
Abstract
Difficulty with everyday activities is a key symptom and defining feature of dementia, relating to subjective reports of well-being and overall quality of life. One way to support individuals in their daily activities is by modifying the physical environment to make it easier to interact with during activity performance. This systematic review explores the range of studies available using physical environmental strategies to support performance in everyday activities for people with dementia. Seventy-two relevant studies were identified by the search. Physical environmental strategies included changes to the global environment and to architectural features, use of moveable environmental aids and tailored individual approaches. Strategies supported general everyday activity functioning (N = 19), as well as specific activities, particularly mealtimes (N = 15) and orientation in space (N = 16); however, few studies were found that focused on aspects of personal care such as dressing (N = 1) and showering or the preferred hobbies of individuals (N = 0). Overall, there appeared to be a lack of research within private home environments, and of studies which specify the dementia syndrome or the whole neuropsychological profile of people with dementia. More work is needed to extend theoretical understandings of how people with dementia interact with their environments so that these spaces can be designed to further support activities of daily living performance. Future work in this field could also incorporate the perspectives and preferences of those living with dementia.
Keywords
Background
Dementia is one of the leading health and social economic challenges of our age (World Health Organisation, 2012) with 47.47 million people worldwide estimated to be living with dementia and this number projected to rise to 135.46 million by 2050 (Prince, Guerchet et al., 2013). Whilst there is no cure, understanding how to support people to live well with dementia is of key importance. The ability to engage independently in everyday activities is closely linked to feelings of well-being for people with dementia (Andersen, Wittrup-Jensen, Lolk, Andersen, & Kragh-Sørensen, 2004) and to reduced carer burden for family members (Potkin, 2002). Therefore, one way to support people living with this disorder, and carers, is to understand difficulties with daily activities and develop strategies to support them.
Previous research has shown that functioning in everyday tasks is affected early in dementia and this has been classified as a defining feature of the disorder (DSM-IV criteria). Activities of daily living (ADL) scales have been developed and standardised to clinically assess these difficulties. Scales typically include measures of basic ADLs (BADLs) or self-care tasks such as eating, drinking and dressing, and measures of instrumental ADLs (IADLs) or more complex everyday tasks such as using the telephone, shopping and participating in hobbies. For example, the Bristol Activities of Daily Living Scale (BADLS) (Bucks, Ashworth, Wilcock, & Siegfried, 1996) developed in the UK includes 20 items assessing both BADLs and IADLs, which carers perceive as challenging for people with dementia. Typically, the more complex IADLs have been found to be impaired early in dementia (Barberger-Gateau, Dartigues, & Letenneur, 1993), followed by BADLs as the disease progresses (Mohs, Schmeidler, & Aryan, 2000). However, these findings should be taken with caution as some research has found significant differences in performance for each IADL (Giebel, Challis & Montaldi, 2014) and BADL item (Giebel, Sutcliffe, & Challis, 2015) and variation across individuals with dementia.
People with dementia can be supported in their ability to perform everyday activities, for example, with behavioural therapy (Rogers et al., 1999; Staal et al., 2007), social support (Phinney, 2006) and cognitive training (Zanetti et al., 1997). Predominantly, however, the focus in the literature is on modifying the external physical environment to make it easier to interact with during activity performance. Theoretically, this is often justified using the ‘Press-Competence Model’ (Lawton & Nahemow, 1973). This model suggests that as competence declines, as in dementia, with a progressive deterioration in various functions, the environment places increasing demands on an individual. These demands are thought to cause maladaptive behaviours, or as evidenced above, for people with dementia, increasing difficulties with performing everyday tasks. Applying Powell-Lawton’s theory, modifying the external environment may help to maintain the ‘maximum performance potential’ for individuals, supporting their independence and quality of life in everyday activities for longer.
Existing reviews on physical environmental interventions for people with dementia demonstrate the positive effects some strategies can have on quality of life (Day, Carreon, & Stump, 2000; Fleming, Crookes, & Sum, 2008; Gitlin, Liebman, & Winter, 2003), affect and behaviour (Beck, 1998; Cohen-Mansfield, 2001; Daykin, Byrne, Soteriou, & O’Connor, 2008; Padilla, 2011) and spatial/perceptual abilities (Caffò et al., 2013; Marquardt, 2011; Letts et al., 2011). For example, Padilla (2011) reviewed 33 papers and found features such as a visually complex environment, music and light therapy reduced agitation and negative behaviours. There is some debate around the definition of the ‘physical environment’ used within existing reviews (Gitlin et al., 2003). For the purpose of this paper, we follow the definition of the ‘physical layer’ of the environment provided by Harris, McBride, Ross and Curtis (2002) to include the ambient environment (lighting, noise, temperature), architectural aspects (permanent features, e.g. physical layout) and interior design features (less permanent aspects, e.g. layout, furnishings, objects and design).
Arguably, carrying out everyday tasks may be particularly well supported by environmental strategies given that they involve direct interaction with the external environment. Nevertheless, there is a knowledge gap in terms of understanding the scope and evidence for environmental strategies supporting performance in various everyday activities. Only one previous review was identified on this topic (van Hoof, Kort, van Waarde, & Blom, 2010); however, this article did not address the full range of everyday activities and focused on good practice guidelines rather than evidence-based studies.
The present review is intended to fill the knowledge gap and address the following questions: (1) How is bodily performance in everyday activities supported by evidence-based research using the physical environment? (2) What is the breadth of this research in terms of the activities that are being supported and the dementia ‘populations’ and settings that are included? Given evidence which suggests the majority of daily activities take place within the living dwelling for people with dementia (Evans, 2003), the review is focused on research in the private home/residential environment as opposed to internal or external public spaces.
Method
The review includes a diverse range of studies with different research designs which called for an integrative and flexible methodology for the evidence to be synthesised and appraised appropriately. Content analysis was applied in the first instance to group and code environmental strategies identified in the articles to support pre-described everyday activity categories. To do this the BADLS (Bucks et al., 1996) with 20 daily activities was used as a framework and each study was assigned a code (1–20) according to the category it fitted. This scale was selected as it covers a range of IADLs and BADLs which are reported to be affected from early in the disease by carers (Bucks et al., 1996). Types of environmental strategies for each activity category are summarised and descriptively appraised in the ‘Findings’ section.
