responsive Behaviour and Contributing to a Positive Dementia Care Culture.
Competent application of person-centred approaches to responsive behaviour
Several participants indicated the most important best practice knowledge gained from GPA was the realisation that patients with dementia could answer questions about potential triggers despite inherent memory difficulties. The information gathered led participants to identify tailored strategies rather than guessing what the problem was. Participants provided case examples from their practice about how new empirical, personal, ethical, and aesthetic knowledge (Carper, 1978) gained from their learning helped them build confidence in their ability to ask deliberate, tailored questions that evoked actionable information from the patients themselves. One focus group participant explained: I learned all behavior means something, I need to ask more questions, they are behaving that way because there is something underlying. Whether they are scared, hungry or they need to go to the bathroom. I never asked enough questions before. If the patient says, ‘I wanna get out of here, I wanna go home!’, now I ask ‘Why do you want to go home? What’s waiting for you? We can get help, your family is going to take care of the cat.’ They are worried about the animals, their home… So, then orienting him to the time of day, ‘it’s the middle of the night, you can’t do this right now, but your family can help you tomorrow during the daylight’. It was interesting, because without knowing a lot about him, I could ask questions, and the patient settled down very quickly. Before I would have just told him to calm down and sit still, I wouldn’t have asked him questions.
Another focus group participant reflected upon the need to assess for issues related to technological aspects of the environment in the acute care setting that elicit behaviours such as calling out for help: It was on night shift and I had a patient … She was screaming, and it came out of the blue, and I went in there, and said, ‘Can you tell me why you are screaming?’ Because I feel that patients are easily labeled, like the ‘screamer’, you know dismissing them as ‘they are just being behavioural’. But she said, ‘There is an animal in my bed’, and so, I said, ‘Tell me what type of animal’, like, I just investigated it, and … instead of saying ‘no there is no animal in your bed’, I played along, and I recognized myself that she was probably having an illusion because she was on an air bed, …and so the patient would feel movement. So I said, ‘let me take a look for you’, …and said, ‘I can understand that this is scary for you, but I’m not seeing the animal myself, but I do know that you are on something called an airbed’, and I explained the movement of the air bed to her, and she snapped right out of it and she was fine.
By asking detailed questions, this participant demonstrated the necessary competence to determine that the patient’s responsive behaviour experience was not pathological, rather, the person’s attempt to interpret sensations according to familiar experiences. The participants were exhibiting confidence that assessment data must go beyond the level of observation. The participants now understood that their clinical intuition based upon observation could also be confirmed by encouraging the person with dementia to give an account of their own experience with a symptom or condition.
Another participant explained their new ability to interpret motor changes associated with dementia and to use professional language to describe observed behaviours, stating: With the 7As, the apraxia; in practice we see a lot of things but didn’t have the knowledge or the label about what is behind those behaviours and what those behaviours are. Like, I had a patient who had a lot of trouble following commands, like for sitting, or if we were going to toilet, or sitting back on the bed, it got to that point where he didn’t seem to understand what to do, how to sit down, so I would be like, ‘sit down, like come on, sit down now’, but something wasn’t adding up for him, so when we took the course we got some techniques and tips and we learned to say it with the actions with it, like you say it and you do it with them as well, you show them what you want them to do. That actually did work with him, so that was a new thing for me. Before I didn’t know the label for it. That was helpful.
Contributing to a positive dementia care culture
Participants identified that completion of the program assisted them to realise that expanding their skills in responsive behaviour care would contribute to strengthening care for positive patient and staff outcomes. One participant stated: I think it is sometimes easy to be sucked into a negative culture on our floor, seeing behaviour can be draining and wear you down, so taking a course like this about behaviour and what the meaning is of it, you feel less um, I think I have a more positive approach about it. Like, okay, they are exhibiting this behaviour, but it’s okay, I think I’m less stereotypical, and less demeaning, and less “surgical” mind set toward the patients, which overall improves my care and thus their care.
One participant was proud to use their new knowledge to discuss the changes observed with other members of the interdisciplinary team. Well, the 7A’s were very useful and interesting. Something I did not see in nursing school. I have a patient that was oriented in all 3 spheres, but she was showing apraxia very clearly…, I went to the doctor, …and said, ‘I’m concerned that while she is oriented X 3, she is showing signs of dementia’, and I was able to use the terminology to sound more professional and I documented that she had apraxia and agnosia, and I said ‘Before this family meeting have you done more cognitive screening?’ And it gave me the terminology and… I was able to advocate for the patient.
