
Abstract
Background
Agitation is a common neuropsychiatric symptom of Alzheimer’s disease; however, limited information exists on how measurable changes in agitated behaviors relate to overall caregiver experience. We sought to describe agitated behaviors measured by the Cohen-Mansfield Agitation Inventory (CMAI) score among individuals with Alzheimer’s disease living in US community-based settings and experience of their caregivers.
Methods
An online survey was conducted (08/26/2021-09/24/2021) among adult caregivers who lived with and provided unpaid care for an individual with Alzheimer’s disease. The 3-part survey involved (1) informed consent and screening; (2) CMAI assessment (total and sub-scores for four agitation factors); (3) characteristics and outcomes of caregivers and individuals with Alzheimer’s disease. Descriptive statistics are reported. Association between the CMAI total score and caregiver burden (measured using the Zarit Burden Interview), mental health (measured using the Patient Health Questionnaire 4-item), and work/activity impairment (measured using the Work Productivity and Activity Impairment: Caregiver scale) was estimated using regression models.
Results
A total of 250 caregivers (mean age: 44.5 years; 55.2% male; 86.4% White) completed the survey. Based on the CMAI, 99.6% of individuals with Alzheimer’s disease (mean age: 68.6 years; 55.2% male; 83.2% White) experienced ≥1 agitated behavior in the past 2 weeks. Caregivers reported providing an average of 39.1 hours of care per week for individuals with Alzheimer’s disease (additional non-paid and paid care provided by other caregivers was 58.8% and 38.4%, respectively); 60.8% of caregivers had a high caregiving burden, 35.2% experienced moderate-to-severe distress, and 68.2/64.0% had impairment in work/daily activities. Agitation among individuals with Alzheimer’s disease was associated with significantly poorer caregiver outcomes.
Conclusions
Individuals with Alzheimer’s disease frequently experience several different agitated behaviors. Effective management of agitated behaviors is important and has the potential to improve the overall caregiver experience.
Keywords
Introduction
Alzheimer’s disease affects approximately 6.5 million Americans aged ≥65 years (Alzheimer's Association, 2022). The condition progresses along a continuum from asymptotic preclinical disease to mild cognitive impairment to dementia (Alzheimer's Association, 2022; Jack et al., 2018). Dementia due to Alzheimer’s disease is characterized by the loss of cognitive functioning that interferes with the individual’s ability to perform everyday activities, along with a wide range of neuropsychiatric symptoms that may impact the quality of life (Desai et al., 2012; Livingston et al., 2017; World Health Organization (WHO), 2021). These neuropsychiatric symptoms associated with Alzheimer’s disease can be categorized into mood-related disturbances (e.g., anxiety, apathy, depression, and euphoria), sleep disturbances (e.g., insomnia, hypersomnia, and day-night reversal), psychotic behaviors (e.g., delusions and hallucinations), and agitation (e.g., physical and verbal aggression, excessive motor activity such as pacing and restlessness, problem wandering, and sexual disinhibition) (Aigbogun et al., 2019; Desai et al., 2012; Sano et al., 2023).
The impact of neuropsychiatric symptoms of Alzheimer’s disease on caregiver experience has been recognized (Allegri et al., 2006; Dauphinot et al., 2016; Delfino et al., 2021; Fischer et al., 2012; Garcia-Martin et al., 2023; Isik et al., 2019). Symptoms such as hallucinations, anxiety, unusual motor behavior, restlessness, disinhibition, and sleep disturbance have been reported to be predictors of burden in primary informal caregivers of individuals with Alzheimer’s disease (Allegri et al., 2006). Other studies have suggested that neuropsychiatric symptoms were associated with reduced employment income among caregivers (Kales et al., 2015; Lindeza et al., 2020). Meanwhile, increased caregiver stress may in turn worsen the relationship between the caregiver and the individual with Alzheimer’s disease, exacerbating the neuropsychiatric symptoms (Isik et al., 2019). A study among caregivers of community-based individuals with dementia, the majority with Alzheimer’s disease, found that poor relationship with caregiver was associated with greater agitation displayed by individuals with dementia (Hamel et al., 1990).
Agitation is among the most common neuropsychiatric symptoms of Alzheimer’s disease and poses a major challenge for the treatment and management of the condition (Howard, 2016; Jones et al., 2021; Sano et al., 2023). Furthermore, prior studies suggested that the caregiver experience associated with neuropsychiatric symptoms in Alzheimer’s disease may be largely driven by disruptive behaviors, including agitation (Cheng, 2017). In an observational study among caregivers of noninstitutionalized individuals with dementia, agitation was among the top neuropsychiatric symptoms causing the most burden, affecting over 85% of caregivers (Garcia-Martin et al., 2023). Agitated behaviors in those with Alzheimer’s disease can also be a source of anxiety for caregivers (Cohen-Mansfield, 2008). A study among professional caregivers in nursing homes found that agitation was associated with the highest mean distress score among neuropsychiatric symptoms displayed by residents of dementia special care units (over half with Alzheimer’s disease), with the level of distress increasing with symptom severity (Zwijsen et al., 2014).
The Cohen-Mansfield Agitation Inventory (CMAI) is a caregiver-rated questionnaire that measures the frequency of 29 different agitated behaviors (Cohen-Mansfield, 1991). The CMAI is widely used in clinical trials to assess the impact of pharmacological and non-pharmacological interventions on agitated behaviors (Ballard et al., 2018; De Mauleon et al., 2021; Porsteinsson et al., 2014). However, there has been a lack of real-world studies that used this clinical measure of agitation to tie the measurable changes in agitated behaviors of individuals with Alzheimer’s disease to caregiver experience (Aggarwal et al., 2023), leading to challenges in reconciling clinical trial results with potential impact of pharmaceutical treatments for the management of agitated behaviors in the real world. To bridge this research gap and help understand how changes in CMAI measurements in clinical trials may be expected to impact those caring for individuals with Alzheimer’s disease, especially unpaid caregivers living with the individuals, this study was conducted to examine agitated behaviors among community-dwelling individuals with Alzheimer’s disease in the United States (US), as measured by the CMAI. The aim was to describe the overall experience of unpaid caregivers regarding the care they provided in the past year, the burden of caregiving, caregiver mental health, and work and activity impairment, as well as the association of agitated behaviors with these caregiver outcomes.
Methods
Data source and study population
An online survey was completed by caregivers living with individuals with Alzheimer’s disease. Caregiver participants were recruited from a well-established online panel proprietary to Dynata (Dynata, 2024). The panel comprises geographically and demographically diverse individuals recruited through multiple channels, including partnerships with trusted loyalty programs, online banners ads, TV advertising, emails, apps, websites, and offline methods. Panel members are fully profiled to capture their key characteristics and ailment (e.g., diseases, caregiving), including through unaided questions, which enable recruitment of targeted populations.
Email invitations containing the survey link were sent by Dynata to members of their existing US panel who met the eligibility criteria of the current study (described below). Panel members who received the email invite and who were willing to participate in the survey used the link to respond to the questionnaire. All data were collected online between August 26, 2021, and September 24, 2021. Dynata pre-estimated a target sample size of 250 based on their eligible panel members. They shared invites to participate with all panel members who were eligible, to which the investigator had no visibility to maintain anonymity; the sample received by the investigator comprised all eligible respondents who answered to the email invite.