Search strategy
A comprehensive literature search was conducted from September 2014 to March 2015. This involved searches using the following electronic databases: Scopus, CINAHL, Google Scholar, Web of Science, PubMed and PsycInfo. A combination of search terms is used including: ‘dementia’ OR ‘alzheimer’s’ AND ‘activities of daily living’ OR ‘ADLs’ OR specific ADL terms from BADLS (e.g. ‘dressing’, ‘hobbies’, ‘orientation in time’) AND ‘physical environment’ OR ‘environmental adaptation/changes/modifications’, ‘design intervention’, ‘assistive technology’. The following relevant journals were also hand searched: ‘Social Care Online’, ‘Dementia’, ‘American Journal of Alzheimer’s Disease and Other Dementias’, ‘Environment and Behaviour’, ‘Journal of Environmental Psychology’, ‘The Gerontologist’, ‘Alzheimer’s Care Quarterly’, ‘Ageing and Society’. This was carried out to ensure all relevant articles were picked up by the search terms used. A final manual searching of reference lists from existing literature reviews on environmental strategies and dementia was conducted and appropriate references were added to the catalogue.
Selection criteria
Articles were included if they met the following inclusion criteria:
The population of interest was people with a diagnosis of dementia. The variable of interest was some element of the ‘physical environment’ here defined as everyday design aspects within the living space such as ambient features (e.g. music/lighting), interior design features (e.g. furnishings and less permanent objects) and architectural features (permanent features, e.g. altering the spatial layout) (similar to Harris et al. (2002)). This included assistive technology and devices which affect the physical design of the environment as opposed to items or articles belonging to the person (e.g. wheelchairs or special clothing). The study included at least one outcome measure relating to the ability of the person with dementia to bodily perform one or more everyday activities. The study was conducted in a real-world setting where the person with dementia spends a sufficient amount of time carrying out everyday tasks (i.e. day centre, home, care home). The study was published in English.
Data synthesis
An online reference manager (Refworks) was used to keep track and sort references during the literature search period. All studies which met the inclusion criteria were read in full and classified into everyday activity categories (see Figure 1). The articles were then split evenly amongst three authors (RW, MPS, EH) and each study was summarised into a data extraction form (Coren & Fisher, 2006). The team then came together to review the forms and arrive at a consensus on types of environmental strategies and to descriptively appraise the findings.
Flow diagram showing results from search strategy and categories of daily activities supported by physical environmental strategies.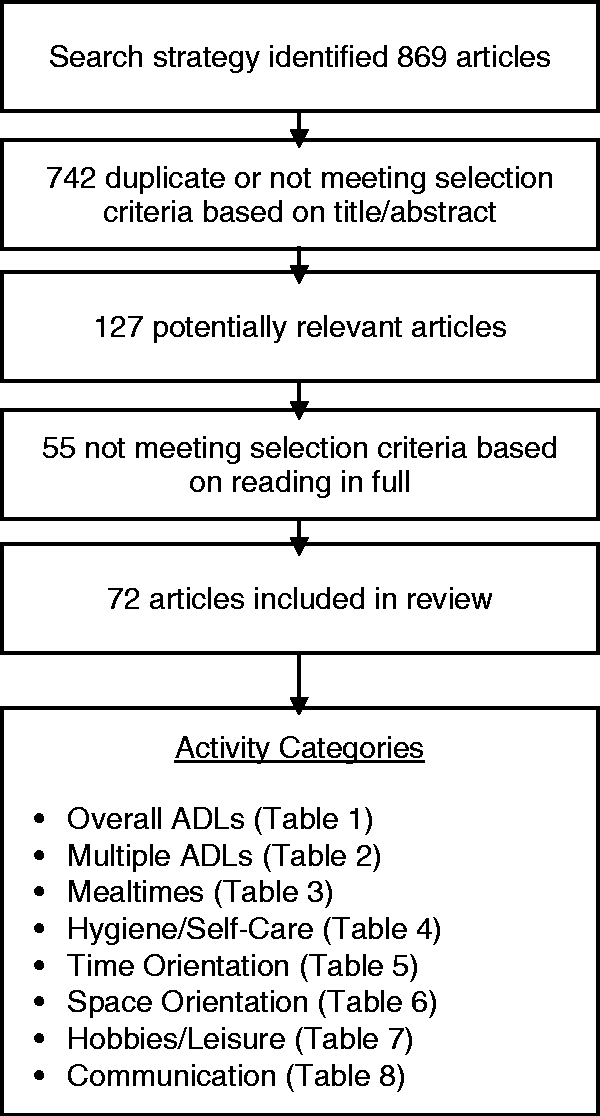
Findings
The systematic search identified a total of 869 results, of which 72 papers were considered relevant for final review (Figure 1). The ‘Findings’ section is organised into subheadings of activity categories with themes of environmental interventions for each grouping.
Study characteristics
Overall, the majority of the studies identified by the search were conducted in the USA (N = 48.6%), followed by Europe (N = 27.8%; N = 9.7% UK based), Canada (N = 16.7%), Australia (N = 5.6%) and Japan (N = 1.4%). Within this research 34.7% included people with moderate–severe cognitive impairment and 15.3% included people with mild–moderate cognitive impairment. Fifty per cent of the studies did not specify cognitive status or included a mixture of people with dementia who had mild-severe cognitive impairment. Eighty-five per cent of the studies identified were conducted in residential settings compared to 15% within private home environments. Overall, from the studies reviewed, specific activities from the BADLS which appeared to be most supported by environmental strategies were orientation in space and eating/drinking whereas aspects of self-care such as dressing, toileting and brushing teeth appeared to be less supported (see Figure 2). The majority of the research identified looked at the impact of environmental strategies on overall ADL performance without specifying which activities, in particular, may be benefiting from the strategy.