Participants provided evidence that GPA eLearning reinforced their prior best practice knowledge, provided new communication skills and taught them that the person with dementia has remaining capacity to provide important assessment information if asked, and provided new language that they could use to communicate their dementia assessment findings to the health care team. Overall, the comments from participants supported the qualitative responses submitted at other points in the evaluation, confirming that GPA eLearning provided them with knowledge to implement tailored action and advocate for dementia care change to improve the overall quality-of-care for patients living with dementia.
Six to eight weeks post-GPA eLearning open-ended questions: Applying responsive behaviour approaches in clinical practice
Six to eight weeks after completing GPA eLearning, 29 participants provided responses to the same open-ended questions they had answered at the earlier two time points and described how they had approached any difficult episodes of responsive behaviour they encountered since completing GPA eLearning. Responses are presented here under two themes; Sustained Application of Person-Centred Approaches to Responsive Behaviour and Application of GPA Self-Protective Techniques.
Sustained application of person-centred approaches to responsive behaviour
When participants reflected six to eight weeks later about the most important thing they learnt in GPA, the most common response was that they now more fully understood the effects of dementia on the brain and why patients with dementia exhibit responsive behaviours. Respondents noted that they were using information provided to them about ‘A’s of dementia (agnosia, apraxia, etc.; Hamilton et al., 2020). They acknowledged they as caregivers need to identify the underlying causes of behaviours to defuse them. At six to eight weeks after GPA, many participants reported that they had continued to use best practices introduced or reinforced during GPA eLearning, either as a new practice or more consistent, conscious application of a previous practice. Recognition of the continued need for practice change was included in many participants’ responses. ‘I would get frustrated and say repetitive sayings such as “Please sit down”’ (#67), demonstrating an awareness that repeated commands can serve to exacerbate responsive behaviours. They acknowledged the patient’s need for personal space, adjusted the care delivery to a slower pace, listened carefully to the patient to identify potential triggers/strategies and tried to address other unmet needs using various means such as music or a quiet environment. ‘I have been more focused on slow clear communication and presenting with a pleasant face’ (#123). ‘I slow down and stop trying to focus on the task and instead focus on the patient’ (#12). ‘Watch an old movie, provide towels/doll/lego, etc., to keep hands & minds busy’ (#40). ‘Music does wonders’ (#29).
Participants’ realisation that they had invaded the patient’s personal space and evoked responsive behaviour, especially during incontinent care, is an important critical consciousness competency. Response details included providing acknowledgement of the emotional message of the patient, using non-pharmacological, person-centred approaches to distract and support the patient and accessing the family as a source of information to tailor care delivery. One participant indicated it was important to take ‘more time to talk to families to find out more about them prior to illness’ (#122). Another participant indicated that completion of GPA eLearning had assisted in the deeper understanding of the lived experience of the illness of dementia. The response was: I always try to put myself in the 'person’s shoes' to try to determine possible reasons for what may be triggering his/her behaviours so that I can choose possible appropriate strategies to resolve the responsive behaviour. (#83)
At baseline, participants often reported pressing on through a care attempt and managing the upset by trying to keep themselves calm, rather than addressing the underlying needs of the patient. Six to eight weeks post-eLearning, respondents were more likely to report that they acknowledged their patients’ emotional responses to care attempts and would provide emotional support, reassurance and rest breaks. As one individual stated, A patient was becoming very anxious because she didn't know where she was and wanted to go home. The patient started to cry hysterically and wave her arms around to the point that she was hitting people. I used a calm voice and validated the patient’s need for wanting to go home… Through calmly talking with her and taking the time to find out her concerns I learned she had to go to the bathroom but was unable to voice that. This intervention was effective. (#4)
Another participant provided a response indicating they understood the number and complexity of modifiable physical and psycho-social variables that the nurse must look for when considering the assessment and treatment of responsive behaviours. Ensure communication is as best as it can be (good lighting, glasses, hearing aids, writing things out), smile, make eye contact. Ensure pain is being treated. Ensure un-met needs are met (constipation, urinary retention, incontinence, hungry, thirsty, lack of sleep etc.). (#122) Another participant indicated that it was important to: …approach with calm voice and be aware of any threatening body language/body positioning that you may be exhibiting. Go in with a back-up plan in place if there is Hx of agitation or difficult/agitated behaviour. Speak to front line staff working with [the] patient that day to obtain Hx of what works/does not work/patient preferences. Offer alternatives for patients when possible - activities, change the conversation, using distractions to gently redirect. (#36)
Yet another example of a new appreciation of the complexity of responsive behaviour management is the following response: I try to gauge, through calm conversation, the correct time to ‘back off’. The most challenging part of this is balancing this strategy with the need to keep the patient and surrounding persons safe. We try to design the patient’s surroundings in such a way that, when the patient is aggressive/agitated/upset, the environment is safe. For example, patients prone to aggression, agitation, that are also at risk for falls, should have protective matting on the floor around them and other safety measures in place; otherwise, staff may not be able to use the STOP & GO approach strategy safely. (#28)
Overall, the six to eight week responses to the open-ended questions included much more detail and reflected a deeper understanding of the need for integrated approaches to unmet needs, both physical and psychological.