Adult caregivers who were comfortable reading and understanding English were eligible to participate in the study if they (1) lived with an individual with Alzheimer’s disease in a community-based setting (e.g., private home, retirement community, independent living group, senior housing complex) in the US at the time of data collection and (2) provided unpaid care for an individual with Alzheimer’s disease (identified based on caregiver self-report) at the time of data collection. Caregivers were compensated $85 for participating in the survey.
Survey design
This descriptive cross-sectional study utilized a survey consisted of an online questionnaire comprising three sections: (1) informed consent, screening, information sheet, and written educational material; (2) CMAI assessment and questions regarding the perceived impact of agitated behaviors on caregivers; and (3) characteristics and outcomes of caregivers and individuals with Alzheimer’s disease, including caregiver burden, mental health, and caregiver work and activity impairment.
The target completion time of the online questionnaire was approximately 60 minutes, and participants were instructed to complete the survey over up to 3 days. Caregivers were asked to complete the online questionnaire on their own. As the CMAI is typically administered by a trained professional, educational materials and detailed definitions of agitated behaviors were provided to help respondents accurately complete the assessments.
To assess the robustness of using a clinical measure in a real-world setting, a sensitivity analysis was conducted in a subset of caregivers who were asked to complete a second CMAI assessment two weeks after completing the questionnaire based on personal notes. The aim was to determine whether changes in the CMAI scores would be observed when respondents were advised to take notes in preparation for the second assessment.
Prior to data collection, pilot tests were conducted with four eligible caregivers in the form of semi-structured virtual interviews to review the survey content, ensure the survey was user-friendly and easy to complete/understand. Based on the feedback from the pilot tests, minor wording refinements were implemented.
Measures and outcomes
For individuals with Alzheimer’s disease, demographics and clinical characteristics, which included the presence of neuropsychiatric symptoms identified with the Neuropsychiatric Inventory Questionnaire (NPI-Q) (Kaufer et al., 2000), were collected through the caregiver survey. Based on the CMAI, the proportions of individuals with Alzheimer’s disease with aggressive agitation, physically non-aggressive agitation, and verbal agitation were determined (these categories of agitation are defined in the CMAI manual and are derived by an algorithm that incorporates both the number and frequency of behaviors (Cohen-Mansfield, 1991)). Data on the frequency and disruptiveness of each of the 29 CMAI agitated behaviors exhibited by the individuals with Alzheimer’s disease in the preceding two weeks were collected. The frequency of each behavior was scored using a 7-point scale from “never” (1 point) to “several times an hour” (7 points). The CMAI total score was derived by summing the frequency responses for all CMAI agitated behaviors. The CMAI subscores for the four factors of agitation (as defined by Rabinowitz et al., 2005; Rabinowitz et al., 2005); i.e., aggressive behavior, physically non-aggressive behavior, verbally agitated behavior, and hiding and hoarding behavior), and an “other” category to capture remaining behaviors, were derived by summing the frequency responses for the CMAI agitated behaviors included in the corresponding factors (Cohen-Mansfield, 1991).
For caregivers, several features were assessed. These features included (1) demographics; (2) clinical characteristics; (3) caregiving characteristics in the year prior to data collection; (4) need for caregiver/others to physically distance themselves from the individual with Alzheimer’s disease due to agitated behaviors; (5) description of the most bothersome agitated behaviors and those most likely to influence long-term care facility transfer decisions; (6) impact of the COVID-19 pandemic on agitated behaviors and caregiver responsibilities; (7) caregiver burden; (8) mental health outcomes; and (9) work and activity impairment.
Specifically, caregiver burden was measured using the Zarit Burden Interview (ZBI-12), which scores range from 0 to 48 points, with higher scores indicating greater caregiver burden (scores >20 points indicate a high degree of burden) (Center to Advance Palliative Care (CAPC), 2018). For caregiver mental health outcomes, distress was measured using the Patient Health Questionnaire 4-item (PHQ-4), which scores range from 0 to 12 points, with higher scores indicating greater distress (scores of 6–12 indicate moderate-to-severe distress) (Kroenke et al., 2009). Likelihood of generalized anxiety disorder was measured using the Generalized Anxiety Disorder-2 (GAD-2) subscale, which scores range from 0 to 6 points, with scores of ≥3 indicating a high likelihood of having generalized anxiety disorder (Kroenke et al., 2007). Likelihood of major depressive disorder was measured using the PHQ-2 subscale, which scores range from 0 to 6 points, with scores of ≥3 indicating a high likelihood of having major depressive disorder (Kroenke et al., 2003). Caregiver work and activity impairment was measured using the Work Productivity and Activity Impairment: Caregiver (WPAI-CG) scale, in which outcomes are expressed as impairment percentages, with higher numbers indicating greater impairment and less productivity (Reilly Associates, 2002).
Statistical analyses
Descriptive statistics were reported for all study measures and outcomes using means, medians, and standard deviations for continuous variables and frequency counts and percentages for categorical variables.
Regression analyses were conducted to estimate the association between the CMAI total score and outcomes of interest (i.e., caregiver burden, mental health, and work and activity impairment). To understand whether certain behavior categories were more likely to drive the association between the CMAI total score and outcomes of interest, regression analyses were also conducted using the CMAI subscores for the four factors of agitation (i.e., aggressive behavior, physically non-aggressive behavior, verbally agitated behavior, hiding and hoarding behavior) as independent variables.
All regressions were adjusted for caregiver age and gender as well as the age, gender, severity of Alzheimer’s disease, and time since diagnosis of Alzheimer’s disease of those receiving care from the caregivers. For categorical outcomes (i.e., caregiver burden and mental health), odds ratios were estimated using logistic regression models. For continuous variables (i.e., caregiver work and activity impairment), differences were estimated using ordinary least square regression models. All analyses were pre-planned and performed using SAS Enterprise Guide software.
Ethical approval and informed consent statements
Caregiver participants provided their informed consent electronically prior to responding to the survey questions. The study did not collect any personal-identifiable information and was approved under the exempted category through an expedited review by the Western Copernicus Group Institutional Review Board (Study No: 1304901) under 45 CFR § 46.104(d)(2), because the research only includes interactions involving educational tests, survey procedures, interview procedures, or observations of public behavior; and the information obtained is recorded by the investigator in such a manner that the identity of the human subjects cannot readily be ascertained, directly or through identifiers linked to the subjects.
Results
Sample characteristics
A total of 250 eligible caregivers completed the survey, and their responses were included in the analyses.