Graph displaying frequency of studies identified by the literature search by BADLS item.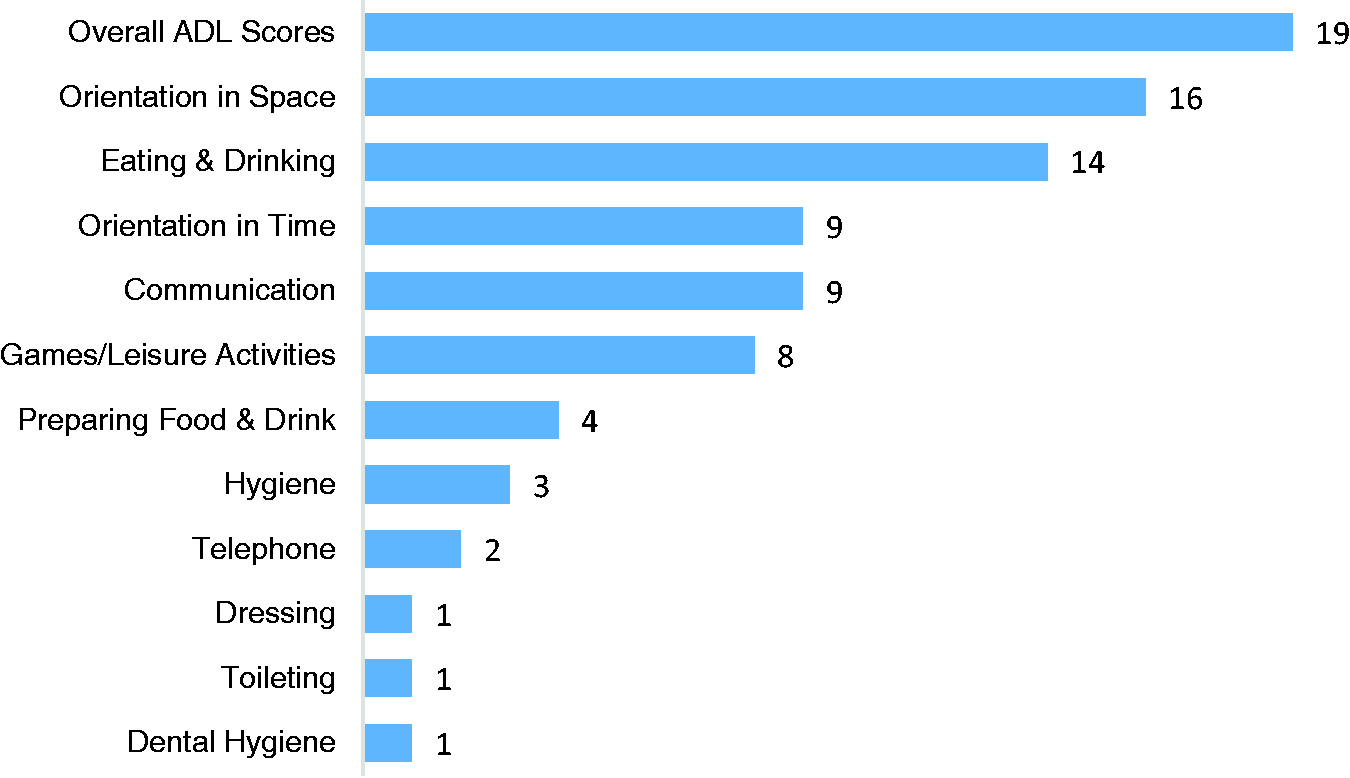
Overall ADL functioning
Overall ADL functioning.
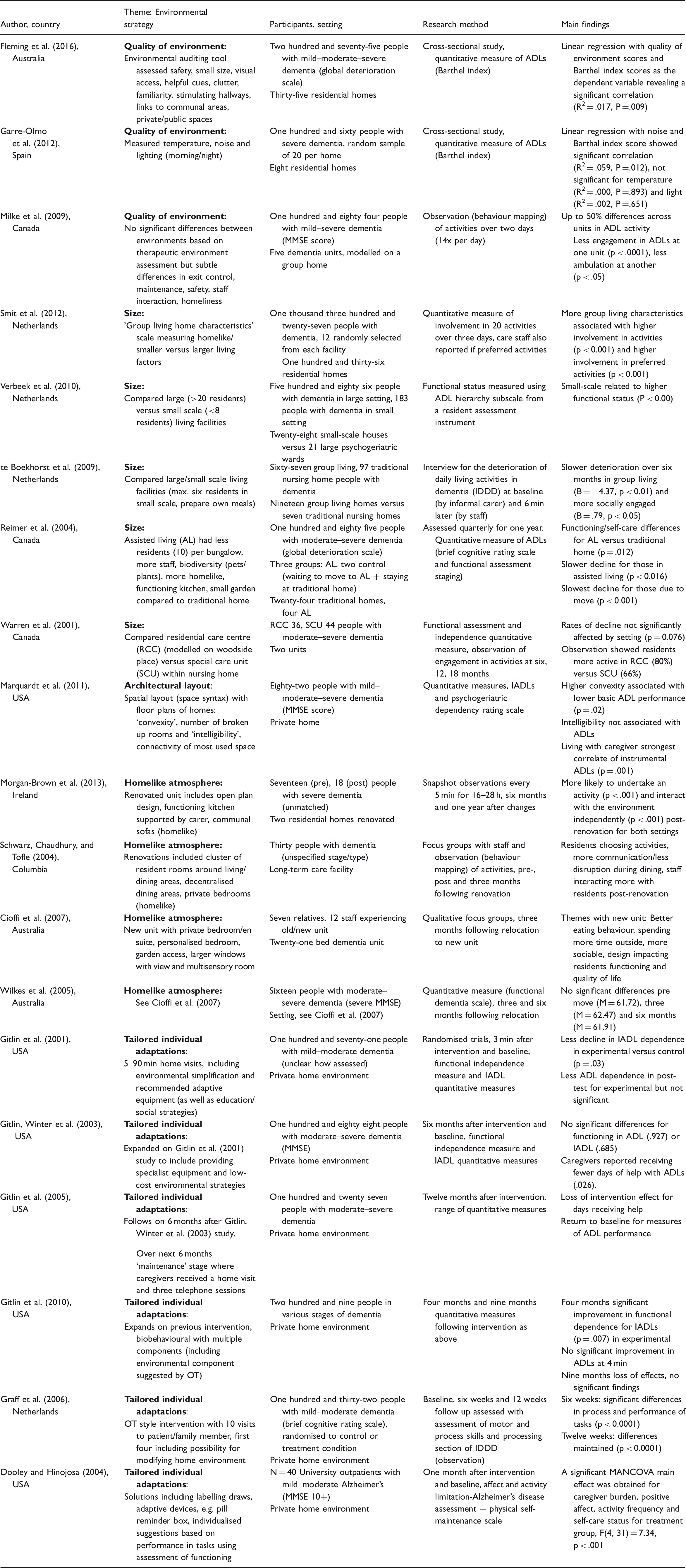
ADL: Activities of daily living; IADLs; instrumental ADLs; MMSE: Mini Mental Status Exam.
