
Abstract
People living with dementia and their carers require ongoing support in the community. Memory clinics can provide a range of supports including education, respite and symptom management. While these clinics improve consumer outcomes, their impact on the carers of people living with dementia is unclear. This review sought to identify and critically synthesise the literature on the effectiveness of memory clinics in supporting carers. An integrative review process was used to identify papers from CINAHL and Medline databases. Of the eight included papers, two were qualitative and six were quantitative studies. Three themes were identified, namely; psychological heath, carer burden and satisfaction with memory clinics. Four studies found decreases in caregiver burden, distress, and psychological symptoms such as anxiety and worry. Satisfaction with the clinic model was discussed as a source of support by carers, highlighting the memory clinics. The variable outcomes seen in this review require further research to elucidate the impacts of memory clinics on carers along the dementia trajectory.
Introduction
Approximately 50 million people worldwide were living with dementia in 2017, and this number is projected to triple by 2050 (World Health Organisation, 2021). In Australia, given that two in three people living with dementia are being cared for in the community (Australian Institute of Health and Welfare, 2023), some 219,000 people and their carers require support in navigating living with dementia (Australian Bureau of Statistics, 2020).
Carers are individuals who provide unpaid care services to a friend or family member who is unable to care for themselves due to their health circumstances (Carers Trust, 2021). Carers for people living with dementia are crucial as they provide essential support to address the complex health needs associated with living with dementia (Lee et al., 2018). Carers help maintain dignity and independence by assisting with daily activities and ensuring safety and well-being (Hochgraeber et al., 2023). They also play a key role in managing challenging behaviours and the emotional distress that is often associated with dementia (Jackson & Browne, 2017). Carers find themselves taking charge of their household, are faced regularly with new challenges as the persons’ health needs change and often need to develop new knowledge and skills about how to better support the person living with dementia (Abendstern et al., 2019).
Embracing the role of caring for a person with dementia is often an unexpected challenge and requires a period of transition (Hooper & Collins, 2019). The demanding nature of being a carer can generate a significant burden and impact psychological well-being as dementia progresses and the person loses functional capacity (Large & Slinger, 2015). Yet, the role of the carer is essential if the person with dementia is to remain living within the community. Living in the community provides a sense of independence for people living with dementia as they retain a feeling of normalcy (Cornelis et al., 2018). Continuing care in the community holds significance for families of people living with dementia as it maintains relationships and family structures. Caring in the community also provides the opportunity to continue to engage in recreational and social activities as well as maintaining family routines (World Health Organisation, 2021). Additionally, keeping people with dementia living in the community for as long as possible reduces the burden on the health care and residential aged care system (Waymouth et al., 2023).
Out-patient memory clinics have been established to facilitate the care of people with dementia in the community and provide resources and support for carers (Cornelis et al., 2018; Lertkratoke et al., 2021). Staffing for memory clinics can be multidisciplinary or can be led by specialist Nurse Practitioners who provide referrals to further services (Phillipson et al., 2021). The various models of memory clinics can provide comprehensive outpatient care for people living with dementia and their carers, empowering care to continue in the community (Kovaleva et al., 2021). Despite the growing popularity of this model and the importance of supporting carers in the community, there have been few attempts to synthesise the literature regarding memory clinics and their impacts on carers. Therefore, this integrative review aims to identify and critically synthesise the literature examining memory clinics’ impact on carers of people living with dementia.
Methods
Given the heterogeneous nature of memory clinic interventions reported in the literature, an integrative review was completed using the five-step approach advocated by Whittemore and Knafl (2005).
Search strategy
Search strategy.