Demographic and clinical characteristics of individuals with Alzheimer’s disease. a
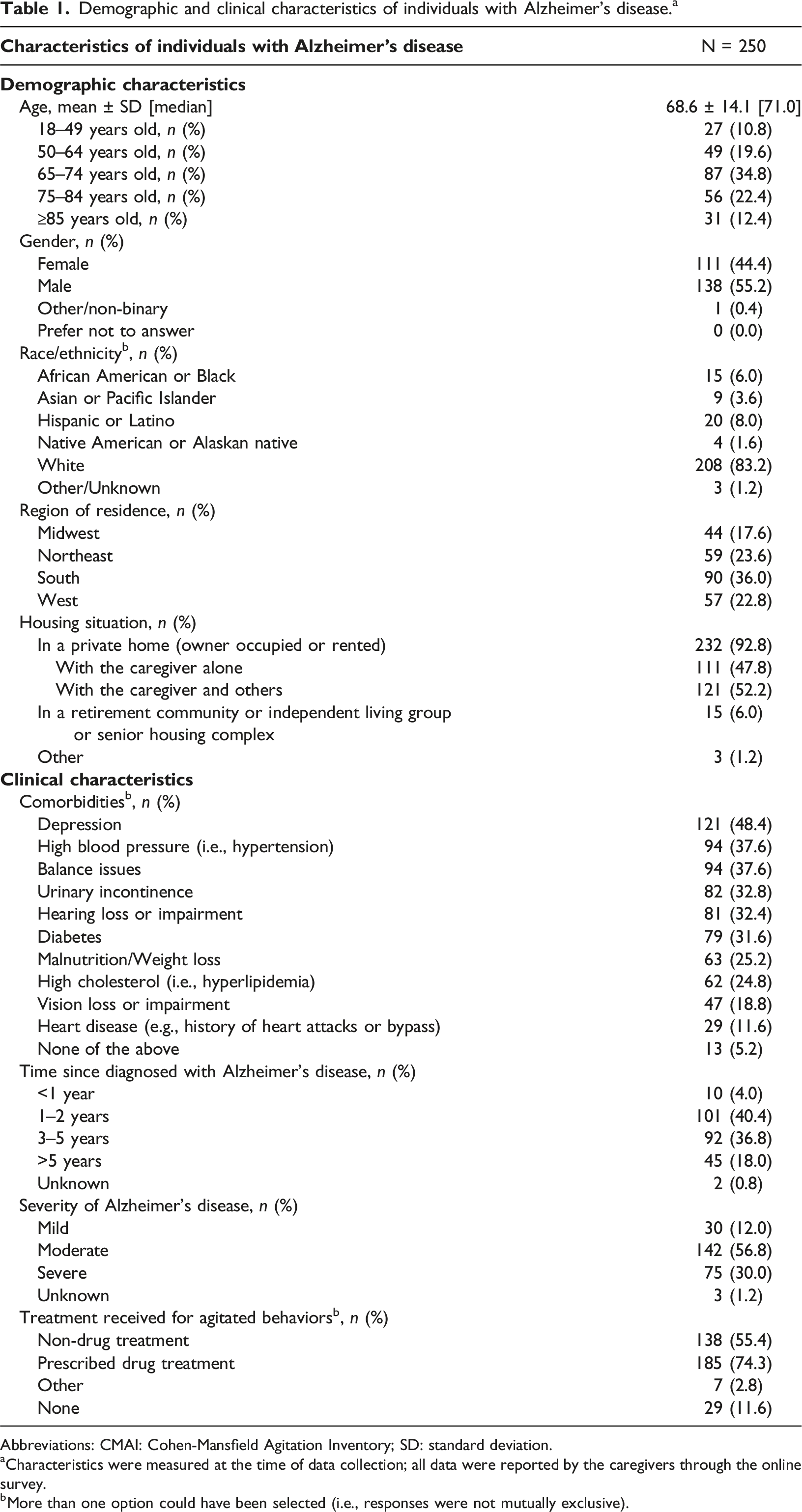
Abbreviations: CMAI: Cohen-Mansfield Agitation Inventory; SD: standard deviation.
aCharacteristics were measured at the time of data collection; all data were reported by the caregivers through the online survey.
bMore than one option could have been selected (i.e., responses were not mutually exclusive).
Demographic and clinical characteristics of caregivers. a
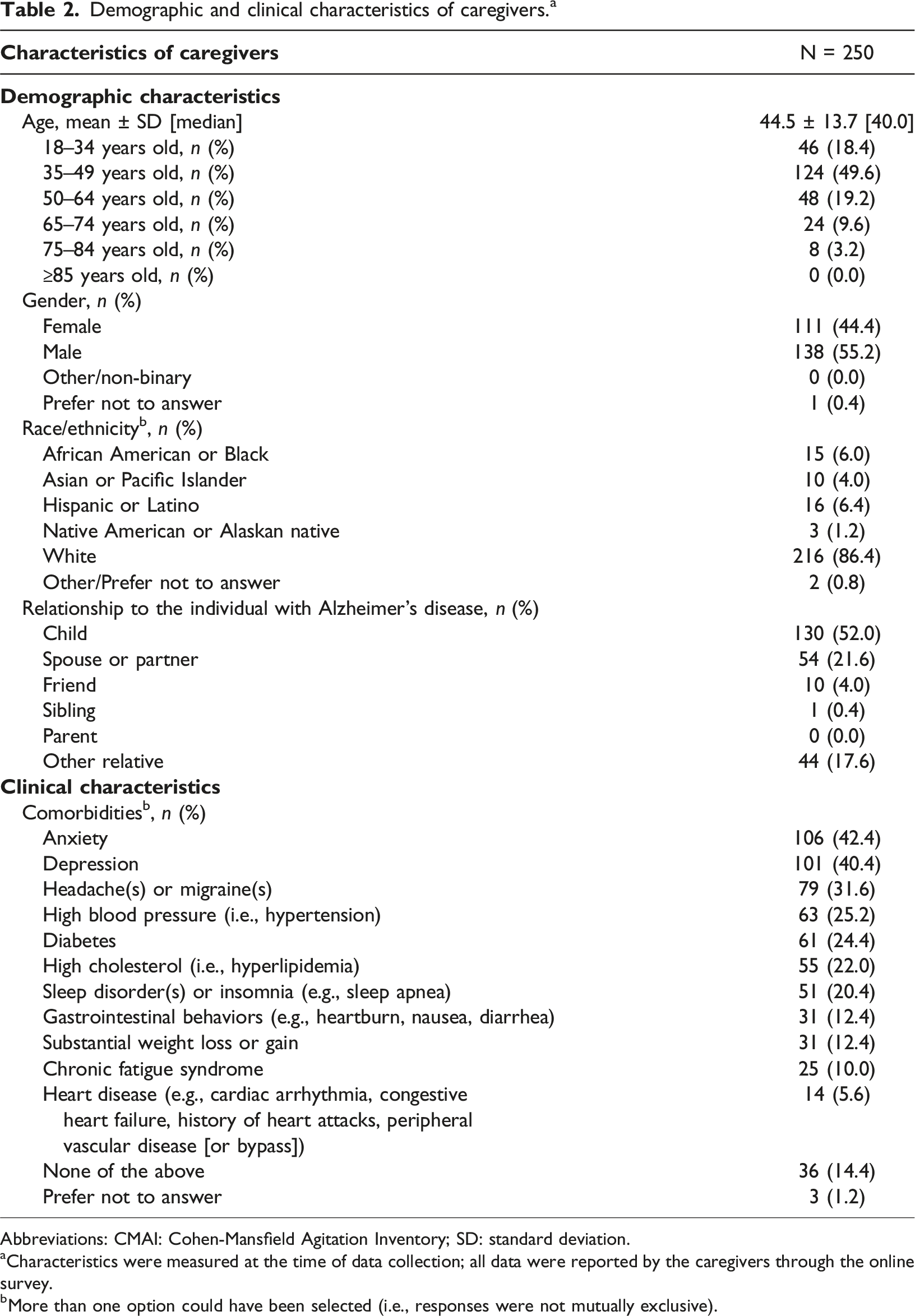
Abbreviations: CMAI: Cohen-Mansfield Agitation Inventory; SD: standard deviation.
aCharacteristics were measured at the time of data collection; all data were reported by the caregivers through the online survey.
bMore than one option could have been selected (i.e., responses were not mutually exclusive).