Quality of the environment
Two studies were interested in looking at associations between the quality of the environment and quality of life for people with dementia. However, both included a measure of ADL performance for residents using the Barthel index and therefore calculations using the original data are reported here (Fleming, Goodenough, Low, Chenoweth, & Brodaty, 2016; Garre-Olmo et al., 2012). Linear regression modelling showed a positive correlation between environmental quality (e.g. familiarity, engaging environments, range of private/communal spaces) and Barthel index scores (Fleming et al., 2016). Garre-Olmo et al. (2012) focused on ambient features of the environment (temperature, noise, lighting) across a smaller selection of eight residential facilities and results suggested ‘noise’ was significantly associated with the ability to perform basic ADLs. Another study by Milke et al. (2009) compared five very similar facilities, modelled on a ‘household’ setting and found subtle environmental differences, (e.g. exit control, safety, homeliness), predicted up to 50% difference in engagement in everyday activities based on observations.
Size
A large study by Smit, de Lange, Willemse and Pot (2012) compared 136 facilities and found smaller settings with more group living/homelike characteristics were associated with significantly higher involvement in activities among residents with dementia and perhaps more importantly, involvement in preferred activities based on staff feedback. Another large study (Verbeek et al., 2010) also found living in a smaller facility was associated with higher functioning in ADLs. Verbeek and colleagues discussed this relationship in terms of people with higher functional status being selected as residents for smaller assisted living facilities, whereas Smit and colleagues discussed the reverse (the environment was causing differences) thereby demonstrating issues with determining cause-and-effect relationships here. Some studies compared small versus large facilities and functioning in ADLs longitudinally. Reimer, Slaughter, Donaldson, Currie and Eliasziw (2004) and te Boekhorst, Depla, de Lange, Pot and Eefsting (2009) found a significantly slower rate of deterioration in everyday activity performance over six months and one year for people living in smaller settings compared to larger settings. Warren et al. (2001) failed to find this effect over 18 months; however, their study was restricted to comparing two settings whereas the former two studies were comparatively larger (comparing 26–28 facilities).
Architectural layout
Marquardt et al. (2011) considered the spatial layout within private home environments (N = 83) in relation to ADL ability among people with dementia. They found negative associations between ‘convexity’ or more open-plan living and BADL performance (but not IADL performance) based on quantitative measures, suggesting enclosed rooms with clear functions are more supportive. ‘Intelligibility’ or connectivity of frequently used space to the rest of the house was not found to be associated with ADL functioning.
Homelike atmosphere
Research comparing the effects of building renovations appeared to be aimed at creating a homelike atmosphere, although they differed in the types of changes they made in order to do this. For example, Morgan-Brown, Newton and Ormerod (2013) observed differences in activity engagement pre/post changes to two dementia units which included open-plan living, a functioning kitchen and communal sofas. They found more engagement in activities and independence in activities (p < .001) post-renovation, for both settings. Schwarz, Chaudhury and Tofle (2004) employed a similar design to examine the impact of renovations such as a decentralised dining space, clustered living rooms and private bedrooms, observing that residents tended to have more choice around which activities to participate in, alternating their time between central and local living spaces. Two studies evaluated the impact of one renovated unit whereby key changes included private bedrooms, personalised rooms, garden access and larger windows. Qualitative focus groups demonstrated changes in ADL performance such as ‘better eating behaviour’ and ‘more time outside’ (Cioffi, Fleming, Wilkes, Sinfield, & Le Miere, 2007) whereas these changes were not picked up in the quantitative assessment as no significant differences in ADL performance were noted at three months or six months post-renovation (Wilkes et al., 2005).
Tailored individual adaptations
Gitlin, Corcoran, Winter, Boyce and Hauck (2001), Gitlin, Hauck, Dennis and Winter (2005) and Gitlin, Winter et al. (2010) have published a series of randomised controlled trials using home-based environmental interventions. The environmental component involved factors such as removing or labelling objects, the use of colour contrast, clutter management and purposeful placement of objects, although it was not specified exactly which changes were implemented. They found limited effects on ADL performance in their early study with people with moderate–severe cognitive impairment. For example, at six months they found family members reported providing significantly less help with ADL activities compared to a control group (p = .026, Gitlin, Winter et al., 2003), however this returned to baseline at 12 months post-intervention (Gitlin et al., 2005). In a later study with people with mild–moderate cognitive impairment and with an extended version of the intervention (including more time with the occupational therapist and a biological component), they found significantly higher independence in IADLs (p = .007) compared to a control group though this was lost 12 months after the intervention (Gitlin et al., 2010). It is worth noting this intervention involved an educational and training aspect for carers and therefore the exact impact of environmental adaptations on outcome measures is unknown. A similar study was conducted by Graff et al. (2006) using a more sensitive measure of ADL ability and found significant effects for the treatment group at six weeks (p < .0001) and 12 weeks (p < .0001) post-intervention; however, again this was a multi-component intervention and exact environmental changes were not specified. Dooley and Hinojosa (2004) conducted a narrower study which involved suggesting environmental solutions based upon observed performance in various everyday tasks for 40 people with dementia living at home. They found a significant group effect for this intervention on activity frequency and self-care ability.
Multiple everyday activities
Multiple everyday activities.

ADL: Activities of daily living; MMSE: Mini Mental Status Exam; QOL: quality of life.
Tailored individual adaptations
Chard, Liu and Mulholland (2009) conducted a study similar to Dooley and Hinojosa (2004) (Table 1) whereby they observed five people with dementia performing an everyday task (e.g. setting the table, folding laundry) and suggested environmental solutions based on their performance. Strategies such as removing clutter, simplifying the environment and using labels were found to be associated with improved performance in a subsequent observation session (p < 0.05).
Assistive technologies
Assistive technology research appears to be in its infancy, with studies identified using exploratory methods (e.g. product testing and qualitative feedback) and small numbers of participants (N < 28) to understand the value of technological devices for people with dementia. A locator device, medication carousel (Cash, 2004), automatic lighting (Evans, Carey-Smith, & Orpwood, 2011), simple mobile phone and TV remote control (Arntez, Holthe, & Jentoft, 2014) have been reported as particularly useful for supporting everyday activities. On the other hand, systems which automatically telephone family members for help (Cash, 2004) and a digital calendar (Arntez et al., 2014) were identified as less useful and confusing to use.
Mealtimes
Mealtimes.

ADL: Activities of daily living; MMSE: Mini Mental Status Exam.
Tailored individual adaptations
Josephsson, Bäckman, Borell, Nygård and Bernspång (1995) used observation of meal preparation tasks to form the basis of environmental changes implemented for individuals. Removing clutter, using labels and providing a table with a model example were found to be associated with improved ability to prepare drinks and set the table in subsequent observations for three (N = 4) people with dementia.