Application of GPA self-protective techniques
Six to eight weeks post-GPA, participants described their use of techniques they had learnt in GPA eLearning. These included sustained awareness of the need to alter their communication and the explicit naming of the interpersonal safety approaches embedded within the last modules of the program. Participants were ‘engaging with these individuals more often instead of being fearful of upsetting the situation’ (#75). They understood their role in provoking responsive behaviours and adjusted their communication techniques. For example, participants indicated that they continued in their awareness that prior to the GPA program they might have been firmly directive and controlling in their attempts to interact with a patient experiencing responsive behaviours. GPA communication strategies were useful to de-escalate responsive behaviours. ‘I used to talk in a firm aggressive voice that could have scared the patient and now I listen and acknowledge their feelings and desires’. (#5)
Participants also identified the specific strategies from the GPA module 3 and 4 content that they found highly useful on a daily basis; STOP & GO, Validation Therapy and Zones of Personal Space. For episodes that involved the need to protect oneself from hitting, punching or kicking, participants stated that Self-Protection Techniques such as the Grasp Reflex Release, One and Two Hand Grasp Releases as well as techniques to deal with attempts of patients to strike out were highly useful to avoid injury and reduce workplace stress. In other responses, the thumb release technique that assists learners to safely and gently remove themselves from a patient’s reflex or defensive grab (Advanced Gerontological Education, 2014) was mentioned as a particularly useful self-protective tool. As one participant stated: I have found the use of stroking the individual’s hand in the manner which we were taught an exceptionally useful tool. Very often this strategy can help and then calms the patient and myself, removing the environmental and physical ‘power struggle’. (#85)
Unlike at baseline, staff were aware of the importance of sharing accurate information about incidents of responsive behaviour through verbal and written means and by asking for help from available resources. Many respondents provided statements demonstrating their integration of all the principles of the course material, suggesting that body containment strategies might not be needed if emotional needs were acknowledged and met. As one group participant explained: In one case, security needed to be called because of violent behavior when trying to change the brief of a patient. It was for the safety of the patient who was agitated and everything went smoothly. I talked in a clear and calm voice, allowed the patient to explain their feelings and concerns, provided the time and patience that they needed in the current moment. The patient became less agitated and allowed me time to gather information regarding the patient’s feelings and expectations of me as their healthcare provider. (#108)
This example illustrates that the recipients of GPA training understood that episodes of responsive behaviour require a team approach, and that requesting help from available resources is an important strategy. Although the presence of security can contribute to team cohesion and greater safety, in this instance the respondent understood that the person-centred approaches learnt in the course were still necessary and useful to provide effective care.
Participants indicated an increased awareness of the need to integrate all competencies into care planning and delivery for best care. One participant responded: I use the following to prevent and diffuse responsive behaviours by: looking for triggers, keeping the person active as able, using positive verbal and body language, address the person by their preferred name, give the person space and offer control, communicate honestly with everyone involved in care. (#123)
Finally, participants indicated understanding of the importance for systematic sharing of information relevant to episodes of responsive behaviour. This included sharing with team members by verbal means but also by providing important details in formal documentation. As one participant wrote: Improved documentation in the chart helps to know which strategies had been tried before to prevent and/or de-escalate responsive behaviours and whether those strategies had been effective or not so that I would know quickly which strategies to implement for the responsive behavior at that time. (#83)
Overall, there were considerable enhancements in the responses given by the GPA intervention evaluation participants at six to eight weeks post-intervention when compared to baseline. The participants identified the importance of recognising unmet needs of the hospitalised patient that might be at the root of the responsive behaviour, understood to look for and identify possible triggers, accepted the need to ask for help from colleagues, mentioned the successful application of tailored validation approaches, mentioned the safety benefits of using the STOP & GO approach and stated the importance of adjusting communication strategies to connect with the patient such as adjusting their body language, facial expression and tone of voice so the patient could feel supported and safe in the unfamiliar and frightening environment of a hospital setting.