In the year prior to data collection, caregivers spent an average of 39.1 hours per week caring for individuals with Alzheimer’s disease due to the condition, with 25.2% of caregivers spending >40 hours per week. In addition to the caregiving provided by the caregivers completing the survey, many individuals with Alzheimer’s disease also received additional non-paid (58.8%) and paid (38.4%) care from other caregivers. The average number of hours of other non-paid and paid care received by the individuals with Alzheimer’s disease was 26.7 and 27.1 hours per week, respectively (Figure 1). Caregiving provided by caregivers completing the survey and other paid and unpaid caregivers. Notes (1). Paid caregiving included assistance, care, supervision, or companionship provided by employees of a residential care facility, as well as the use of adult daycare. This was evaluated among caregivers that indicated paid help was provided. (2). This was evaluated among caregivers that indicated other non-paid help was provided.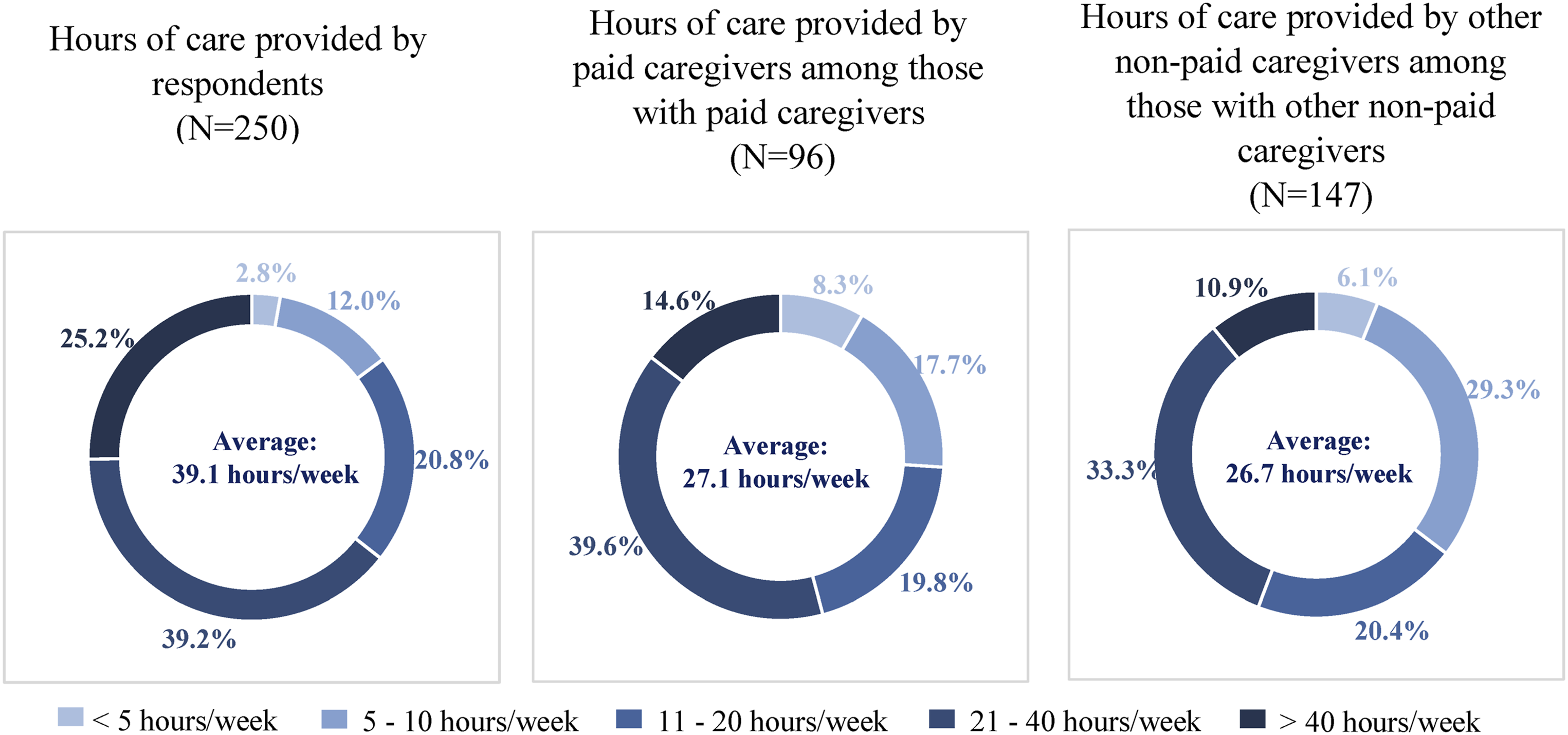
Agitation among individuals with Alzheimer’s disease
Based on the NPI-Q, agitation was the most prevalent neuropsychiatric symptom among individuals with Alzheimer’s disease, with 83.2% experiencing any symptoms on the agitation/aggression scale.
The CMAI showed that at the time of data collection, nearly all (99.6%) individuals with Alzheimer’s disease exhibited ≥1 agitated behavior in the past 2 weeks. Based on the agitation categories defined in the CMAI manual (Cohen-Mansfield, 1991), 83.6%, 85.6%, and 86.0% were considered to have aggressive agitation, physically non-aggressive agitation, and verbal agitation, respectively.