Assistive technologies
One qualitative study looked at the use of an assistive device attached to the stove to support meal preparation for nine people living at home with dementia (Starkhammar & Nygård, 2008). Consistent with above reports of assistive technologies, the device enabled people to begin or carry on cooking. However, it was also reported to be irritating and confusing to learn how to use this technology.
Lighting and contrast
Koss and Gilmore (1998) found increased light intensity and visual contrast related to increased food intake for 13 people with dementia. This was replicated by Dunne et al. (2004) who focused solely on effects of visual contrast of dining ware with nine residents and found significant increases in food (>25%) and fluid (>84%) consumption for high visual compared with low visual contrast (p < .001) regardless of colour (i.e. blue or red). Brush, Meehan and Calkins (2002) compared intake in a nursing home (N = 11) and assisted living setting (N = 14) and found a significant increase in food intake for higher light levels and table contrast conditions in the assisted living setting, whereas results did not reach significance for the nursing home. This suggests other factors may impact on the effects lighting and contrast can have overall. For example, as discussed earlier, people with less severe cognitive impairment are more likely to live in assisted living facilities (Verbeek et al., 2010) which may have affected outcomes for this study.
Quality of the environment
Two cross-sectional studies were identified which compared eating environments across different care settings finding that ‘quality’ of the environment, particularly less institutional (more homelike features) related to increased food intake for residents with dementia (Reed, Zimmerman, Sloane, Williams, & Boustani, 2005; Slaughter & Morgan, 2012). Another study by Perivolaris, Leclerc, Wilkinson and Buchanan (2006) relates to quality and creating a more homelike dining atmosphere. They renovated the dining area in two facilities to include a fireplace, bright design, aromas of food, a menu board and more food choice. They found significantly more food was consumed for 11 people with dementia following the environmental changes (p = 0.05), with further positive effects when staff were given nutrition training. A similar study by McDaniel, Hunt, Hackes and Pope (2001) evaluated the effects of renovating a residential facility and found no significant increases in calorie intake. However, whilst some changes may be supportive such as ‘no television’ and ‘relaxing music’ during meals, the refurbished setting also included higher noise and lower lighting levels which may have counteracted effects.
Environmental ambiance
One study looked at the effects of introducing an aquarium with eight large fish into the dining settings of three residential facilities for 70 people with dementia (Edwards & Beck, 2013). They found there was a significant increase in food intake with the aquarium at two weeks (p < .000) and this trend continued for the following six weeks. Another piece of research was concerned with creating a pleasant acoustic environment around resident’s music preferences (Thomas & Smith, 2009). They reported descriptive results whereby playing the most preferred music during dining, compared to no music, led to a 20% increase in the amount of food consumed for 12 people with dementia.
Choice
Another theme emerged for mealtimes around providing choice at mealtimes. Three studies looked at the effects of serving help yourself meals versus a more institutional approach of pre-prepared plates within care settings. All found significant effects for the help yourself layout: residents with dementia consumed more (Altus, Engelman, & Mathews, 2002; Desai, Winter, Young, & Greenwood, 2007), exhibiting more positive mealtime behaviours (e.g. appropriate use of utensils and napkins) (Melin & Götestam, 1981) and communicated more at the table with fellow residents (Altus et al., 2002; Melin & Götestam, 1981). A further observation study fits this theme whereby they looked at placing snacks in accessible refrigerators around a dementia facility (Namazi & Johnson, 1992b), comparing a glass door fridge where snacks were visible to a standard fridge where snacks were not visible. They found visibility of snacks did not affect independent snacking although lack of rigor within the research design, such as adding red tape to a fridge door handle during the study as it was proving difficult to open, may affect the validity of these findings.
Hygiene and self-care
Hygiene and self-care.

MMSE: Mini Mental Status Exam.
Tailored individual adaptations
A study by Connell, McConnell and Francis (2002) examined the impact of tailored environmental solutions to support oral care for five individuals with dementia. Strategies included using pictures as models, providing coloured cups and magnified mirrors and a consistent layout. They observed that four out of five of the residents became more independent in this task and there was a 47% improvement in dentist hygiene ratings with the environmental intervention.
Assistive technology
Two studies evaluated the effects of a wall-mounted prompting system to support handwashing steps by videoing trials to examine the number of steps completed by individuals with dementia (Labelle & Mihailidis, 2006; Mihailidis, Boger, Craig, & Hoey, 2008). The first of these studies compared audio and visual-audio prompting systems and found the video system was most effective in supporting people with dementia (n = 8). The later study developed the audio-visual prompting device and found people with dementia (n = 6) were able to complete 11% more handwashing steps individually with 60% fewer interactions with professional carers. Cognitive status based on Mini Mental Status Exam (MMSE) scores was not found to affect the ability to interact with the device in this study.
Familiar cues
Boger, Craig and Mihailidis (2013) examined the effects of five different tap designs which varied in familiarity. They observed familiarity correlated with ease of use with the dual-lever design found to be most accommodating in supporting independent handwashing. They also found familiarity of tap design was more important than cognitive status (MMSE) in predicting the ability to complete handwashing steps.
Simplifying the environment
Namazi and Johnson (1992a) found sequentially arranging clothes in a separate section of the wardrobe for eight people with moderate–severe dementia increased independent dressing by 19% according to staff observations. This was the only study identified around dressing and whilst it offers a simple demonstration of the effectiveness of wardrobe modification, it could benefit from replication with a larger sample.
Orientation to space
Although an ADL is its own right (Table 6), environmental strategies to increase orientation to space can also be used to support other activities, in this case toileting. Namazi and Johnson (1991) (Table 6) found that arrows and a sign with the word ‘toilet’ to cue people with dementia towards the bathroom were effective in supporting 44 people with dementia to enter and use the toilet independently. Picture cues were found to be less effective overall based upon these observations.
Orientation to time
Orientation to time.

MMSE: Mini Mental Status Exam.
Orientation to space.

MMSE: Mini Mental Status Exam.
Familiar cues
Bailey and Haight (1994) found pairing bath day with a pictorial cue of a duck resulted in a significant increase in recognition (p < .005) of bath time by people with dementia. Another more recent study (Tanaka & Hoshiyama, 2014) looked at enhancing visual cues in the dining area to support mealtimes. They found introducing a bright tablecloth and flowers to signify lunchtime resulted in a significant increase in recognition before and after the meal. Pairing this with music resulted in a further increase in recognition. These findings may help to explain mealtime research which suggests renovated, homelike environments relate to increased food intake; perhaps these new environments provide stronger cues to signify it is dinner time. Another study by Nolan and Mathews (2004) used a large clock and sign to signify mealtimes for 35 residents with dementia. They found significantly less questioning about time of day to staff before breakfast and dinner (not lunchtimes) with this cue.