Study selection and data extraction
Ninety-four papers were identified from the database search. After removing duplicates, 91 papers were imported into Covidence (Veritas Health Innovation, n.d) for screening. Further review of abstracts revealed that 69 papers were not relevant. This left 22 papers, which were retrieved for full-text review by two authors (AB and AM). Disagreements were resolved by a third reviewer (EH). As 14 papers were excluded, eight papers remained and were included in the review. The selection process is displayed using the Preferred Reporting Items for Systematic Reviews (PRISMA) (Moher et al., 2009) (Figure 1). PRISMA flow-chart.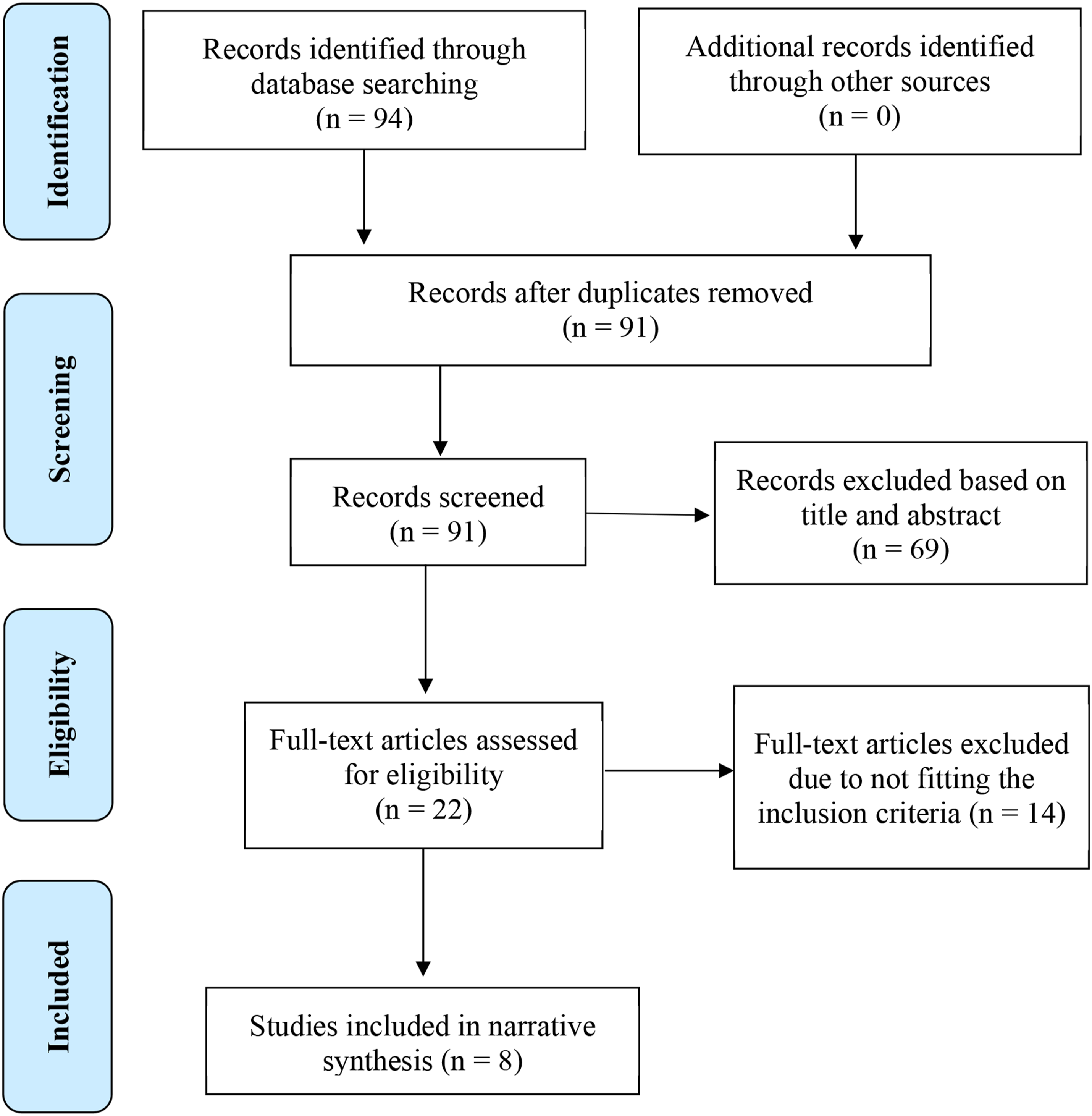
Data extraction and quality assessment
Summary table.