Across all CMAI factors of agitation (Rabinowitz et al., 2005), the most prevalent agitated behaviors included repetitive sentences or questions (94.8%), complaining (90.8%), negativism (88.4%), general restlessness (88.4%), and pacing or aimless wandering (86.8%) (Figure 2). While the frequency of the agitated behaviors varied significantly by, and within, the CMAI factors, each of the behaviors were exhibited at least once a day by more than 1 in 3 individuals with Alzheimer’s disease. Additionally, agitated behaviors exhibited at higher frequencies were generally rated more disruptive by caregivers (Supplemental Figure 1). Frequency of agitated behaviors as measured by the CMAI.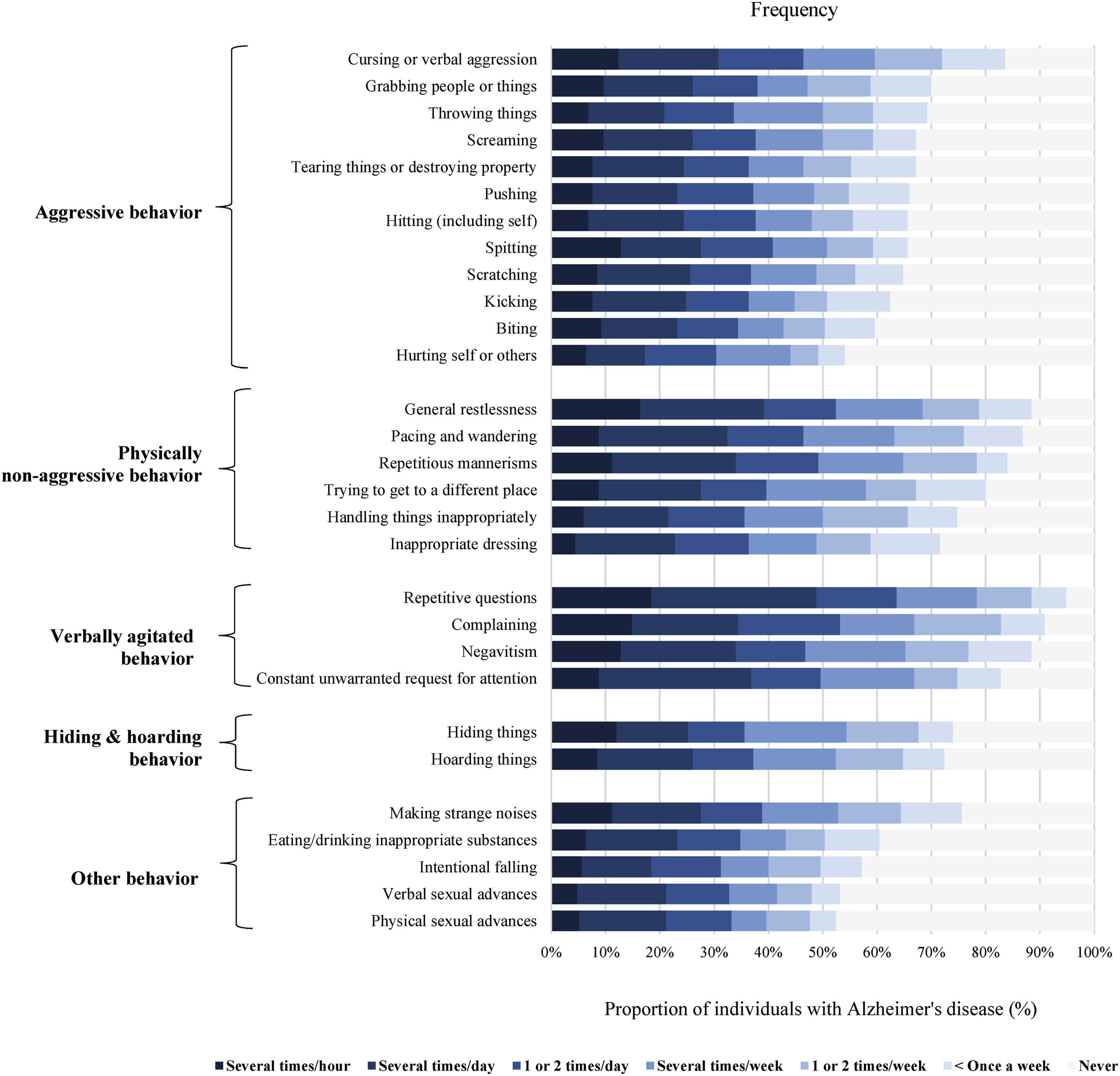
The CMAI total score remained consistent for the subset of caregivers (N = 75) who completed a second CMAI assessment after taking notes on behaviors for 2 weeks (Supplemental Figure 2).
Impact of agitated behaviors on caregivers
More than 1 in 4 caregivers reported that they or others “nearly always” (3.2%) or “quite frequently” (24.5%) needed to be physically distanced from the individual with Alzheimer’s disease due to agitated behaviors; the proportions of caregivers reporting “sometimes,” “rarely,” and “never” were 34.9%, 21.3%, and 16.1%, respectively.
The most bothersome agitated behaviors to the caregivers included cursing or verbal aggression (28.5%), spitting (22.5%), repetitive sentences or questions (18.9%), hitting self or others (18.1%), and constant unwarranted requests for attention or help (16.5%) (Figure 3). Except for repetitive sentences or questions, these most bothersome agitated behaviors reported were not among the most prevalent agitated behaviors reported for individuals with Alzheimer’s disease in this study. Perceived impact of agitated behaviors.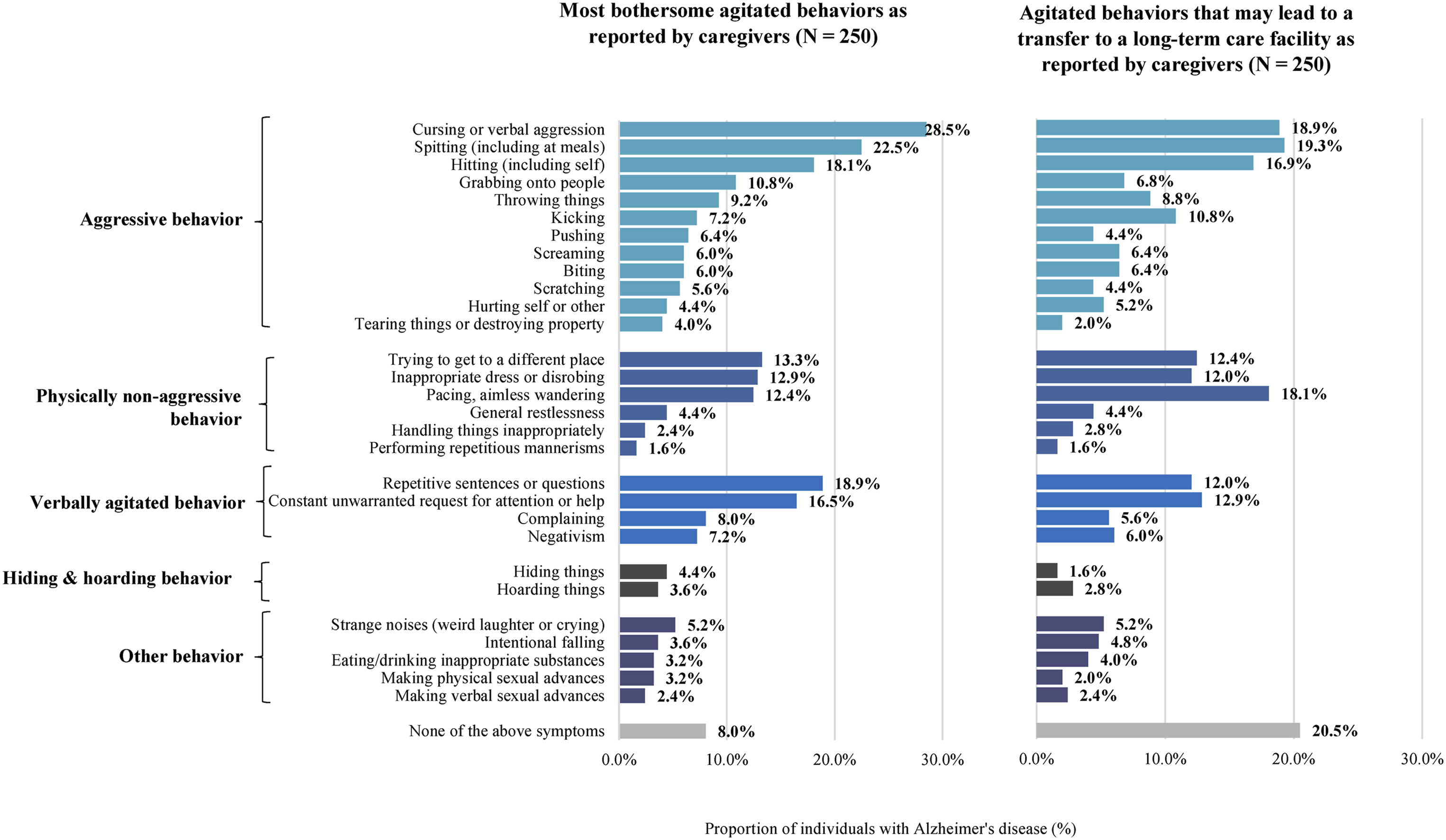
The behaviors most likely to influence caregivers’ decision to transfer an individual with Alzheimer’s disease to long-term care were spitting (19.3%), cursing or verbal aggression (18.9%), pacing or aimless wandering (18.1%), hitting self or others (16.9%), constant unwarranted requests for attention or help (12.9%), and trying to get to a different place (e.g., out of the room, building; 12.4%) (Figure 3).