Discussion
Although acute care staff knowledge and confidence with dementia care best practices demonstrated at baseline can be considered at an acceptable level, quantitative and qualitative data revealed that both immediately after and six to eight weeks post-GPA eLearning, an advanced level of exemplary best practice is achievable and sustainable with introduction of specialised dementia care training such as GPA eLearning. As a result of completing the course, participants realised displays of upset were not pathological behaviours, rather, normal psychological behaviours of anxiety and fear the person with dementia experiences secondary to agnosia, apraxia and other cognitive and sensory deficits. Participants were then able to address unmet needs for reassurance and safety. Participants offered specific comfort statements relevant to the stimuli being misinterpreted by the patient, rather than motherhood statements such as ‘don’t worry, you are okay, there is nothing in your bed’. Examples of application of GPA principles indicated participants asked the patient what they were experiencing, and then ‘validated’ for the patient that there was indeed something being experienced, rather than dismissing or minimising expressions of fear. This advanced understanding and best practice communication is part of the GPA curriculum, module 2 (Advanced Gerontological Education, 2014).
Prior to GPA eLearning, most respondents relied on their own approach to achieve calmness as a behavioural de-escalation technique. Controlling one’s own emotional response in the face of responsive behaviour is a crucial skill. However, care staff who are well-educated about dementia care strategies should be able to provide more detailed examples of non-pharmacological person-centred interventions that extend beyond personal attempts to remain calm (Canadian Gerontological Nursing Association, 2020; Legere et al., 2017; Yous, Ploeg et al., 2020a; Yous, Schindel Martin et al., 2020b). After GPA eLearning, participants demonstrated newfound understanding of person-centred distraction techniques, dementia communication skills and appropriate body containment strategies that are safe, easily applied and effective. In keeping with the progressive hierarchical models of learning objectives classified in revised versions of Bloom’s Taxonomy (Adams, 2015; Anderson & Krathwohl, 2001; Su & Osisek, 2011), participants in this project demonstrated learning outcomes of a higher order level of application, and most importantly achieved the highest order of knowledge building; ‘creation’ of novel, tailored interventions specific to their patients’ contextual experience of responsive behaviour (Adams, 2015). This is particularly significant because while ‘understanding and awareness’ levels are necessary for building exemplary best practice, it is achievement of higher order levels of learning for application and tailoring that are essential to meet the complex and unique needs of older people living with dementia when they are admitted to acute hospitals with medical co-morbidities. Findings indicate GPA eLearning is an effective intervention essential for acute care hospitals to deliver patient-centred care that older people living with dementia and their families require for positive outcomes.
The GPA curriculum includes factors recently identified in a review of dementia education programs as being associated with a greater likelihood of positive outcomes, including the inclusion of practical strategies that can be easily applied in clinical settings, program content suitable to the specific role and workplace of those attending, at least some face-to-face delivery of material by a skilled facilitator, and the training of in-house ‘champions’ to promote sustainability (Surr & Gates, 2017). A blended learning model, like the one used in the present evaluation with both online and classroom components, has been proposed as particularly effective strategy for delivering dementia-related education (Innes et al., 2012). The effectiveness of dementia education is also enhanced by the support of managers and leaders, which gives staff the permission and confidence to make changes in culture and practice, and the availability of sufficient staff and resources (Handley et al., 2017; Surr et al., 2018). Because acute care hospital workforces are ageing and can have relatively high turnover, a plan for sustainability of dementia education within an organisation is essential (Brooke & Ojo, 2018). GPA’s in-house certified coach model ensures that continued training remains accessible.
Interpretation of the findings suggest that the cohort, the majority of whom were nurses, experienced professional practice growth after the GPA eLearning program. Statistically significant changes in self-efficacy, competence and knowledge of dementia care were observed, as in previous evaluations of GPA implementations (Schindel Martin et al., 2016). These quantitative findings, together with descriptive evidence that these participants applied non-pharmacological interventions with more confidence and precision, acquired greater self-awareness through reflection, and tailored communication to include asking critical questions rather than giving false reassurance, all support the advancement of their critical thinking. These findings align with our hypothesis that dementia education specific to higher level responsive behaviours will expand the capacity for hospital staff to deliver care that is informed by empiric, ethical, aesthetic and personal knowledges (Carper, 1978; Chinn & Kramer, 2018), essential for best practice. In support of on-going best-practice change for older people with responsive behaviours, the organisation within which this quality improvement project was implemented is developing a sustainability plan that will ensure the continual implementation of GPA principles and training.