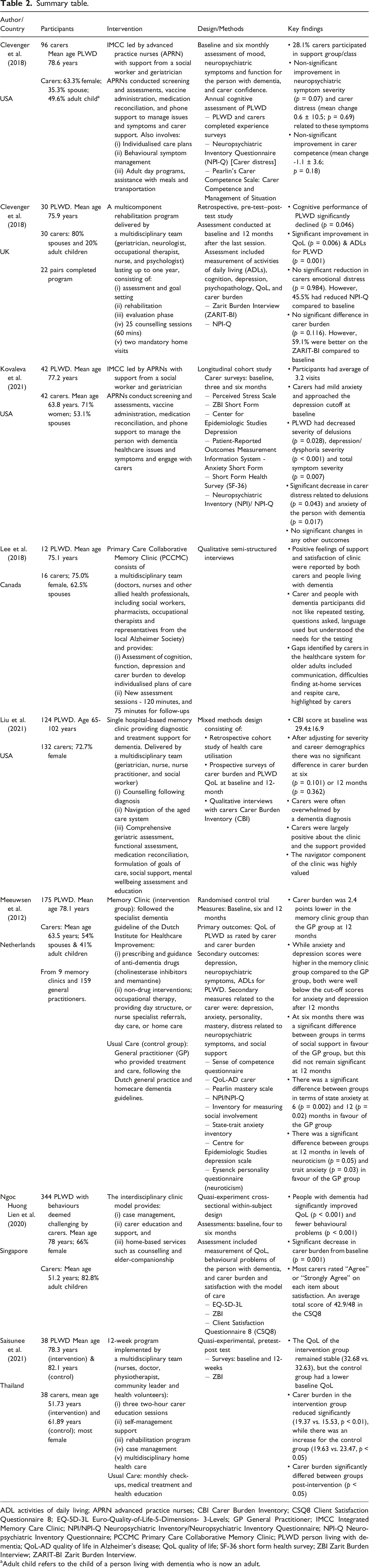
ADL activities of daily living; APRN advanced practice nurses; CBI Carer Burden Inventory; CSQ8 Client Satisfaction Questionnaire 8; EQ-5D-3L Euro-Quality-of-Life-5-Dimensions- 3-Levels; GP General Practitioner; IMCC Integrated Memory Care Clinic; NPI/NPI-Q Neuropsychiatric Inventory/Neuropsychiatric Inventory Questionnaire; NPI-Q Neuropsychiatric Inventory Questionnaire; PCCMC Primary Care Collaborative Memory Clinic; PLWD person living with dementia; QoL-AD quality of life in Alzheimer’s disease; QoL quality of life; SF-36 short form health survey; ZBI Zarit Burden Interview; ZARIT-BI Zarit Burden Interview.
Adult child refers to the child of a person living with dementia who is now an adult.
Results
Characteristics of included studies
Of the eight included studies, three (37.5%) were undertaken in America (Clevenger et al., 2018; Kovaleva et al., 2021; Liu et al., 2021), with one (12.5%) study each reported from Canada, the Netherlands, Singapore, Thailand and the United Kingdom (Table 2). There were four (50.0%) quasi-experimental studies (Clevenger et al., 2018; Cornelis et al., 2018; Ngoc Huong Lien et al., 2020; Saisunee et al., 2021), one randomised control trial (12.5%) (Meeuwsen et al., 2012), one qualitative study (12.5%) (Lee et al., 2018), one cohort study (12.5%) (Kovaleva et al., 2021) and one mixed-method study (12.5%) (Liu et al., 2021).
All studies included both carers and people living with dementia. Sample sizes ranged from 12 (Lee et al., 2018) to 344 (Ngoc Huong Lien et al., 2020) participants. Two studies (25.0%) implemented the same care model, the Integrated Memory Clinic (IMCC) (Clevenger et al., 2018; Kovaleva et al., 2021), while the remaining studies varied in intervention design. In three studies (37.5%), the specific model of care delivered was unclear (Cornelis et al., 2018; Liu et al., 2021; Saisunee et al., 2021).
Two studies (25.0%) focused primarily on carer burden and quality of life (QoL) (Meeuwsen et al., 2012; Saisunee et al., 2021), while the remainder discussed psychological symptoms. The included studies discussed three themes, namely: (1) psychological health, (2) carer burden, and (3) satisfaction with the memory clinic.