Caregiver burden, mental health, and work/activity impairment.
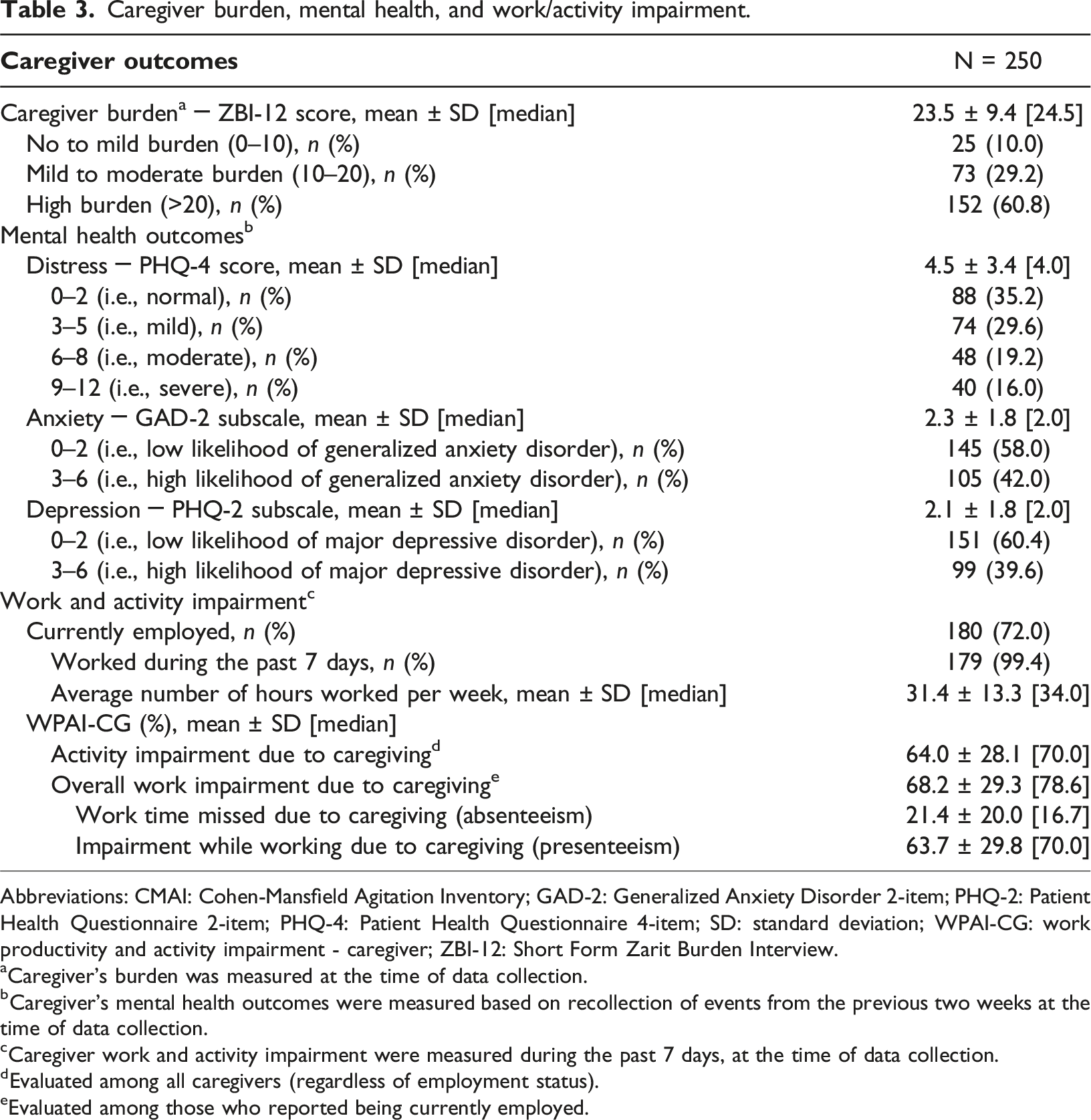
Abbreviations: CMAI: Cohen-Mansfield Agitation Inventory; GAD-2: Generalized Anxiety Disorder 2-item; PHQ-2: Patient Health Questionnaire 2-item; PHQ-4: Patient Health Questionnaire 4-item; SD: standard deviation; WPAI-CG: work productivity and activity impairment - caregiver; ZBI-12: Short Form Zarit Burden Interview.
aCaregiver’s burden was measured at the time of data collection.
bCaregiver’s mental health outcomes were measured based on recollection of events from the previous two weeks at the time of data collection.
cCaregiver work and activity impairment were measured during the past 7 days, at the time of data collection.
dEvaluated among all caregivers (regardless of employment status).
eEvaluated among those who reported being currently employed.
When asked about the impact of the COVID-19 pandemic, most caregivers (76.8%) felt that their caregiving responsibilities increased due to the pandemic. Among caregivers who indicated the presence of ≥1 agitated behavior in the individual with Alzheimer’s disease they cared for (99.6%), 64.3% reported that the frequency the behaviors increased due to pandemic.
Association between the CMAI total score and selected caregiver outcomes
Association between the CMAI total score and selected caregiver outcomes.