Assistive technology
The only multi-country study identified for this review features here involving 50 people living at home with dementia across Norway, Lithuania, Ireland, UK and Finland (Topo et al., 2007). They conducted repeated qualitative interviews with patients and family members over 12 months of using a night and day calendar. As with other assistive devices there were some issues reported around ease of use but most found it useful overall, particularly when motivated to use it. Another study by Kerkhof, Rabiee and Willems (2015) examined the use of a digital planning board mounted to the walls in the living room and residents’ bedrooms in a group living facility in the Netherlands. The daily schedule, including mealtimes and housekeeping activities, was presented on the boards under photographs of each resident. When it was time for an activity this sounded in the living room and the activity lit up on the board. Similar to Topo et al. (2007), positive qualitative responses included confidence, peace of mind and convenience for residents; however, others had problems with use and some felt staff should tell them the daily schedule.
Orientation to space
A large number of studies were identified around using the physical environment to support wayfinding, all within residential facilities (Table 6).
Architectural layout
Early research by Netten (1989) compared the layout of six group homes and seven communal homes and the wayfinding abilities of 104 residents with moderate–severe dementia, as rated by staff. They found for communal homes, simple two-way decision pathways and a smaller number of exits supported independent wayfinding whereas shorter length of routes and a clear decision point was supportive in smaller group homes. Later research by Elmståhl, Annerstedt and Åhlund (1997) found L-shaped corridors were useful for wayfinding when comparing 18 residential facilities. A more recent larger investigation by Marquardt and Schmieg (2009) compared 30 nursing homes and wayfinding skills for 450 residents with mild–severe cognitive impairment. They found straight direct routes supported orientation more than routes that required a change in direction.
Familiar cues
The study mentioned earlier by Namazi and Johnson (1991) is relevant here, whereby they observed the ability of people with dementia to find their way to the toilet using various cues. They found wayfinding skills were better with signs using the word ‘toilet’ and arrows, rather than familiar pictures (e.g. of a toilet). Two further studies looked at the effects of cues when residents were asked to find their way to various locations. One issue with this, in comparison to naturalistic observation, is that residents may have been less motivated to get to locations. Nolan, Mathews and Harrison (2001) found bedroom wayfinding ability increased from one-third correct trials to 100% correct within a few days when pictures of the residents as children and a sign with their name was placed on the bedroom door for three people with severe cognitive impairment. An earlier study by Namazi, Rosner and Rechlin (1991) failed to find an effect of providing familiar objects (memorabilia) outside people’s bedrooms, although trials for this study were not repeated. Two studies have explored the use of multi-sensory cues to facilitate wayfinding ability. Gibson, MacLean, Borrie and Geiger (2004) provided differential cues outside the bedrooms of 19 people with dementia, varying colour, texture, structure and location. Respondents reported using colour and structure, in particular to help them find their way, and the researchers found those who were better able to find their rooms reported using two or more environmental cues. A study by Caffò et al. (2014) compared the effects of providing familiar cues along routes versus assistive technology with lights and remote controlled sounds to cue wayfinding. They observed that four residents with dementia were significantly better finding their way using the assistive technology cues over familiar objects, highlighting the importance of developing and using new technological devices.
Distracting cues
A set of six early studies emerged from the literature search which involved disorientating people with dementia by providing distracting cues away from the exit door of residential facilities. These included environmental strategies such as distracting grid patterns of black tape (Chafetz, 1990; Hewawasam, 1996; Hussain & Brown, 1987) or covering up the exit door with a blind (Dickinson, McLain-Kark, & Marshall-Baker, 1995), mirrors (Mayer & Darby, 1991) or a wall mural (Kincaid & Peacock, 2003). Whilst all but one (Chafetz, 1990) found significant effects of these barriers on exit-seeking behaviour, this raises an important issue: who is this for? Whilst distracting people with dementia may be orientating them into spaces staff would prefer them to be in (with safety in mind), this may be disorientating the person with dementia if their aim is to go outside, which could cause distress and a loss of freedom.
Leisure activities
Leisure activities.

MMSE: Mini Mental Status Exam; QOL: Quality Of Life.
Gardens
A study by Mather, Nemecek and Oliver (1997) examined behaviour when access to the garden was available in the summer compared to when it was locked in winter. They observed that in summer, 54% of time was spent sitting in the garden and only 7% was spent actively conversing with others in this space. The study by Murphy, Miyazaki, Detweiler and Kim (2010) was more robust and measured visits to a new garden area over 12 months for 34 residents with dementia. They found the garden was most used when first introduced whereas use decreased significantly over time suggesting ‘novelty’ of the garden area as a leisure space may wear off. They also found for residents in wheelchairs spending time in the garden was associated with increased agitation, highlighting the importance of taking into account individual’s health limitations. Another study by Edwards, McDonnell and Merl (2013) observed residents use of a new addition garden to a dementia facility. They found all residents used the garden space over a TV room during leisure time; however, measures were only taken at baseline and three months therefore it is unknown if this is a ‘novelty’ effect. Hernandez (2007) conducted qualitative interviews with 45 residents with dementia following the introduction of a garden at two different facilities. This space enabled activities such as planting in the garden, sunbathing and relaxing. Another study using qualitative interviews found garden space was useful for staff and family members to spend time with residents (Detweiler, Murphy, Myers, & Kim, 2008).
Environmental ambiance
Yao and Algase (2006) conducted a naturalistic comparison of 30 nursing homes and 17 assisted living facilities and used video recording to analyse the movement of residents within these settings. They found engaging and soothing spaces related to more sitting time and less walking. Similarly, Cohen-Mansfield and Werner (1998) found residents spent more time sitting in corridor areas after they were refurbished, with a nature setting (including pictures of forests and sounds of birdsong) rated as significantly more ‘pleasing’ than the plain corridor setting.
Simplifying the environment
An early study by Namazi and Johnson (1992c) looked at the effects of reducing environmental stimulation during an art activity on concentration during the task, by putting up barriers between individuals. They found higher barriers reduced distractions significantly for 12 individuals with dementia. Again, this raises the issue of whether this environmental strategy is for the resident with dementia or staff. Completing the recreational activity may be important to the teacher facilitating this activity whereas perhaps the person with dementia would prefer to be distracted by their neighbour and communicate with others around the room.