Themes
Psychological health
The psychological health of carers was explored in terms of carer distress (4 studies) (Clevenger et al., 2018; Cornelis et al., 2018; Kovaleva et al., 2021; Meeuwsen et al., 2012), depression (2 studies) (Kovaleva et al., 2021; Meeuwsen et al., 2012) and anxiety (2 studies) (Kovaleva et al., 2021; Meeuwsen et al., 2012). All four studies that examined carer distress measured it using the NPI-Q. While Kovaleva et al. (2021) found a significant decrease in symptoms of carer distress in response to the delusions and anxiety of people with dementia, the other studies found no significant reduction in carer distress following attendance at the memory clinic (Clevenger et al., 2018; Cornelis et al., 2018; Meeuwsen et al., 2012).
Anxiety was explored by two (25.0%) studies (Kovaleva et al., 2021; Meeuwsen et al., 2012). A statistical significance reported by Kovaleva et al. (2021) from mild depression at baseline and decreasing after three or six months (p = 0.001), with a decrease in distress related to anxiety of their person living with dementia was also reported within the same timeframe (p = 0.017). Meeuwsen et al. (2012) also recorded a significant difference in anxiety between the study groups in favour of the GP group over the memory clinic group at 12 months (p = 0.03).
Carer burden
Five (62.5%) studies examined carer burden (Cornelis et al., 2018; Kovaleva et al., 2021; Liu et al., 2021; Ngoc Huong Lien et al., 2020; Saisunee et al., 2021). Versions of the Zarit Burden Interview (ZBI) measured carer burden in four (80.0%) studies (Cornelis et al., 2018; Kovaleva et al., 2021; Ngoc Huong Lien et al., 2020; Saisunee et al., 2021), while the remaining study used the Caregiver Burden Inventory (CBI) (Liu et al., 2021).
While three studies (75.0%) reported no significant improvement (Cornelis et al., 2018; Kovaleva et al., 2021; Liu et al., 2021), the remaining two (25.0%) studies reported significant decreases in carer burden following the intervention (Ngoc Huong Lien et al., 2020; Saisunee et al., 2021). Saisunee et al. (2021) found both a significant decrease in carer burden in the intervention group from baseline (p = 0.03) and a significant difference between intervention and control groups (p ≤ 0.05). Similarly, in their study of people with dementia with challenging behaviours, Ngoc Huong Lien et al. (2020) showed significant reductions in carer burden from baseline (p = 0.001). In the three studies that failed to detect a significant difference in carer burden, it was hypothesised that this could either indicate stability in carer burden and levels of stress as positive outcomes for clinics or may show more research is required (Cornelis et al., 2018; Kovaleva et al., 2021; Liu et al., 2021).
Satisfaction with memory clinics
Satisfaction with the memory clinics was explored in three studies (37.5%) (Lee et al., 2018; Liu et al., 2021; Ngoc Huong Lien et al., 2020). Two studies collected qualitative data about the clinic experience for carers and their perceptions of support (Lee et al., 2018; Liu et al., 2021), while Ngoc Huong Lien et al. (2020) used the Client Satisfaction Questionnaire (CSQ8) to measure carer satisfaction. Satisfaction with the clinics stemmed from the social support, individualised care and person-centred approach created, allowing carers to feel that their concerns were heard (Lee et al., 2018; Liu et al., 2021). In their study, Lee et al. (2018) reported that the clinic staff were perceived as knowledgeable, and the clinic environment was found to be welcoming. Additionally, carers drew comparisons between the clinics and primary care visits, expressing appreciation for the longer time allocated for clinic visits (Lee et al., 2018). Interviews conducted by Liu et al. (2021) highlighted the experiences of carers attending the clinic, stating “the memory clinic has been… essential” in their experience of caring for a person living with dementia. Similarly, Ngoc Huong Lien et al. (2020) reported high satisfaction scores among carers.
Discussion
This integrative review has identified and critically synthesised the limited available evidence on the impact of memory clinics on carers of people living with dementia. The focus on caregiver health is paramount to ensuring carers can provide consistent, compassionate care for people living with dementia. Indeed, carer well-being directly influences the quality and sustainability of care provided (Mansfield et al., 2023). This review highlights the limited and mixed evidence to demonstrate the impact of memory clinic interventions on carer burden and psychological health. However, the relatively small number of included studies and challenges in measuring carer outcomes demonstrate the need for further evaluation of memory clinics to provide clearer evidence for future practice. What was clear, however, was the satisfaction of carers with the clinic model as a source of valued support (Lee et al., 2018; Liu et al., 2021; Ngoc Huong Lien et al., 2020). Such a finding encourages further exploration of this model in clinical practice.