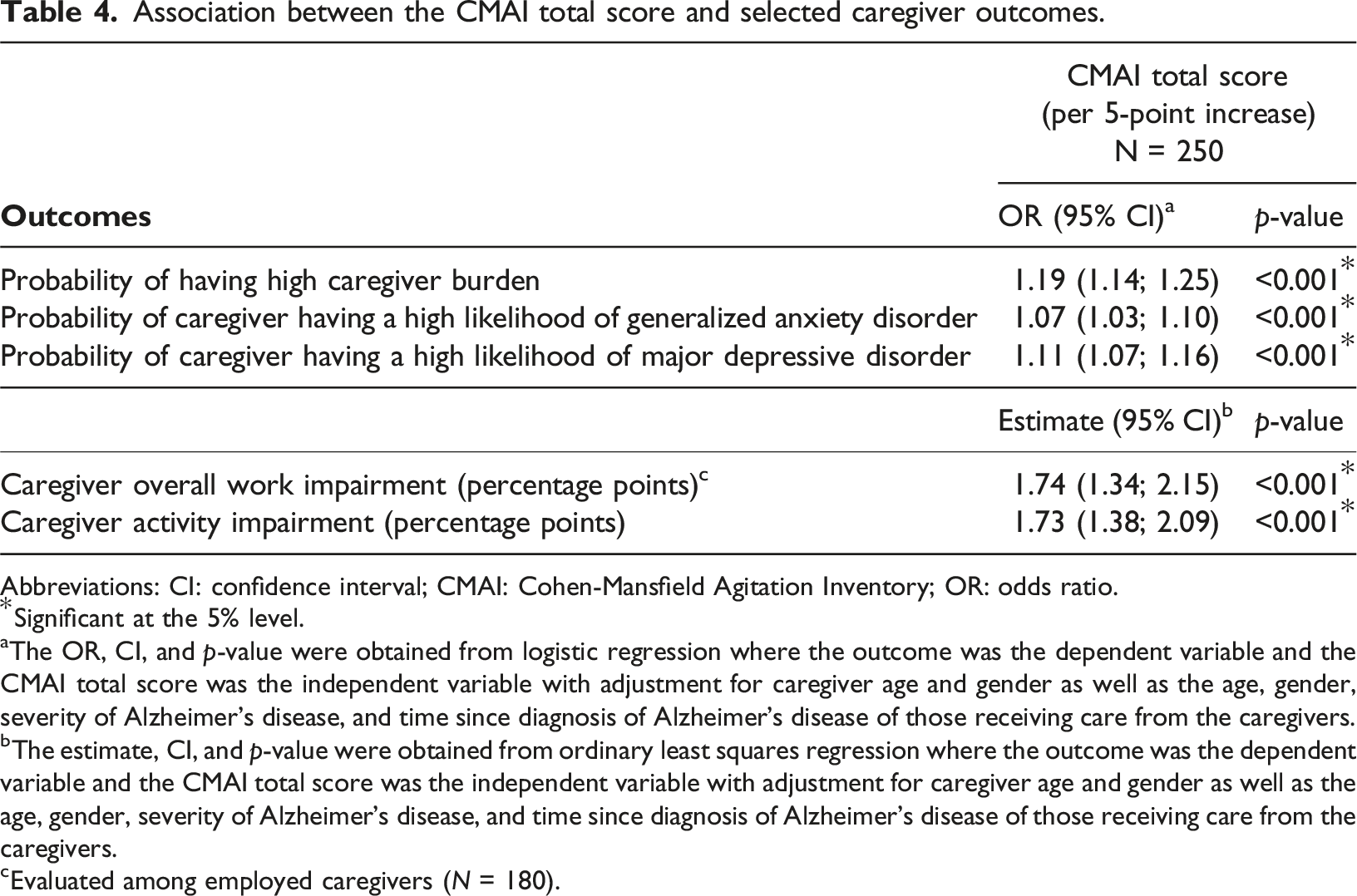
Abbreviations: CI: confidence interval; CMAI: Cohen-Mansfield Agitation Inventory; OR: odds ratio.
*Significant at the 5% level.
aThe OR, CI, and p-value were obtained from logistic regression where the outcome was the dependent variable and the CMAI total score was the independent variable with adjustment for caregiver age and gender as well as the age, gender, severity of Alzheimer’s disease, and time since diagnosis of Alzheimer’s disease of those receiving care from the caregivers.
bThe estimate, CI, and p-value were obtained from ordinary least squares regression where the outcome was the dependent variable and the CMAI total score was the independent variable with adjustment for caregiver age and gender as well as the age, gender, severity of Alzheimer’s disease, and time since diagnosis of Alzheimer’s disease of those receiving care from the caregivers.
cEvaluated among employed caregivers (N = 180).
Among CMAI subscores, the aggressive behaviors subscore was significantly associated with a high caregiving burden, work impairment, and activity impairment, whereas the verbally agitated behaviors subscore was significantly associated with higher risks of generalized anxiety disorder and major depressive disorder (all p < .05; Supplemental Table 1).
Discussion
This study characterized the relationship between agitated behaviors in individuals with Alzheimer’s disease, as measured by the CMAI, and caregiver experience in US community-dwelling individuals. The study found that nearly all individuals with Alzheimer’s disease exhibited one or more agitated behaviors in the past two weeks of data collection, and these behaviors occurred daily for over one-third of individuals with Alzheimer’s disease. The high frequency of agitation in Alzheimer’s disease is largely consistent with published reports, although prior estimates varied depending on study methodologies and populations (Ballard & Corbett, 2013; Sano et al., 2023). Notably, the frequency of some agitated behaviors found in the current study such as sexual advances was higher than expected from clinical observations (Alagiakrishnan et al., 2005; Chapman et al., 2019), suggesting that caregivers may be underreporting potentially treatable agitated behaviors to clinicians during routine medical care. Potential reasons for underreporting may include embarrassment (e.g., if individuals with Alzheimer’s disease display inappropriate sexual behaviors (Cohen-Mansfield, 2008)), poor appreciation that agitation might be assessed medically and even treated, and insufficient time during routine appointments to discuss all behaviors. Further exploration of these issues is warranted.
Agitated behaviors exhibited by individuals with Alzheimer’s disease in this study spanned all three agitation domains defined by the International Psychogeriatric Association (i.e., excessive motor activity, verbal aggression, physical aggression (Sano et al., 2023)). Importantly, higher frequency of agitation in individuals with Alzheimer’s disease was associated with significantly poorer caregiver outcomes including (1) likelihood of high burden; (2) likelihood of anxiety and depression; and (3) work and activity impairment. The association between agitation and caregiver experience is consistent with the literature, which generally supports a linkage between neuropsychiatric symptoms such as agitation/aggression and increased stress among caregivers of individuals with Alzheimer’s disease (Delfino et al., 2021). Furthermore, specific agitated behaviors have been shown to contribute to different aspects of caregiver experience (Patrick et al., 2022). Relatedly, anxiety and depression have also been reported in caregivers of individuals with Alzheimer’s disease, with more severe symptoms among caregivers caring for those with more problematic behaviors, including agitation (Delfino et al., 2021; Dura et al., 1991; Givens et al., 2014). Regarding work and activity impairment, caregivers reported providing an average of 39.1 hours of care per week for their loved ones, equating to a full-time work week in the US. In addition to caregiving, more than two-thirds of caregivers were employed elsewhere, meaning the hours spent on caregiving were added onto their regular work obligations. Despite the caregivers’ commitment, supplementation with additional non-paid and paid care was often required. Together, these findings suggest that agitated behaviors have a great impact on caregivers, calling to attention the need to develop long-term strategies to support caregivers and protect their mental health. Future longitudinal research is also warranted to assess the impact of agitation and other neuropsychiatric symptoms on both caregivers and those living with Alzheimer’s disease over time.