Implementation challenges included participant attrition that could have been improved by incentives for completion of evaluation measures. Participants with outdated browsers encountered technical issues with the eLearning format or with enrolment in the course, but these issues were resolved via online or telephone support. Additionally, the project time frame did not allow evaluation to take place later than six to eight weeks post-intervention. Evaluation of outcome measures at six months and one-year post-GPA would allow more robust statements about sustainable impact. Finally, like most published dementia education evaluations (Abley et al., 2019; Surr & Gates, 2017), this project focused on staff-related outcomes of the GPA eLearning program, and funding did not allow for the collection of data about the impact on quality of life for patients with dementia. It would be beneficial for future projects implementing the GPA eLearning program to collect patient-related outcome variables such as length of stay, frequency as well as duration and intensity of behavioural incidents, chemical and physical restraint use and patient-family experience to provide a more complete understanding of the impact of the GPA eLearning in the acute care sector.
Staff participants wanted more time to review and practice the body containment strategies demonstrated using video clips embedded within Module 4 of GPA eLearning to feel comfortable applying them in their clinical practice. Participants also asked for opportunity to review the core content on a regular basis. Sessions during which GPA techniques can be reviewed and reinforced by in-house GPA certified coaches will be important for the sustainability of GPA knowledge and best practice skills in the future. This is particularly important given prior studies showing that improvements in person-centred dementia care practice often are not sustained long-term without regular reinforcement of training (Yous, Ploeg et al., 2020a; Yous, Schindel Martin et al., 2020b). Lastly, provision of equipment to engage patients experiencing responsive behaviours in preferred activities would be useful for staff in acute hospital settings. Activities such as these mitigate boredom from social isolation and a program wherein volunteers facilitate such activities using purchased equipment would provide staff and families with the means to provide non-pharmacological interventions (Yous, Ploeg et al., 2020a; Yous, Schindel Martin et al., 2020b).
The GPA eLearning program was successfully introduced as specialised dementia care training for interdisciplinary staff employees on five participating in-patient medicine units in a large Ontario hospital system. GPA was received positively by staff who participated in this program evaluation. Quantitative findings revealed that after GPA eLearning, participants showed significant increases in overall self-efficacy, competence and knowledge to perform respectful, person-centred care to older adults living with dementia who experience responsive behaviours during admission to hospital. Moreover, these increases were sustained six to eight weeks post-intervention. Qualitative findings demonstrate that participants were able to apply GPA principles in their practice, and that the four-module GPA curriculum assists learners to reach the most complex levels of learning objectives (Adams, 2015), including the meaningful synthesis of information and subsequent creation and implementation of safe, respectful and highly-tailored, non-pharmacological, relational interventions for management of responsive behaviours. Without such synthesis, there is a risk that staff knowledge of responsive behaviours will be limited to recognition, understanding and awareness without the capacity for flexible application of patient-centred strategies. Given the complex nature of responsive behaviours, this type of education expands the capacity for professional caregivers to meet patients’ needs.
We strongly recommend that hospitals incorporate dementia education that addresses responsive behaviours for professional caregivers to expand their capacity to deliver tailored care to patients living with dementia. GPA is one such program, and here its eLearning format was demonstrated as effective at providing staff with the needed knowledge and skills to self-reflect, then apply all fundamental ways of knowing (Carper, 1978) to responsive behaviours. Participants thereby interacted with dignity and compassion and in a person-centred fashion, aligning with the hospital’s commitment to provide patient-centred care and to enhance the patient experience.
Footnotes
Acknowledgements
The authors would like to wholeheartedly acknowledge and thank Laurie McKellar, BScN, for her leadership, passion, and diligence as the Project Lead for the GPA eLearning project. We would also like to thank Tim Rice, Ann Turcotte, and Sherri Lawson, Directors within the London Health Sciences Centre for their leadership support. Finally, we acknowledge the efforts and dedication of the interdisciplinary group of educators and clinicians, including manuscript author Dr Lori Schindel Martin, who collaboratively developed the GPA curriculum.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Foundation for Healthcare Improvement (CFHI) in partnership with the Canadian Frailty Network, who jointly funded participation in the Acute Care for Elders (ACE) Collaborative.
![]()