This review demonstrated inconsistent findings in terms of carer distress, anxiety, and depression when pre- and post-scores were compared. However, this finding needs to be considered in the wider context. As a person living with dementia experiences disease progression, the carer may be required to adapt to increasing care needs and higher levels of impairment (Liu et al., 2021; Teahan et al., 2021). Carers may also experience increasing levels of distress due to worsening behavioural symptoms of the person living with dementia (Brennan et al., 2017; Teahan et al., 2021). Carers experience significant changes in their daily routines as they revolve more around care requirements. Increasing caring responsibilities may also leave the carer with less time to engage in self-care and meaningful activities for themselves, creating a higher risk for carer burden to develop (Hooper & Collins, 2019).
The limited statistically significant differences in outcome measures seen in this review could be due to the difficulties in measuring outcomes in a group caring for people on a downward health trajectory (Moore et al., 2020). Although there are likely to be periods of stability, people living with dementia and their carers are going to see a general decline in cognition and function over time (Teahan et al., 2021). The unpredictable decline of dementia can have direct implications on the health of the carer as they experience numerous losses throughout their caring journey, as the person with dementia loses cognitive, communication and motor skills (Large & Slinger, 2015). Therefore, the absence of significant worsening should be highlighted as potentially suggesting a positive outcome, that carers have maintained well-being despite the declining disease trajectory (Kovaleva et al., 2021). This complexity highlights the need to consider how to best measure the success of support interventions such as memory clinics.
The relatively small sample sizes, short follow-up duration and research designs may have also impeded the ability of the findings to show statistical significance. Additionally, using single-memory clinics to deliver the interventions may introduce bias (Lee et al., 2018). As such, this review evidences the need for further large-scale, robust studies to provide clearer evidence around outcomes and the impact of this kind of intervention.
This review has demonstrated that qualitative data can provide important insights into the impact of the memory clinic intervention on carers. Qualitative data highlighted several key insights into the experiences of carers, who commonly expressed feelings of being overwhelmed and stressed due to the relentless nature of caring, including managing challenging behaviours, assisting with daily tasks, and coping with their own emotional responses (Liu et al., 2021). Some carers report feeling alienated from the person living with dementia as the disease progresses, and many described a sense of social isolation and a lack of support from their diminishing social networks, exacerbating feelings of carer burden (Engel et al., 2022; Hooper & Collins, 2019). However, the limited qualitative research captured within this review highlights the need for future work to include qualitative data to explore carers’ experiences and their perspectives on interventions such as memory clinics.
Strengths and limitations
A strength of this review is that it has identified and critically synthesised the body of literature on the impact of memory clinics for dementia on carers. A further strength was using an established process to guide the integrative review. The small number of papers included in this review has demonstrated that this area is undervalued in the literature. Additionally, the variations in interventions around the structure of the clinics and the scope of the interventions precluded meta-analysis. The increased burden on carers during the study period may not have been accounted for when comparing pre- and post-intervention scores due to increased caring responsibilities. While the included studies all measured carer outcomes, these were often secondary to the outcomes related to the person living with dementia. Given the carers’ important role in keeping the person living with dementia in the community, further research should be designed to more carefully evaluate the impact of the clinic on their health and well-being and the caring role.
Conclusion
The literature examined in this review highlighted the lived experiences of carers for people living with dementia attending memory clinics through key elements of psychological health, carer burden and satisfaction with clinics. The psychological well-being of carers requires constant adaptation due to the increasing care needs of people living with dementia. This review identified that carers had significant support needs that the memory clinics addressed to some extent. However, further qualitative research examining carers’ experiences attending memory clinics may provide deeper insight into the carers’ experiences and the value of the clinic to their health and well-being.
Footnotes
Author contributions
AB, AM & EH were responsible for the conceptualisation, literature searching, formal analysis and project administration. AM & EH were the research supervisors. AB drafted the manuscript and all authors contributed to the review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.