Communication
This final category includes studies which have been mentioned in previous sections. For example, creating homelike meal settings was found to enhance communication between staff and residents with dementia (see Altus et al., 2002; Brush et al., 2002; Melin & Götestam, 1981; Nolan et al., 2001; Perivolaris et al., 2006; Thomas & Smith, 2009, Table 2). The study by Mather et al. (1997) also observed 7% active communication among staff and residents with dementia when a garden space was provided. On the other hand, some environmental solutions may be ‘disabling’ communication (e.g. Mihailidis et al., 2008; Nolan & Mathew, 2004) as they support people with dementia to independently complete everyday tasks without the need to interact with staff.
Communication.
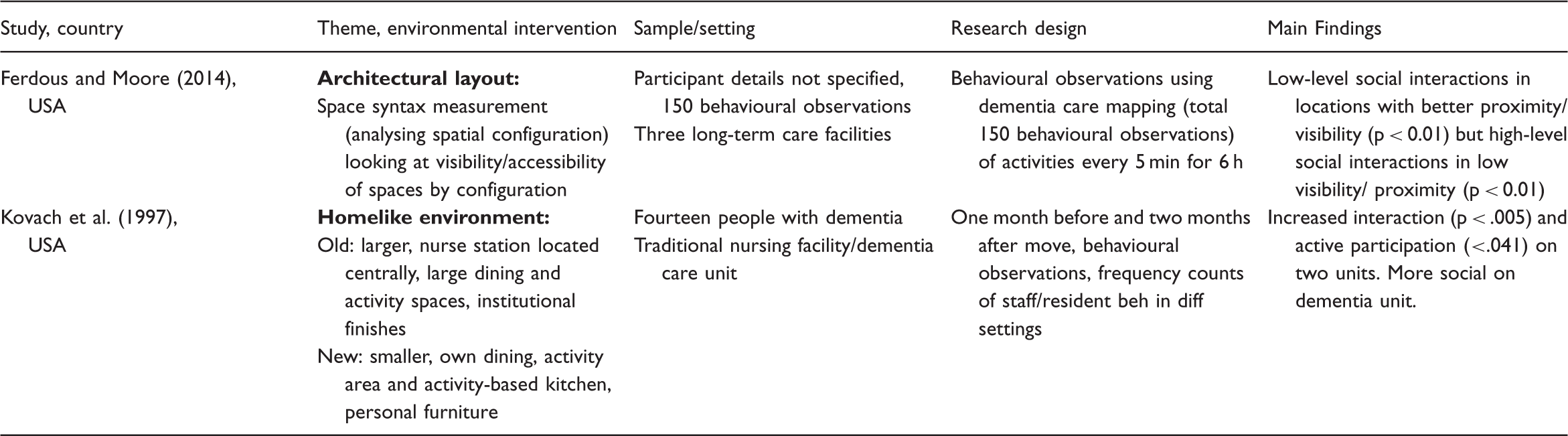
The final study (Kovach, Weisman, Chaudhury, & Calkins, 1997) relates to the strategy of creating a homelike environment whereby the researchers examined the impact of renovating two different facilities on interaction among residents. They found the renovations related to an increase in interaction (p < .005) for both centres demonstrating the importance of homelike atmospheres for fostering social relations.
Discussion
Overall, this review demonstrates there is a role for the physical environment in supporting bodily performance in everyday activities among people with dementia. A diverse range of papers testing various physical environmental strategies across a range of everyday activities were identified. Given this diversity it was not possible to use existing quality appraisal measures to assess the quality of research; however, the studies were descriptively assessed for quality (similar to Caffò et al. (2013)). In reviewing and appraising this work, some important discussion points were raised around the complexity of research on the physical environment and where resources should be targeted in future to best support people with dementia.
Researching the physical environment
The research identified aims to understand how the real-world physical environment impacts the way people with dementia externally perform everyday activities, a topic which is methodologically complex but vitally important for understanding how to design dementia-friendly supportive spaces. As with any research in real-world environments, the independent variable is co-existing with multiple other variables making it methodologically challenging to manipulate. Large-scale studies examining the effects of multiple changes in the environment or comparing multiple buildings to overall ADL performance (e.g. Fleming et al., 2016; Smit et al., 2012; Verbeek et al., 2010) provide strong evidence that the holistic environment does impact performance of daily activities for people with dementia. Longitudinal research even suggests the holistic environment may be protective in terms of slowing decline in everyday functioning for people with dementia (Reimer et al., 2004; te Boekhort et al., 2009) highlighting the importance of research into the physical environment. However, these large-scale, macro-level studies do not tell us which aspects of the holistic environment have an impact on performance, making it difficult to replicate these findings and translate them into practice settings. Furthermore, understanding how the environment is affecting activity performance is difficult; for example, ‘quality’ environments and building renovations may impact staff well-being and the way staff support residents with dementia, having an indirect effect on daily activity performance. These potentially confounding variables are difficult to control for, as summarised by Fleming et al. (2008), the psycho-social and physical environment often go hand in hand.
In contrast, studies which measure the effects of more specific changes to the environment, e.g. colour contrast crockery versus white plates for food intake (Dunne et al., 2004) (Table 3), are advantaged in demonstrating the specific environmental elements that have an impact, however they often lack methodological rigour. For example, the study by Dunne et al. (2004) was conducted with nine people with advanced dementia and limited to one setting, making it difficult to generalise findings. However, the environment is made up of infinite components and to test each, and replicate this work, would require an extensive amount of resources, possibly explaining why many environmental suggestions are based upon work with small samples or good practice guidelines (see van Hoof et al., 2010).
From the studies identified, a range of measures were used to determine effects of physical environmental strategies on activity performance making it difficult to appraise the quality of this research overall, for example using critical appraisal tools. Quantitative research provides significant data for a number of environmental strategies supporting activity performance (e.g. Marquardt & Schmieg 2009; Tanaka & Hoshiyama, 2014). Some quantitative studies used existing ADL scales to measure overall everyday activity performance (e.g. Gitlin et al., 2001; Wilkes, Fleming, Wilkes, Cioffi, & Le Miere, 2005); however, from this data it is unclear which everyday activities in particular may be benefitting from the environmental strategy. Coupled with the above issue of not knowing which environmental change has an impact, this poses a significant challenge to the applicability of such findings. Qualitative research demonstrates people’s opinions of how environmental strategies benefitted their everyday performance, providing important information, e.g. that some assistive technologies are difficult to learn to use (e.g. Kerkhof et al., 2015; Topo et al., 2007). However, people may not be able to accurately report the effects of the environment on overall daily functioning, as exemplified by Wohlwill’s (1973) report title ‘The Environment is Not in the Head!’. Observation methods may provide a more objective measure of the effects of the environmental strategy, however do not tell us how people with dementia feel about the environmental component and are open to observer bias. Ten of the studies identified by the search used a combination of measures (e.g. Brush et al., 2002; Edwards et al., 2013; Schwarz et al., 2004) which may be most effective, albeit time consuming, for this type of research.