The effect of agitation on caregiving was exacerbated by the COVID-19 pandemic, during which most caregivers reported increases in frequency of agitated behaviors displayed by individuals with Alzheimer’s disease and their own caregiving responsibilities. These results were consistent with a previous pandemic study that showed worsening of behavioral symptoms in 52% of individuals with Alzheimer’s disease, which were associated with an increase in anxiety, depression, and distress among their caregivers (Rainero et al., 2020). These changes may have manifested due to the isolation policies implemented during the pandemic, which may have led to exacerbation of agitated behaviors. Alternatively, the prolonged period of home confinement may have made caregivers more aware of certain behaviors that have been overlooked in usual circumstances. Caregivers of individuals with Alzheimer’s disease often lack social contact and experience feelings of social isolation (Brodaty & Donkin, 2009; Brodaty & Hadzi-Pavlovic, 1990), issues that may have further been worsened by the pandemic (Roach et al., 2021). Indeed, in a prior study implementing a caregiver survey, half of caregiver respondents reportedly seeing someone from outside their home only once a week or less during the pandemic (Altieri & Santangelo, 2021), despite evidence of a protective effect against a pandemic-related sense of abandonment with help available from acquaintances or services (Zucca et al., 2021). These findings highlight the importance of support for caregivers caring for individuals with Alzheimer’s disease, particularly when faced with behavioral symptoms such as agitation.
Overall, our study builds upon prior studies and illustrates the experience of caregivers of individuals with Alzheimer’s disease in relation to agitated behaviors. It also quantifies the caregiver experience in terms of mental health and work and activity impairment, thereby demonstrating how improvements in agitated behaviors may help improve the overall experience of caregivers. Evidence-based strategies aimed at managing agitation may therefore not only ameliorate outcomes of individuals with Alzheimer’s disease but also have the potential to improve the caregivers’ mental health and productivity in their daily lives. Assessment and management of agitation in Alzheimer’s disease is an area of interest in the field (De Mauleon et al., 2021; Ismail et al., 2013), and treatments aimed at reducing the frequency of agitated behaviors in individuals with Alzheimer’s disease are undergoing clinical evaluations (Magierski et al., 2020). If proven effective, these treatments may help improve the experience when caring for individuals with Alzheimer’s disease. Furthermore, the development of tools and resources to mitigate agitation among individuals with Alzheimer’s disease may help them foster a better relationship with their caregivers, which may in turn enhance the caregivers’ overall well-being.
Despite the novelty, the current study is subject to certain limitations. First, the study included only respondents accessible through the Dynata’s panel who wished to participate in the study; as a result, the sample may not be representative of the US population of caregivers of individuals with Alzheimer’s disease living in community-based settings. For instance, the caregiver respondents and the individuals they cared for tended to be younger than the average population of caregivers and individuals with Alzheimer’s disease in the US, and most of them were White; again, potentially affecting generalizability. The younger demographics of respondents may be due to younger people having more willingness and ability to complete online surveys; future studies including caregivers of more diverse age and race/ethnic groups should evaluate whether caregiver experience differs in various populations. Meanwhile, individuals caring for individuals with Alzheimer’s disease who exhibited agitated behaviors may have a higher tendency to participate in studies on this topic, resulting in potential enrichment of agitation in the response. Second, although the survey was designed to evaluate recent events, recall bias or errors in the accuracy or completeness of recalled experiences is possible. Additionally, there was no operational definition of Alzheimer’s disease in this study. The survey relied on anonymous, caregiver-reported medical information, including Alzheimer’s disease diagnosis and agitated behaviors, which may be subject to inaccuracies; further, in the absence of access to medical records, it was not possible to obtain information on the clinical workup that led to the Alzheimer’s disease diagnosis (e.g., biomarkers, imaging and laboratory assessments). Third, while the CMAI is intended to be administered by a trained professional, the CMAI assessments in this study were completed independently and online by the respondents, potentially introducing error. However, pilot tests with eligible respondents were conducted prior to data collection, in which respondents indicated that the CMAI was easy to understand and complete. Further, educational materials were provided to respondents in advance to help them accurately complete the assessments and mitigate this issue. Fourth, the sample size was limited to the maximum that could be collected in the vendor’s panel (i.e., based on the number of eligible panel members and response rates), and the current sample size did not have sufficient power to allow for adjustments for multiple comparisons. Future studies with larger sample sizes are warranted to confirm these results. Lastly, this is an observational study, and thus no causal inferences can be drawn.
Conclusion
Findings from this US caregiver survey suggest that individuals with Alzheimer’s disease frequently experience several different agitated behaviors, and these behaviors are associated with substantial negative effects on caregiving experience, mental health, work productivity, and daily activities of their caregivers, underscoring the importance of agitation management. Strategies supporting caregivers caring for individuals with Alzheimer’s disease are warranted to protect their mental health. The development of tools and resources, as well as treatments, to mitigate agitated behaviors in Alzheimer’s disease has the potential to improve the overall caregiver experience.
Supplemental Material
Supplemental Material - Agitation in individuals with Alzheimer’s disease: An assessment of behaviors using the cohen-mansfield agitation inventory in community-dwellers and impact on caregiver experience
Supplemental Material for Agitation in individuals with Alzheimer’s disease: An assessment of behaviors using the cohen-mansfield agitation inventory in community-dwellers and impact on caregiver experience by George Grossberg, Cynthia Willey, Christy Houle, Jeff Schein, Rebecca Bungay, Martin Cloutier, Marjolaine Gauthier-Loiselle, Deborah Chan and Annie Guerin, Zahinoor Ismail in Dementia
Footnotes
Acknowledgements
Medical writing assistance was provided by Loraine Georgy, PhD, and Flora Chik, PhD, MWC, employees of Analysis Group, Inc., a consulting company that has provided paid consulting services to Otsuka Pharmaceutical Development & Commercialization, Inc.
Author contributions
George Grossberg, Cynthia Willey, Christy Houle, Jeff Schein, Zahinoor Ismail, and Jyoti Aggarwal contributed to study conception and design, data analysis and interpretation. Rebecca Bungay, Martin Cloutier, Marjolaine Gauthier-Loiselle, Deborah Chan, and Annie Guerin contributed to study conception and design, collection and assembly of data, and data analysis and interpretation. All authors were involved in the writing and reviewing of this manuscript and approved the final content.
Declaration of conflict of interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: George Grossberg served as a clinical consultant to Otsuka Pharmaceutical Development & Commercialization, Inc. and Lundbeck LLC at the time the study was conducted. Cynthia Willey served as an epidemiologic consultant to Janssen Pharmaceuticals and Otsuka Pharmaceutical Development & Commercialization, Inc. at the time the study was conducted. Christy Houle was an employee of Lundbeck LLC at the time the study was conducted. Jeff Schein and Jyoti Aggarwal are employees of Otsuka Pharmaceutical Development & Commercialization, Inc. Rebecca Bungay, Martin Cloutier, Marjolaine Gauthier-Loiselle, and Annie Guerin are employees of Analysis Group, Inc./ULC, a consulting company that has provided paid consulting services to Otsuka Pharmaceutical Development & Commercialization, Inc. Deborah Chan was an employee of Analysis Group, Inc. at the time the study was conducted. Zahinoor Ismail has served as a consultant to Biogen Inc., Eisai Co., Ltd., Lundbeck LLC, Otsuka Pharmaceutical Development & Commercialization, Inc., and F. Hoffmann-La Roche Ltd.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Otsuka Pharmaceutical Development & Commercialization, Inc. The study sponsor was involved in several aspects of the research, including the study design, interpretation of data, and writing of the manuscript.
Ethical statements
Data Availability Statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental Material
Supplemental material for this article is available online.
Appendix
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.