A further complication when researching the physical environment for people with dementia concerns ‘novelty’ effects of new environments. Behaviour (of people with dementia and/or carers) may change in association with an environmental change, but individuals may become habituated to these new environments, with functioning in everyday activities returning to baseline in time (e.g. Murphy et al., 2010). This is further complicated by the fact dementia is a progressive disease; therefore, it is unknown how people with dementia may habituate or respond to environmental strategies in time. Some of the research identified for review was conducted longitudinally for over 12 months (e.g. Murphy et al., 2010; Warren et al., 2001); however, the majority was cross-sectional and longer term follow-up research may be necessary. Cross-sectional studies are further complicated by the fact there may be key between-group differences which may explain differences in ADL performance (e.g. Smit et al., 2012; Verbeek et al., 2010).
Applicability of the Powell-Lawton model
Theoretically, many of the studies identified drew on Lawton & Nahemow (1973) ‘Press-Competence Model’ to justify the use of physical environmental strategies. However, this model was originally designed in relation to ageing as opposed to dementia. With this in mind, many of the studies focused on cognitive function (e.g. MMSE score) to measure competence. However, dementia is a multi-faceted disease which can affect multiple other cognitive domains including memory, language, perception and decision making as well as motor functions. Furthermore, different types of dementia syndromes exist and there is a lack of specification in the studies identified regarding the specific disease profile.
The linear model designed by Powell-Lawton may not be detailed enough to capture the dementia experience and in turn, understand the effects of the environmental strategies to support these. This is supported by the fact that some studies did not find MMSE scores related to the effectiveness of environmental solutions (e.g. Labelle & Mihailidis, 2006; Mihailidis et al., 2008). Perhaps to move forward with this type of research, a more complex model taking into account the full ‘neuropsychological profile’ of individuals with dementia combined with ‘environmental press’ (Lawton & Nahemow, 1973) and psycho-social factors is needed. This is supported by a recent review (Giebel et al., 2015) which highlights there is a lack of knowledge about the error patterns associated with individual everyday activities for people with dementia.
Providing tailored environmental strategies for individuals which support specific areas of difficulty may be the most effective way to facilitate ADLs, given profiles of dementia can vary considerably from person to person (e.g. Gitlin, Winter et al., 2005, 2003; Graff et al., 2006). For example, using written signs to support wayfinding may be helpful for a person with exclusive memory impairment whereas visual contrast and pictorial cues may support someone who in addition has perceptual difficulties due to dementia.
Future directions
From the literature search, it appears activities such as mealtimes and orientation in space are particularly well researched in this field, whereas other daily activities such as self-care and dressing may be overlooked (Figure 2). This may be due to mealtimes being reported as a significant problem for people with dementia, e.g. increasing weight loss (White, Pieper, & Schmader, 1998) and/or functioning in this activity being easier to measure, e.g. food intake, over personal activities such as showering. Hobbies were one activity which appears to be overlooked by this research, as no studies were identified using the physical environment to support people with their preferred leisure activities. This raises the important issue around where resources should be targeted to help people with dementia (and carers) to live well. An article by Harmer and Orrell (2008) examined meaningful activity for people with dementia within residential settings and found activities which support psychological and social needs are important for individuals with dementia, therefore supporting hobbies with environmental strategies may be particularly useful. Personhood is important here, in terms of recognising an individual’s needs and desires around the daily activities that are most important to him/her. Future qualitative research could work more with people with dementia in being a part of developing and discussing environmental strategies.
Following on from this, studies should be clear about who the environmental strategy is for. For example, some residential studies may be more supportive for staff as opposed to people with dementia. For example, research around disorientating people with dementia away from exit doors (e.g. Chafetz, 1990; Hewawasam, 1996) may be seen as helpful for staff as opposed to people with dementia, whereby such strategies may cause distress or confusion. Often strategies designed to increase independence in activities, by definition, reduce social interactions. For example, adding a digital planning board reduces the need for residents to talk to staff about the day’s activities (Kerkhof et al., 2015). This may have a negative impact on the quality of life of people with dementia, where engaging with others in this context may be socially important. Staff are an important aspect of the holistic residential environment, therefore providing solutions which support all setting participants may be advantageous; however, studies should be clear on this focus.
Given 85% of the studies identified were conducted in residential settings where people in more severe stages of dementia are likely to live (Knapp et al., 2007), this raises issues around whether supporting independence in everyday functioning is most appropriate. Environmental strategies in residential settings may be better targeted towards supporting affect or overall well-being (e.g. Gitlin, Liebman et al., 2003; Padilla, 2011) rather than activity performance outcomes. Supporting people at home in earlier stages with environmental strategies for activity performance may be particularly useful, both in terms of maintaining their self-identity in everyday tasks and for supporting family carers in terms of reducing stress and carer burden (Graff et al., 2006). However, entering the home space for environmental research is overwhelmingly complex given these spaces are highly variable. Nevertheless, research such as by Dooley and Hinojosa (2004) and Marquardt et al. (2011) demonstrates possibilities for this type of research.
Conclusion
To conclude, this is an important area of research which appears to support a role for the environment in assisting people with dementia to perform a range of everyday tasks. Future studies could include individuals with dementia in developing environmental strategies to further understand where to focus resources to best support ADL function and related quality of life and well-being (Andersen et al., 2004). Theoretical understanding of how people with dementia interact with the environment during activities may also help in designing specific environmental adaptations. Models would need to incorporate the multi-faceted nature of dementia which differs across individuals. Targeting neglected spaces such as the private home and activities such as hobbies and personal care may also be beneficial. Overall, this research area is rich with plenty of opportunities for growth. The wide range of studies demonstrates opportunities for developing a battery of design concepts which can support individuals with dementia in daily life.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review was supported by a studentship from Brunel University London. The studentship is attached to a grant from the ESRC-NIHR (UK) (Grant ES/L001810/1). Grant title: Seeing what they see: compensating for cortical visual dysfunction in Alzheimer’s Disease. SC is also supported by the NIHR Queen Square Dementia Biomedical Research Unit and an Alzheimer’s Research UK Senior Research Fellowship.